
Abstract
The media portrayal of sports concussion (SC) contributes to community understanding of injury. However, this could be hampered by inaccurately framed (minimising) SC coverage. 157 volunteers were randomly allocated to one of six online survey conditions. The conditions used a brief written news sports report with a non-serious (MI) or serious (MA) SC frame. Additional conditions varied the injured player’s sex (male or female) or the sport (unnamed or basketball). Standardised measures were administered, including the Illness Perceptions Questionnaire-Revised, and a custom-measure of perceptions of SC seriousness (SISI). A series of one-way ANOVA’s revealed one statistically significant framing effect for the SISI (p < .05, large effect). Post-hoc pairwise comparisons found higher SISI scores for MA compared to MI conditions. There was no difference in the player sex or sport variants. No differences were found on other outcome measures. This study replicated a MA versus MI framing effect on the SISI, however wider effects were not seen. The framing effect on community perceptions of SC may be more circumscribed than previously suggested. While this requires further investigation, minimising frames should still be avoided as per existing recommendations.
Keywords
Introduction
Mild traumatic brain injury (mTBI) is a major health problem internationally (Maas et al., 2022; Yue et al., 2023), with estimates ranging from 476 to 1153 cases per 100000 individuals annually (Maas et al., 2022). The actual case number is probably higher than estimated because concussion is under-reported (Craig et al., 2020), and this has spurred efforts to this situation (Kroshus et al., 2017). MTBI leads to acute adverse effects including debilitating symptoms such as headache, dizziness, confusion, and disorientation. These symptoms impact daily living, can persist over time, and can be compounded by poor management (Cancelliere et al., 2022; Fordal et al., 2022; Gaudette et al., 2022). A mTBI can have many causes including collision sport (e.g., rugby, ice hockey), sports with a high falls risk (e.g., equestrian sports), and sports where objects (such as balls) can collide with a player’s body or head (e.g., soccer, volleyball).
Many factors contribute to outcomes from sport-related mTBI (hereafter, sport concussion [SC]) including if players, spectators, and officials recognise, report, and manage the injury. The likelihood of such actions depends on many factors, including people’s injury perceptions (e.g., it’s perceived seriousness) (Craig et al., 2020). Compared to professional sport, in amateur and junior competition the parents of junior players and community supporters play a particularly important role in concussion identification (Elkington et al., 2019). This understanding has led to calls from sports authorities to improve community awareness about concussion, especially its perceived seriousness (Elkington et al., 2019). These efforts must be sufficient to overcome concussion messaging from sources that have historically downplayed seriousness, including the media (Jeckell et al., 2024).
The public’s use of the media for concussion information is well-documented (Jeckell et al., 2024); however, reporting accuracy has been strongly critiqued from a health perspective. For example, a published research review of 153 online SC news articles found they contained inaccurate terminology (e.g., head vs. brain injury) effectively downplaying seriousness (Ahmed & Hall, 2017), and that the cultural messaging could influence or reinforce poor health decisions by players (e.g., describing a player as “lionhearted” if competing whilst injured) (Ahmed et al., 2016). Similar conclusions were reached in the analyses of auditory-visual materials from online sources (Williams et al., 2014), televised sport (Ku et al., 2020), ‘action’ films (Aitken et al., 2016), and other online news reports (Schwartz, 2017; Townsend, 2021). Most of these studies show that concussion is not depicted or described accurately from a health perspective, and its seriousness is downplayed. This research implies but does not show a negative effect of such reporting on community understanding of SC, even though this could be empirically tested.
To date, two empirical studies have shown the potential for the sports media to influence SC identification (Ku et al., 2020), and perceptions of injury seriousness (Schwartz, 2017). The study by Ku et al. with >800 participants showed that concussion recognition among members of the public could be improved with supplemented media commentary (adding information to actual reports about what happened to the player in the moments after the injury, and whether they stayed in play, were rested then returned, or were removed from the game). The Schwartz study with 55 participants showed that the injury framing from actual media reports (Heim, 2016; Hill, 2016) altered perceptions of injury seriousness. While both studies would clearly benefit from independent replication given their importance in bridging the gap between implied and direct effects of SC media exposure, there are notable differences between them, including that the study by Ku et al. (2020) was a published international collaboration, whereas the study by Schwartz (2017) was not published except as a dissertation.
