
Abstract
Background: Nurse suicide, a complex occupational health concern, is urgently in need of research due to the personal and occupational suicide risk factors experienced by nurses, namely mental health problems (e.g., depression), job problems, and substance misuse. Therefore, the study aims were to determine the contextual characteristics and circumstantial factors associated with nurse suicide in Kentucky. Methods: Secondary suicide data were obtained from the Kentucky Violent Death Reporting System (KYVDRS) from 2005 to 2019. Nurse suicide cases were identified using the Bureau of Labor Statistics Standard Occupational Classification. A mixed-methods analysis using descriptive statistics and qualitative evaluation was conducted to determine the distributions of demographic, injury, and weapon characteristics, followed by a qualitative analysis of the KYVDRS incident narrative text of nurse suicide decedents. Results: There were 88 decedents identified with a nursing occupation. The predominant means of death for male (59%) and female (45%) nurses involved firearms. Thematic analysis showed nurse decedents experienced a mental health problem (51%) and premeditated (50%) suicide preceding death. Incidentally, 51% of all cases experienced multiple circumstantial factors (e.g., relationship problems and premeditation) preceding their death by suicide. Discussion/Application to Practice: Nurse suicide decedents experienced multifactorial risk factors preceding their death by suicide, namely depression, premeditated suicide, and relationship problems. Occupational health practitioners and health care organizations can implement individual and organizational prevention efforts to help prevent nurse suicide.
Background
Nursing is an occupation known for its stressors and challenges that perniciously impact the nursing workforce (Melnyk et al., 2018). The personal and occupational stressors nurses experience are multifactorial and comprised mental health problems, understaffing, workplace violence and conflict, and feeling lonely, overwhelmed, and stressed (Davidson, Accardi, et al., 2020; Huang et al., 2018; Letvak et al., 2012). The convergence of nursing-related stressors can bring about the onset of chronic stress and burnout, ultimately playing a role in the emergence of depression and anxiety (Feskanich et al., 2002; Huang et al., 2018; Letvak et al., 2012). Consequently, the culmination of stress, anxiety, and depression increases the likelihood of alcohol and substance misuse among nurses, which is 10% to 20% higher than in the general population (Trinkoff et al., 2022). Nurse-related personal and occupational stressors place them at heightened risk for suicide (Davidson, Proudfoot, et al., 2020; Feskanich et al., 2002; Huang et al., 2018).
Surveillance of occupational suicide shows varying occupational-specific suicide rates; however, female registered nurse suicide rates were significantly higher than other health care occupations in 2016 (Peterson et al., 2020). Davis et al. (2021), in a comparison of nurse and physician suicide mortality, documented that female nurses (relative risk [RR] = 1.99) were more likely to die by suicide compared with females in the general population (Davis et al., 2021). Moreover, nurses (RR = 1.17) were more likely to die by suicide than physicians. In contrast, a longitudinal study of nurse suicide showed elevated suicide risk for female and male nurses versus the general population (Davidson, Proudfoot, et al., 2020). Furthermore, nurses were more likely to experience job problems and have a history of mental health problems than the general population.
A thematic study of nurse suicide contextual characteristics showed that over half of nurse decedents experienced depression, substance misuse, and job loss, while 44% previously attempted suicide (Davidson et al., 2021). The elevated suicide risk among nurses is concerning, given their personal and workplace stressors associated with mental health conditions and a higher prevalence of alcohol and substance misuse in nurses across health care settings (Huang et al., 2018; Letvak et al., 2012; Trinkoff et al., 2022).
Based on national data, prior research findings show nurses experience numerous circumstantial factors associated with their suicides, namely depression, substance misuse, job problems, and premeditated suicide (Davidson et al., 2021; Davidson, Proudfoot, et al., 2020). Nationally, there is scant information on nurse-centric suicide prevention programs, like the Healer Education Assessment and Referral (HEAR), and the effects of prevention programs to reduce nurse suicide mortality (Davidson et al., 2018). Moreover, few state-based studies evaluate the characteristics and circumstantial factors of nurse suicide. Therefore, it is imperative to conduct state-based research to determine the characteristics and circumstantial factors of nurse suicide. In Kentucky, suicide rates are 33% higher on average than national rates, efforts are underway to prevent nurse suicide. However, little is known about the characteristics and factors attributed to nurse suicide in Kentucky (Kentucky Board of Nursing, 2022). Therefore, the study aims were to determine the demographic, injury, and death characteristics and qualitatively evaluate the circumstantial factors of nurse suicide in Kentucky.
Methods
Study Design and Data Source
A retrospective cohort study was conducted to determine the characteristics and circumstantial factors of nurse suicide in Kentucky. Secondary data were obtained from the Kentucky Violent Death Reporting System (KYVDRS), which is part of the National Violent Death Reporting System (NVDRS; Centers for Disease Control and Prevention, 2020). The KYVDRS is a federally funded, state-based surveillance system that collects information on legal interventions, homicides, suicides, unintentional firearm deaths, and deaths of undetermined intent. The data are collected and abstracted from multiple sources, including death certificates, coroner/medical examiner (CME), and law enforcement (LE) reports, which contribute to over 600 unique data elements about suicide and the factors contributing to it. The KYVDRS secondary data examined in this study included all suicide cases from 2005 to 2019. The University of Kentucky Institutional Review Board (IRB) approved the study and determined that informed consent was not required since all study subjects were deceased.
