
Abstract
Background:
Workplace violence (WPV) is a global public health problem and a threat to the health of Korean workers. This study assessed the prevalence and risk factors of WPV and its association with mental and physical health among Korean workers.
Methods:
Data obtained for 50,205 respondents to the Fifth Korean Working Conditions Survey were utilized for this study. Verbal abuse, threats, physical violence, and sexual harassment were assessed individually and as a composite for “any WPV.” Workers were characterized by education, income, shift work status, access to a health and safety education program, work sector and overall health. Descriptive analyses and multiple logistic regression analyses were used to estimate the prevalence of WPV and its association with mental and physical health.
Findings:
Overall, 5.6% of workers reported experiencing one of four forms of WPV. The prevalence of verbal abuse, threats, physical violence, and sexual harassment were 4.9%, 0.7%, 0.2%, and 1.1%, respectively. Most perpetrators were customers. Prevalence of WPV was associated with lower education level, poor health status, long working hours, shift work, and no experience of health and safety education; 9.0% of service workers experienced violence. Workers who had experienced WPV were more likely to experience anxiety, sleep-related problems, depressive symptoms, back pain, headache/eye strain, and overall fatigue.
Conclusions/Applications to Practice:
Workplace violence is a serious occupational and public health concern in Korea. These results suggest managing WPV may improve workers’ well-being and that violence-prevention strategies, policies, and regulations should be implemented across most industries.
Background
Workplace violence (WPV) has become an important public health issue in many countries. According to the International Labor Office (ILO, 2003), the definition of WPV is “any action, incident, or behavior that departs from reasonable conduct in which a person is assaulted, threatened, harmed, injured in the course of, or as a direct result of, his or her work.” In the World Health Organization’s 2004 World Report on Violence and Health, WPV includes behavior from aggressive language to physical violence (Butchart et al., 2004). WPV has been a poorly controlled problem since it was recognized in the 1970s (Magnavita et al., 2019), and its prevalence has not improved in recent Korean Working Conditions Survey (KWCS) and European Working Conditions Survey (EWCS) reports (García-Herrero et al., 2017; Kim, 2017), becoming an increasing social concern in Korea (Yoo & Lee, 2018). Workers’ demographic characteristics, working conditions, and job sector are considered risk factors for WPV in Korea (Choi et al., 2018; Hong et al., 2019; Hwang et al., 2020; Kim & Yoon, 2017); for example, long work hours are known to increase the prevalence of WPV (Choi et al., 2018). A recent national survey found that the following groups were more likely to report sexual harassment, bullying, and physical violence: women, high school graduates rather than college graduates, those engaged in shift work, and those working in service sectors with frequent customer contact (Hong et al., 2019).
Workplace violence may lead to health problems among workers; it is theorized that sadness, anger, and fear of violence may weaken an individual’s stress regulation, therefore, WPV may result in victims’ negative mental reactions (Portoghese et al., 2017; Szczygiel & Mikolajczak, 2018). According to a 7-year population-based follow-up study of adverse health outcomes related to experiencing physical violence at work, those exposed to physical violence required more treatment for both physical and mental health problems than non-exposed workers (Friis et al., 2019). In another study, nurses exposed to WPV were 1.5 times more likely to report anxiety symptoms than nurses who were not exposed (Cheung & Yip, 2017). Systematic reviews and meta-analyses have shown that exposure to bullying, physical, verbal, or sexual violence have been associated with sleep problems (Magnavita et al., 2019; Nielsen et al., 2020). In a Korean study, risk of sleep disorders was four times higher in workers experiencing WPV than non-exposed workers (Yoo et al., 2016). A study among physicians and nurses in China found that participants who experienced violence were approximately twice as likely to report depression and anxiety as participants who did not (Shi et al., 2020). Finally, a representative workplace survey in Denmark showed that, among employees from various professional fields, sexual harassment exposure had a higher mean level of depressive symptoms compared to non-exposure (Friborg et al., 2017).
Negative psychological response from WPV has been considered a mediator between WPV and physical problems (Choi et al., 2018; Sun et al., 2017). It is essential to recognize that individuals’ failure to cope with psychological stress may lead to physical health problems (Sultan-Taïeb et al., 2017). Since WPV may be considered a serious stressor, persistent psychological stress and maladaptive responses to violence may manifest in the form of physical symptoms (García-Herrero et al., 2017; Lever et al., 2019). For example, a study found that mental health problems from verbal violence were associated with teachers’ musculoskeletal pain (Ceballos & Carvalho, 2020). Anxiety due to violence results in workers rarely changing posture and taking little breaks during work (Roncoleta et al., 2020). This persistent physical strain or mental stress may lead to musculoskeletal pain (Khubchandani & Price, 2015) and headache (Lever et al., 2019).
In recent years, WPV has been discussed in terms of health risk factors among various job sectors in Korea (Hwang et al., 2020; Kang et al., 2019; Kim & Yoon, 2017; Yoo & Lee, 2018). However, there is a gap in the literature linking the prevalence of WPV to the health impacts on workers. Therefore, based on a nationally representative data set of the Korean worker population, this study aimed to examine the prevalence of WPV in the working population and identify which working conditions are risk factors for WPV. In addition, this study investigated the association between experiences of WPV and mental and physical health outcomes.
Methods
This study analyzed data from the Fifth KWCS conducted by the Korea Occupational Safety and Health Agency (KOSHA) from June 22, 2017 to July 4, 2017. The KWCS is a nationally recognized triennial survey which investigates the occupational environment, socioeconomics, and workers’ health conditions. The methodology and survey questionnaire used by the KWCS are the same as those used in the EWCS (Eurofound, 2017). A representative sample of the economically active population aged 15 years and above who were employees, employers, or self-employed was selected as participants. The KWCS has been described in detail in the working conditions report in Korea published by KOSHA (2019) and Eurofound (2017).
