
Abstract
The aim of this study was to explore perceptions of mental health services from the perspectives of adolescents with no prior service experience. Thirty students in the Transition Year (fourth year) of secondary school participated in this study: 22 females and 8 males, aged 15 to 16. There was equal distribution across rural and urban settings. Participants had no prior experience of accessing mental health services. Data were collected in secondary school settings in the Republic of Ireland. An interpretive description approach guided this study. Data were collected through individual interviews. To complement interviews, participants drew images of mental health care environments and mental health staff members; drawings were not subjected to analysis. Data (participant interviews) were analyzed using qualitative content analysis. Three themes were identified. Participants suggested that “mental health services” differed from “psychiatric services,” with the latter term perceived more negatively. Uncertainty about how to access these services was voiced. Considering the vulnerability of adolescents to the experience of mental distress, education around mental health services is warranted. It is expected that provision of education in this area would enhance service delivery, improve adolescents’ help-seeking behaviors for mental distress, and reduce stigma.
Introduction
The word “adolescence” stems from the Roman “adolescere” (to grow up). Although there are inconsistencies in terms of how the various stages of adolescence are defined, Steinberg (2019) acknowledged that, within the social science literature, adolescence is generally categorized as early (10–13 years), middle (14–17 years), and late (18–21 years). During adolescence, individuals undergo a psychosocial transition from the dependence of childhood into independent adult roles (Moses-Payne et al., 2021; Steinberg, 2019). It is a period associated with self-discovery, with shaping and consolidating one’s identity. Adolescents learn to think in abstract terms about their position in the social environment, and how environments and relationships with others affect them (Briggs, 2008; Steinberg, 2019).
Relationships with peers, exposure to multimedia and education, and parental guidance, all influence the construction of a belief model about the world during adolescence (Ardèvol-Abreu, 2015; Valle et al., 2015). Wray-Lake et al. (2010) suggest that, through observing the perceptions of adolescents, it is possible to catch some glimpse of the likely nature of the future state of our world. They argue that identities begin to form in adolescence, and influential events encountered during this important period can often impact on the person’s decisions in adulthood. Although people will constantly revise their understandings of the world as they encounter new information and experiences (McLean, 2008), their core values, attitudes, and behaviors can often be traced back to experiences and influences encountered during their adolescence (Flanagan, 2004; White & Swartzwelder, 2013; Wray-Lake et al., 2010). It is also a pivotal time for the advancement of decision-making faculties, with individuals beginning to make more complex inferences about the social world (Steinberg, 2019).
It is during adolescence that many individuals first experience symptoms of mental distress (Kaasbøll et al., 2021; Okewole et al., 2016). Mental distress is defined as a wide variety and heterogeneous set of experiences that can make it difficult to carry on with everyday activities, including anxiety, low mood, and psychoses (Cromby et al., 2013; Gordon et al., 2018). Although early intervention is recommended to effectively address the needs of adolescents experiencing mental distress (Vusio et al., 2021), this population often demonstrate poor help-seeking behaviors (Goodwin, Behan et al., 2016; Sears, 2020). While it has been suggested that lack of knowledge about services and stigma act as barriers to help-seeking (Byrne et al., 2015; Gagnon et al., 2017), little is known about how adolescents perceive mental health services.
Studies have been conducted on the general public’s beliefs and knowledge about mental illnesses, with adolescents frequently being the target population of this research. The focus of these studies has been depression (Askevis-Leherpeux et al., 2015; Coles et al., 2016; Tissera & Tairi, 2020) and schizophrenia (Melas et al., 2013; Sawamura et al., 2012; Tissera & Tairi, 2020). Less is known about how adolescents view mental health services. Previous research has reported that adolescents are unlikely to consider psychiatrists (Aluh et al., 2018; Essau et al., 2013; Thai et al., 2020) and psychologists (Aluh et al., 2018; Thai et al., 2020) as helpful resources in the event of experiencing mental distress. Furthermore, it has been noted that adolescents are unable to describe the role of counselors (Tharaldsen et al., 2017). Adolescents have also expressed uncertainty and negative attitudes toward psychiatric medication (Munizza et al., 2013; Ojio et al., 2015) and psychiatric hospitals (Aluh et al., 2018; Goodwin, Savage et al., 2016). Coles et al. (2016) found that adolescents would not recommend help from anybody; this is a concern, given the vulnerability of this population group to the experience of mental distress.
Although it has been noted that perceptions of mental health can be traced back to childhood (Weiss, 1994), it is during adolescence that people begin to make sense of the social world around them, using their observations to make decisions about how to model themselves (Steinberg, 2019). However, the extant research suggests that observations about mental health services are primarily negative, which may result in poor help-seeking behaviors at a time where service intervention may be crucial. Therefore, it is important to explore the perceptions of mental health services from the perspectives of adolescents with no prior experience of accessing services. Such exploration helps to highlight deficiencies in knowledge and areas where awareness needed to be enhanced and to identify barriers to accessing healthcare services (Bowers et al., 2020; Simons et al., 2017). Although there are some limited qualitative investigations into adolescents’ perceptions of mental health services (e.g., Tharaldsen et al., 2017), much of this research has adopted quantitative designs (e.g., Aluh et al., 2018; Ojio et al., 2015), resulting in a lack of context for why mental health staff, treatments, and care environments are often negatively perceived. The aim of this qualitative study is to explore perceptions of mental health services from the perspectives of adolescents with no service experience.