Schwartz used framing theory to explain how the media could influence community views of SC (Schwartz, 2017). According to this theory, the meaning drawn from media communications is changed by factors such as the selection of content and choice of terminology (Reese, Gandy, 2001; Chong & Druckman, 2007; Bullock & Shulman, 2021). In Schwartz’s experiment, two frames were selected from existing sports news articles: one with SC framed as “more serious” (major [MA] injury frame) where, for example, the coach/player quote says extended time out from sport is needed, versus “less serious” (minor [MI injury frame) where the quotation implies minimal time out. The Schwartz study found a frame effect on perceived SC seriousness. However, this effect was observed on a custom-built scale (seriousness index, p. 31), as opposed to an established measure. Although the Schwartz study suggests that actual media reporting of SC (specifically, framing) affects perceptions of injury seriousness, and it appears to be the only study to have done so to date. A replication and extension of Schwartz (2017) is required to address some of these concerns.
In summary, the literature shows that SC is a significant health issue, and its correct management relies on community awareness of SC, especially at amateur and junior sports levels. Previous studies indicate that the media portrayal of SC can be inaccurate, especially downplaying injury seriousness. Crucially, there are indications from a very small number of mixed quality studies to suggest that this portrayal influences community understanding and perceptions of SC in ways that could impact its correct management. Since community members use the media for information about SC (Jeckell et al., 2024), and the community contributes to injury identifcation (Elkington et al., 2019), it is vital to establish how the media portrayal of SC impacts community views of SC. The limited past research suggests that both the content (Ku et al., 2020) and framing (Schwartz, 2017) of SC media reports could be important for such ends, but further research is needed. Therefore, the present study aimed to (a) replicate the findings of Schwartz (2017) to determine if the same framing manipulation (MI vs. MA) alters perceptions of SC seriousness, and; (b) extend Schwartz (2017) to determine if the frame effects are measurable on an established measure of perceived injury seriousness and other variables important for injury management, for example, injury reporting intentions and the proposed behavioural response to injury (whether to limit usual activities).
Materials and Methods
Participants
This study was a component of a larger SC study. An initial pool of 182 adults (aged ≥18 years) completed the study. The participants were recruited via a range of methods including word of mouth, electronic communications, and advertisement to a first-year psychology research participation pool. An eligibility requirement was valid completion of at least 50% of the survey. Twenty-five records failed this requirement primarily because of missing data (>50% missing data, n = 21). Four people did not pass a validity check (see Method), leaving a sample of 157 respondents.
Measures
The Schwartz injury severity index (SISI)
Schwartz, (2017) The SISI is a four-item scale assessing the perceived seriousness of an SC. An example SISI item is: How is the injury to [the player] portrayed…? For this study, the item response scale was reversed for consistency with other measures (i.e., 1 = not at all important to 5 = extremely important). Minor item changes were made (e.g., replacing “head trauma/concussions” with “concussion” and replacing “article” with “news report”). The total score is the sum of responses, with higher score indicating SC was perceived as more seriousness. The internal consistency for this and all other scales is shown in Table 2. The SISI had acceptable reliability (α = 82 cf Schwartz (2017) α = 75).
Behavioural responses to illness questionnaire (BRIQ)
Spence et al., (2005) The BRIQ is a 19-item questionnaire assessing the frequency of behavioural responses to illness. The BRIQ has four subscales, including the 7-item “limiting behaviours” (LB) subscale. This study used the LB subscale. The LB subscale has items such as: “I would put parts of my life on hold [because of illness].” Each item is evaluated using a 5-point Likert scale from 1 (not at all) to 5 (every day). Minor modifications were made to the LB scale (e.g., my life changed to their life; illness changed to injury, normal changed to usual), and a modified instruction was employed (e.g., In the week following the injury, how often should the athlete…[put parts of their life on hold]). A total score is the sum of item responses (possible score range: 7–35). Higher scores indicate a higher frequency of limiting behaviours following injury.
