
Abstract
Background: Workplace violence has a significant impact on patients, families, and staff safety. Workplace violence can produce traumatic results for those involved; the importance of preventive measures needs to be paramount in health service policy and process. Health care staff are required to document their experiences of violent incidents after every occasion, usually via an incident reporting system, which allows for a free text description of the event. There is a lack of understanding of how health care staff document reports of violence and how they explain the events. Methods: This study aims to determine the circumstances surrounding workplace violent events as documented by health care staff. The four-step Review, Extract, Analyze, and Document (READ) approach to document analysis was used to examine workplace violence incident reports over 12 months (September 2021–September 2022) in a tertiary referral hospital. Findings: Six categories of workplace violence were found: (a) “Escalation Dynamics”—patterns and progression of how violence incidents intensify; (b) “Warning Behaviors”—verbal or non-verbal signals that may foreshadow physical violence if not addressed; (c) “Authoritative Institutional Interventions”—how aggression correlates to protocols involving security personnel or law enforcement; (d) “Care Delivery Methods”—how certain treatment procedures and approaches might inadvertently elicit violence; (e) “Situational Stressors”—external circumstances or changes that act as triggers for violence; and (f) “Unprovoked triggers”—sudden and seemingly unprovoked violent outbursts. Conclusions and application to practice: Workplace violence in health care is a multifaceted interplay of events with the nurse involved in all aspects of the process. These findings can be used by occupational health nurses in education and policy development. The findings can be used to focus education on how violent incidents may escalate and provide more opportunities for de-escalation by health care staff.
Keywords
Background
Workplace violence (WPV) in health care remains highly prevalent and constitutes a major concern to patient safety (Hou et al., 2024). The phenomenon is defined as, “Incidents where staff are abused, threatened or assaulted in circumstances related to their work, including commuting to and from work, involving an explicit or implicit challenge to their safety, well-being or health” (International Labour Office, 2002, p. 3). In a recent meta-analysis of 14 studies, the overall prevalence of violence was as follows: WPV (58.7%); physical violence (20.8%); verbal violence (66.8%); and sexual harassment (10.5%; Sahebi et al., 2022). For occupational and environmental health nurses, WPV remains a key focus in their workplace (Byon et al., 2023). The literature on WPV highlights the significant negative behavioral, emotional, cognitive, and physical outcomes for health care staff, such as anxiety, stress, physical injury, decreased job satisfaction, and poor organizational commitment (Kumari et al., 2022; Mento et al., 2020). Most research into WPV in health care focuses on its prevalence with little effort into understanding the experience as documented and the harm caused to health care staff (Liu et al., 2019). In most contemporary health care services, serious adverse events are recorded in incident management systems. These incident reports are then used to develop and inform health care policy, systems and processes, education, prevention and management systems (Ramírez et al., 2018). Limited research has been conducted into the impact and use of WPV incident reports in tertiary referral hospitals.
In an international meta-analytic study of the prevalence of WPV, 61.9% of staff reported any exposure to WPV, with 24.4% reporting physical violence in the preceding 12-month period (Liu et al., 2019). Noticeably, WPV gained prominence during the COVID-19 pandemic, with reports of violence toward health care staff increasing during the period of lockdown and the restrictive nature of public health orders (Chirico et al., 2022; Stewart et al., 2020). These high prevalence statistics confirm the need for an ongoing effort to prevent and manage WPV in health care These prevention efforts need to mitigate the risk of physical harm toward health clinicians who are likely to experience WPV while providing care.
Reviews of WPV incidents in health care have primarily focused on mental health and emergency department services where violence is reportedly more prevalent (Aljohani et al., 2021; Drori et al., 2017; Gillespie & Berry, 2023). In a study from a mental health unit in Israel (Drori et al., 2017), 80 WPV incidents were reviewed; 70% included physical violence with most cases directed at a single health care staff member. Patients who were displaying violence were described as agitated, male, experiencing hallucinations, and suffering from depression. Recommendations from the study included increased awareness, knowledge of risk factors and patient histories, not working in isolated areas and reducing crowding in ward areas. In a systematic review of 26 studies of violence in emergency departments, 72% involved cases of verbal abuse, 18% related to physical abuse, with perpetrators described as family members 52%, patients 27%, and 21% other friends or relatives (Aljohani et al., 2021).
A further focus on capturing risk factors for WPV in patients was seen in the following two studies. In the United Kingdom, a study of 1,422 incidents in 84 mental health wards (Renwick et al., 2016) described risk factors associated for WPV perpetrated by younger males with substance use issues and psychosis. In this study, patient–staff interactions were thought to have led to a sizable portion of WPV incidents. Limited research exists that explores patient–staff interactions that lead to WPV. In a forensic mental health hospital in Finland, a review of 840 WPV incidents showed higher risks for violence in voluntary/civil patients versus criminal patients, with over half the incidents reported considered to be unexplained (Kuivalainen et al., 2014).
These studies primarily used quantitative methods to elucidate the frequency of violence and highlight at-risk individuals. However, they do not explore the nuances of how staff describe WPV incidents, such as those including patient–staff interactions. In an emergency department study of 38 incidents in the United Kingdom, 25 incident reports were found to be incomplete or lacking sufficient details, and further qualitative semi-structured interviews with staff found that many WPV incidents went unreported (Ferns, 2012). A critical discourse analysis of WPV incidents conducted in Denmark (Berring et al., 2015) in a forensic mental health service aimed to examine how mental health staff construct accounts of WPV via incident reports. This qualitative study reported that staff found that the WPV incident itself led to the stereotyping of forensic psychiatric patients as deviant, unpredictable, and dangerous. In a qualitative study of non-mental health patients in a general hospital (Arnetz et al., 2015), an analysis of 214 WPV incidents reported three themes: patient behavior, patient care, and situational events. The study led the authors to identify catalysts to WPV incidents, such as patient pain, discomfort, physical transfer, and cognitive impairment. This level of qualitative analysis may lead to a deeper understanding of the social interactions between patients, staff, family, and the broader health care system.