Method
Design
An interpretive descriptive methodology was adopted (Thorne et al., 1997), underpinned by ontological relativism (i.e., the assumption of multiple realities) and epistemological interpretivism (i.e., knowledge is a highly subjective, and the researcher’s interpretations play an integral part in the research process) (Scotland, 2012).
Interpretive description facilitates researchers to create a design consistent with the research questions/aims and work outside the confines of traditional “off-the-shelf” methodologies, allowing the research question to dictate the way in which methods should be applied. It encourages a highly inductive approach to research, producing description, but also uncovering the deeper meaning within data (Thorne, 2016). Interpretive description distinguishes itself from other qualitative approaches—such as grounded theory—in that it is not interested in theory testing, and is does not hold the requirement “that all studies must be explicitly positioned within one or another formal theory” (Thorne, 2016, p. 70). In this regard, interpretive description may be considered “atheoretical” (Thorne, 2016).
Sample
Adolescents undertaking the transition year (TY) secondary school education program were included in this study. In Ireland, many adolescents aged 15 to 17 undertake the TY program, during which, in addition to education needs, an emphasis is placed on personal and social development, with mental health and wellbeing becoming a recent emphasis (Mental Health Ireland, 2021). Therefore, TY students were deemed to be a suitable group to invite as participants in this study.
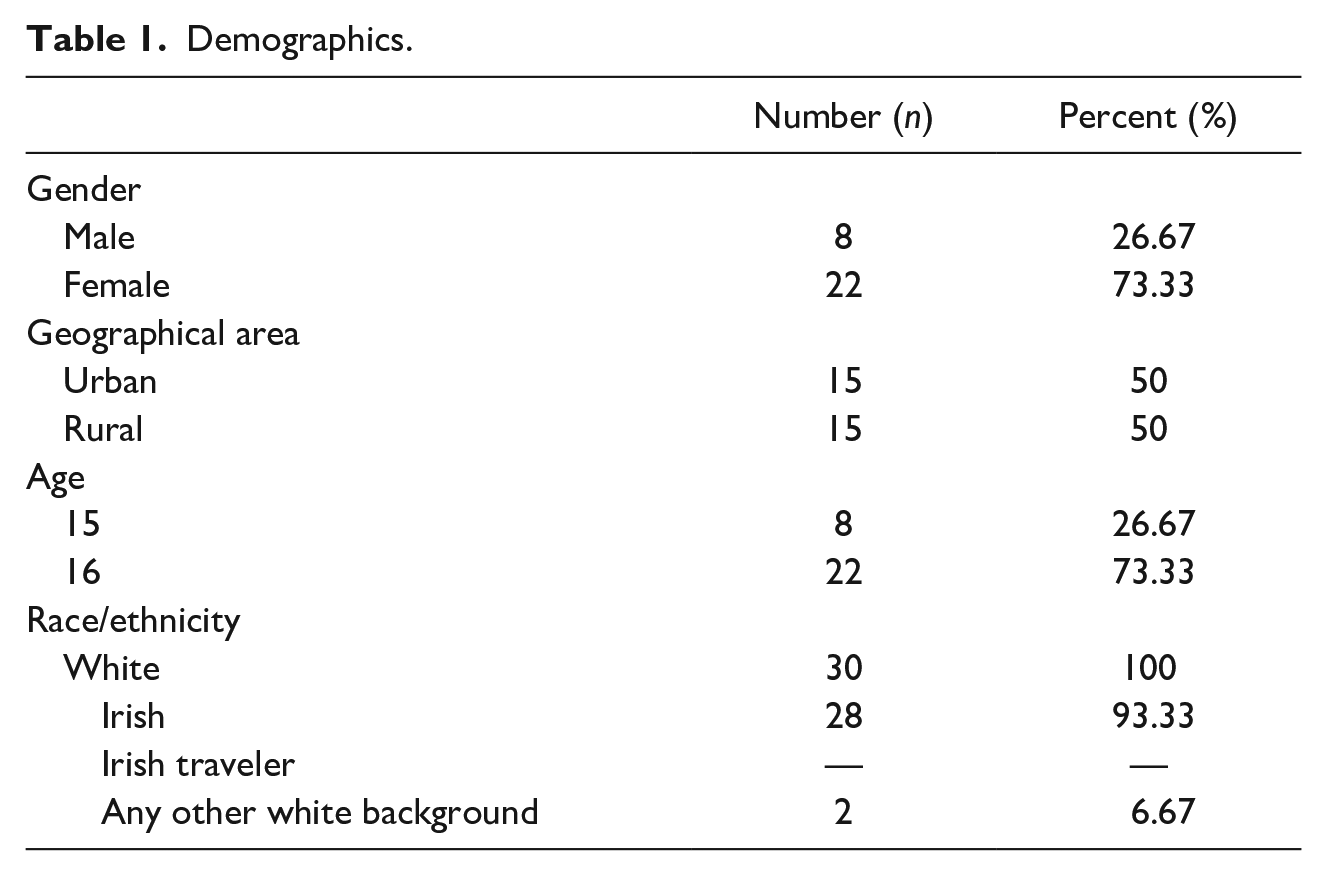
In studies where interviews are conducted with those without experience of phenomena, the sample size is often quite large when compared to other qualitative studies, with Rasche et al. (2016) sampling 30 participants; we also aimed to recruit 30 participants. Letters were sent to schools informing them of the study, with school contact details retrieved from an online repository (IrelandStats, 2017). Schools were chosen at random; however, given that geographical location may have some influence on perceptions of mental health services (Goodwin, Savage et al., 2016), both rural and urban areas were approached. Once contact was made, a gatekeeper (teacher) was established at each site. Six schools were initially approached and three schools (one urban, two rural) agreed to participate. The first author visited each school to introduce the study and distribute an information pack. We aimed to recruit an equal number of participants from rural and urban areas, that is, 15 from both areas. Fewer males than females initially agreed to participate in the study. All males, other than one who did not meet the inclusion criteria, were included. Female students were selected on a “first-come-first-serve” basis. Fifteen students (four males, eleven females) from the urban school participated. Ten students (one male, nine females) from the first rural school participated. Five students (three males, two females) from the second rural school participated. Overall, a purposive sample of 30 students in the Transition (4th) Year of secondary school participated in the study: 22 females, 8 males (see Table 1).
Demographics.
Ethics
Ethical approval to undertake the study was gained from the University’s Social Research Ethics Committee. Participation was voluntary and all data were anonymized (pseudonyms are used to disguise participants’ identities). Informed consent was obtained from parents/guardians who filled out a form provided in the information pack. Informed written and verbal assent was obtained from each participant at the point of data collection. Written consent and assent was obtained to use quotes from participants and to reproduce their drawings in a thesis, publications, and conference presentations.