Illness Perceptions Questionnaire-Revised (IPQ-R)
Moss-Morris et al., (2002) The IPQ-R is a measure of illness perceptions originally based on the Leventhal’s Self-Regulatory Model (Leventhal et al., 1980, 1992, 1997). The IPQ-R has previously been used in studies of mild mTBI (Whittaker et al., 2007). The IPQ-R has 7 subscales, four of which were used in this study. Each subscale has ≥6 items. A sample IPQ-R acute-chronic subscale item is: my illness will last a short time. Agreement with IPQ-R items is rated on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Minor changes to item wording were used (e.g., the word injury replaced the word illness). The following subscales were measured: the perceived acute-chronic timeline [IPQ-R-Timeline] and consequences of the injury [IPQ-R-Consequences], where higher scores indicate greater perceived chronicity and seriousness, respectively; and the perceived personal or treatment controllability of the injury [IPQ-R-Personal Control, IPQ-R-Treatment Control], where higher scores indicate a greater perception of control over the injury, via one’s personal actions or available treatments, respectively. The IPQ-R was scored as per standard instructions, including item reversal as required.
Expected concussion reporting behaviour (CR-E)
Kroshus et al., (2021) The CR-E is a relatively new 4-item measure of expected youth athlete concussion reporting behaviour, with excellent psychometric properties (Kroshus et al., 2021). This measure was recommended over Kroshus and colleagues’ previous, widely-used, one-item measure of concussion reporting intention (Kroshus et al., 2021). The CR-E assesses how often a person would report a SC if symptomatic under 4 specific circumstances (e.g. even if I really wanted to keep playing). Responses are recorded on a 5-point Likert scale (1 = never to 5 = always). Minor modifications of this scale were made for this study, including removing personal references (e.g., “I”) and using a modified instruction (e.g., If the athlete felt dizzy after the injury, they should tell their coach right away… even if they really wanted to keep playing).
Protocol Validity Score
As per precedent and recommendations (e.g., Oppenheimer et al., 2009; Rosenbaum & Arnett, 2010), selected survey items were deployed to check response authenticity. Such checks are increasingly recognised as vital for the integrity of online data collection (e.g., Griffin et al., 2022; Wang et al., 2023). A protocol validity score was calculated from the responses to five custom items designed for this study, and three existing items from a full administration of the Rosenbaum Concussion Knowledge and Attitudes Scale [RoCKAS] (Rosenbaum & Arnett, 2010) (other RoCKAS data not reported). The three RoCKAS items constitute an inbuilt “validity scale [VS]” (Rosenbaum & Arnett, 2010). The VS items were empirically-derived and represent items that are very rarely answered incorrectly (Rosenbaum & Arnett, 2010). To supplement the RoCKAS-embedded VS items, five custom items were deployed elsewhere in the survey. These items comprised two “news report recall” [NRR] multiple-choice items (to check correct recall of key details from the news reports; e.g., What was the injury in the news report?), and three instructional manipulation check [IMC] items (Oppenheimer et al., 2009), where the respondent is told which answer to give (e.g., select “not often”]) and the failure to give the instructed response is taken as low response quality (or the potential for invalidity). A VS score of at least two out of three is usually required to establish profile validity (Rosenbaum & Arnett, 2010). This threshold was employed in this study, together with the requirement of at least one correct NRR response, and at least two correct IMC responses.
Injury Frames
Frame Condition Stimuli. The MI and MA Frames With the “-M” Extension Refer to a Male Athlete (he/his) who is Concussed in an Unnamed Sport. Variants Were Created by Changing the Athlete Pronouns to She/her (-F [or Female Athlete] Condition) or Naming the Sport (-B [or Basketball] Condition).
