
Abstract
Objectives:
To determine the predictors of knowledge and awareness of concussion symptoms and outcomes through a survey of athletes, parents of players and coaches in sports settings in Canada.
Methods:
A cross-sectional survey of athletic communities in Canada was conducted. Respondents’ concussion knowledge score consists of responses to questions about the symptoms, diagnosis, and treatment of a concussion and the timing of return-to-sport post-concussion. The percentage of correct responses was defined as the “identification rate.” The extent to which participant factors affected the scores was examined by univariate and multivariate analyses.
Results:
Respondents were able to identify a mean of 80.6% of symptoms. Cognitive symptoms were most commonly known, and mental health symptoms associated with concussion were least known, and health professionals, coaches, and those with a personal history of concussion had the highest levels of overall knowledge. Language, age, educational level, annual household income, and traumatic brain injury history were good predictors of better concussion knowledge.
Conclusion:
Those designing and implementing interventions aimed at concussion management and prevention should ensure that younger, lower income, lower educational, non-English-speaking persons, and those without experience of traumatic brain injury or concussion be specifically accounted for in the design and implementation of interventions to prevent and treat concussion and mild traumatic brain injury.
Introduction
Traumatic brain injury (TBI) affects up to 3.8 million people in the United States annually and is a major source of disability.1–5 Annually, over 300,000 people suffer sports-related concussions in the United States and those between the ages of 15–24 years are most commonly affected.6,7 In total, 75%–90% of all TBIs are classified as mild traumatic brain injury (mTBI),8–10 and while most mTBI symptoms typically resolve within 3–10 days, approximately 20%–30% of patients will continue to experience persisting cognitive, physical, mental, or emotional symptoms at 6 months post mTBI.11–19
However, it is important to note that recognizing the symptoms of concussion is imperative in making decisions regarding diagnosis, treatment, and prevention of concussion. Programs aimed to limit repeated concussion, particularly before recovery from an initial concussion, like return-to-play and return-to-work are all based on the provision of an accurate knowledge of the history of concussion symptoms by the patient to a doctor or another person such as a coach or an athletic trainer. As such, recognizing and understanding the symptoms of concussion is paramount for accurate patient management and for the prevention of future events. A previous study that examined football players’ concussion awareness showed that 70.4% of the studied football players experienced at least one concussion, but only 23.4% of them realized the symptoms they experienced represented a concussion.6,20 Our prior research showed roughly one-quarter of adults and 25%–50% of children in a hockey league could not recall any symptoms or recalled only one symptom of a concussion. Moreover, almost half of the players and a fifth of the adults incorrectly stated that concussion was treated with medication or physical therapy and nearly one-quarter of all players did not know if an athlete experiencing symptoms of concussion should continue playing. 21 Indeed the extent to which the lack of concussion knowledge hinders proper treatment has been clearly highlighted by others. 22 In addition to compromising treatment, a lack of injury prevention knowledge and related factors including misconceptions, distorted perceived susceptibility, downplayed perceived severity, and miscommunicated cues to action as defined in the health belief model (HBM) 23 may also contribute to a resistance to change unhealthy behaviors or seek medical help in the first place. 24 Not recognizing symptoms of concussion may lead to inappropriately early return to play in sports and the potentially negative and serious consequences of second and repeated injuries prior to full recovery. So efforts at preventing first and subsequent concussions do require knowledge of the symptoms and treatment of concussion.
It is well known that the socioeconomic status (SES) plays an important role in health behaviours. 25 SES has also been found to modify interest–knowledge associations among adolescents. 26 Moreover, socioeconomic factors are closely associated with the knowledge on various diseases among adults and youths.27–29
Our prior report indicated that Canadians’ knowledge of the potential mental health sequelae of concussion was limited across all groups in Canada, even to health professionals. 30 In this report, we were particularly interested in determining the factors that predict concussion knowledge and awareness of respondents. We hypothesized that individuals from different sociodemographic profiles would demonstrate different levels of awareness and that those with previous concussion experience (their own, or someone close to them) would have greater knowledge of concussion symptoms than those without previous experience.