Procedures and Measures
Nurse Suicide Case Ascertainment
Suicide cases for Kentucky were ascertained using the KYVDRS “death manner per abstractor” variable (Centers for Disease Control and Prevention, 2022). Following case ascertainment, the Bureau of Labor Statistics Standard Occupational Classification codes were used to classify suicide cases with a nursing occupation (Supplemental Material).
Decedent Characteristics
The KYVDRS variables for demographic, injury, death, and weapon type (i.e., means of death) were used to determine characteristics of nurse suicide decedents. Variables were recoded based on the methodology employed by Norrod et al. (2023) to prevent small cell sizes (≤5) per NVDRS guidelines (Centers for Disease Control and Prevention, 2022; Norrod et al., 2023). Three age groups were created based on biological epochs of life, while race was recoded into two categories. Similarly, educational degree, relationship status, and weapon type variables were each recoded into three categories. All data coding, case ascertainment, and analysis used SAS 9.4 software for Windows (SAS Institute Inc., 2013).
Incident Narrative Text
The nurse suicide incident narrative text for the thematic analysis used the KYVDRS CME and LE incident narrative free text variables (Centers for Disease Control and Prevention, 2022). The incident narrative text provides detailed contextual information obtained through interviews during CME and LE investigations. All information from the CME and LE reports were abstracted verbatim into the KYVDRS using NVDRS standards.
Analysis
A mixed-methods analysis consisting of descriptive statistics and a qualitative evaluation was conducted to determine the characteristics and circumstantial factors of nurse suicide decedents. Descriptive statistics were used to determine the central tendency of nurse suicide decedents’ average age and the distributions across age groups, race, education level, relationship status, and weapon type (i.e., means of death) by biological sex (Kaur et al., 2018). Following the descriptive assessment, we qualitatively analyzed the KYVDRS incident narrative text. No inferential statistics were employed because the study aims were descriptive and qualitative in nature.
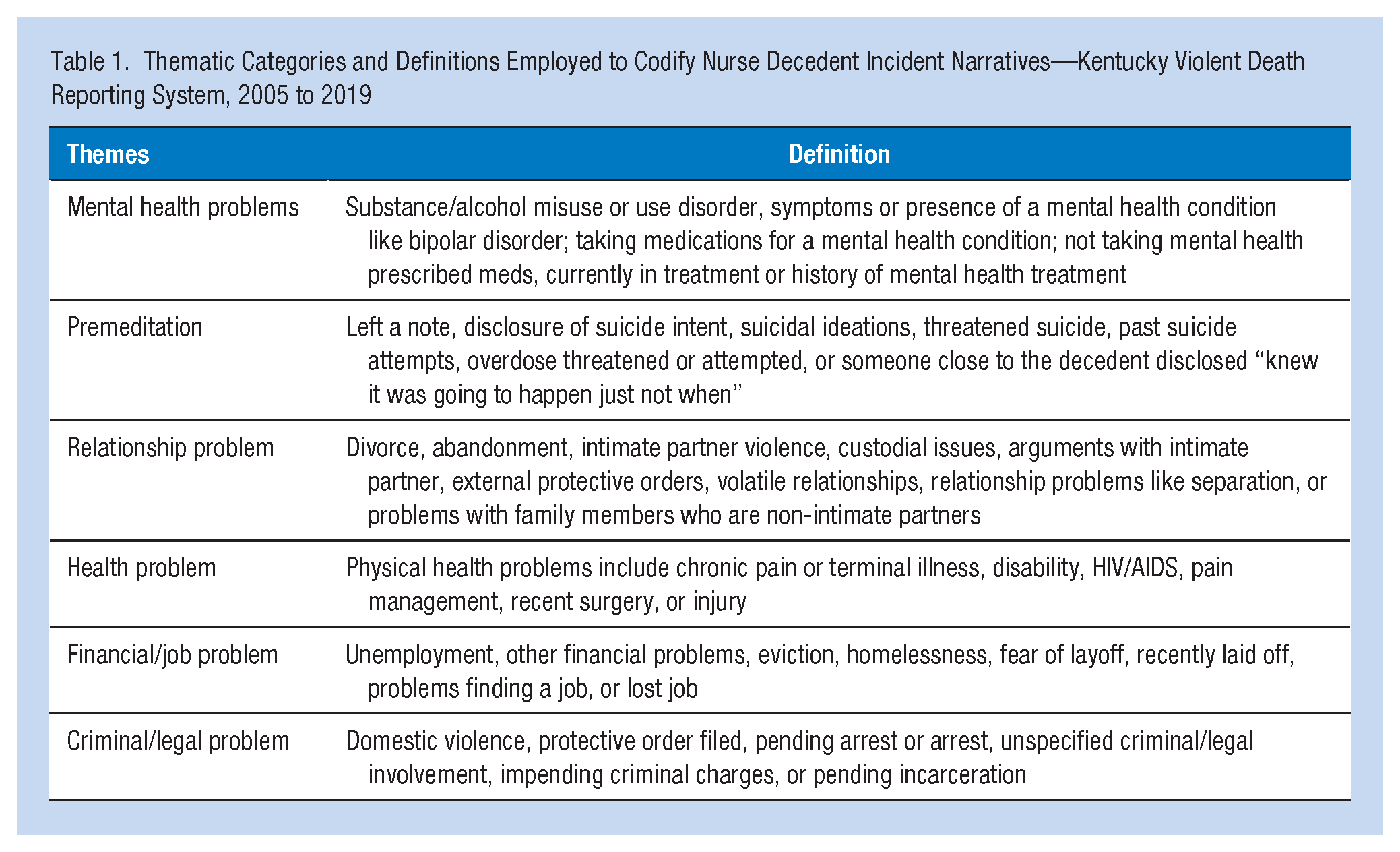
The qualitative analysis employed an a priori thematic coding methodology to classify the CME and LE incident narratives (Brown & Seals, 2019; Holland et al., 2017, 2018). The methodology employed an iterative qualitative coding process conducted by inter-raters using six thematic categories to thematically classify NVDRS incident narrative text. Using this methodology, the qualitative analysis of incident narratives provided in-depth insights into the complex factors contributing to suicide that are not elucidated through quantitative analysis (Holland et al., 2018). Table 1 shows the a priori thematic categories with definitions, which include mental health problems, premeditation, relationship problems, health problems, financial/job problems, and criminal/legal problems.