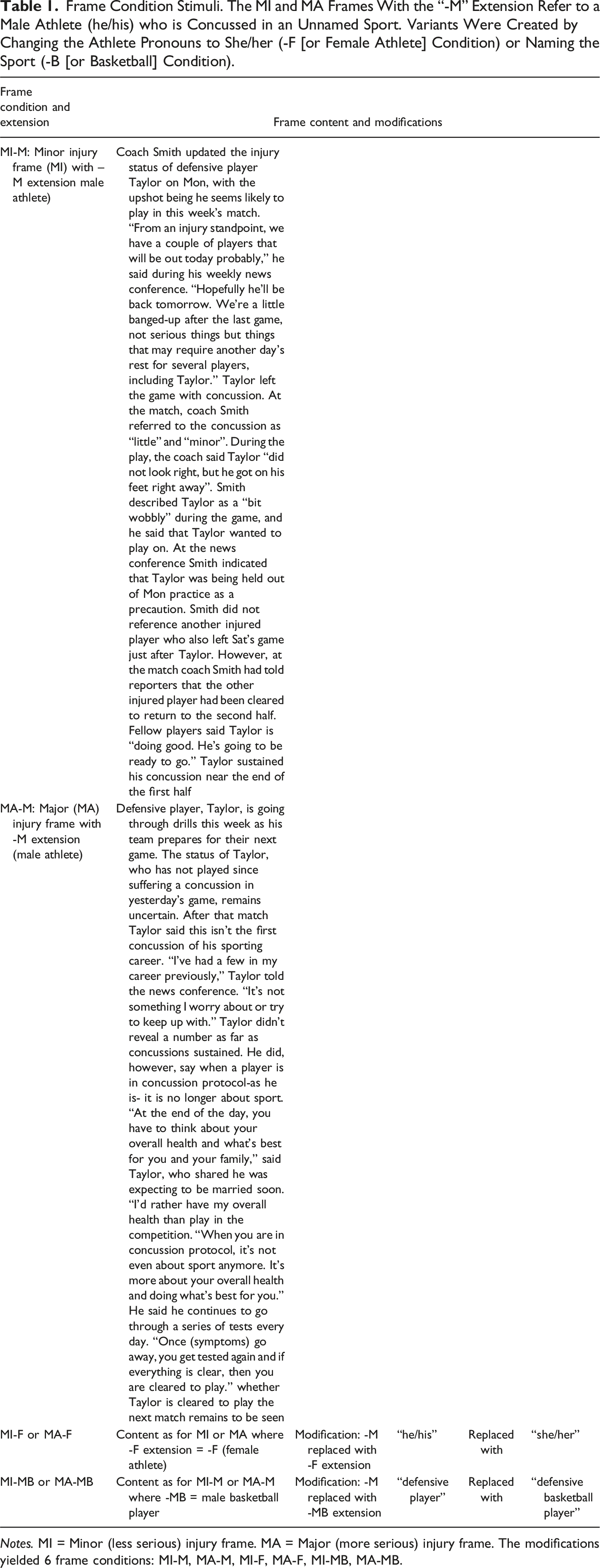
Notes. MI = Minor (less serious) injury frame. MA = Major (more serious) injury frame. The modifications yielded 6 frame conditions: MI-M, MA-M, MI-F, MA-F, MI-MB, MA-MB.
Procedure
This study was approved by the University’s Human Research Ethics Committee [approval no.: 5567]. An online survey delivery platform was used (Qualtrics, 2022 [CoreXM, Commercial Use]). The recruitment materials with information about the online survey were disseminated. Interested participants entered the study (e.g., clicking an embedded link, scanning a QR code, or via URL). They saw additional study information and registered their decision about participation via a yes or no radio-button. Non-consenting persons were thanked for their interest and exited. Consenting participants continued the study. They were asked preliminary questions, then were randomly allocated to one of the six frame conditions. After reading a ‘short news report’ (frame), they completed the measures, one for the replication objective (the SISI), and the remainder for the extension objective. The survey included some open-ended (free-text) items (e.g., List three things you would recommend to someone who has just had a concussion to help with their recovery), and demographic questions. To conclude the survey, the participants chose to exit the survey directly, or to exit the survey after providing their contact information (separately stored) for token administration and/or to receive a summary of the study results. Two tokens of thanks were offered (i.e., prize draw entry to win a small gift voucher, or the awarding of a small amount of academic course credit if applicable).
