
Abstract
Background:
Workplace violence (WPV) in healthcare has become an issue worldwide, with increasing prevalence after the COVID-19 pandemic. Notably, WPV in any setting has individual and systemic repercussions. However, despite extensive literature reporting the prevalence of WPV in healthcare worldwide, effective, standardized prevention policies have not been established. We developed and piloted a WPV initiative at an urban hospital in the state of Maryland. Here, we aim to describe our program development methods and implementation.
Methods:
The 6-month program utilized a reporting tool developed within patients’ electronic medical records (EMRs) to request the display of a Staff Safety Alert (SSA) banner to alert healthcare professionals of patients who engaged in violent behavior and are at increased risk of subsequent behavior. This tool was piloted on 21 patient care units. A review committee either approved or denied case requests filed by frontline workers, with holistic consideration involving patient status, potential biases, and communication flaws.
Results:
Twenty-one banner requests were filed during the course of the pilot. Of which, eight were approved, and 13 were denied. The multi-trauma intermediate care floor filed the most case requests for a safety banner.
Conclusions/Application to Practice:
Our pilot program offers a patient-centered intervention program where extensive personnel training and patient-focused considerations were applied prior to the approval or denial of a banner display. The SSA program was the initial step in institutionally combatting WPV in healthcare as staff are encouraged to officially document unsafe events followed by careful action in response.
Background
Workplace violence (WPV), specifically in healthcare, has become a prevalent issue worldwide. Though there is an absence of a universal definition of WPV in healthcare, a current operational definition describes WPV as “any act or threat of physical violence . . . harassment . . . intimidation, or other threatening disruptive heavier that occurs at the worksite with the intention of abusing or injuring the target” (Al-Qadi, 2021). According to National Institute for Occupational Safety and Health (NIOSH, 2006), WPV has been classified into four types based on the relationship between the perpetrator and the institution itself: (a) no association, (b) customer or patient, (c) current or former employee, and (d) personal relationship with employee not institution, with type ii being the most common form of WPV experienced in hospital settings (Hamblin et al., 2016; Phillips, 2016). Workplace violence can further be quantified by the nature of aggression as physical, verbal, or psychological (Escribano et al., 2019; NIOSH, 2006; Yan et al., 2023; S. Zhao et al., 2018). Of these, verbal violence is most common in a professional setting (Escribano et al., 2019; Sachdeva et al., 2019; Yan et al., 2023; Zhang et al., 2023).
Naturally, WPV leads to individual and institutional repercussions. Individually, physical violence correlated directly with post-traumatic stress disorder (PTSD) and inversely with patient compassion, while verbal violence correlated with negative emotions, such as depression, anxiety, and so on, and both led to an overall higher stress perception, absenteeism, and low job satisfaction (Cannavò et al., 2019; Copeland & Henry, 2018; D’Ettorre et al., 2018; Escribano et al., 2019; S.-H. Zhao et al., 2018; S. Zhao et al., 2018). Consequently, these outcomes cumulate to staff burnout, which has been seen to negatively impact patient outcomes and leads to increased reports of patient safety events (Kim et al., 2023; Occupational Safety and Health Administration [OSHA], 2016). Institutionally, WPV negatively impacts productivity, retention, and monetary costs for indemnity and treatment (Arnetz, 2022; OSHA, 2016M; Speroni et al., 2014; S.-H. Zhao et al., 2018). Despite these pervasive consequences, WPV remains a prevalent issue with rising incidence.