An analysis of incidents experienced by health care staff directly affected by WPV could potentially show insight into various social interactions that influence this phenomenon. Descriptions of the social interactions between patients, staff, and family/carers are difficult to understand through quantitative survey results or epidemiological data. Qualitative interviews with perpetrators of violence in health care pose significant ethical challenges as individuals may have had a cognitive impairment or may be engaged in grievance processes with health care systems. In each of these possible scenarios, the perpetrators as research participants are highly vulnerable. Documented descriptions are largely socially constructed and provide a safer avenue to retrospectively explore the social interactions between patients, staff, carers/families, and organizational systems. The aim of this study is to understand the circumstances surrounding workplace violent incidents as documented by nursing professionals on an incident database in the tertiary referral hospital.
Guiding Frameworks
The SQUIRE checklist (Attachment A) was applied in line with EQUATOR guidelines as a framework for the study (Ogrinc, 2015). The SQUIRE guidelines provide a framework for the reporting new knowledge in health care research settings. These guidelines guide authors in how to describe system-level work that aims to improve the quality, safety, and value of health care service (Ogrinc, 2015). This study is reported using these guidelines. For example, the SQUIRE guidelines recommend that the “Introduction” section includes the problem description and available knowledge (e.g., prevalence of WPV in health care), and the “Discussion” section should describe limitations (e.g., the study was only conducted in one site).
Methods
Prior to the conduct of the study, ethical approval was sought and received from Southeast Sydney Local Human Research Ethics committee on the February 21, 2023, ethics number 2023/PID00207 as a low-negligible risk study. All data were de-identified before being analyzed by the researchers, and care was taken to screen each incident description that was studied to ensure there was no identifying information given by the nurse. If any identifying information was found, it was removed before analysis.
Study Setting
The study was set in a 400-bed tertiary referral metropolitan hospital in Australia. The study site offers a wide range of clinical specialties, and approximately 50 different clinical service units including the following: Emergency department, neurosciences, mental health, medical, surgical, spinal units, operating theaters, aged care, and several other smaller specialties. The site has a 24-hr clinical violence response team comprising nursing, medical, ward persons, and security officers. All staff from the high-risk areas are required to attend a 1-day training covering violence assessment and management which has been evaluated elsewhere (Lamont & Brunero, 2018). All clinical staff from across the hospital are required to complete two online education modules covering legal issues and personal safety awareness. Violence-related tabletop exercises are also conducted using a simulated discussion of a violent incident in each of the clinical units annually (Brunero, Dunn, et al., 2021). All violent incidents are required to be reported via an incident management system. Violent incidents are defined as verbal or a physical threat to objects or others. All incidents that occur are discussed at patient safety huddles, and the staff member involved in the incident is allocated to document the incident, which usually occurs at the end of each shift.
Using the READ Approach
The four-step Review, Extract, Analyze, and Document (READ) approach to document analysis was followed systematically and includes “(a) read your materials, (b) extract data, (c) analyze data, and (d) distill your findings” (Dalglish et al., 2020, p. 1424; see Table 1 for description of steps used).
Description of Steps Used in the READ Approach Adapted From the Work by Dalglish et al. (2020)
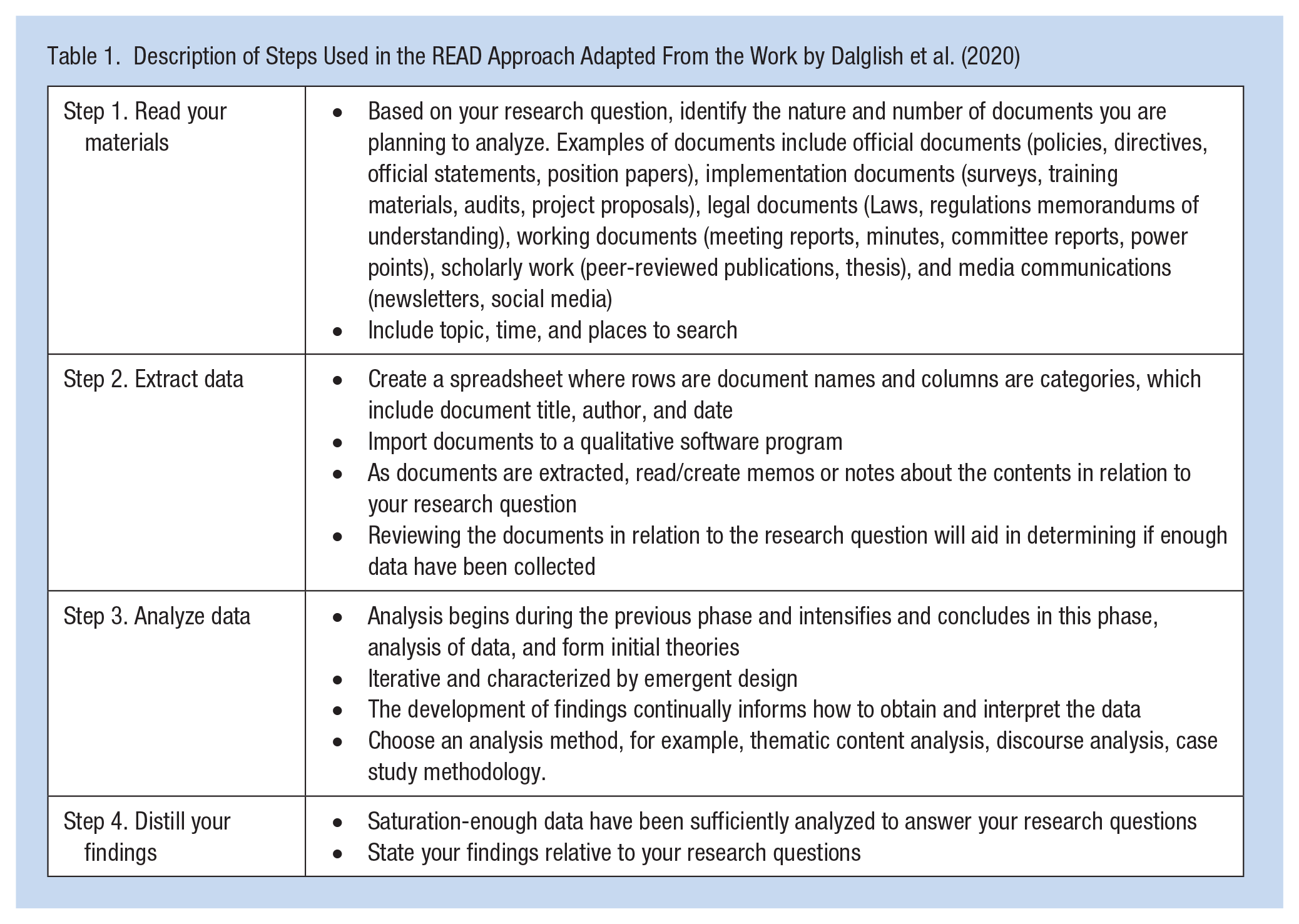
During the first step, the authors, who are clinicians involved in WPV management, readied the materials as they considered the availability of documented material which would address the study aim. Consideration was given to examine medical records and incident reports which are collated separately from the medical record. The incident report system was chosen as the source of the data as it provided a succinct description of the WPV event. These incident reports are also used in the organization’s review processes including the mandatory reporting process for each incident attached to them in which clinicians describe specific outcomes resulting from the incidents. The incident reports were seen as a more powerful influence on the practice of WPV prevention in the organization than other records of violence, such as medical records. The reports containing 775 WPV incident descriptions between September 2021 and September 2022 were included for analysis. However, 12 months was chosen as the time interval because these incidents cover high and low seasonal hospital admission rates at the study site.