Data Collection
Data were collected using semi-structured interviews. Several authors have commented that engaging adolescents in research can be challenging (Nolan et al., 2018; Thompson, 2016). To enhance engagement in the study, adolescents were encouraged to produce drawings. These drawings acted as prompts, complementing the interview process. The draw-and-tell technique (Williams et al., 1989) has been used with children (Coyne et al., 2021), but also with adolescent populations, aged 11 to 16 (Kwon et al., 2017; McWhirter et al., 2004).
Participants were provided with paper, pencils, crayons, and markers; they were also given the option to draw using an electronic tablet and stylus. No time restrictions to produce drawings were placed on participants. Participants were first invited to draw images of “a person who works in mental health services,” followed by a series of questions and prompts related to their drawing. Next, they were invited to draw “a place where mental health care is delivered”; again, this was followed by a series of relevant questions. As recommended by McWhirter et al. (2004), participants were initially asked general questions about the person or the place in their drawing—what their professional role was, or where the place was located. Once it was apparent that participants were more comfortable in answering questions and had spent some time thinking about the topic, as recommended by McWhirter et al. (2004) the focus of the questions became more narrow; for example, participants were asked, “if a friend of yours needed to access mental health services, how would you feel about this person caring for them?.” These drawings were then used to facilitate discussion through an individual interview (participants’ drawings were not analyzed).
All interviews were conducted in a private room within the participant’s school by a male researcher (JG) and female colleague. Interviews were guided by a semi-structured interview guide, and audio recorded. The interview guide was reviewed following the first five interviews. We observed that the question “draw a mental health professional” resulted in participants drawing someone in professional attire and discussing professional attributes, and that we may have been influencing answers. The wording of this question was changed to “draw a person who works in mental health services.”
Data Analysis
It has been emphasized that, when analyzing participants’ drawings, the researchers should have a solid foundation in art interpretation (Thorne, 2016). As the researchers did not have the requisite skills, drawings were not subjected to analysis.
Interview data were analyzed using qualitative content analysis. This method was chosen as it facilitates investigation at both a manifest level (descriptive, or surface level content) and a latent level (interpretation of the underlying meaning) (Graneheim & Lundman, 2004). Interview data were transcribed verbatim. Transcripts were read numerous times in order to enhance immersion (Green et al., 2007). Transcripts were uploaded into NVivo version 11 and coded. In order to ensure rigor of the analysis, the co-authors worked with the first author in developing a deep understanding of the data (Adeagbo & Naidoo, 2021). Initial coding was conducted by the lead author. Codes were cross-checked by another member of the research team, and refinements made through a process of consensus. Codes were grouped into sub-categories and categories, before overall themes were identified (Graneheim & Lundman, 2004; Green et al., 2007). This process was completed by the lead author, with two members of the research team cross-checking at each stage, that is, forming of sub-categories, categories, and themes. Illustrative quotes and drawings from several participants are provided to enhance transferability and credibility (Munson et al., 2015).