Applications to Professional Practice
The Staff Safety Alert Banner program was piloted to establish an institutional stance and response to workplace violence in healthcare. Our 6-month pilot program implemented on 21 units lead to a total of 21 officially documented banner requests, with 8 approved and 13 denied. These banner requests are most frequently submitted by nursing staff. Though the intervention’s efficacy in workplace violence management and prevention lacks the long-term analysis of the effects of this program, the pilot program is the initial step in addressing workplace violence in the hospital as it provides a timely response from administration to address cases of unsafe behaviors exhibited by patients against their care team. The program is standardized in its implementation, but requires a holistic approach with understandings of cultural relativities, biases, patient emotional/physical/pain status, de-escalation opportunities, and communication approaches to address the cases submitted
Prior to the COVID-19 pandemic, the U.S. Bureau of Labor Statistics (BLS) (2018) reported an incidence of 10.4 per 10,000 full-time workers for WPV in healthcare, which accounted for 73% of all nonfatal workplace injuries and illnesses due to violence that year. Furthermore, there was an annual incidence of 2.1 that year (U.S. Bureau of Labor Statistics, 2018). Prior to COVID-19, a meta-analysis of 26 studies worldwide reported an overall prevalence of WPV of 43%, with a highest rate verbal violence, followed by emotional, physical, and combined, respectively (Zhang et al., 2018). Following COVID-19, a surge of 600 cases of WPV was reported in 40 countries within the first 6 months of the pandemic (Devi, 2020). However, these reported values do not accurately represent the scope of WPV against healthcare workers due to underreporting or trivialization as healthcare workers often believed WPV to be “part of the job,” especially in the absence of physical injury or lost work time (Brophy et al., 2018; Copeland & Henry, 2017; OSHA, 2016; Phillips, 2016; Song et al., 2020). In fact, many healthcare staff, specifically nurses, have long believed that since WPV is potentially expected in a hospital setting, personal incidents are seen as a sign of incompetence (Babiarczyk et al., 2020). Multiple international studies found that staff experiencing WPV also underreport due to fear of losing their job or a lack of trust in their hospital administration to respond appropriately, describing reporting to just a formality (Alsharari et al., 2022; Alsmael et al., 2020; Cannavò et al., 2019; Song et al., 2020). Furthermore, individuals who have previously reported WPV incidents to their institutions were unsatisfied with how the report was handled (Alsharari et al., 2022; Alsmael et al., 2020; Babiarczyk et al., 2020; Cannavò et al., 2019; Douglas & Enikanoselu, 2019; Song et al., 2020). At an organization level, institutions either do not have any established WPV interventions or do not properly inform their staff of how to utilize existing resources. (Alsmael et al., 2020). The major avenues of strategies to combat underreporting include thorough education for administration and staff that WPV is unacceptable, the implementation of a robust intervention program, and education to staff on how and when to utilize these resources. Despite cultural differences and institutional structures of healthcare among countries, there is a universal consensus that WPV must be addressed through staff education and instituting proper reporting channels.
Currently, many studies have attempted to quantify the prevalence and incidence of WPV in healthcare, but few sources in the literature analyzed the utility and efficacy of specific interventions in the workplace (Arnetz, 2022). Staff education has been shown to provide increased support to staff. Current education programs, including Cognitive Rehearsal Program (CRP) and programs using Culture of Civility, Respect, and Engagement in the Workplace (CREW) initiative have improved the trust relationships between nurses and their supervisors, as well as equip staff with strong coping mechanisms and prevention/de-escalation skills (Armstrong, 2017; Laschinger et al., 2012; Stagg et al., 2013). However, very limited literature evaluated the effects of patient flagging. Current literature regarding potential patient flagging interventions raised concerns for patient stigmatization, violation of patient privacy, and gaps between policy and procedure (Ferron et al., 2022). Here, we approach WPV prevention with a focus on understanding the clinical, patient-centered picture to address the concern of patient stigmatization. We highlight the design, implementation, and metrics of a WPV initiative piloted at the University of Maryland Medical Center, a large urban academic center, in which we apply safety alert banners to patients’ electronic medical records (EMRs). This pilot program follows the Joint Commission (n.d.) Standards for WPV prevention.
Methods
Committee Creation
The institution formed a Workplace Violence Prevention Steering Committee in 2020. The steering committee’s mission stated, “The partnership between the Operations and Patient Care Services teams will provide leadership and oversight for the creation, operationalization, and monitoring of initiatives that improve and sustain safety at the hospital.” From the steering committee, nine multidisciplinary subgroups created policies, recommendations, and action items to support the mission. One of these subgroups was named “Complex Patients,” whose directive was: strategies to safely care for complex patients who exhibit violent behavior or who have been assessed to be a risk for violent behavior (e.g., behavioral contracts); formalize recommendations on immediately responding to events that occur while this initiative is in progress. Review current data and trends, policies, procedures, and guidelines and recommend any necessary changes; and work on the logistics for identifying, selecting, and managing patients that warrant universal notification of violence in the EMR.