The study design employed multistage random sampling based on the Population and Housing Census (Seo, 2016). The primary sampling units were the population and housing enumeration district, which were selected by systematic sampling in proportion to the number of households within the enumeration district. The secondary sampling units were household and household member. Ten target households were selected in the enumeration district by systematic sampling from the household lists and district maps. The KOSHRI hired professional surveyors to conduct the survey and trained them on interviewing methods, such as paper and pen interview (PAPI), using paper questionnaires, and computer-assisted personal interview (CAPI). Professional surveyors conducted 30- to 40-minute face-to-face interviews with 50,000 workers from 50,000 households (1 per household). Based on the household list, households were visited following the set contact order. The maximum number of visits for each household was six, each with different days and hours (twice on weekdays, four times on weekends).
Records of response rates and other statistics are core measurement indicators that allow the quality of the survey to be assessed. The KWCS uses a seven-code recording method, based on the definitions of The American Association for Public Opinion Research (2016). Using this coding system, the response rates, cooperation rates, refusal rates, and contact rates for the KWCS were calculated (Kim et al., 2013). In the Fifth KWCS, the cooperation rate was 64.0%, the contact rate was 72.1%, the refusal rate was 25.3%, and response rate was 44.9% (primary sampling: 130,645, excluded data: 80,440). The 2017 KWCS collected final data from 50,205 representative of the working population (Kang et al., 2019; Figure 1). The validity and reliability of the 2010 KWCS, which used the same study design as the 2017 KWCS, were evaluated, and the quality of the survey was assured (Kim et al., 2013). Therefore, KWCS’s demographic data show the extent to which the results of a study can be generalized to the overall Korean population.
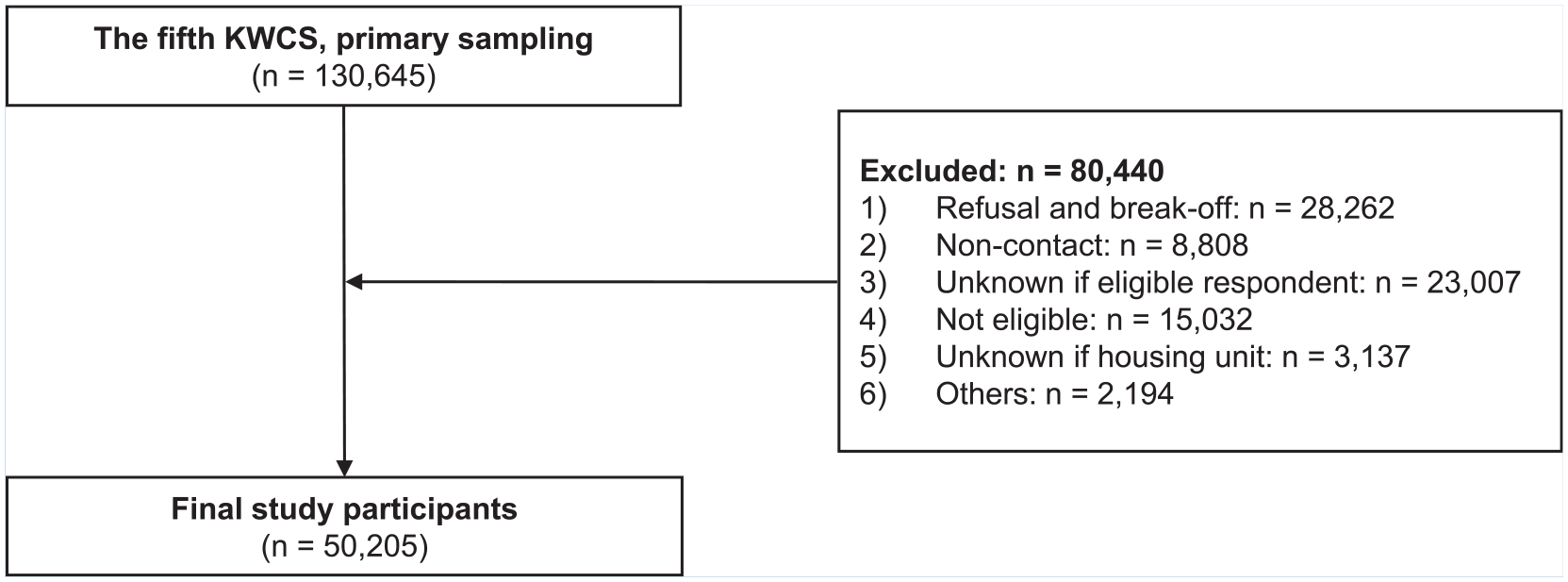
Schematic diagram depicting study population.
The KWCS comprises nationally approved statistical data available to the public (approval number: 380002), with safeguards to protect the participants’ anonymity and privacy rights. This study was exempted from the need to obtain approval from an institutional review board.