Thematic Categories and Definitions Employed to Codify Nurse Decedent Incident Narratives—Kentucky Violent Death Reporting System, 2005 to 2019
To increase the overall rigor and reliability of the qualitative results, an inter-rater review panel of authors with expertise in injury prevention, nursing, and epidemiology thematically classified the incident narratives independently. The classification strategy permitted consistent coding of the incident narratives; thus, each suicide case was classified to identify the six thematic categories. The senior author, who participated in developing the themes and coding methodology, reviewed the classifications of the other three authors to assess and improve inter-rater reliability.
Reliability showed that the three reviewers agreed on 61% of cases in the initial independent review. The remaining 39% of cases with discrepant codes were discussed in a consensus conference until all authors reached consensus. The four main reconciled discrepancies were as follows: (a) when there was polysubstance overdose, one coder considered that to be premeditation—to have acquired so many different types of substances there must have been forethought—this accounted for 21% of the discrepancies; (b) in 9% of the cases “suicidal ideation” was coded as a “mental health problem”; and (c) coders varied (9%) about whether “divorce” was a “criminal legal problem.”
Reviewers discussed how to reconcile coding discrepancies, and case discrepancies were corrected within the formal coding guidelines. Further coding followed these established guidelines. Changes included (a) a polysubstance overdose was not coded as “premeditation”; (b) suicidal ideation was not coded as a “mental health problem”; and (c) “divorce” was not coded as a “legal problem” unless “criminal/legal problems” were mentioned.
Results
A total of 88 suicide decedents were identified with nursing occupations out of the 9,797 adult suicides in Kentucky for the study period. Table 2 shows the decedents’ demographic characteristics. The average age of male nurse decedents was 43 years (SD = 9.39); female nurse decedents were 51 years (SD = 12.05) old on average. Over half of the suicide deaths occurred among nurses between 40 and 59 years old. In addition, a quarter of female nurses over age 60 died by suicide. The number of suicides for male nurses under 40 was unreportable due to the small cell sizes (≤5) of deaths in that age group. Racial-ethnic distributions showed that over three quarters of nurse suicide deaths occurred among nurses identified as White. The frequency of non-White female nurse decedents was unreportable due to low counts (Table 2).