Data Analysis
Descriptive statistics were calculated for the demographic variables and measures. The internal consistency for each measure was derived (Cronbach’s alpha) and interpreted using established guidelines (Boateng et al., 2018). Levene’s test for equality of variance was checked and, in most cases, this assumption was met. Where this assumption was not met, the reported values do not assume equality of variance. A series of one-way ANOVAs were run to test for an effect of the six framing conditions on the outcomes. Statistical significance and effect size (ŋ2) (Lakens, 2013) was evaluated as per convention (i.e. p > .05).
Results
The sample characteristics have been reported previously. Briefly, the average age of participants was approximately 28 years (range = 18–69 years). Most (75%) participants were women and born in Australia. The sample included people with (n = 44) and without (n = 113) a self-reported concussion history, a third of which were due to sport (34%). There was no significant difference in outcome measures due to participant sex or concussion history (all p’s > .05), with the exception that people with a concussion history scored higher on average on two IPQ-R subscales (timeline and consequences) than people with no prior injury.
Descriptive Statistics and Condition Comparisons
Frame Condition Stimuli. The MI and MA Frames With the “-M” Extension Refer to a Male Athlete (he/his) who is Concussed in an Unnamed Sport. Variants Were Created by Changing the Athlete Pronouns to She/her (-F [or Female Athlete] Condition) or Naming the Sport (-B [or Basketball] Condition).
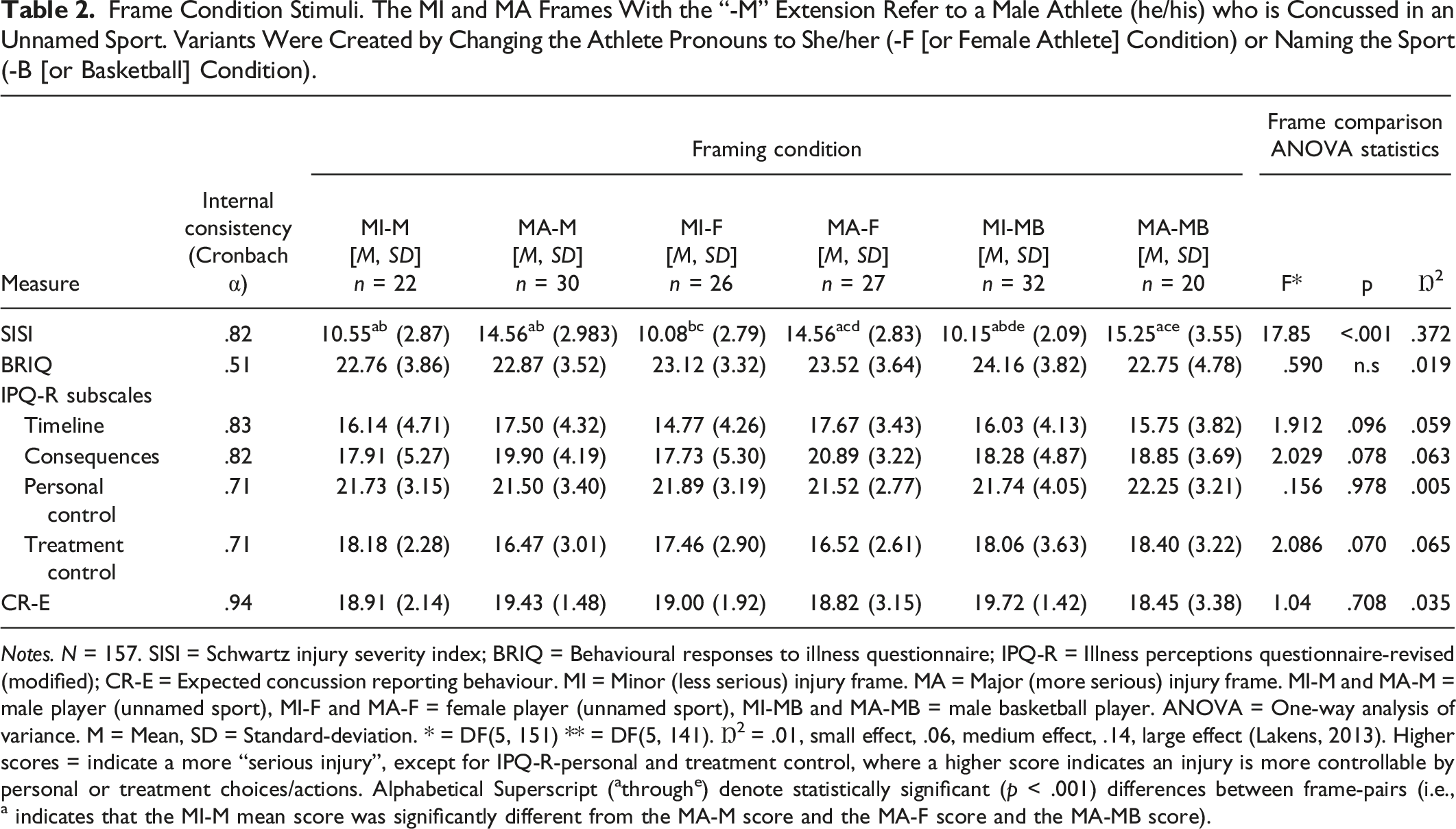
Notes. N = 157. SISI = Schwartz injury severity index; BRIQ = Behavioural responses to illness questionnaire; IPQ-R = Illness perceptions questionnaire-revised (modified); CR-E = Expected concussion reporting behaviour. MI = Minor (less serious) injury frame. MA = Major (more serious) injury frame. MI-M and MA-M = male player (unnamed sport), MI-F and MA-F = female player (unnamed sport), MI-MB and MA-MB = male basketball player. ANOVA = One-way analysis of variance. M = Mean, SD = Standard-deviation. * = DF(5, 151) ** = DF(5, 141). Ŋ2 = .01, small effect, .06, medium effect, .14, large effect (Lakens, 2013). Higher scores = indicate a more “serious injury”, except for IPQ-R-personal and treatment control, where a higher score indicates an injury is more controllable by personal or treatment choices/actions. Alphabetical Superscript (athroughe) denote statistically significant (p < .001) differences between frame-pairs (i.e., a indicates that the MI-M mean score was significantly different from the MA-M score and the MA-F score and the MA-MB score).