Step 2 involved extracting the data from the incident reporting system. The incident reporting system is a standalone database that clinicians enter event descriptions into after an incident. These incidents descriptions are subject of review, investigation, and presentation at organizational governance meetings with key performance indicators for the organization. The WPV incidents were downloaded from the incident database to an excel spreadsheet and were de-identified during this process. Each incident was assigned a de-identified random unique identifier. The free text incident description, immediate actions, and outcomes of incident (also free text) were collected, usually containing approximately three to four sentences of description per incident. There is no clinical diagnostic information nor gender recorded on the incident. The incidents across the hospital were analyzed as a whole and were not broken down into specialty areas.
Step 3 involved analyzing the data. Inductive content analysis was chosen to analyze the incident descriptions (Elo & Kyngäs, 2008). Inductive content analysis is frequently used in health care to understand the meaning behind written descriptions. Inductive content analysis is an iterative process where codes are used to label relevant data identified during the analysis. The process included open coding, creating categories and abstraction. During open coding, the first and second author wrote notes and headings as the incident reports were read and re-read. “Memoing” was used during the analysis to assist the researchers in making conceptual leaps from the early open coding through the abstraction to the final theme development (Birks et al., 2008; Charmaz, 2014). Memoing included the researchers documenting ideas and conceptualization of categories as they read and re-read the incident descriptions. Categories began to emerge from the open coding done by the first and second authors. These categories were grouped and developed into higher-order categories. The next step, abstraction, included formulating general descriptions of the main categories of the WPV incidents (Elo & Kyngäs, 2008; Vears & Gillam, 2022). This process continued until the first and second authors came to agreement on the final theme.
The quality and rigor of the study was determined by following Stenfors et al.’s (2020) five criteria for rigor in qualitative research (credibility, dependability, confirmability, transferability, and reflexivity). First, to determine credibility, the study’s aim, method, analysis, and result need to align. All the authors individually reviewed the study process to ensure alignment. During a consensus meeting post this independent review, the authors came to agreement on the alignment of the study. Second, during an author meeting the dependability or ensuring sufficient information provided, so another researcher could follow the same process and be replicated was clearly documented and recorded. Third, confirmability or the demonstration of a relationship between the data and findings was shown by having key quotes from the dataset in the “Findings” section. Fourth, transferability was achieved by the detailed descriptions in the “Method” and “Findings” section of this case allowing other readers of the research to transfer the findings or not to their own setting. Finally, reflexivity or the place of the researchers and the context of the research; the first and second authors are clinically involved in the hospital emergency response systems attending violent incidents, the second and third authors have extensive experience in their clinical specialties, acute care and aged care, with violent behaviors. These insights enabled an analysis of the data from an insider’s perspective, allowing a deeper understanding of the dataset as the authors, a part of the process, were involved in WPV at the study site.
The last stage, “distill your findings” (Dalglish et al., 2020, p. 1430), included ascertaining that enough data had been analyzed to address the study aim and that the study duration was adequate. This stage included the formal writing of the study findings, discussion, and recommendations to the study site. Recommendations from the study have been escalated to the governance process at the study site. The hospital has a violence prevention committee which oversees all aspects of WPV, including education, policy, and review of critical incidents. The accountability for the recommendations now sits with this committee for action.
Findings
The total number of incidents reviewed was 775. This figure represents an unknown number of individual patients, as there may have been several incidents per patient during the hospital admission, which was a known limit of the database. The analysis of patient violent incidents revealed several categories related to the contexts, triggers, and patterns associated with violent behavior. Insights indicate that violent behavior in generalist health settings is multifaceted, influenced by risk factors, patient conditions, environmental factors, and the dynamics of interactions with health care staff. Understanding antecedents is crucial for developing strategies to prevent, mitigate, and manage violence in health care (McDougall, 2000). The findings were generated into six main themes; see Table 2, for themes and defining characteristics.