Demographic Characteristics of Nurse Suicide Decedents by Sex—Kentucky Violent Death Reporting System, 2005 to 2019
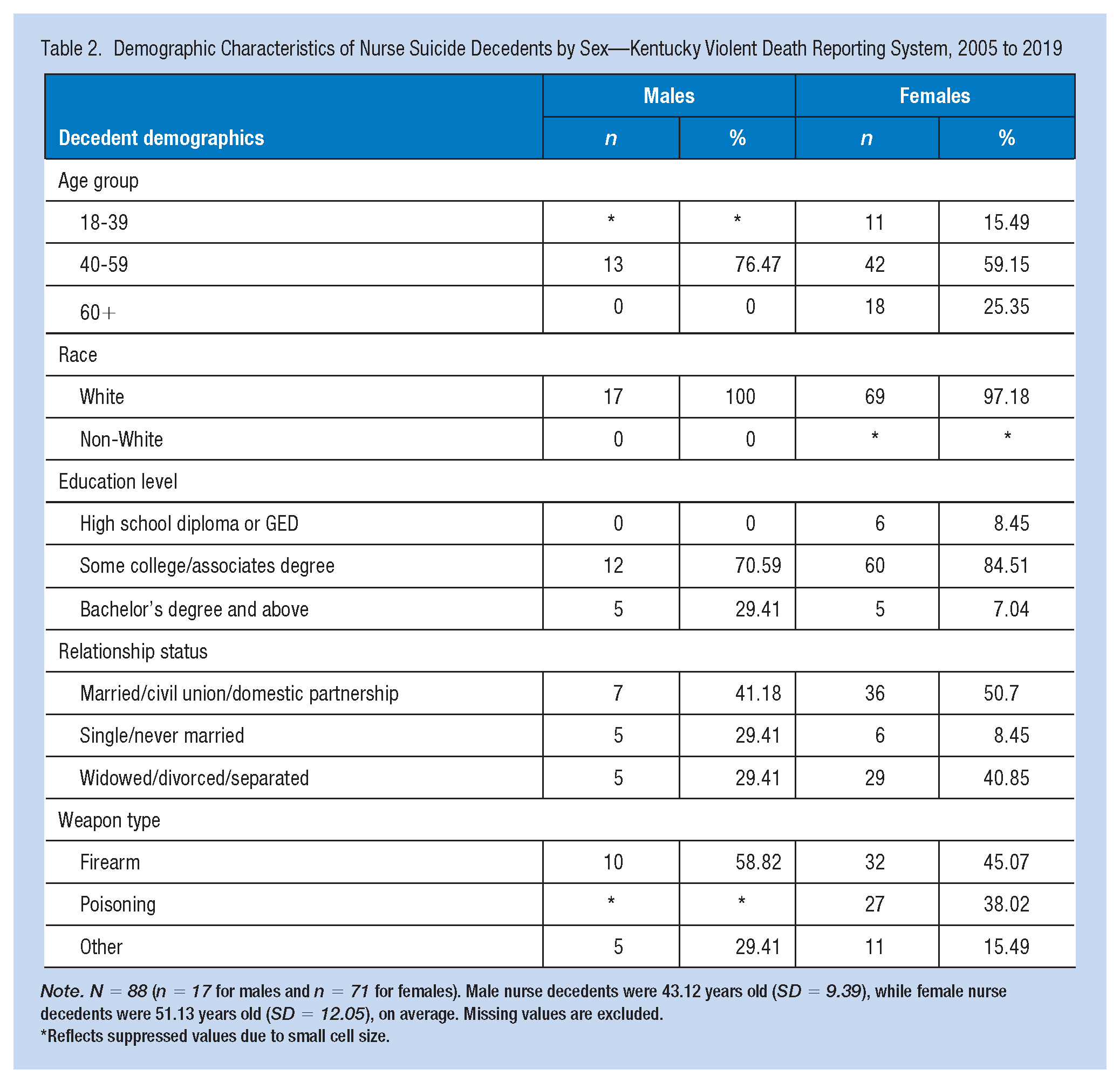
Note. N = 88 (n = 17 for males and n = 71 for females). Male nurse decedents were 43.12 years old (SD = 9.39), while female nurse decedents were 51.13 years old (SD = 12.05), on average. Missing values are excluded.
Reflects suppressed values due to small cell size.
Over half of female nurse decedents were married, in a civil union, or domestic partnership, followed by widowed, divorced, or separated nurses. Education status of nurse decedents showed that almost three quarters of male and over 80% of female decedents received some college or held at least an associate’s degree, while less than a quarter had a bachelor’s degree or above. The use of firearms and poisoning as methods of fatal injury showed similar distributions for female nurse decedents. Specifically, 45% of female nurse decedents used a firearm, while 38% used poisoning. Conversely, over half of male nurse decedents used a firearm as the fatal means of death.
Thematic Results
The thematic analysis of incident narratives revealed multiple circumstantial factors associated with nurse suicide. Furthermore, 93%of the cases had completed CME and LE narrative text. It should be noted, however, that thematic categories are not mutually exclusive because each case may experience multiple circumstantial factors preceding death by suicide. The narrative excerpts below represent a verbatim composite of text from the CME and LE incident narratives.