Results
Three themes were identified from data analysis, which were: The Mental Health-Psychiatric Continuum (comprising the categories mental health issues and psychiatric issues, mental health care environments and psychiatric care environments, and mental health staff and psychiatric staff), Accessing Mental Health Services (comprising the categories the path to access and the cost of access), and The Delivery of Mental Health Care (comprising the categories types of mental health treatment and mental health staff). These theme titles were based on the “red thread” which were found running through several categories. This red thread brought meaning to recurring topics and experiences; essentially, the red thread was an expression of the latent content of the text (Graneheim et al., 2017).
The mental health-psychiatric continuum
Mental health issues and psychiatric issues
Participants described an intrinsic link between the experience of mental health issues and a diagnosis of depression, with no other illnesses mentioned. Mental health issues were viewed as existing within an affective domain or pertaining to one’s emotional status and were not perceived to affect other areas.
I think if you’re depressed, it’s like that you’re sad all the time (Grace)
Yeah, because obviously if you have mental health issues, then you’re upset (Colette)
It was suggested that, to relieve mental health issues, all someone would have to do was talk to others. Once a person’s issues had been disclosed, symptoms could be easily ameliorated, and the burden associated with them could be quickly reduced.
I think, like, once you tell someone something, you know, it just gets it off your chest in a second (Grace)
Just talking to someone about it. Talking to someone about mental health is a good thing, so. . . anyone who will listen: it’s a good thing (Colm)
Psychiatric issues were perceived as different to mental health issues. People experiencing psychiatric issues—such as schizophrenia—were regarded to have difficulties with how they perceived reality, lacked control, and were not responsible for their own actions, meaning they could be a danger to society.
It’s not anybody else like, it is you: it’s your mind that’s playing games with you (Colette)
you don’t know what you’re doing or anything like that (Connor)
And, like, psychiatric, [. . .] like, a danger to, like others, like, schizophrenia (Hilda)
It was suggested that a person’s mental health issues could be traced back to a “root cause.” One participant indicated that bullying, linked with the school environment was a cause of mental health issues. Another cause was abuse, linked with the home environment. These perceptions indicate that the triggers which result in mental health issues are considered to be multifarious.
They might’ve been bullied in school or something like that (Colette)
that could be why they have mental health issues, maybe there’s abuse in the home (Beatrice)
Participants spoke of psychiatric issues having different, more extreme, etiologies to mental health issues. These included congenital brain abnormalities, or severe trauma, such as “war” that resulted in irreparable psychological damage.
Like, ‘psychiatric,’ you could be born with (Eimear)
They’ve been through stuff, like, war or something. . . can’t get over what happened (Darragh)
Although mental health and psychiatric issues were perceived to be different terms, participants felt that they were connected. A person might initially experience mental health issues. However, should these issues persist, they could become more extreme, and ultimately develop into “psychiatric issues.”
I think they kinda like connect in a way [. . .] I think psychiatric would be, like, more severe than just mental illness (Hilda)
Psychiatric is more long-term and mental health can be short-term (Darragh)
Participants perceived these terms as existing along a “continuum,” based on extremity of symptoms, with less significant issues (“mental health issues”) at the lower end, and more extreme issues (“psychiatric issues”) at the higher end. Mental health and psychiatric were perceived as “different branches” of the “same tree.”
Well they’re all kinda the same—they’re under the same band like but, d’you know, there’s one way more extreme [. . .] Same tree, different branches (Denise)
They’re all in the same kinda like umbrella [. . .] like, it’s all still mental health but some of it’s a lot worse than others (Colm)
Mental health care environments and psychiatric care environments
Participants believed that mental health care was offered in offices. Offices were perceived to consist of a desk and chairs, typical of a traditional office environment. Here, people would engage with mental health staff in talk-based mental health care, in a welcoming, relaxing environment. Being comfortable was deemed paramount here, enabling people to feel more at ease, and thus more likely to engage with staff (see Figure 1).