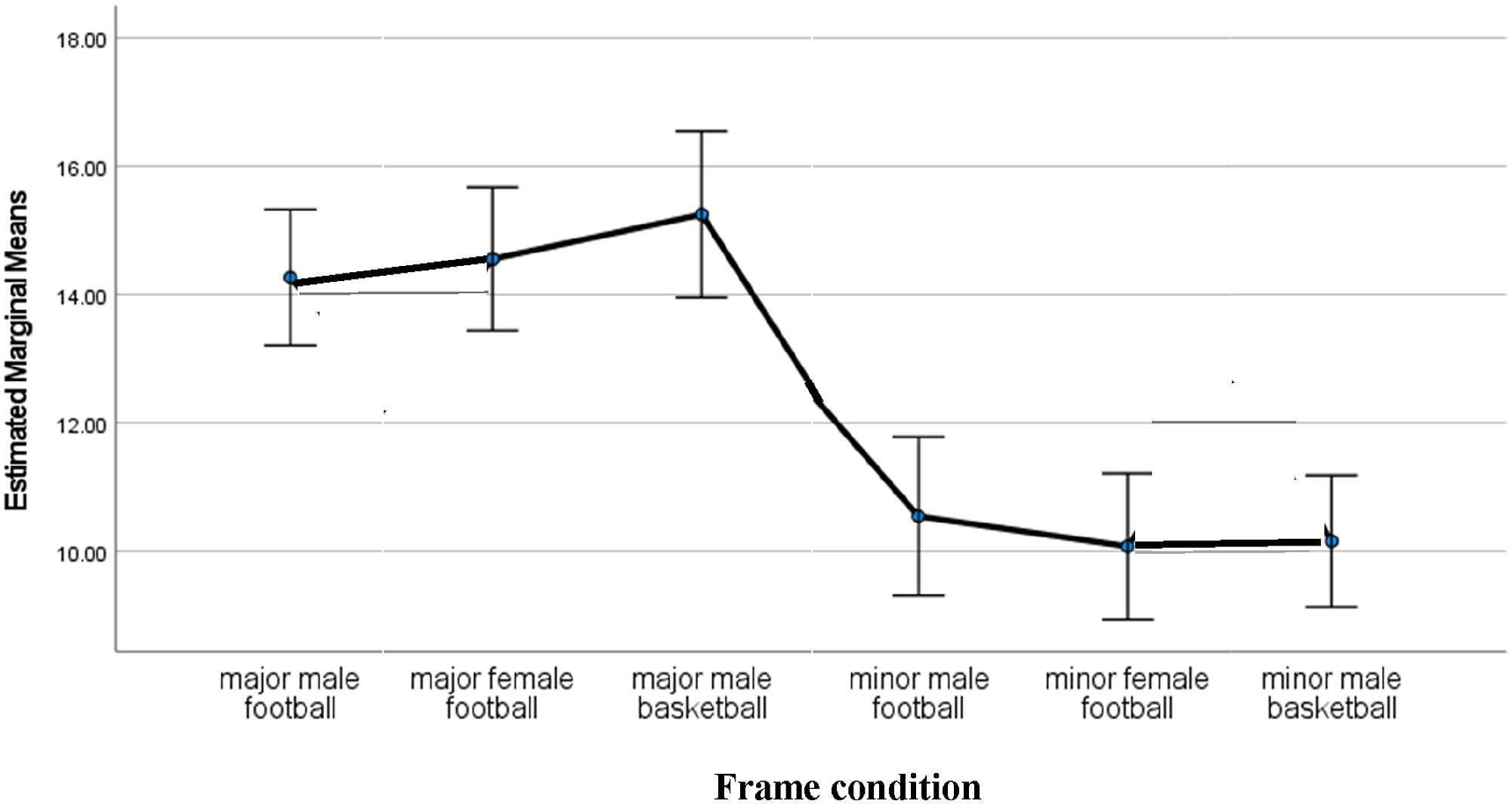
Estimated marginal means for SISI total score by frame condition with 95% standard error bars.
Discussion
The public utilises the media for SC information (Jeckell et al., 2024) necessitating an understanding of how this information affects community perceptions of SC. The limited available research suggests that this portrayal affects the ability to recognise SC (Ku et al., 2020) and perceptions of its seriousness (Schwartz, 2017). The present study aimed to replicate and extend the findings of Schwartz (2017). The extension aimed to determine if frame effects would be found on an established measure of injury seriousness (IPQ-R-consequences) and other measures relevant to SC, such as injury reporting (CR-E) and limiting behaviours (BRIQ).
This study successfully replicated Schwartz’s (2017) finding of a media frame effect on the perceived seriousness of SC (SISI). As Schwartz found, the media portrayal of SC, when constructed with a minor vs. major injury frame, led to significantly lower vs. higher SISI ratings, respectively. Schwartz found this effect using two frame conditions for one sport played by a male sportsperson. The present study found this effect using an expanded set of six conditions, and the frame effect held despite variations in: (a) the depicted sport (unnamed vs. basketball) and (b) the injured player’s sex (female vs. male).