Mental Health Problem
Over half of decedents experienced a mental health problem before suicide. Table 3 shows the distribution of mental health problems, namely depression, anxiety, and a history or presence of substance/alcohol use. In several cases, the nurse decedents were treated for multiple mental health problems, prescribed psychotropic medications, and received psychotherapy. For cases coded with three or more circumstantial factors, the nurse experienced a mental health problem in all but two cases. There were three cases with a recent hospital discharge (psychiatric or following surgery) within 2 weeks of death. A family history of suicide was noted in three cases. Of the decedents who experienced a mental health problem, substance/alcohol misuse (19%) was reported as a circumstantial factor, including situations, such as:
Thematic Analysis of Coroner/Medical Examiner and Law Enforcement Incident Narratives of Nurses Who Died by Suicide in Kentucky, 2005 to 2019
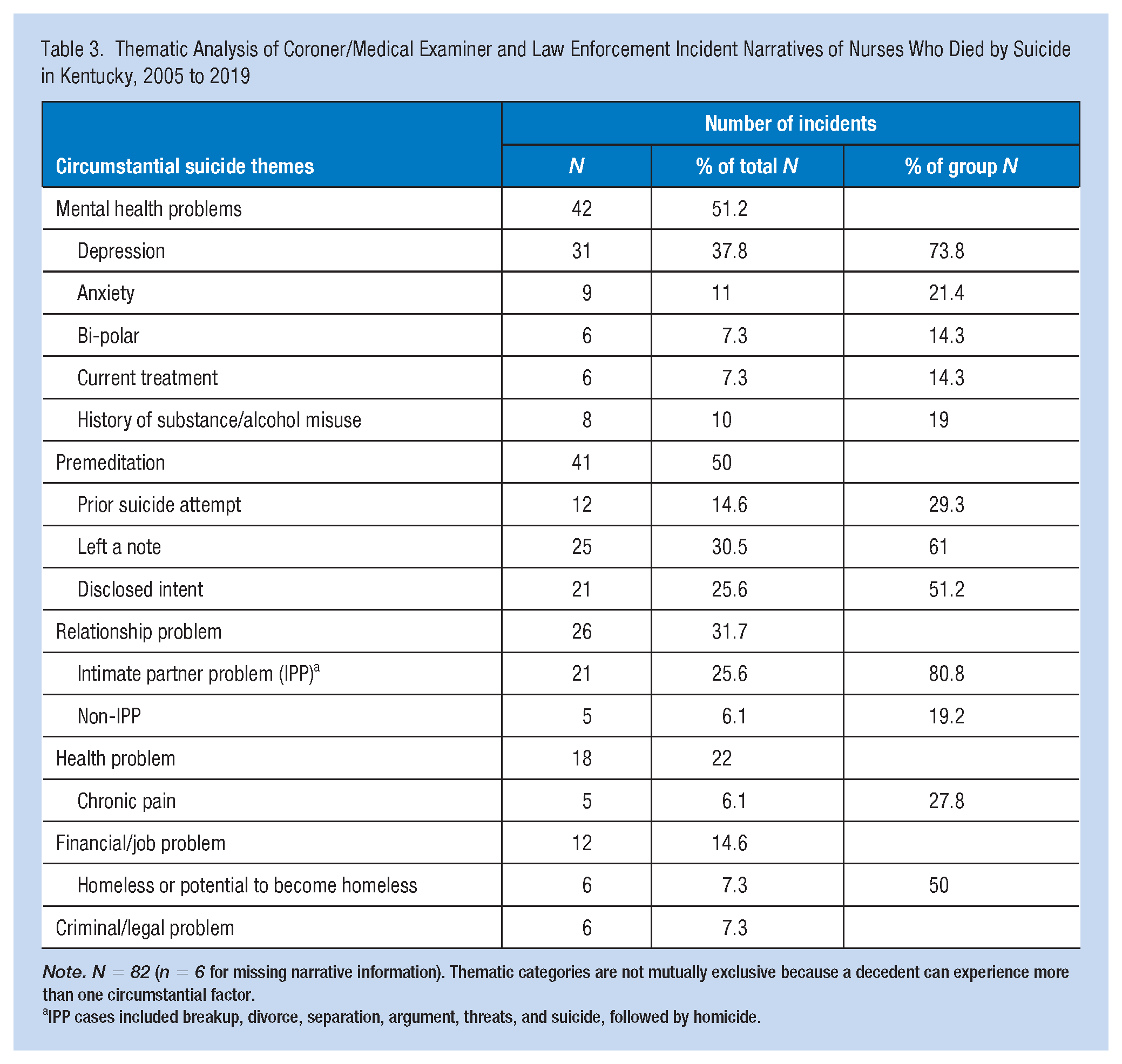
Note. N = 82 (n = 6 for missing narrative information). Thematic categories are not mutually exclusive because a decedent can experience more than one circumstantial factor.
IPP cases included breakup, divorce, separation, argument, threats, and suicide, followed by homicide.
Victim was found by her daughter after she had not heard from her. Victim had been treated for anxiety and depression and was on medication. Victim had been released from a psychiatric hospital two weeks prior and was staying with her daughter, but insisted she stay at her own home that day. Victim was going through a divorce and had told her daughter she would attempt suicide weeks prior. Victim left a long and detailed note talking about her depression, anxiety, and alcohol abuse problems.