The general population characteristics collected were gender, age (<30, 30–39, 40–49, or ≥50 years), education level (≤high school, bachelor, or ≥master), monthly income (<US$776, US$776, <US$1553, ≥US$1553; US$1 = 1,300 won), and subjective health status (good or poor). The work-related characteristics consisted of workplace size (<30, 30–99, or ≥100 employees), number of years working at present workplace (<3, 3–5, >5–10, >10 years, or unknown), weekly hours worked (<35, 35–45, ≥46 hours, or unknown), shift work (yes or no), received health and safety education (yes or no), and job sector. For this we used the ISCO-08 (International Standard Classification of Occupations) by the National Institute for Occupational Safety and Health (NIOSH) which comprises the following major groups (Choi et al., 2020): managers (legislators and senior officials, etc.); professionals (accountant, lawyer, doctor, etc.); engineering professionals; clerical support workers; service workers (police officer, prison guard, hairdressers, cabin crews and workers in restaurants, etc.); sales workers; skilled agricultural, forestry, and fishery workers; craft and related trade workers; plant and machine operators and assemblers; general labor (guard, cleaner, caretaker, car park attendant, etc.); and armed forces. Participants could also give the following responses “unknown,” “no response,” or “refused to respond.”
Workplace violence was defined as experiencing verbal abuse and threats in the past 1 month, and physical violence and sexual harassment in the previous 12 months. Participants could choose between the following responses: “yes,” “no,” and “unknown, no response, or refused to respond.” Participants who answered “yes” were classified as experiencing WPV and were further asked about the perpetrators of the type of violence they experienced; multiple responses were allowed. Perpetrators of violence included customers (clients, students, and patients) and/or colleagues (boss, colleague, and subordinates). The professional surveyor explained the definition of each type of WPV to participants and collected the responses. The definitions were (Boyle & Wallis, 2016) (a) verbal abuse: a person’s perception of being personally attacked through spoken words. In this study, bullying and harassment were combined with verbal abuse; (b) threat: the behavior of an intention to inflict pain, injury, damage, or other hostile action on someone; (c) physical violence: attempts to cause physical harm; and (d) sexual harassment: unwanted verbal, non-verbal, or physical conduct of a sexual nature with the purpose or effect of violating the dignity of a person. In this study, unwanted sexual attention was combined with sexual harassment.
Assessment of mental health included anxiety, sleep problems, and depressive symptoms. Anxiety and depressive symptoms were assessed using the following question: “Have you had any of the following problems during the past 12 months?” Participants could choose between the following responses: “yes,” “no,” and “unknown, no response, or refused to respond.” Participants who had experienced anxiety and depression were defined as anyone who responded “yes.” Sleep problems included difficulty falling asleep, waking up often, and waking up feeling exhausted or extremely tired. All sleep problems were assessed in the past 12 months before the survey. Participants could choose between the following responses: “every day,” “several times a week,” “several times a month,” “rarely,” “none,” and “unknown, no response, or refused to respond.” Participants whose answers were “every day,” “several times a week,” and “several times a month” were classified as experiencing sleep problems.
Physical health assessed included back pain, headache/eye strain, and overall fatigue. Each physical health variable was assessed in the past 12 months before the survey. Participants could choose between the following responses: “yes,” “no,” and “unknown, no response, or refused to respond.”
Data Analysis
All statistical analyses were conducted using SPSS version 26.0 (SPSS Inc., Chicago, IL). In the sampling process, bias may have arisen due to differences in the population structure of the survey districts. Therefore, the KWCS conducted weighted adjustments similar to the population norms of South Korea (Seo, 2016). Weights distributions by region, locality, size, gender, age, economic activity, and occupation were identical to those of the overall economically active population at the time of the survey. Descriptive statistics were used to calculate the proportions and 95% confidence intervals (CIs) of each experience of WPV by general characteristics. Multiple logistic regression analyses were conducted to (a) examine the association of WPV and mental health and (b) examine the association of WPV and physical health, then odds ratios (ORs) and 95% CIs were calculated. Multiple logistic regression analysis was used after adjusting for gender, age, education, monthly income, subjective health status, workplace size, working period at present workplace, weekly working hours, shift work, health and safety education, and job sector. Depressive symptoms were investigated after additional adjustments for anxiety and sleep problems.
Results
Table 1 shows that of the 50,205 workers investigated, 4.9% reported experiencing verbal abuse at work, and 0.7% reported experiencing threats. In addition, 0.2% reported physical violence, 1.1% reported sexual harassment, and 5.6% reported one or more of these experiences. Workers with less than a diploma reported a higher prevalence of WPV than those with more education.