Themes Generated and Defining Characteristics
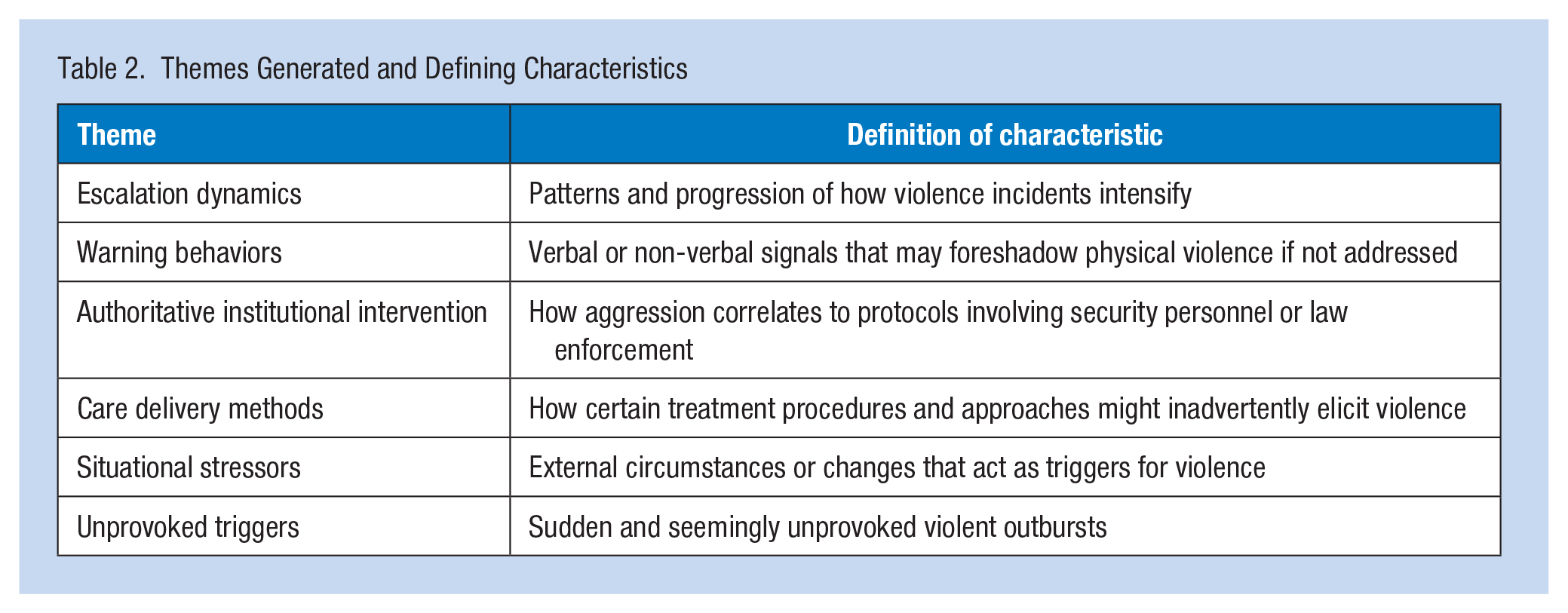
The narratives below are structured to succinctly describe the context, prevalence, and specific aspects of each theme.
Escalation Dynamics
A significant portion of the incidents (42%) escalated from verbal altercations to physical violence. In many incidents, what began as a benign interaction rapidly escalated. A typical scenario often started with a verbal disagreement between a patient and staff related to treatment or care, which intensified due to dissatisfaction regarding the trajectory or outcome of the interaction. One participant wrote, “A verbal dispute over medication dosage quickly escalated, with the patient throwing punches at the attending nurse”; another stated “The patient, initially arguing about the delay in discharge, suddenly lunged at the staff member, hitting them.”
On occasions, verbal altercations with staff were preceded by tensions arising from interactions with patients, family members, or disputes with other patients. Understanding the dynamics of these interactions is pivotal for health care practitioners to identify early warning signs and employ strategies to de-escalate the situation and prevent physical altercations. The transition to physical violence can follow recognizable patterns. The prevalence of these patterns underscores the critical importance of effective communication, conflict resolution, and de-escalation techniques in health care settings to prevent such escalations.
Warning Behaviors
Situations where patients verbally threatened or insulted health care staff often preceded physically violent behaviors (30.8%). Warning behaviors served as precursors to violence, manifesting as verbal threats or distinct non-verbal cues, such as clenched fists, raising hands, starting and gritting teeth, and pacing. One participant stated, “Following a series of verbal threats, the patient physically assaulted the nurse,” another stated “The patient’s aggressive behaviour began with pacing and insults and escalated to throwing objects at staff.”
Before an incident turned physically violent, patients often exhibited warning behaviors. These ranged from explicit verbal threats to subtle non-verbal cues, such as body language or facial expressions, for example, where people intensely stare, fold their arms, hold objects indicating a threat, and raised fists. This pattern indicates that verbal aggression can be an important early warning sign of escalating behavior and requires prompt and effective response to prevent further escalation. Training health care staff to recognize and respond to these early warning signs and signals early and appropriately is crucial in mitigating potential violence.
Authoritative Institutional Interventions
The involvement of security or law enforcement in violence emergency team response systems (e.g., Code Black-violence prevention team attendance) was associated with violent behaviors in 23% of incidents. These instances often involved the presence or intervention of security personnel or police, which in some cases, seemed to exacerbate the violent behavior. This suggests that the approach to involving security and law enforcement in health care settings requires careful consideration and potentially more nuanced protocols. There may be a link between violence and the representation of authoritative uniforms. For example, one participant wrote, “Upon the arrival of security personnel, the patient’s aggressive behaviour intensified, resulting in a physical altercation” and another nurse documented the following, “The involvement of police in managing the patient led to an escalation in aggression, with the patient becoming more combative.”
Attendance of security personnel or police in escalating situations may inadvertently provoke patients who are angry or fearful, rather than de-escalate situations. Although often necessary, or perceived so for safety, these interventions can significantly affect the dynamics of complex health care situations. Balancing staff safety with patient care is a delicate task, requiring well-defined protocols, response, and training.
Care Delivery Methods
The method of care delivery, including specific treatment procedures, can sometimes provoke violent reactions from patients. Violent behavior occurred during routine care activities in 11.8% of the incidents analyzed. These episodes often occurred during regular care procedures, possibly indicating that certain aspects of patient care or the way in which care is provided can act as catalysts for violence. For example, one person wrote “During a routine dressing change, the patient grew increasingly agitated and began to hit the nurse” and another wrote, “While assisting the patient with bathing, he suddenly became aggressive, pushing the staff member away.”