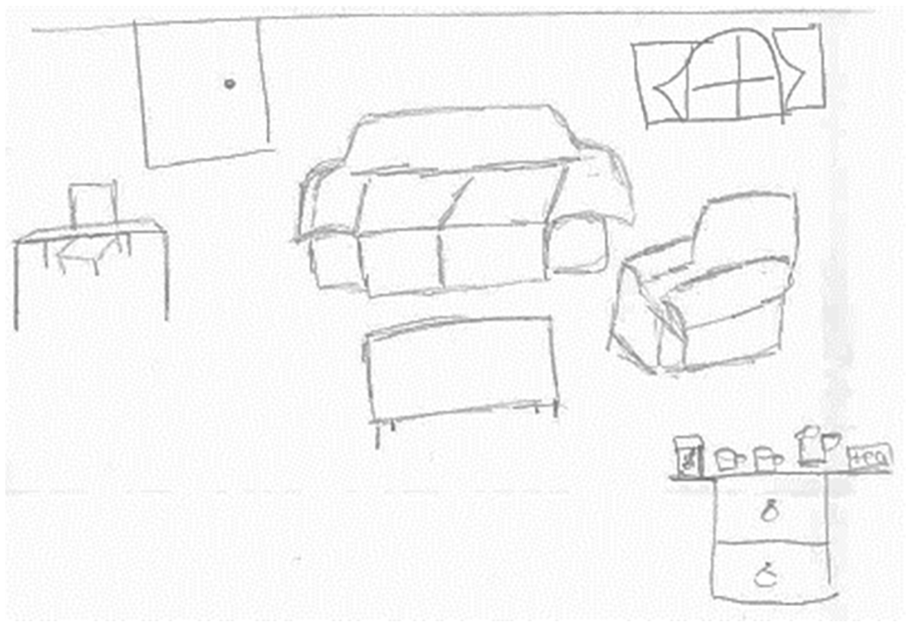
Emma’s drawing of a mental health care environment.
a really comfortable office, like, with really, like, warm tones of color, like, comfortable chairs and just a warm environment, so the person can come in and talk to her and just feel really comfortable (Millie)
It was also suggested that mental health care would be delivered in “hospital-like environments.” What set such environments apart from regular hospitals was the provision of rooms to facilitate counseling sessions.
I think it would look. . . um. . . kind of a bit like a hospital in a way, you know, and there’d be some beds, like, you know, for hospital people, but then there’d be, like, a lot of little rooms, just really small rooms so if you went, like, for counseling lessons (Grace)
Participants also spoke about psychiatric hospitals. People in these environments would experience difficulties considered more extreme than mental health issues and would require care from psychiatric staff, not mental health staff. Owing to the severity of psychiatric issues, longer-term care would need to be offered to people, with some individuals having to remain in care for years.
Not sure, just, kinda, like, a normal hospital but. . . just, different type of people working there, just more people are, that know about psychiatric. . . people (Darragh)
A psychiatric hospital is, like, for people who have to stay there for, like, long periods of time. [. . .] Like. . . um. . . a few months, or years (Eimear)
It was stated that, in the case where a person could not be rehabilitated in psychiatric hospitals, they would require care in an asylum. Asylums were perceived as providing more intense care to those for whom all other options had been exhausted. There was a sense of hopelessness associated with such care: once transferred to an asylum, it would be unlikely that people would ever be discharged again.
Asylum is [. . .] a word for a building where people who are typically labeled as insane go to spend the rest of their lives, or for the most part of their lives (Adam)
Well, maybe not in an asylum but that’s if it’s really, really bad. Like, that’s the end result if you cannot get better (Ingrid)
Psychiatric care environments were described like prisons. The rooms in asylums were referred to as “cells” which would house people considered to be dangerous. An emphasis was placed on the need for high levels of security, consisting of robust, impenetrable locking systems. In this regard, participants viewed psychiatric service users as dangerous individuals who would need to be locked away to protect society (see Figure 2).

Denise’s drawing of a psychiatric care environment.
eerily similar to that of prisons and cells in a way – very little comfort or very little happiness factor. It’s just cells with a bed and perhaps running water (Adam)
I presume there’d be, like, lock systems so it’d be harder to get in the doors in these, so there’d be kind of buzzers and things like that (Colette)
Mental health staff and psychiatric staff
Commonly cited mental health staff were therapists and counselors. It was suggested that such staff members would dress professionally, although there was also a casual element described here. This indicates that mental health staff were considered able to adopt an informal approach to care, while maintaining a professional appearance (see Figures 3 and 4).

Millie’s drawing of a mental health staff member (“mental health guider”).

Denise’s drawing of a mental health staff member (“psychologist”).
someone who’s, like, well-kept, like, they would wear a shirt and, like, jeans and with a belt and they have well-kept hair, and they just look professional (Anna)
Psychiatric services were perceived in more medical terms, with staff, such as nurses and doctors, wearing white clothes. Here, the difference between the staff in the perceived separate services is made explicit, with one side of the continuum (mental health services) reflecting a practitioner more associated with a casual approach to care, and the other side (psychiatric services) reflecting a practitioner associated with medical care.
I think psychiatric is more, like, nurses, doctors, like, things, like, that that look after people (Joan)
Yeah, just. . . usually wear white – the white jackets or something (Darragh)
they’d dress a lot more like the doctor that I was talking about. [. . .] White lab coat (Edward)
Accessing mental health care
The path to access
Participants commented that they would not feel comfortable disclosing mental health issues to informal sources, such as friends and family members. Furthermore, issues around confidentiality were highlighted in relation to school guidance counselors. Owing to a desire to maintain their privacy, it was suggested that accessing the formal mental health sources would be preferable.