Experience of Workplace Violence (WPV) in a Korean Population Sample by Subjects’ Demographic and Health Characteristics (n = 50,205)
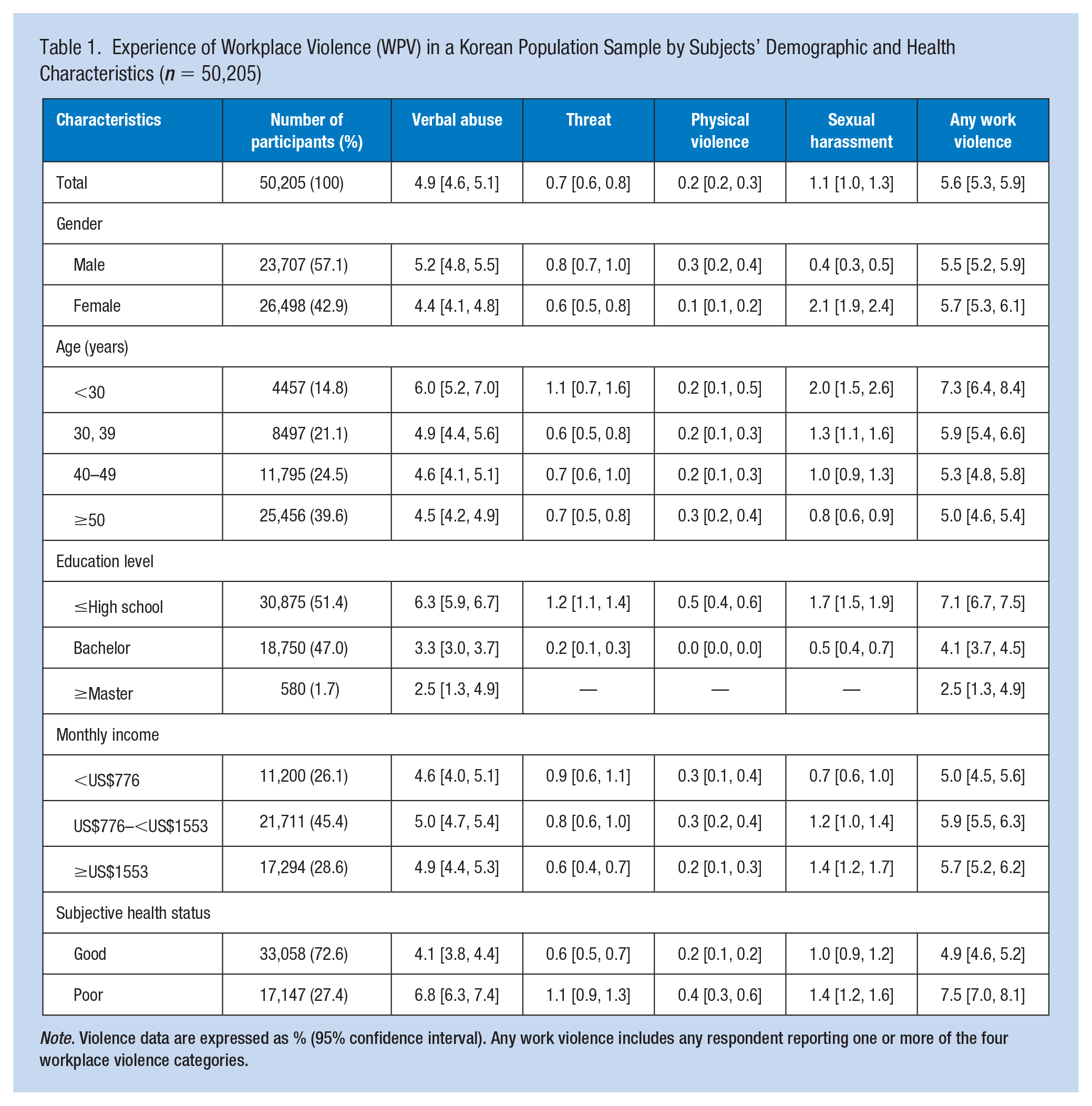
Note. Violence data are expressed as % (95% confidence interval). Any work violence includes any respondent reporting one or more of the four workplace violence categories.
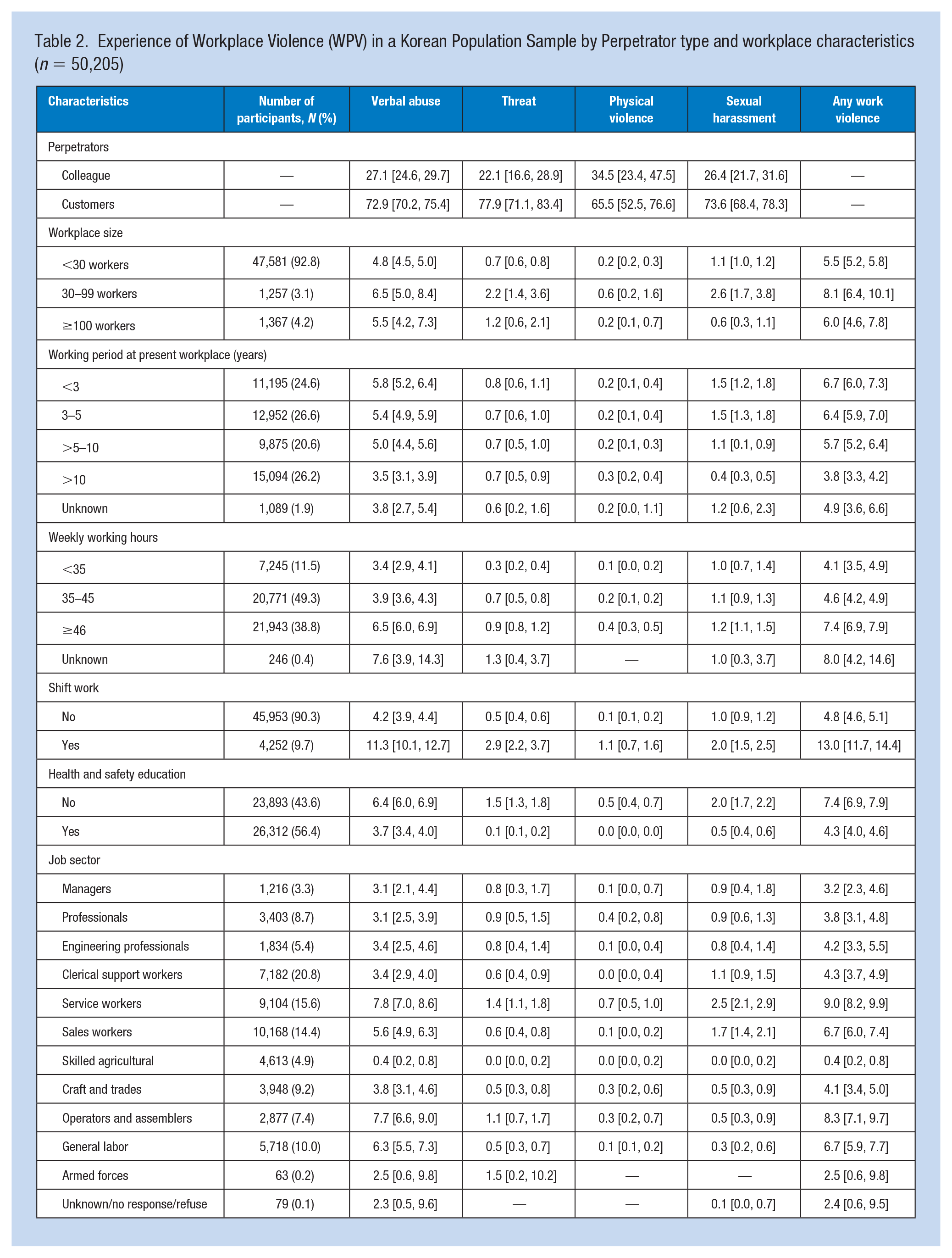
Table 2 shows that the proportion of customers that were reported as the perpetrator was higher than the participants’ colleagues regardless of the form of violence. Workers with <35, 35–45, and ≥46 working hours per week reported experiencing violence in 4.1%, 4.6%, and 7.4%, respectively. In addition, shift workers and those with no experience of health and safety education had a higher prevalence of WPV than workers who did not. Among service workers, 9.0% reported one or more violent experiences.