Premeditation
Premeditation was present in half of the cases, with most decedents communicating their intent verbally or in writing to a family member or friend. Of the cases with premeditation, 29% of decedents previously attempted suicide. Of the 21 times where decedents disclosed their intent, there were six occurrences where the nurse disclosed or threatened suicide followed by an attempt. Examples of premeditation are noted as:
Male victim hung himself in the living room. According to the witness, the victim often expressed suicidal thoughts and ideations. The victim stated he would do something to himself earlier in the day to his wife. Victim was found by K-Mart employees in the parking lot. There were three notes in the car. Victim lost her son in a car accident about a year ago and had also gotten divorced since the loss of her son.
Relationship Problems
Relationship problems occurred in almost one third of cases, of which 21 were determined to have experienced an intimate partner problem (IPP) preceding their death by suicide. Common themes associated with IPPs involved arguments, separation, or divorce. Other IPP cases pertained to ongoing separation or divorce and co-occurrence of a mental health condition. In a more extreme case, the victim shot their significant other, then shot themself, resulting in a homicide-suicide. In contrast, there were only five cases of a non-IPP. Relationship problems were noted as:
Victim had recently moved back in with his parents after living in a different state. Victim was separated from his wife and going through a divorce. Victim felt that she had no one to care for her and was depressed. Victim was going through a divorce and had told her daughter she was going to attempt suicide weeks prior.
Health Problem
Health problems constituted less than a quarter of circumstantial factors, and when present, the narrative text indicated multiple contributing health conditions. Three cases listed a single health problem as a circumstantial factor. The health problems involved recent surgery, terminal illness, neurologic disorders, and chronic pain. Of the 18 cases classified with a health problem, five of those cases (28%) were noted to experience chronic pain, such as:
Victim died at her residence. The death certificate indicated that chronic pain, depression, and hypertension contributed to the cause of death. Oxycodone and tramadol are indicated as drugs contributing to the overdose death. Victim had a history of chronic pain, hypertension, depression, suicidal threats and attempts, and a substance misuse problem. Victim was reported to have a currently depressed mood and left a suicide note for her children, talking about her pain and that the medicines were not working.
Financial/Job Problems
Twelve cases were classified as associated with financial/job problems. For cases with a financial/job problem, a recent job loss or being fired contributed to the suicide death. In at least one instance, the victim was noted to be struggling with the death of a patient. Finally, six cases were identified as being homeless or having the potential to become homeless. Financial/job problems were noted as:
Victim with a self-inflicted gunshot wound from an unspecified firearm. Victim reported having a history of depression, current depression exacerbated by losing his job the week before. Victim had been fired from his job the week before. Victim left a suicide note. V was found at home by her ex-husband and daughter. It was reported that the victim had been depressed over the loss of a patient when she was a kidney dialysis nurse.
Criminal/Legal Problem
Only six cases were identified as having criminal/legal problems. In three cases, the criminal/legal problems involved IPPs resulting in an arrest, an external order of protection, or the filing of domestic charges. No specific information was provided for the other cases to indicate the criminal/legal problem type. Criminal/legal problem narratives were noted as:
Victim female intentionally overdosed at her residence. She had threatened and attempted suicide in the past. The victim was being treated for depression over impending criminal charges. She had an argument with her spouse, who had taken out an EPO against her. V had been kicked out of her house.
Polysubstance Overdose
Poisoning was used by over one third of female nurse decedents and about 12% of male nurse decedents. Evaluation of incident narratives revealed that 16% of polysubstance overdose cases included ingestion of non-pharmacologic substances, such as:
Victim died from ingesting multiple drugs with ethanol and isopropanol. Victim had a history of depression. Victim tested positive for benzodiazepines, ethanol alcohol, acetone, isopropanol, antidepressants, antihistamines, and stimulants.
Multiple Circumstantial Factors
Throughout the qualitative analysis, investigators observed narratives with multiple circumstantial factors. Cases with multiple circumstantial factors accounted for over half of all codified cases. Of the 42 cases with multiple circumstances, 76% of the cases involved a mental health problem with premeditation, mental health and relationship problems (33%), mental health and physical health problems (21%), and mental health and financial/job problems (19%). Finally, we identified 18 cases containing three or more precedent circumstantial factors. The combination of factors varied across the 18 cases; however, the narrative indicated a mental health, health, relationship, and job/financial problem preceding death in at least three cases.
Discussion
There has been an emergence of research on nurse suicide because of occupational suicide surveillance indicating rising nurse suicide mortality. However, to our knowledge, there are no state-specific evaluations of nurse suicide, although suicide mortality varies by geography (Phillips, 2013). Thus, this study evaluated secondary suicide data using a mixed-methods approach to determine the characteristics and circumstantial factors of decedents identified with a nursing occupation in Kentucky—a state known for elevated suicide mortality that exceeds the national average (Kaiser Family Foundation, 2023).
As found in nurse suicide studies using NVDRS data, more than half of suicide deaths occurred among middle-aged and female nurses (Davidson, Proudfoot, et al., 2020; Davis et al., 2021). The findings related to sex and age align with the reports by Davis et al. (2021), indicating that the average age of female nurse decedents was 51 years (Davis et al., 2021). Male nurse decedents were comparatively fewer, aligning with national trends in nurse suicide but diverging from higher sex-specific incidence of male suicide in the general population (Davis et al., 2021). The predominance of White and female nurse decedents is consistent with national data on nurse suicide and nurse workforce trends (American Association of Colleges of Nursing, 2023; Davidson, Proudfoot, et al., 2020).