This finding highlights the necessity for human-centered care approaches and sensitivity to individual patient needs and preferences. Certain routine and invasive care activities can inadvertently distress patients, cause unintentional pain, and elicit violent reactions, if not conducted with adequate communication. Health care practitioners should be mindful that procedures perceived as invasive, painful, or violating personal boundaries should be handled with caution. Modifying treatment approaches and enhancing patient communication are key strategies to reduce such incidents.
Situational Stressors
Violence in health care settings is often precipitated by situational stressors or circumstances or changes that act as triggers for violent behavior. Environmental or situational changes were frequently linked to violent reactions (11.2%), with patients responding negatively to adjustments in their vicinity or care routines. These situations included patient transfers, moving items in bed vicinity or bed adjustments, highlighting the need for careful consideration of the patient’s environment and space during care. The following examples were documented: “Patient became agitated when nurse moved his belongings during a routine room clean. He shouted, “Don’t touch my stuff!” and “proceeded to shove the nurse,” and “Aggression escalated after staff attempted to adjust the patient’s bed for treatment, leading to the patient yelling and physically resisting.”
The incident reports suggest environmental factors in health care settings can sometimes act as triggers that lead to violent responses from patients. Specifically, alterations to the environment and moving of personal belongings patients perceive as intrusive or threatening may provoke such behaviors. Other notable examples of problematic environmental disturbances included noisy, chaotic, and overcrowded clinical spaces, and extended wait times for care. Clinical areas such as the Emergency Department are areas of greater risk of WPV incidents. These triggers indicate a need to better understand and control for external stressors in high-risk areas that can negatively affect the patient experience.
Unprovoked Triggers
Sudden and seemingly unprovoked violence outbursts were noted in 4.8% of incidents. These incidents were characterized by abrupt and unexpected violent behavior from patients, without a clear immediate trigger, suggestive of potential underlying dispositions or latent behavioral health factors that manifest as violence. One person wrote, “Without warning, the patient, who was calm moments before, began to scream and throw objects at the health care team.” Another example was “The patient suddenly became violent, hitting a staff member, with no apparent provocation.”
This unpredictability poses a unique challenge in managing patient behavior and may be related to underlying health or psychological issues which require further investigation and intervention. Recognizing and managing these underlying factors is crucial in providing appropriate care and preventing WPV. This underscores the need for health practitioners to be vigilant, “situationally aware,” and to observe for subtle cues and changes in patient behaviors and ensure communication throughout all aspects of patient care (Bingöl & İnce, 2021; Davids et al., 2021).
The role of intoxication, whether due to alcohol, drugs, or withdrawal effects, was also identified as a risk factor associated with WPV. Patients under the influence of substances or experiencing withdrawal symptoms exhibited violence behaviors (4%), indicating a relationship. One person writing, “Patient in withdrawal became highly aggressive, throwing items and threatening staff.” Another example from the incidents was, “Under the influence of [substance], the patient exhibited unpredictable and violent behaviour towards the care team.”
Such states can severely impair judgment, increase impulsivity, and lead to unpredictable behavior. This underscores the importance of careful engagement with those patients who are intoxicated, and the need for comprehensive substance use screening, monitoring, management, and referral as part of assessment and admission processes.
Demographic Insights