Methods
National surveys and ethics
As a part of a series of educational programs developed by ThinkFirst Canada (now a part of Parachute), the Coaching Association of Canada (CAC), the Canadian Centre for Ethics in Sports (CCES), and Hockey Canada (HC) (called the “PHAC Partners”), under the auspices of the Public Health Agency of Canada (PHAC), a large cross-sectional national voluntary electronic open survey with a sample as described previously 30 was conducted to determine the levels of knowledge associated with concussion in athletic communities across Canada. The questionnaire we used was composed of questions from a published questionnaire 21 with additions and modifications provided in conjunction with the PHAC partners. The core content focused on three areas: concussion awareness, concussion knowledge, and first-hand experience with concussion. The survey was conducted electronically, and 5231 out of 6031 respondents provided valid answers in the survey that was sent to 6348 people. Completion and submission implied consent to participate. Field Day Inc. collated the data and provided the anonymized unidentified dataset to the research team ensuring the responses provided by individuals who completed the survey could not be identified and analysis was performed on the aggregated data. The study was approved by St. Michael’s Hospital’s Research Ethics Board.
Measures
Identification rate
Participants were asked to identify, from a list of options, the symptoms, diagnosis, and treatment of a concussion and when one should return-to-sport (RTS) post-concussion. The percentage of correctly identified options was defined as the identification rate.
Concussion knowledge score
We developed a concussion knowledge score (CKS) that consisted of a sum of correct answers to 27 items and generated seven additional subscores on the basis of the symptoms, diagnosis, treatment, or RTS aspect of concussion: “physical” CKS (11 items), “cognitive” CKS (3 items), “mental health” CKS (3 items), “treatment” CKS (4 items), “return-to-sport” CKS (4 items), and “diagnosis” CKS (2 items). An “all symptoms” CKS (17 items) was also calculated as a sum of the “physical,” “cognitive,” and “mental health” CKS. The 27 items were scored on a dichotomous yes (1) or no (0) scale and higher scores indicated better knowledge of concussion. The CKS had a high intraclass correlation coefficient (Cronbach’s alpha of 0.82).
Social and demographic characteristics
Language, sex, age, educational level, annual household income, geographic location, and social/community role were included as independent variables in our analyses, and CKS “total” (27 items) and subscores (physical, cognitive, mental, diagnosis, treatment, and RTS) as outcomes. Participants, or their immediate family/close friends (teammates), that experienced TBI were categorized as the “TBI+” group, and all others were categorized into the “TBI−”group.
Data analyses
Mean values and standard deviation were used for description of continuous variables (CKS total and subscores), while frequencies and percentages were calculated for categorical variables (age range, language, sex, history of concussion/TBI, social/community role, educational level, annual household income range, and geographic location of survey completion). Total CKS and all subscores were calculated based on demographic characteristics and compared between TBI+ and TBI− groups and across demographic variables (language, sex, age, educational level, annual household income, geographic location, and social/community role) using an analysis of variance (ANOVA) or Wilcoxon rank-sum test for non-normally distributed data. Least significant difference method was used for the post hoc test after ANOVA. A Chi-square test was used to compare identification rates between TBI+ and TBI− groups. A multilevel logistic regression analysis was performed to identify which demographic/socioeconomic factors had an effect on the total CKS. If the total CKS was more than 25 (maximum 27), it was considered as “High”; If CKS was between 20 and 25, it was “Medium”; and if it was lower than 20, it was “Low.” The overall response rate is 95%. Multicollinearity was assessed with a variance inflation factor over 4. Odds ratio less than 1 means the variable was associated with more possibilities of lower CKS scores. All statistical analyses were performed using SAS 9.4 (Chicago, IL, USA). A p-value of less than 5% was considered significant.
Results
Survey respondents
Table 1 shows the characteristics of respondents who gave valid answers in the survey (n = 5231). The respondents were from all provinces and territories in Canada with the highest proportion coming from Canada’s most populated province, Ontario (40.1%); the majority identified themselves as coaches (64.2%) and had post-secondary or higher level of education (78.5%), 5.3% self-identified as athletes, and 6.3% as medical professionals (Table 1).