If you don’t really want to admit to your family or friends about that, it’d be best to go there [formal source] first, ‘cause you know that it’s private (Barbara)
people could be really scared to go talk to the guidance counselor especially because [. . .] people are probably, like, “Why is she talking to the guidance counselor and what’s wrong with her?” So, again, that is a big struggle in the school (Millie)
Indeed, confidentiality was considered paramount for participants. There was confidence voiced in mental health service providers’ ability to maintain confidentiality,
Yeah, confidentiality, kind of, so people know that, like, once they go in there, their business isn’t gonna be, like, spread around, kind of. . . and if someone’s afraid to, like, talk because they don’t want other people finding out, like, they know that it won’t be said outside (Hilda)
However, participants generally communicated a lack of awareness about how to access such services.
I personally wouldn’t know where to go if I had to (Janet)
I wouldn’t know where to access it, really (Emma)
Some participants demonstrated an awareness that services could be accessed through general practitioners (GPs). Again, there was a lack of certainty here, with participants unable to state with conviction that GPs are gatekeepers to mental health services.
I’d say first, probably, like, go to their doctor and ask, tell them what’s happening; the doctor would tell them probably to go to someone who has more of an idea. That’s probably what I’d say (Denise)
The cost of access
Some participants perceived that accessing services was free. Although not all participants were certain that services were actually free, owing to the serious nature of mental health, it was recommended that there should be no cost associated with availing of mental health care.
I wouldn’t think that there would be a cost (Colette)
I don’t think there should be a cost because you shouldn’t pay money to help people with such a big, like, problem, so I don’t think there should be a cost (Millie)
Other participants commented that mental health care was expensive. They suggested that a person might have to spend a significant amount of money on care, particularly if their mental health issue escalated.
if you’re walking into, like, an office or into a hospital, then it’s probably gonna cost a lot more, like, probably even into the thousands if you’re in a bad situation (Colm)
I feel like it would be expensive. A couple grand, [. . .] like, 5/10 thousand (Leanne)
When the cost of care was perceived as being expensive, it was suggested that those in need of care may be deterred from accessing services. Of note, several participants commented that, owing to the cost of care, only affluent people would be able to engage with services. This indicates that mental health services were sometimes perceived as exclusive and would not cater for people from all socioeconomic groups.
Because, like, if they’re not very well-off, like, they wouldn’t be able to get their help and they wouldn’t get any better, like, they’d get worse (Barry)
The delivery of mental health care
Types of mental health treatment
Some participants spoke about medication; however, this form of treatment was not viewed favorably, nor was it considered to be frequently use, particularly with adolescents.
I don’t think I’d like someone my own age to be prescribed with drugs straightaway, um. . . but if you are, say, in your 40s or 50s and you have been dealing with it your whole life, then there is like a need for prescription drugs because that could be, like, their last resort (Janet)
Instead, participants considered that “talk therapy” would be commonly used within the services. This would involve discussing personal issues with staff, who would primarily investigate the “root causes” to mental health issues.
Maybe, trying to, like, see your past experiences, to see if there’s like a root to your problems maybe. . . and trying to help you come to terms with that (Colm)
Provision of advice was considered central to talk therapy, with staff devising solutions based on people’s personal situations. In the absence of advice—or where the “wrong” advice was given—participants suggested that there would be little point in engaging with mental health services.
if you give them the wrong advice, it’s kind of—it’s not really great for them, and they don’t gain from actually going to you. There’s no point in even going (Isla)
they’d want to be able to help that person as much as possible by leading them in the right direction and telling them where to go and what they can do and how they can solve their problems as well (Emma)
Mental health staff
It was suggested that mental health staff might begin their professional life in one area, and then pursue further education to work as a mental health practitioner. One participant commented that a “doctorate” would need to be awarded in order to practice in mental health. In this regard, the path to securing a position in mental health services was perceived as lengthy, and associated with a vast amount of study.
Maybe people who have studied in more depth than her, um. . . like higher degrees that could have. . . like the degrees to talk with someone in more detail than she would (Janet)
Probably, like, school [. . .] then college, like, going to—or university, a degree in. . . I don’t know, medicine. [. . .] They probably get like their doctorate or something and then go on and work with people (Oonagh)
Once a person had gained enough experience over time in mental health, they could consider pursuing further training and move to a career in psychiatric services.
if someone who works in the mental health office, if they wanna focus more, they could easily upgrade, go up into the [psychiatric services] (Joan)
Commonly cited staff members were therapists, counselors, and psychologists, all of whom would engage in talk therapy with people. This would involve the person lying back and discussing their issues. The staff member would explore their narrative, and attempt to make a link between their current situation and a memory from their past, one which they may have buried deep within their subconscious.
It’s, like, a therapist office, and there’s the therapist’s chair and the way where the person lies back and tells you about their problems (Deirdre)
I think that you’d be able to talk to the psychologist and they can try and help you with whatever mental health issue you have, by maybe, like, asking you about your past (Colm)
Psychiatrists were not often mentioned by participants, indicating a lack of familiarity with them. It was suggested that, unlike most other staff members, psychiatrists’ format of talk therapy involved a more face-to-face level of engagement. Psychiatrists were perceived as having a more active role in the therapy process than other staff members (see Figure 5).