Secondary analysis of the incident data elucidated how the different health care settings and specific age groups were uniquely associated with violence categories. For example, Emergency Care settings were predominantly linked with the Authoritative Institutional Interventions theme, highlighting the frequent interactions with security or law enforcement. Elsewhere, Ambulatory Care/Outpatient services were distinguished by the interplay of Care Delivery Methods and Situational Stressors categories, suggesting that both the delivery of care and external pressures may affect these environments. Community Nursing—Adult / General and Renal Medicine settings were notable for their complex entanglement of violence categories, particularly Escalation Dynamics and Situational Stressors, indicating a multifaceted nature of violence in these settings. Furthermore, the age groups of 30–34 and 45–49 years were the age groups most prevalently associated with a spectrum of violence categories, including Warning Behaviors, Situational Stressors, and Care Delivery Methods, pointing to potential age-specific risk factors or triggers worthy of consideration.
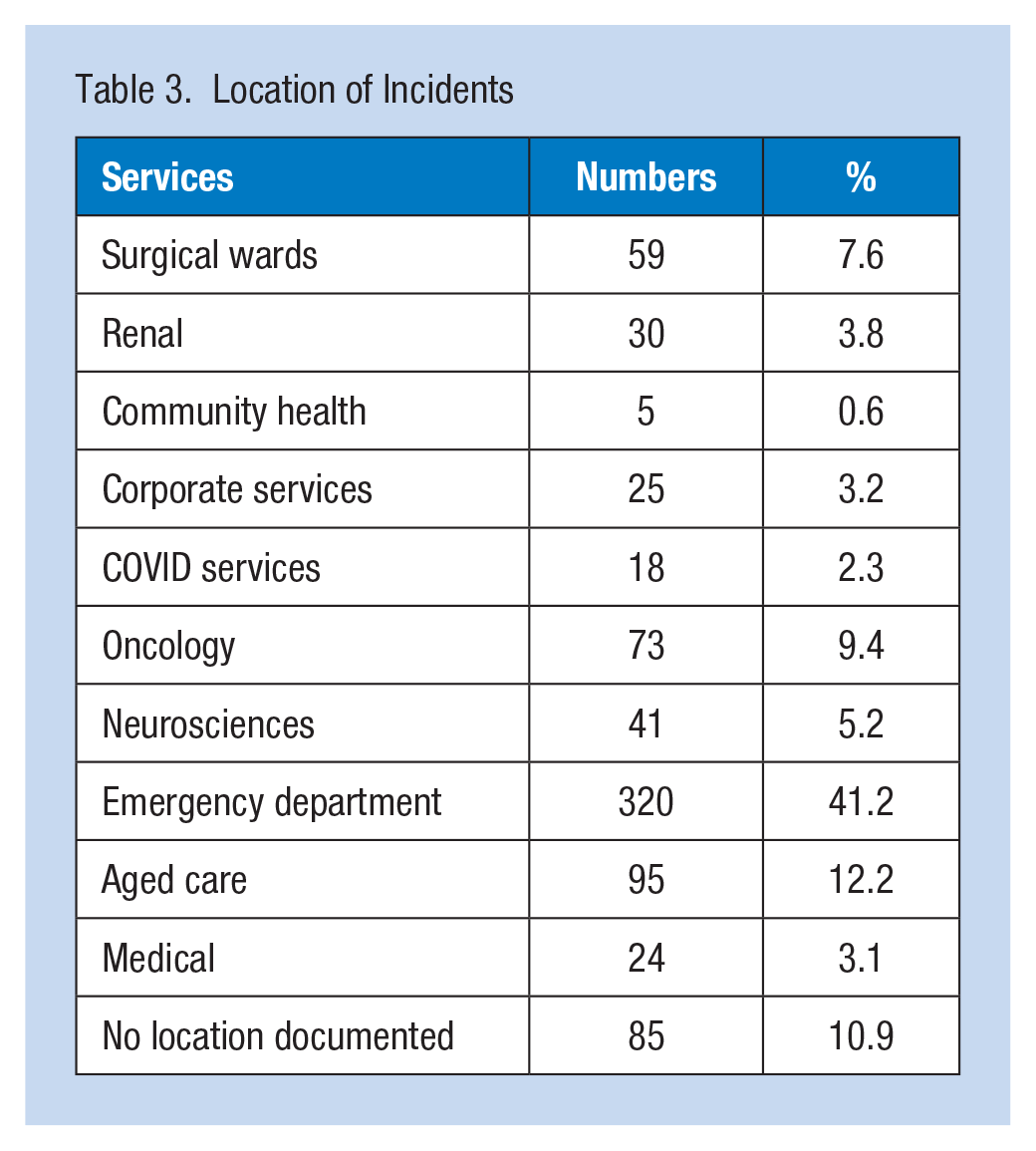
Distribution of age can be seen in Figure 1. Visually, the ranges can be seen to skew to the left with patients in the 30–34 years of age range with the most violent incident reports in admission to Oncology, Surgical, and Neuroscience services. Table 3 contains the clinical specialty areas where the violent incidents took place, with the emergency department followed by the aged care services having the most incidents.
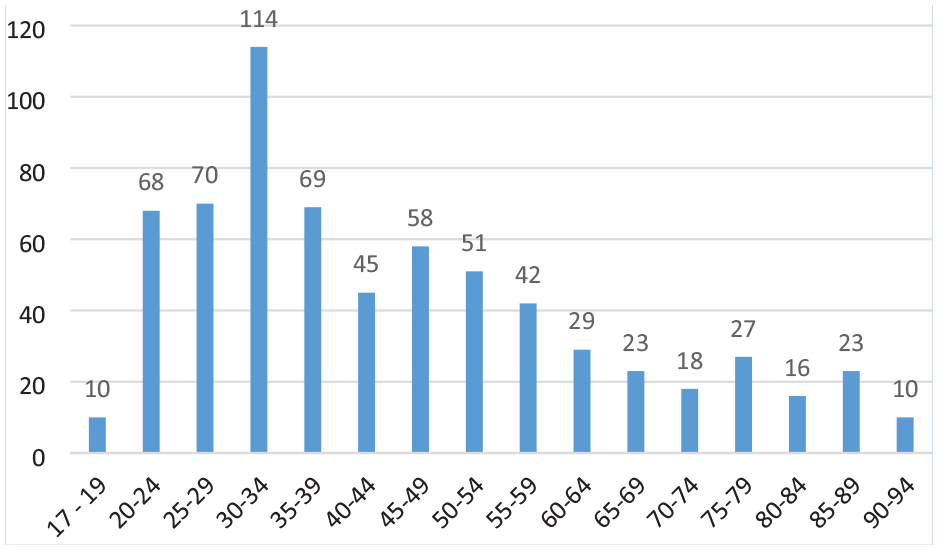
Distribution of Age
Location of Incidents
These findings indicate the multifactorial nature of WPV in this setting, related to situational and environmental stressors, communication factors, underlying medical/psychological factors, care delivery methods, security measures, and substance use. A comprehensive approach accounting for this complexity is essential to mitigate and defuse violence in health care environments. Further investigation is warranted into specific best practices regarding environmental adjustments, de-escalation techniques, behavioral interventions, human-centered practices, substance use assessment screening and management, and measured security and police involvement.
Discussion
This study explored the complexities of WPV, in a general hospital setting as documented by health care practitioners. Employing the READ (Dalglish et al., 2020) and content analysis methods (Elo & Kyngäs, 2008), the research examined 12 months of incident reports from incident reporting system, capturing a snapshot of the nature and context of WPV occurrences. The findings revealed several key themes: Escalation Dynamics, Warning Behaviors, Authoritative Institutional Interventions, Care Delivery Methods, Situational Stressors, and Unprovoked triggers. Each of these themes provide a unique lens through which the phenomenon of WPV can be understood, pointing toward a multifactorial genesis and manifestation of such incidents in health care environments.
The identified theme of “Escalation Dynamics” resonates with the broader literature that underscores the progressive nature of violent incidents in health care settings. Studies have highlighted how seemingly minor confrontations or disagreements can spiral into violent episodes (Kumari et al., 2022; Quigley et al., 2021). This aligns with our findings that emphasize the gradual build-up of tension, often culminating in a violent outburst. This progression underscores the critical need for early intervention strategies, a point echoed in recent research advocating for proactive measures to identify and mitigate escalating behaviors (Pérez-Toribio et al., 2022; Thompson et al., 2022; Timmins et al., 2023).
The concept of “Warning Behaviors” identified in our study is also a significant contribution to the existing body of knowledge. Literature has long emphasized the importance of recognizing pre-violent indicators to prevent escalation (Kumari et al., 2020). Our study adds depth to this understanding by categorizing specific behaviors and interactions that precede violence, thereby offering a practical framework for health care professionals to recognize and respond to these early warning signs. Figure 2 provides a visual description of the escalation of violence incidents derived from the themes produced in this study. Beginning with the patient interacting with an object or person where they attempt to meet an unmet need, followed by the need for the nurse to have a verbal interaction with the patient to resolve the unmet need, and if the patients unmet need is still not resolved and escalation to verbal or physical violence results, necessitating the nurse to escalate emergency procedures.