Experience of Workplace Violence (WPV) in a Korean Population Sample by Perpetrator type and workplace characteristics (n = 50,205)
A significant number of the study population had mental health problems associated with violence experienced at work: 3.1% had anxiety, 52.3% had sleep problems, and 2.4% had depressive symptoms (Table 3). Compared to those workers who did not experience WPV, workers who experienced verbal abuse were more likely to report anxiety, adjusted odds ratio (aOR) = 4.41, 95% CI = 3.64–5.34, sleep problems (aOR = 2.06, 95% CI = 1.82–2.34), and depressive symptoms (aOR = 4.84, 95% CI = 3.95–5.94). Threats, physical violence, and sexual harassment were associated with an increased odds ratio of anxiety (aOR = 7.58, 7.33, 4.41, and 4.24, respectively). In addition, threats and physical violence were associated with an increased odds ratio of sleep problems and depressive symptoms
Result of Multiple Logistic Regression Analysis of the Associations between Experience of Workplace Violence and Mental Health (n = 50,525)
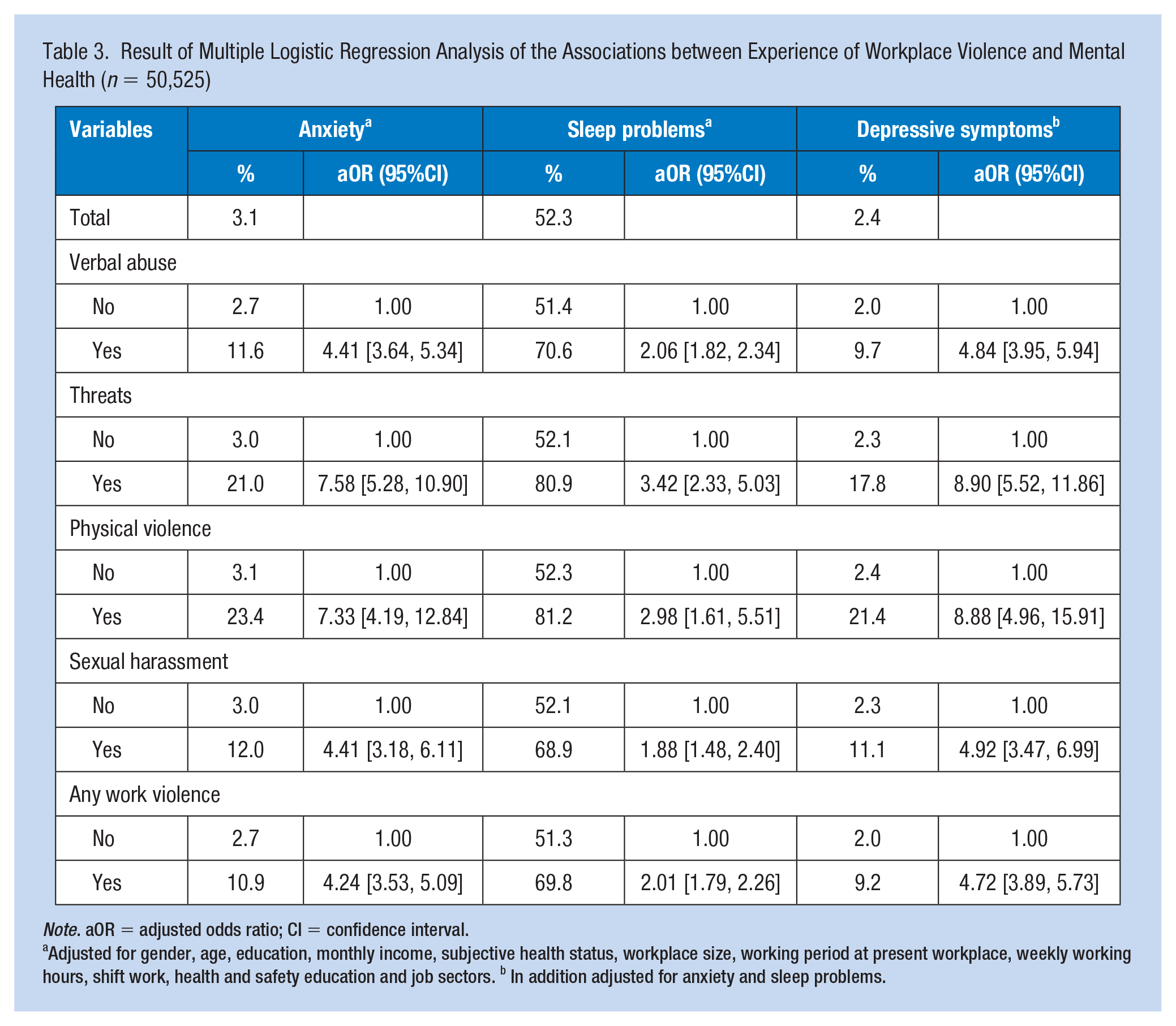
Note. aOR = adjusted odds ratio; CI = confidence interval.