The incidence of nurse decedents in an intimate partner relationship and the frequency of IPP mirrors characteristic frequencies in nurses and the general population. Examination of KYVDRS incident narratives revealed that 32% of nurses experienced an IPP before their death. In an NVDRS sample of nurse suicide decedents, IPP was antecedent to nurses dying by suicide. (Davidson et al., 2021). In contrast, analysis of risk factors among nurse suicide decedents has shown that female nurses experience fewer IPP than the general population (Davidson, Proudfoot, et al., 2020). Nurse decedents, though, may have experienced increased suicide risk in the face of stressors associated with being a nurse, especially if accompanied by burdensome feelings and thwarted belongingness (Bagge et al., 2013; Ho Choi et al., 2013; Van Orden et al., 2010).
The heightened interpersonal suicide risk among nurses is concerning, given the thematic analysis findings showed that over half of nurse suicides involved a mental health problem, with 76% of those cases experiencing depression. Recent national studies that employed thematic analysis have shed light on the alarming presence of mental health problems, specifically depression, among nurse suicide decedents (Davidson et al., 2021). The prevalence of mental health problems in nurses is further underscored by recent state-based research showing that nurse depression scores were statistically associated with decreased job satisfaction and well-being (Letvak et al., 2012). These pervasive multiple circumstantial factors shown in the thematic analysis in this study and by Davidson et al. (2021), namely interpersonal problems, mental health problems, and substance/alcohol use raise concerns about the adequacy of support available to nurses. Moreover, it is conceivable that job problems related to unemployment, job loss, and occupational stress may have been a detrimental factor among nurse decedents amid their persistent struggle with mental and physical health problems.
The absence of ample protective factors, specifically support from colleagues and health care organizations, may be attributed to various individual, cultural, and systemic factors that include work environments where peers, due to their stress, cannot offer emotional support or assess for crisis among coworkers. Moreover, inadequate support within professional settings may reflect cultural stigmas surrounding mental health or stringent zero-tolerance policies on substance/alcohol misuse. Inadequate support systems and maladaptive work environments may have led to Kentucky nurse decedents experiencing unbearable emotional turmoil, marked by desperate, unmet pleas for relief from their mental, emotional, and physical pain. Thus, the culmination of unaddressed distress resulted in suicide, primarily through highly lethal means, namely firearms and multisubstance poisoning.
The high incidence of firearms use by female nurses contradicts the nurse suicide literature documenting a lower utilization of firearms (Davidson, Proudfoot, et al., 2020; Davis et al., 2021). Nationwide, though, firearms are involved in nearly half of all suicides, possibly related to availability, accessibility, and lethality (Centers for Disease Control and Prevention, 2019). In contrast, over 38% of Kentucky female nurse suicide decedents poisoned themselves, which aligns with national and health care suicide statistics (Centers for Disease Control and Prevention, 2019; Davidson et al., 2021; Davidson, Proudfoot, et al., 2020; Davis et al., 2021). The prevalence of polysubstance poisoning as a method of death among nurse suicide decedents suggests a connection between the means of death and occupational knowledge about fatal substances (Davis et al., 2021).
The substances nurses used as lethal means varied. Still, postmortem toxicology tests and evaluation of the incident narrative text revealed the presence of opiates, antidepressants, benzodiazepines, anticonvulsants, and muscle relaxants. Notably, several cases in this study tested positive for non-pharmacologic substances, namely organic solvents, a finding that, to our knowledge, was previously undocumented. The lethal means employed by nurses in this study and nationally suggest a potential relationship between accessibility and availability of specific lethal means, warranting further exploration of nurse knowledge of and access to lethal means with a clear need for means-specific preventive measures.
There are several limitations in this study. First, study data are collected retrospectively and relies on the investigation and reporting of case information by CME and LE officials to the KYVDRS. Second, incident narrative text may be subjective because findings are, in part, based on recall and perspectives of family and friends of the decedent. Thus, case narratives may be subject to recall bias. Recall bias may be inadvertent; however, the prevalence of stigma and awareness about suicide may affect recall (Walsh et al., 2007). Third, data abstractors are limited to the data included in the reports they receive; some CME and LE reports lack comprehensive descriptions of the incidents, limiting the abstractors’ ability to capture all contributing factors. Finally, stratification by licensure type was impossible because of low frequencies across certain licensure types. Because our study focused on Kentucky nurse suicide and employed a descriptive evaluation of nurse suicide characteristics followed by a qualitative analysis of incident narrative text, results may not generalize to all nurses (Walsh et al., 2007).