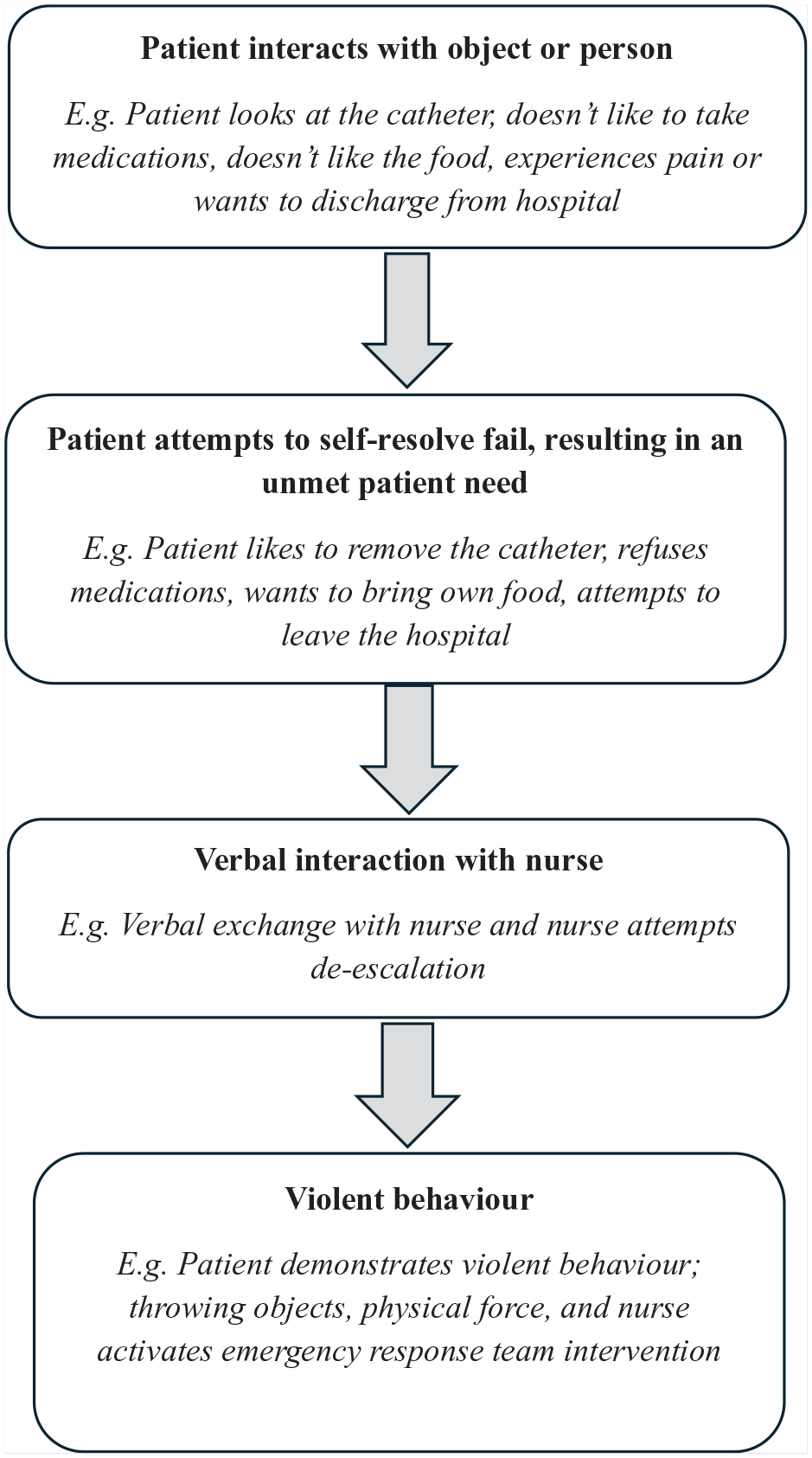
Violence Escalation Model
In examining “Authoritative Institutional Interventions,” our findings contribute to the existing debate on the role of security and law enforcement in health care settings. While necessary for ensuring safety, the presence of security personnel can sometimes inadvertently heighten tensions, a finding that is somewhat at odds with the traditional view of security as a purely stabilizing presence. This highlights a critical need for a balanced approach that integrates security measures with a deep understanding of the psychosocial aspects of health care environments (Davids et al., 2021; Wirth et al., 2021). A combination role of security officer and health care assistant is emerging in New South Wales, Australia, where the individual receives both security and health care assistant training with the aim to mitigate against the authoritative nature of a security only presence. The process surrounding the presence of security staff needs further study. While recognizing that security staff are needed, processes such as security waiting “nearby” out of line of sight until absolutely needed, wearing of uniforms so they appear more clinical and engaging mixed genders in security teams may all help to mitigate against authoritative institutional interventions (Ramacciati & Giusti, 2020; Wand et al., 2020).
The study’s insights into “Care Delivery Methods” and “Situational Stressors” echo the growing consensus in the literature about the environmental and systemic factors contributing to WPV in health care (Brunero, Lamont, et al., 2021). Research has increasingly pointed to the role of environmental stressors, such as overcrowding and understaffing, in exacerbating tensions in health care settings (Wirth et al., 2021). Our findings build on this by illustrating how routine care activities, when coupled with these stressors, can become catalysts for violence.
The 30–34 years of age group had the most reports of violence which is similar to another Australian study who cited patients below the age of 35 years posing greater risk (Pich et al., 2017). Another study from Italy found the average age to be 50 years with both these studies were located in the emergency department. The majority of incidents in this study occurred in the emergency department and the aged care. These findings suggest that violence in health care settings is influenced by a complex interplay of service-specific factors, incident types, and patient demographics. The prevalence of certain violence categories in specific settings and among particular age groups indicates areas where targeted interventions could significantly improve safety and care quality. For example, enhancing staff training in emergency care settings to better manage situations involving authoritative interventions, or focusing on environmental modifications and patient communication strategies in outpatient services to reduce situational stressors, could be effective strategies.