Adjusted for gender, age, education, monthly income, subjective health status, workplace size, working period at present workplace, weekly working hours, shift work, health and safety education and job sectors. b In addition adjusted for anxiety and sleep problems.
Physical health problems were reported among the workers experiencing violence at work (Table 4). About 11.5% reported having back pain, 13.4% had headache/eye strain, and 23.4% had overall fatigue. Verbal abuse was associated with back pain, headache/eye strain, and overall fatigue (aOR = 2.73, 2.49, and 2.59, respectively). In addition, threats, physical violence and sexual harassment were associated with an increased odds ratio of back pain, headache/eye strain, and overall fatigue.
Result of Multiple Logistic Regression Analysis of the Associations between Experience of Workplace Violence and Physical Health (n = 50,205)
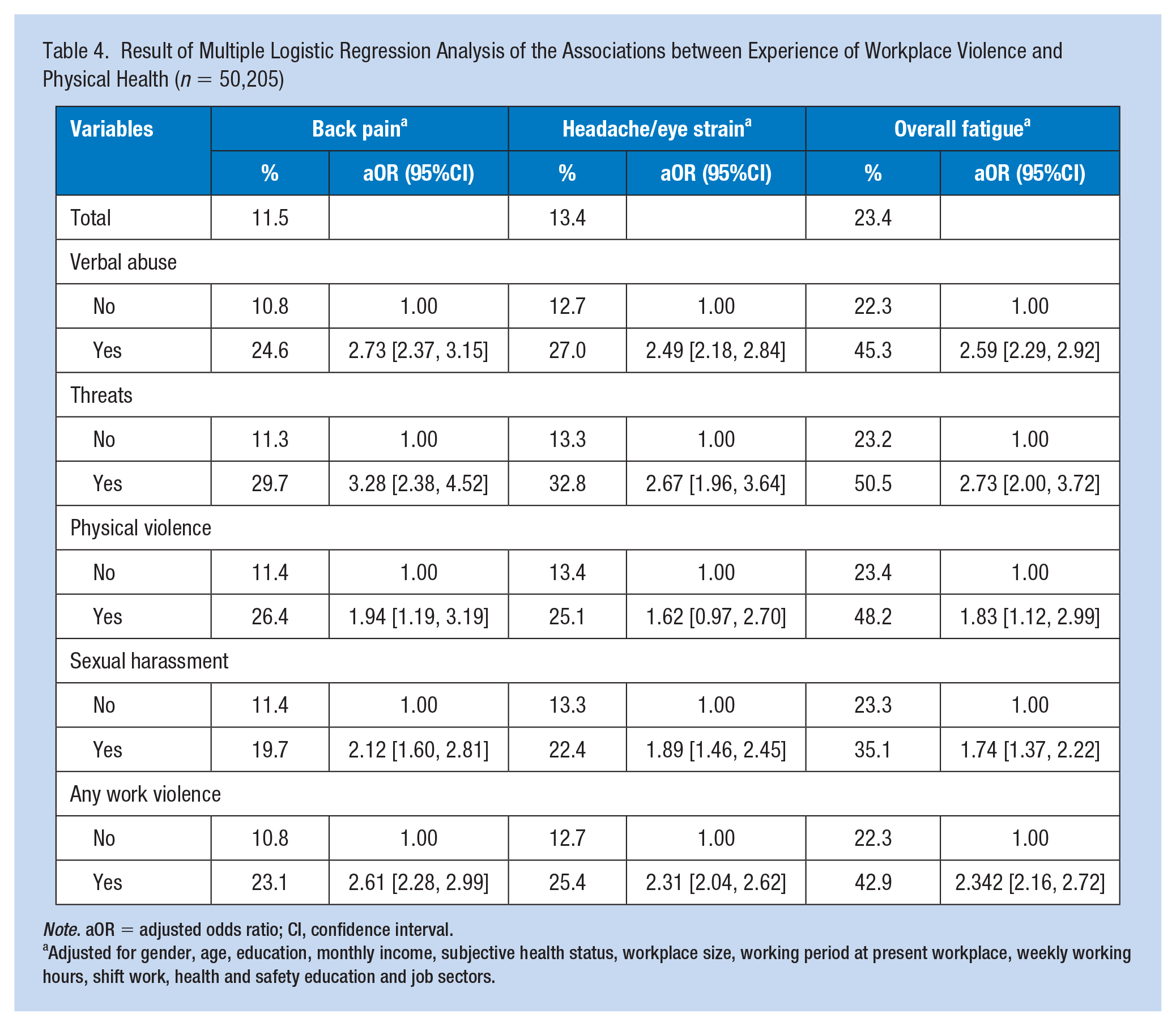
Note. aOR = adjusted odds ratio; CI, confidence interval.
Adjusted for gender, age, education, monthly income, subjective health status, workplace size, working period at present workplace, weekly working hours, shift work, health and safety education and job sectors.