Fionn’s drawing of a mental health staff member (psychiatrist).
Talk to the person face-to-face, try and see what they’re going through and try to help them through it [. . .] I’d say they just talk to them (Darragh)
Psychiatrist just talks [. . .] Like, the psychiatrists specialize in talking (Adrian)
The nurse’s role was perceived in the context of general health care, with a focus on the activities of daily living, such as attending to service users’ personal hygiene and ensuring that their nutritional/dietary needs were met.
Like, for food and stuff, ‘cause you obviously have to feed them. But then for, like, showering and stuff like that, then again, it depends what the people are or what’s wrong or. . . They just look after them, really (Ingrid)
Participants perceived nurses’ role in mental health care as limited. It was noted that people with mental health issues may engage in self-harming behaviors, and it would be the nurse’s role to attend to their physical health following such behaviors.
Say, if they did physical harm to themselves from mental health. Like, that’s where they’d come into play for this (Fionn)
Discussion
This study explored perceptions of mental health services from the perspectives of adolescents (aged 15 and 16) with no service experience. Mental distress can have a serious impact on adolescent development (Chu et al., 2018). The benefits of early intervention among adolescents are manifold: the prevention of mental distress, the promotion of recovery, and the development of resilience (Vusio et al., 2021). However, the lack of knowledge around mental health services combined with negative, stigmatizing attitudes demonstrated by adolescents in the current study indicate that early intervention may not always be realistic among this population, which may have effect their developmental needs. Consequently, the findings from the study have implications for how conversations around mental health need to evolve, and how barriers to care need to be addressed. It is known that adolescents lack knowledge about mental distress, which leads to stigma, and it has been recommended that education needs to be provided to this population group (Coles et al., 2016; Melas et al., 2013). The findings of the current study demonstrate that adolescents also lack knowledge about mental health services.
There was a difference in how adolescents understood the terms “mental health” and “psychiatric.” Adolescents commented on the difference between different illnesses, linking diagnoses such as depression with “mental health” and schizophrenia with “psychiatric”; the latter illness was associated with “danger.” The extant literature (e.g., Berry et al., 2020; Patel et al., 2018) has identified that illnesses such as depression and schizophrenia are perceived differently among the general public. However, it has not previously been reported that such illnesses would be catered for by different services. The findings from the current study contribute to the growing body of knowledge in this area, highlighting that “psychiatric” is another term in use amongst adolescents, related to mental distress, but bringing with it negative connotations. Future initiatives aimed at stigma reduction—such as school education programs and media campaigns—should explain terms such as “psychiatric”; otherwise, we run the risk of reserving residual stigma in our social discourses and fostering poor help-seeking behaviors.
Barriers to seeking help from informal sources, such as friends and family, were also reported. While adolescents demonstrated a preference for informal sources of help over formal mental health services, they also voiced reluctance to address the experience of mental distress with friends and family. Previous research, using quantitative cross-sectional survey approaches, have found that, among the general public, including adolescents (aged 14–19), there is a statistically significant preference for informal sources over formal sources (Carleton et al., 2020; Lubman et al., 2017; Melas et al., 2013; Ojio et al., 2015; Suka et al., 2016;). However, it could be argued that “preference for informal sources” may not be tantamount to “willingness to engage with informal sources.” Given the important role informal supports play in how people manage mental distress, with engagement with family members and friends often minimizing the need for accessing formal mental health services (Chen, Xu et al., 2019; Martinez et al., 2020), further research is warranted to explore barriers to accessing informal sources of help.
It was evident that adolescents lacked knowledge about how to access mental health services, a finding which corresponds with previous research with adolescents aged 12 to 18 (Clark et al., 2018), university students (mean age: 20) (Czyz et al., 2013), and young adults aged 18 to 25 (Salaheddin & Mason, 2016). Although the aforesaid research is based on hypothetical scenarios, Cadigan et al. (2019) reported that poor knowledge about accessing services resulted in over a third of young adults delaying seeking help for mental distress, indicating that uncertainty and lack of knowledge do indeed influence delays in help-seeking. Following a stigma reduction educational intervention conducted by Chisholm et al. (2016), adolescents (aged 12–13) highlighted deficits in their knowledge about accessing services. For example, one participant in their study requested “[m]ore on what you could do if you like did have mental illness [. . .] they didn’t really tell us anything else that we could do” (p. 9). Mental health education initiatives aimed at adolescents should incorporate information around accessing services so that help-seeking and service engagement can be enhanced. Otherwise, considering the uncertainty about how to access services expressed in the current study, adolescents may be unable to make appropriate decisions about help-seeking and contact with services may be delayed or obstructed.