Moreover, understanding the association between specific incident types and violence categories can guide the development of prevention and management protocols tailored to the nuances of different patient interactions. Similarly, recognizing the age bands most associated with various violence categories can inform the creation of age-appropriate prevention and intervention strategies, acknowledging that factors contributing to violence may vary significantly across different life stages. These insights highlight the importance of a nuanced approach to violence prevention in health care, underscoring the need for policies and practices that are responsive to the specific challenges of different service areas, patient types, and age groups.
Berring et al. (2015) argue that written records of nursing discourse play a key role in how WPV is represented and mediates a reality which can lead to social consequences. Written documents of WPV by nursing can perpetuate unspoken assumptions about patient–staff interactions, social realities, and identities. Reports of patient interactions have shown to highlight the subjectiveness that are recorded, often showing hidden staff attitudes and stigmatizations rather than a report being written in objective reality, in the context of WPV that these reports are often completed in highly emotive circumstances by staff. A way forward with documenting violent incidents maybe to use a functional analysis framework, that is, antecedent, behaviors, and consequences as triggers for incident reporting templates (McDougall, 2000). Examples of questions that staff could complete on an incident form include the following: Please describe the triggers observed and unobserved prior to the incident? please describe the violent behavior, give examples? What was the consequences of the violence to the patient, staff, and environment (give examples, injury, damage)?
The multifactorial nature of WPV highlighted in this study suggests that addressing this issue requires a comprehensive and nuanced approach (Ramacciati, 2021). Training health care staff to recognize and respond to early warning signs is crucial, as is fostering an organizational culture that prioritizes safety and encourages reporting of all incidents, including minor or non-physical altercations (Brunero, Dunn, et al., 2021; Lamont & Brunero, 2018; Wirth et al., 2021). WPV tabletop exercises are one such educational approach, which has been adapted from the disaster management literature (Brunero, Dunn et al., 2021). Support and reflexive processes embedded into routine workforce practices will also allow health care practitioners to develop a deeper understanding of WPV dynamics and context. Moreover, the findings indicate a need for health care policies to ensure they are sensitive to the dynamics of patient care and the psychosocial environment of hospitals. Continued monitoring, evaluation, and learning from incidents will also help develop a better understanding of this multifaceted and complex health care issue (Kumari et al., 2020).
This study lays the groundwork for future research in several key areas. While this case focuses on the documentation of WPV by nursing staff within our hospital. The consequences and significance of the physical and psychological effects of WPV for nursing staff are unknown and underreported (American Nurses Association, 2019). Clinicians may experience symptoms of stress, anxiety, depression, and post-traumatic stress disorders following exposure to a WPV incident (Hilton et al., 2021). It is crucial for health care organizations to have robust support systems in place to respond effectively to WPV that includes offering counseling and other resources to cope with the physical, emotional, and psychological consequences because of WPV. Staff working in clinical areas with high rates of WPV may suffer from compassion fatigue, burnout, decreased job satisfaction, absenteeism, increased turnover rates while negatively affecting overall staff morale and care delivery (Cranage & Foster, 2022). There is a need for further investigation into the effectiveness of de-escalation techniques and how they can be integrated into routine generalist health care practice. In addition, research exploring the perspectives of patients and families involved in violent incidents could provide valuable insights into preventive strategies. Finally, comparative studies across different health care settings could help understand the variability in the nature and frequency of WPV, thereby aiding in the development of more tailored and contextual interventions.
Study Limitations
This study has several limitations which should be understood when contextualizing its findings and application. First, it relied on a single source of data incident reports from health care staff in the tertiary referral hospital, which may introduce bias due to the subjective nature of self-reporting. Furthermore, there is no uniform reporting structure for such incidents, increasing content and depth variability. Patient diagnosis and length of stay are not reported in the database, and several demographics were unavailable. Future studies should consider incorporating more demographic variables in their incident reporting systems. Second, the absence of perspectives from patients and potential family members limits a comprehensive multi-perspective view of violence incidents in health care. Third, the data were collected during the COVID pandemic, during the time of increased demands in health care; this may limit the study findings to other time periods. These limitations, and limited generalizability due to its specific single health care organization context, suggest a need for caution in interpreting the findings.
Implications for Occupational Health Practice
This study provides critical insights into the multifaceted nature of WPV in health care settings, as experienced and documented by health care staff. Our findings reveal that violent incidents are not isolated events but are influenced by a complex interplay of factors, including escalation dynamics, warning behaviors, institutional interventions, care delivery methods, and situational stressors. These elements highlight the need for a comprehensive approach to addressing WPV, which encompasses training in recognizing early warning signs, effective communication strategies, nuanced care delivery methods, and understanding the psychosocial environment in health care settings. The significance of our study lies not only in its exploration of the dimensions of WPV but also in its implications for policy and practice. By illuminating the experiences and perceptions of health care staff, this research underscores the need for tailored, context-sensitive strategies to mitigate WPV.
Applying Research to Occupational Health Practice
This research provides guidance for staff working in the occupational health space to enhance education and policy initiatives particularly focusing on recognizing triggers and escalation factors in patient-related violence escalation. Incident reports as documented by health care staff can provide a useful insight into the daily workings of violence in health care settings. Although the incident reports can provide valuable insights the way in which the report is structured and entered can be improved to ensure more useful data are collected, this study suggests following a functional analysis format. Increasing staff ability to recognize and then subsequently plan for escalation in violence may lead to reductions in incidents of violence toward health care staff.
Footnotes
Acknowledgements
None.
Author Credit
S.B. contributed to conceptualization, writing original draft, and formal analysis. S.L. involved in formal analysis, data curation, review and editing. E.T. participated in data curation, review, and editing. N.D. performed review and editing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was sought and received from South East Sydney Local Human Research Ethics committee on February 21, 2023, ethics number 2023/PID00207 as a low-negligible risk study.