Demographic characteristics and CKS of survey respondents.

CKS: concussion knowledge score; SD: standard deviation; TBI: traumatic brain injury.
All data are reported as n (%).
Includes community, competitive, and high-performance coach.
Includes parent or guardian of athlete, sports trainer, team or club personnel, sports league, association or organization personnel, educator, teacher, learning facilitator, and others specified.
Participants or their family member/friends had a sport TBI.
Only include participants who had concussion history.
p < 0.001.
Identification rate and CKS
The identification rate and CKS were used to measure respondents’ adequate knowledge in recognizing the symptoms, diagnosis, and treatment of concussion and in regards to RTS guidelines (Table 1 and Figure 1). Respondents correctly identified the majority of concussion symptoms with mean identification rate of 80.6% (Figure 1). The highest identification rate was observed for cognitive symptoms (94.3%) and the lowest for mental symptoms (61.3%) (χ2 = 1716.9924, p < 0.0001).

Correct identification rates regarding respondents’ overall knowledge and subdomains of concussion knowledge.
Respondents’ total CKS varied corresponding to their demographic characteristics. Univariate analysis showed that compared to Ontario respondents, those residing in Nova Scotia and New Brunswick had significantly higher CKS (Table 1, Cohen’s d = 0.9, 1.2, respectively), while those who lived in Newfoundland and Labrador, Manitoba, Yukon, and Northwest Territories had significantly lower CKS (F = 14.94, p < 0.001, Cohen’s d = 0.3, 0.1, 0.1, and 0.5, respectively). In addition, total CKS of medical professionals (23.1 ± 3.5) and coaches (22.0 ± 3.9) were significantly higher than that of athletes (20.3 ± 4.9, p < 0.001, Cohen’s d = 0.7 and 0.4, respectively) and parents and athletic trainers (21.5 ± 4.2, p < 0.001, Cohen’s d = 0.3 and 0.3, respectively). Respondents with a history of TBI (22.3 ± 3.6) were significantly more knowledgeable than those who had no TBI (20.8 ± 4.4, p < 0.001, Cohen’s d = 0.4), and those still experiencing concussion symptoms also had significantly higher CKS than their counterparts (Table 1).
We compared the CKS and CKS subscores between TBI+ and TBI− groups. The former had significantly higher CKS and subscores in physical, mental, and cognitive symptoms as well as in treatment and RTS subscores. The TBI+ group had a slightly but significantly lower subscore in diagnosis (Table 2).
Correct identification rate, total CKS and all subscores of TBI+ and TBI− respondents.

CKS: concussion knowledge score; TBI+: with history of TBI; TBI−: without history of TBI; CT: computed tomography; MRI: magnetic resonance imaging.
p < 0.05.
A logistic regression analysis was performed to elucidate whether or not language, sex, age, annual household income, educational level, social/community role, TBI history, and geographic location played a role in predicting a high CKS. The analysis showed all these factors except geographic location affected a respondent’s CKS. French-speaking, lower level of education, lower household income, age between 15 and 44 years, and without a history of TBI had an odds ratio ranging from 0.4 to 0.8 (Table 3).
Odds ratio (OR) related to characteristics of respondents with CKS scores.