A second aim of the present study was to extend the study by Schwartz (2017) to explore the wider effects, if any, of the media portrayal (framing) of SC. This included using an established measure of perceived injury seriousness (to confirm the SISI effects), and other variables important for concussion outcomes, such as if an injury occurred, whether the injured person would report their injury to someone (e.g., coach). The present study did not find a framing effect on an established measure of injury seriousness (IPQ-R consequences). The framing of SC as a minor versus major injury did not lead to significant differences in the mean IPQ-R consequence score, which measures perceptions of injury consequences, across the six conditions. In other words, when people read a brief news report about SC, then reported if SC has serious consequences, their perceptions were not changed by the report’s contents, specifically if it minimised or portrayed SC as serious. This result was unexpected because of the SISI finding. This difference does not appear to be due to the reliability of the scales since both scales had acceptable internal consistency. However, on closer inspection a possible explanation could be differences in the item content (validity) of these scales. The SISI items appear to assess the respondents’ perception of how the article’s author or character views the importance of SC (e.g., does the coach view SC as serious), whereas the IPQ-R consequence items assess their views about the injury itself (e.g., is the athlete’s injury a “serious condition”).
A further study objective was to determine any wider effects on perceptions of SC of variations in the brief news reports, but these effects were not found. One reason for expecting wider effects was Ku and colleagues’ (2020) finding that public concussion recognition was improved by supplemented media reporting. On closer inspection, the supplementation in Ku et al. (2020) involved showing participants a written statement about the player’s fate (i.e., adding typed text to a screen with SC vision and commentary). Ku et al. (2020) acknowledged that the improved injury recognition could have been due to the supplemented message per se, which was not integrated with the reporting. In the present study, an integrated message was used, and no effect of frame (news report) variation was seen on wider measures. Thus, although the results of the present study suggest that the SC media framing did not impact these wider variables, this is a tentative conclusion.
This study has several limitations. First, this study had a relatively small sample. Whilst this was sufficient to detect the large effect on the SISI measure, it might have been too small (insufficiently powered) to detect other effects. To investigate this, future studies could recruit more participants, use fewer conditions, or both. Second, a convenience sample was used with the effect that the resulting participant pool is not representative of the community. While this approach mirrors that of Schwartz (2017) and others (e.g., Ku et al., 2020), future studies must recruit a truly representative sample. Third, the characterisation of SC as “minor” is recognised as inconsistent with best practice, according to the health-information oriented media guidelines (Ahmed & Hall, 2017). Although this practice appears to remain widespread (Jeckell et al., 2024), the guidelines explicitly warn against terms such as “minor” concussion. This study was about SC only and the results may not generalise to concussion from other causes. Finally, this study investigated the effect on community beliefs about SC following exposure to one form of media communication (a written report), and the findings may not generalise to other media, including televised or visual media, which could be more potent because of mixed modality messaging (auditory-visual).
In conclusion, this study provides support for a previously unpublished finding that the media framing of SC effects perceptions about it. However, a more qualified conclusion is advised based on the present study, since this effect appears to be specific to perceptions about the frame, as opposed to SC per se. In other words, the participants recognised the framing of the injury as serious to the news report’s author or other people in the story (such as the injured athelete). Overall, it can be cautiously concluded that this study suggests a more limited or circumscribed impact on public understanding of SC arising from the media portrayal than previously suggested, although this requires further testing. Despite this, reporters should avoid MI framing as this has already been recommended (Ahmed & Hall, 2017) and the potential for harm via public misinformation cannot be ruled out. These potential harms should be further investigated to build a body of research that will clarify how the media affects community perceptions of SC, and if can be harnessed to improved injury prevention and management.
Footnotes
Acknowledgments
The author/s thank the volunteers who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The author/s assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. This study was approved by the University’s Human Research Ethics Committee [approval number: 5567].
Data Availability Statement
The data that support this study will be shared upon reasonable request to the corresponding author.*