Discussion
According to this study, 4.9% of Korean workers reported experiencing verbal abuse, 0.7% threats, 0.2 % physical violence, and 1.1% sexual harassment. In the Sixth EWCS, workers reported experiencing verbal abuse, threats, physical violence, and sexual harassment at 12%, 4%, 2%, and 1%, respectively (Eurofound, 2017). The results of this study showed a lower prevalence of WPV compared with the results of EWCS; however, there was no improvement compared with results of the 2011–2014 KWCS (Hwang et al., 2020). The methodology and questionnaire used in the KWCS were the same as those used in the EWCS. For this reason, the difference in the prevalence of workplace violence between KWCS and EWCS is probably not due to differences in the definition and measurement methodology of workplace violence (Kim, 2017). It may be due to differences in organizational culture or national policy. Korean culture traditionally values the group rather than the individual, and demands patience and concession, this may explain why reports of workplace violence may be lower in Korea than in Europe (Hong et al., 2019; Jung et al., 2015). In Korea, legal definitions for assault, sexual harassment, and bullying have been provided under the Labor Standards Act, but the financial and administrative burdens are on victims who seek restitution (Mun, 2016). This may be why workers are reluctant to report experiences of WPV, and it is not improving. Furthermore, many WPV victims do not want to report WPV officially for fear of retaliation (Mun, 2016; Yoo et al., 2018). It is necessary to improve the current reporting system in order that workers can report WPV without fear of retaliation. It is important to establish an appropriate official reporting system—in order to develop appropriate programs to reduce the risk of chronic verbal and physical violence (Lu et al., 2019).
Consistent with previous studies (Lu et al., 2019; Saberi et al., 2019), the highest rates of violence in the KWCS were verbal abuse and the lowest rates were from physical violence. This is significant because both verbal and physical violence have been reported to be associated with poor health status (Hwang et al., 2020; Pien et al., 2019).
In previous studies, WPV was shown to increase with lower education levels (Havaei et al., 2020; Kim & Yoon, 2017), poor subjective health status (Zhang et al., 2018), and long work hours (Cavalcanti et al., 2018; Hwang et al., 2020). Although the definitions and categories of WPV are different, this study’s results are consistent with previous results. Job dissatisfaction and negative emotional experiences from WPV were associated with workers’ harmful health outcomes (Duan et al., 2019; Zhang et al., 2018). However, in studies of medical staff and emotional laborers, it was reported that higher education levels were more likely to experience WPV (Hong et al., 2019; Hwang et al., 2020; Li et al., 2017). According to a study based on the EWCS data, unwanted sexual behavior was more often reported by workers who were highly educated and had fewer working hours (Reuter et al., 2020). This result suggests that the impact of education level and working hours on violence differ by job sector or type of violence, and further study is needed.
Consistent with previous studies (Cavalcanti et al., 2018; Hong et al., 2019), shift workers were more likely to report WPV. Shift work refers to outside of daytime, including irregular or rotating schedules, shift work is common in Korean health care facilities (Kim et al., 2017). It may be a risk factor for WPV among Korean health care workers. Organizational interventions to improve shift schedules might help prevent WPV in health care workplace (D’Ettorre et al., 2019). Without regular WPV prevention programs, including those involving management and employee participation, worksite analysis, hazard prevention and control, safety and health training, and recordkeeping and program evaluation, workers have a limited ability to communicate their safety and health risks to leadership (Arbury et al., 2017). Education programs that seek to promote healthy and safe working environments and focus on the effects, prevention, and responses to WPV may increase workers’ ability to respond to violence in the workplace (Havaei et al., 2019). In Korea, WPV prevention education is provided to workers in accordance with the Occupational Safety and Health Act, but it has been reported that organizational awareness regarding WPV is insufficient (Seo & Park, 2017). Campaigns that increase awareness regarding the risks of WPV and improve workplace culture, relevant education, and policies are necessary.
Service work, including police service, prison service, hairdressing, cabin crew service, and restaurant work, imposes a huge emotional burden and causes burnout wherein even minor communication issues may expose workers to violence (Kim & Yoon, 2017; Shier et al., 2018). Since the rate of violence correlates with customer-contact time, emotional laborers are exposed to verbal and physical violence in their interactions with customers (Saleem et al., 2020). Interventions including appropriate workload intensity, consumer risk assessment, occupational stress management programs, and violence management team activation may help to prevent WPV (Morphet et al., 2018).
This study found customers to be the main source of WPV, which is a similar finding to the Fourth KWCS (Yoo et al., 2016). Experiences of violence among health care and customer-care workers were characterized by either verbal or physical assaults perpetrated by patients and visitors (Cavalcanti et al., 2018; Chang & Cho, 2016). They are expected to interact with patients and customers, and if this interaction does not go well, they may be subjected to complaints, verbal abuse, or even unreasonable demands from the customers or patients (Morphet et al., 2018; Robertson & O’Reilly, 2020). Organizational support may reduce WPV perpetrated by customers. For example, employers’ collaborative problem-solving activities may help increase awareness of violence among health care workers and violence-prevention strategies for aggressive patients or visitors (Havaei et al., 2019; Saleem et al., 2020). According to a scoping review, customer risk assessment and aggression-management teams also may help reduce the incidence of violence (Morphet et al., 2018). According to a study of nurses in a hospital in Korea, it was reported that the violence coping system and managers’ active response may prevent violence by patients (Yoo et al., 2018). However, violence prevention and response systems are not common in Korean workplaces (Mun, 2016). Only legal regulations prevent physical assault, sexual harassment, and bullying by customers are stipulated, and there are limits to protecting workers from violence (Mun, 2016). Improvements in the legal system may help to improve health care workers protection from WPV by customers and patients in Korea (Baek, 2019).