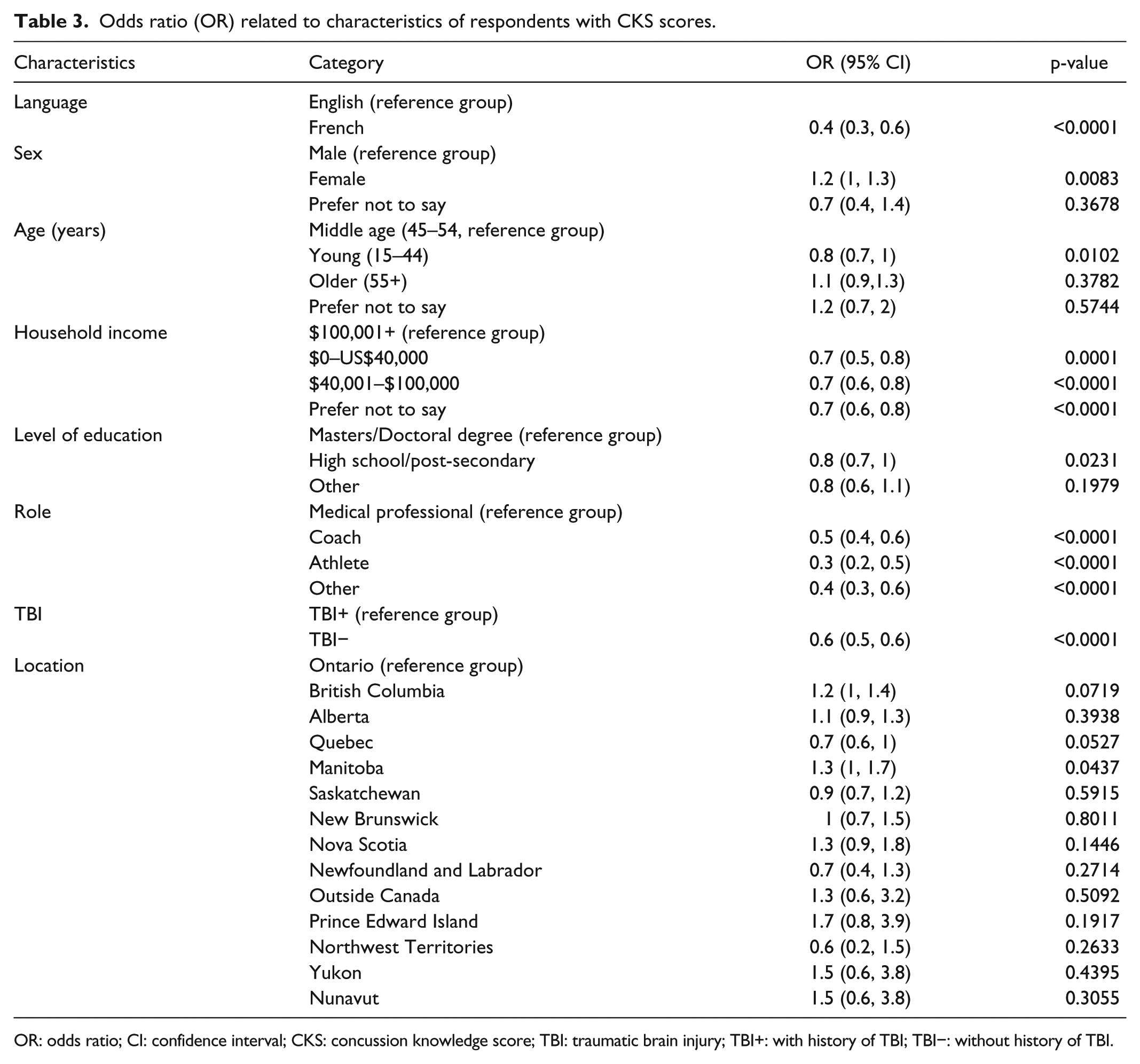
OR: odds ratio; CI: confidence interval; CKS: concussion knowledge score; TBI: traumatic brain injury; TBI+: with history of TBI; TBI−: without history of TBI.