There was uncertainty also communicated about the cost of accessing services, with responses ranging from “free” to “expensive.” In instances where accessing services was perceived as expensive, participants suggested this would be a barrier to seeking help. Salaheddin and Mason (2016) found that almost 67% of young people from the general public would consider the cost of care as a barrier to accessing mental health services. Similarly, Iskra et al. (2018) found that the cost of care was cited as a barrier to accessing child and adolescent services (despite this service being free in Australia, where this study was conducted). In most developed countries, governments usually fund mental health services, whether or not other health sectors are publicly or privately funded (Perera et al., 2018). However, there are countries where mental health care may be unaffordable for its citizens (Choudhry et al., 2021). In order to increase the chances of young people accessing care, accurate, country-specific information regarding the cost of care needs to be disseminated.
In relation to mental health care, while participants demonstrated negative attitudes toward medication, they perceived talk therapy positively, provided that such therapy involved staff members offering advice. Arora and Algios (2019) reported that adolescents (aged 14–20) were ambivalent about some mental health supports, owing to their perceptions that staff would deal with problems superficially (they would “just say something to make you feel better” [p. 172]), meaning the “problem is not solved” (p. 172). It is clear that provision of “advice” is paramount to adolescents. Further research around adolescents’ perceptions of talking therapies is warranted, including their expectations of these therapies, with the aim of enhancing engagement upon access.
Psychiatrists were the staff members participants considered most associated with talk therapy while nurses were associated with a more medical model of care. Prescription of medication is standard practice for psychiatrists (Yeisen et al., 2019); conversely, mental health nursing has aimed to move beyond a medical model of care and develop a more holistic approach (Goodwin et al., 2020). It is important that adolescents considering accessing mental health services are more informed about the role of psychiatrists in their care; otherwise, dissatisfaction with and disengagement from treatment may occur.
The road to becoming a mental health practitioner was perceived as protracted and associated with a vast amount of study. Although previous research has identified a link between perceived time spent in university and career goals, adolescents often demonstrate a preference for a more expedited university experience, stating they “just want the degree and to finish as soon as possible” (Willis, 2005, p. 36) or they “just want the end result. [They] just want the degree” (Kahu & Picton, 2020). Globally, people working in mental health report that staff shortages are a cause for concern in professions such as nursing and psychiatry (Barrett & Twycross, 2020; Jansen & Venter, 2015; Katschnig, 2010; Sobekwa & Arunachallam, 2015; Verduin, 2017). Given their preference for an expedited university experience, adolescents may be unlikely to pursue a career in mental health services, which may contribute to future staff shortages. Considering the global issue of mental health staff shortages, the perception of protracted university courses should be challenged, and adolescents should be provided with more information about career pathways of staff. Such information may be best provided through career guidance counselors or at university open days.
Limitations
It is important for the researcher to position themselves, and to demonstrate transparency regarding the impact of this position on the study (Levitt et al., 2018). Despite putting participants at ease using a relaxed, friendly demeanor, the researchers’ position as “outsiders” may have influenced how participants spoke about mental health services, in the sense that they may have been covertly uncomfortable conversing on this topic. Furthermore, the authors acknowledge their familiarity with mental health services. Because of this, we may have made assumptions that some topics suggested by participants matched the topics with which we are familiar, and for this reason, it is possible that certain areas were underexplored.
Males were unrepresented in the study when compared with their female counterparts, thus limiting transferability. However, it should be noted that it is common for males not to take part in research in general (Kazlauskaite & Fife, 2021) and in mental health research in particular (Gagnon et al., 2017; Goodwin, Behan et al., 2016). Furthermore, it should be acknowledged that all participants identified as White. While this represents the majority of residents in Ireland (82.2%) (Central Statistics Office, 2016), it should be acknowledged that transferability would be increased with a more diverse sample (Kazlauskaite & Fife, 2021). Another limitation is that participants’ drawings were not subjected to analysis. Such an approach may have yielded further interpretive insights. Additionally, other insights may have been facilitated through the use of another analysis technique. For example, a discourse analysis approach could have been used to investigate how adolescents discussed concepts associated with services, and this is certainly an area for future consideration. Finally, although coding of data was cross-checked within the team, rigor would have been enhanced—and bias reduced—through independent coding (Becher et al., 2021).
Conclusion
Internationally, efforts are being made to educate adolescents more about mental distress (Chisholm et al., 2016; Mental Health Ireland, 2021). However, this population hold stigmatizing perceptions of mental health services and are uncertain about how these services operate, and so, education around services is also warranted. It is expected that provision of education in this area would enhance service delivery, improve adolescents’ help-seeking behaviors for mental distress, and reduce stigma. Such education could also demystify the role of mental health staff and may enhance service recruitment at a time when staffing shortages are a major service concern. It is recommended that adolescents’ perceptions of treatments used in mental health services are further explored, so that services can offer adolescent service users more appropriate care, in addition to promoting an image of mental health care that is more attractive to this age group. The current study focused on adolescent populations; further research is warranted to explore all members of the general public’s perceptions of mental health services, such as younger children and adults. Finally, we recommend that the current study is replicated with adolescents in resource-constrained contexts to determine the transferability of our findings outside of developed countries.
Footnotes
Acknowledgements
We wish to thank Dr Stephen K Bradley for his contributions to the design of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.