We found that many nurse suicide decedents experienced multiple precedent co-occurrent circumstantial factors, which has been shown in evaluations of nurse suicide using the NVDRS (Davidson et al., 2021). Therefore, comprehensive upstream interventions and suicide prevention efforts, driven by occupational health practitioners and organizations that employ nurses, are needed to address the multiple circumstantial factors attributed to nurse suicide.
Nationally, there is a renewed emphasis on occupational violence prevention, particularly suicide prevention among agricultural workers (NORA Agriculture Forestry, and Fishing Sector Council, 2018). However, suicide prevention in health care generally prioritizes in-patient suicide prevention rather than focusing on health care professionals like nurses (Brodsky et al., 2018; Hogan & Grumet, 2016). One of the few evidenced-based suicide prevention programs, the HEAR program, was recently adapted for nurses and evaluated. The evaluation showed encouraging findings; however, program referrals were limited in number and only included suicidal nurses (Davidson et al., 2018). Nurses who completed screenings disclosed escalating work stress, emotional pain, and feelings of loneliness, which is noted in this study and nationally (Davidson et al., 2021). In response to emerging research on nurse suicide, the American Nurses Association (ANA) published several articles on it to help raise awareness (Carpenter et al., 2021; Howard et al., 2021; Tucker et al., 2023). Yet, there are still shortcomings in nurse suicide prevention at the individual and organizational levels.
Nationally, there are several evidence-based suicide prevention programs that occupational health nurses can utilize to help reduce suicide in the nursing workforce. Programs like Mental Health First Aid (MHFA), Question–Persuade–Refer (QPR), and Applied Suicide Intervention Skills Training (ASIST) are designed to train anyone as a suicide gatekeeper (Gould et al., 2013; Keil, 2019; Schurtz et al., 2010). Each training focuses on increasing knowledge and awareness about suicide behaviors, increasing peer support, and linking suicidal persons to a licensed mental health or health care professional. In contrast, clinical-focused suicide prevention training includes those like the HEAR program and Collaborative Assessment and Management of Suicidality (CAMS), allowing for assessment, treatment, and tracking of suicide behaviors. Each gatekeeper and clinical-focused training, except for ASIST, is available nationwide through a live, online training setting. In addition to suicide prevention training for individual nurses, there are several other prevention approaches for occupational health nurses to consider.
Comprehensive nurse suicide prevention efforts might include advocating for policy changes, as seen in Kentucky, where the Board of Nursing requires all licensed nurses to complete continuing education on suicide prevention (Kentucky Board of Nursing, 2022). Other approaches could involve annual workforce screenings for suicide risk factors and awareness-raising campaigns during in-service yearly training. Incidentally, each suicide affects about 135 people (Cerel et al., 2019). Should suicide occur among in the patient population or nurse workforce, postvention services are crucial and have proven effective at reducing suicide bereavement (Cerel et al., 2013, 2017; Moore et al., 2022).
With the emphasis on total occupational health and workforce violence prevention, nurse suicide prevention requires comprehensive prevention efforts at all levels (NORA HCSA Council, 2019). Moreover, there is a need for additional research partnerships between research institutions and occupational health nurses to pilot and evaluate suicide prevention programs, given the scant information on suicide prevention among the nursing workforce.
Applications to Professional Practice
This study identified 88 suicide decedents with a nursing occupation between 2005 and 2019. Most nurse decedents were 40 to 59 years old, while fewer female nurses were 60 or over. The prevalent means of death for male (59%) and female (45%) nurses was firearms, followed by poisoning for female nurses. Nurse decedents experienced multiple comorbid risk factors preceding their suicide, namely mental health problems and premeditated suicide, potentially indicating chronic stress and failed support systems. Given nurses’ persistent occupational stressors, occupational health practitioners and health care organizations must prioritize comprehensive nurse suicide prevention efforts. Furthermore, interventions must encompass all aspects of prevention and include addressing upstream etiologies associated with suicide in the nursing workforce.
Supplemental Material
sj-docx-1-whs-10.1177_21650799241289139 – Supplemental material for Circumstantial Factors Among Kentucky Nurse Suicide Decedents, 2005 to 2019
Supplemental material, sj-docx-1-whs-10.1177_21650799241289139 for Circumstantial Factors Among Kentucky Nurse Suicide Decedents, 2005 to 2019 by Paul E. Norrod, Julie Marfell, Lee Anne Walmsley and Sabrina Brown in Workplace Health & Safety
Footnotes
Authors’ Note
The analyses, results, and conclusions presented here represent the authors and do not necessarily reflect those of the CDC. The Institutional Review Board at the University of Kentucky reviewed and approved the study—IRB #81529—on September 15, 2022.
Author Contributions
P.E.N., J.M., L.A.W., and S.B. designed the study and conducted the inter-rater review. P.E.N. and S.B. conducted the analysis. P.E.N. and S.B. drafted the manuscript, and J.M. and L.A.W. critically revised it for intellectual content. All authors approved the final manuscript for publication.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by pilot grant 5T42OH010278-10 from the Centers for Disease Control–National Institute for Occupational Safety and Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.