In this study, WPV was negatively associated with poor mental health among Korean workers. Consistent with previous studies (Cheung & Yip, 2017; Friis et al., 2019; Shi et al., 2020), this study found that physical and non-physical violence increased the risk of anxiety and depression compared to non-exposed workers. In addition, sleep problems were the most frequently reported among workers with WPV. Chronic occupational stress from WPV may cause sleep complaints through hormone reactions such as cortisol or hypothalamic-pituitary-adrenal axis activation (Eddy et al., 2018). Consistent with previous studies, WPV was associated with back pain, headache/eye strain, and overall fatigue among Korean workers. In a Chinese study, chronic multisystem illness including headaches, multi-joint, and muscle pain was 1.3 times higher in nurses with WPV than those not exposed to violence (Li et al., 2020). WPV may also exacerbate musculoskeletal disorders among Korean emotional-labor workers (Kim & Choo, 2016). Although some epidemiological studies of the prevalence and health consequences of WPV have been conducted (Ceballos & Carvalho, 2020; Park & Kim, 2020), they are limited for understanding the mechanisms for such associations. This would require a large study that involved repeated observations of the same variables over long periods of time, given the high prevalence of poor physical health outcomes among workers exposed to WPV. If not solved at an earlier stage, mental problems cause by the WPV may lead to harmful health outcomes, affecting workers’ physical and psychological functioning (Fordjour et al., 2020). Employers’ awareness of the impact of WPV on workers’ health outcomes and support of workplace health management strategies may improve the mental and physical damage caused by WPV (Attridge, 2019).
The cross-sectional design of the study presents some limitations. The KWCS used two time periods (1 month and 1 year) according to the type of workplace violence. Physical and mental health data were defined by experience during the past year. The study could not avoid the limitation caused by using these two time-periods in the operational definition of WPV and dependent variables. Due to the cross-sectional nature of the study and the differences in time-period, the study was not able to assess the direct causal relationship between WPV and physical and mental health. In addition, the one-time survey for WPV during the past 12 months or 1 month may lead to recall bias, and the health effects of WPV may attenuate with time (Pien et al., 2019). To identify the causality or temporal association between WPV and health problems, further longitudinal studies should be performed. However, considering that previous studies reported that WPV was a cause of musculoskeletal disorders (Choi et al., 2018) and psychosocial functioning (Eyasu & Taa, 2019), and looking at the mechanism by which various experiences of WPV cause poor health conditions (Fisekovic Kremic et al., 2016; Jung et al., 2015), the association between WPV and physical and mental health may be understood. Second, this study was based on the KWCS, which is a self-report questionnaire. Therefore, there was a possibility of an information bias. For example, workers with poor mental health might over-report on WPV, leading to a possible overestimation of the association of mental health and violence (Hogh et al., 2016). Third, mental and physical health is also associated with occupational characteristics, work environments, and supervision factors, but since these were not investigated, their effects are unknown. In addition, health variables were not measured using a standardized instrument, which may affect the prevalence of health problems (Lee et al., 2018). Further studies are needed to account for these factors. Fourth, the healthy-worker effect may cause a potential selection bias (Chowdhury et al., 2017). For example, since a worker experiencing WPV may leave work, and healthy workers tend to remain in the workforce, this study may not reflect the possible experiences of all workers. Finally, because of data limitations, it was difficult to assess whether WPV caused mental or physical health problems among the workers, or if the health problems preceded the violence. Workers with poor health are more likely to experience negative effects after exposure to WPV than healthy workers (Park & Kim, 2020). Therefore, this study suggests that longitudinal studies with several measurement points over an extended period are necessary to identify the dynamics between WPV and health problems.
Implications for Occupational Health Practice
This study investigated the prevalence and risk factors of workplace violence among Korean workers and the association between WPV and mental and physical health, using nationally representative data. High prevalence of WPV was associated with lack of safety and health education, poor subjective health status, long working hours, shift work, and service workers. Compliance with legal working hours, safety and health monitoring for shift workers and workers with patient and customer interaction, a zero-tolerance policy for perpetrators, and continuing education may help to protect workers from WPV. Employers must take preventive action in a collaborative manner, such as accepting an employee’s suggestions to control and illuminate the potential of violence. Our findings showed that workplace violence has a statistically significant association with mental and physical health, highlighting the need for developing intervention programs that prevent WPV and protect workers’ safety and health. It is also crucial to implement programs that stabilize and heal workers who are impacted from unfair verbal abuse, threats, physical violence, and sexual harassment. KOSHA made recommendations for a workplace violence-prevention guide in Korea. The practical implication of this study is the need to develop policies including penalizing perpetrators and post-exposure support at the national level.
Applying Research to Occupational Health Practice
Workplace violence is prevalent in all industries studied in this representative sample of Korean workers. There is an association between WPV and mental and physical health problems. Although many Korean workers suffer from workplace violence, currently there are no specific regulations requiring employers to institute workplace violence prevention programs. Workplace Violence should be considered a public health crisis in Korea and legal policy approaches may be effective in its reduction. Occupational health professionals can utilize the evidence to advocate for improved reporting systems, preventive education and counseling, and health-support programs for the recovery of workers exposed to violence. Also, knowing that perpetrators are mostly customers should encourage employers to enact strict policies or guidelines.
Footnotes
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Hae Ran Kim is currently an assistant professor in Department of Nursing at Chosun University, South Korea. Her research interests are health statics nursing education, and health promotion for vulnerable population.