Discussion
Overall, respondents showed high levels of knowledge of symptoms and treatment of concussion and were somewhat knowledgeable of concussion diagnosis and return-to-play guidelines as demonstrated by the moderate CKS subscore. Although both multivariate and univariate analyses showed that having a history of concussion was positively correlated with more concussion knowledge in general, it is noteworthy that the TBI+ group did not have better knowledge than the TBI− group regarding the diagnosis of concussion and only 51.0% TBI+ respondents believed that a psychiatric evaluation was appropriate if symptoms such as depression are present. This low rate warrants the need for additional educational initiatives to further promote and raise awareness of concussion, including an understanding that concussion can cause mental health problems for which appropriate treatments should be considered.30–32
Misconceptions about concussion, incorrect injury management (e.g. immediate RTS post-concussion), as well as delays in getting medical attention or treatment can lead to more concussions or have long-term harmful consequences.22,33 Delays in seeking treatment have been reported to patients with other medical conditions, and factors causing such delays have been reported, including lack of knowledge, stigma, costs, and attitude.34–36 Some of these factors may be applicable to concussed patients as well. For instance, concussed patients did not seek treatment if their symptoms were not a bother, disruptive, or resolved quickly, 2 which could be caused by the lack of concussion knowledge or attitudes. In addition, our findings indicate that one’s experience or encounter with an identified individual within their social circle (friends or relatives) with TBI was a predictor for higher level of concussion knowledge. This contradicts the findings by Weber and Edwards 22 who examined sport concussion knowledge in the UK general public and found that the experience of sport concussion had no influence on respondent’s knowledge, and if a concussed person did not experience certain symptoms, they would not think such symptoms would occur to other concussed individuals. 22 These contrasting results require further study but do suggest that future initiatives to prevent concussion should be made accessible to people regardless of their history or encounters with TBI. In particular, attention should be paid to the promotion of mental health symptoms recognition, appropriate diagnosis of concussion, and stepwise RTS procedures for which various educational approaches have been reported to be effective.21,37–44
Identifying factors affecting CKS could serve to inform more effective and efficient prevention programs, identifying key groups for educational and other preventative programs using tools like Haddon’s matrix.45,46 For example, our findings clearly suggest our French-speaking cohort could be a key group for enhanced awareness programs aimed at the sports population. The reason for the noticeable lack of concussion knowledge in this subpopulation is unknown; however, a recent report 47 has suggested sports organizations in French-speaking regions may be less engaged in efforts to track the incidence of concussion. Another possible reason is the provincial, regional, and even sports-organizational policy differences regarding athletic coaches’ and trainers’ official training in the area of concussion. For instance, beginning in the 2016–2017 season all coaches and team officials of North Vancouver Minor Hockey Association must complete the Concussion Awareness Training Tool (CATT) course as part of their certification process, while this requirement is not found in the 2014 policy from the National Coaching Certification Program (NCCP).48,49 This may reflect an overall value position on the importance of concussion research or potentially that concussion is perceived to be less of a problem; however, further research is required to examine this puzzling difference.
Our results also reinforce pervious studies 50 showing annual household income and level of education to be positively correlated with the level of concussion knowledge. These findings also show that those with lower income and education levels could benefit from prevention strategies. Thus, public initiatives should be tailored with these needs in mind. Previous studies of coaches, athletes, and parents regarding concussion knowledge demonstrated that coaches were more knowledgeable than athletes and parents.51–53 Our data supported this and further suggested that although medical professionals and coaches had more concussion knowledge than athletes and other participants, and there is still room for improvement. Considering the findings from our research and previous studies, we recommend that educating coaches and medical professionals in various formats with the integration of up-to-date guidelines may pay dividends in translating knowledge more widely to the general population.
There are several limitations to this study. Although our sample size was large and the assessment was concurrent for various participant groups including athletes, parents, coaches, and medical professionals, our findings are limited by evaluating group level data rather than individual level data. In addition, the disproportionate number of respondents from each of the provinces may result in an imbalance of findings and opinions related to their concussion knowledge. Another important limitation is that the survey used convenience sampling, and the self-reported responses are prone to recall errors and sampling bias. Nonetheless, the results represent the responses from a significant sample in an important segment of the population prone to concussion and can still be helpful in future studies and initiatives.
Conclusion
We found that groups involved in sports-related activities could improve their level of awareness of factors related to concussion. Experience of TBI, age, language, annual household income, social/community role, and level of education are important predicting factors of one’s concussion knowledge. Future strategies toward younger people (15–44 years old), those with lower economic and educational status, non-professionals like parents and players, non-English speakers, and those without a prior history of TBI may yield significant gains.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was partially supported by the Public Health Agency of Canada (M.D.C), the Canadian Institutes of Health Research Strategic Team Grant in Applied Injury Research #TIR-103946 (M.D.C), and the Ontario Neurotrauma Foundation (M.D.C).
Ethical approval
Ethical approval for this study was obtained from St. Michael’s Hospital’s Research Ethics Board.
Informed consent
Completion and submission implied consent to participate.