The complex patients’ subgroup work started in June 2021. The members of the subgroup utilized a just culture approach to focus on the action or event rather than the individual (Murray et al., 2023) to assess the risk for violence and address bias. Next, an operational definition informed by the literature was created to align with the organizational mission. Our definition was “A form of communication (verbal or non-verbal) that expresses hostile intentions and includes an immediate goal, a specific target, and an actionable plan to harm.” This communication may lead to physical and/or psychological harm to others and/or to property (Bjørkly et al., 2009; Meloy et al., 2012, 2021; Rugala & Isaacs, 2003; Semeah et al., 2019; Simons & Meloy, 2017; Warren et al., 2021). Furthermore, the literature guided the development of a fillable note in the EMR to prompt the requester to include information to support decision-making if violence met our definition and, therefore, warrant universal notification (Supplementary Appendix A). From here, we set to name this universal notification. “Staff Safety Alert” (SSA) was chosen because it reflected our values of a just culture. Together, the above process reflected 5 months of work.
Beginning December 2021, our EMR informatics team began working on building the infrastructure for the clinical teams to request an SSA and for the review team to approve or deny the request. On July 2022, the subgroup identified members within the team to continue the work as members of the review team. The review team comprised 13 people with various backgrounds from risk management, psychiatry, clinical safety, social work, security, nursing, internal medicine, and ambulatory.
Pilot Planning
Two subgroup members met weekly for 2 months to draft a proposal for a pilot that incorporated the group-at-large recommendations. Key recommendations included the number of people needed to review requests, the frequency of the reviewing requests, a manual of procedures to guide the review team, and a systematic way to collect pilot data. Based on the literature about group decision-making, three members of the interdisciplinary review team were tasked with being on call Monday through Friday for 1 week at a time (Bonner et al., 2002). A schedule was created that rotated the team members to ensure diverse experiences and perspectives were represented. A project manager and subgroup chair provided each subgroup with a manual detailing the following information, and the project manager was on call throughout the pilot to continuously provide education to the group. Distinct roles were assigned to each of the three members. Role 1 was responsible for leading the chart review by navigating the EMR via the screen share function on behalf of the group, as not all team members had access to the chart. Role 2 communicated with the SSA requester, unit leadership, and the primary medical team. Communication templates were created and utilized by this role to standardize messaging across on-call teams. Role 3 was responsible for data recording by completing a survey housed within the HIPAA (Health Insurance Portability and Accountability Act)-compliant data management software. The survey mirrored the information in the requester’s file entry in the EMR and was used as a tool for the review team to approve or deny the request. This double entry was developed while waiting for the EMR informatics team to build a reporting tool. Our group deemed this necessary to access information and monitor pilot progress, especially for diversity, equity, and inclusion. In addition, we used this survey opportunity to ask process questions. The on-call team answered questions about the documentation that informed their decision to accept or deny the SSA, specifically which locations in the chart were reviewed (i.e., labs, medical notes, nursing notes) and how much time was spent reviewing the case. This aggregated report was then submitted to the hospitals’ internal safety reporting system for reports categorized as WPV. To compare outcomes of the three-member review team versus a single reviewer, people not on-call were asked to review the requests and log their decision using the process described above.
Next, our team worked to identify units to implement the pilot. We sought to pilot this initiative on units that reported high incidents of WPV to our internal safety reporting system. These units were identified as general medicine, neurotrauma, and medical surgical units. Additional units were later identified to add to the pilot as our team could handle. The units included cardiology, all trauma, all medicine, intermediate care medicine, acute medicine, and observation medical. In total, 21 units were selected to participate in this pilot out of 45 units in total. Each participating unit were provided training during hour-long, pre-existing unit meetings with nursing and patient care technicians (PCTs), which covered the SSA purpose, considerations before request, treating clinical factors first, addressing triggers, documentation of behaviors, implementing treatment agreements, signage on patient’s door, refer to WPV intranet page, alert units before transfer, and provides recourses for WPV incidents for self-care, volume of requests. In consultation with unit leadership, we determined that a “Just-in-time” learning strategy would best support education efforts. Just-in-time learning is an approach to individual or organizational learning and development that promotes need-related training readily available exactly when and how it is needed by the learner. The training was published in the form of PDF slides to the intranet. To note, 75% of staff per unit directly received the “Just-in-time” training. Furthermore, two team members met with unit leadership and attended multidisciplinary forums to thoroughly review training, answer questions, and problem-solve. Education for the review team occurred during simulated practice cases. After training commenced, our pilot went live from November 2022 to April 2023 and requested cases were selected from the internal safety reporting system. Figure 1 depicts the workflow.
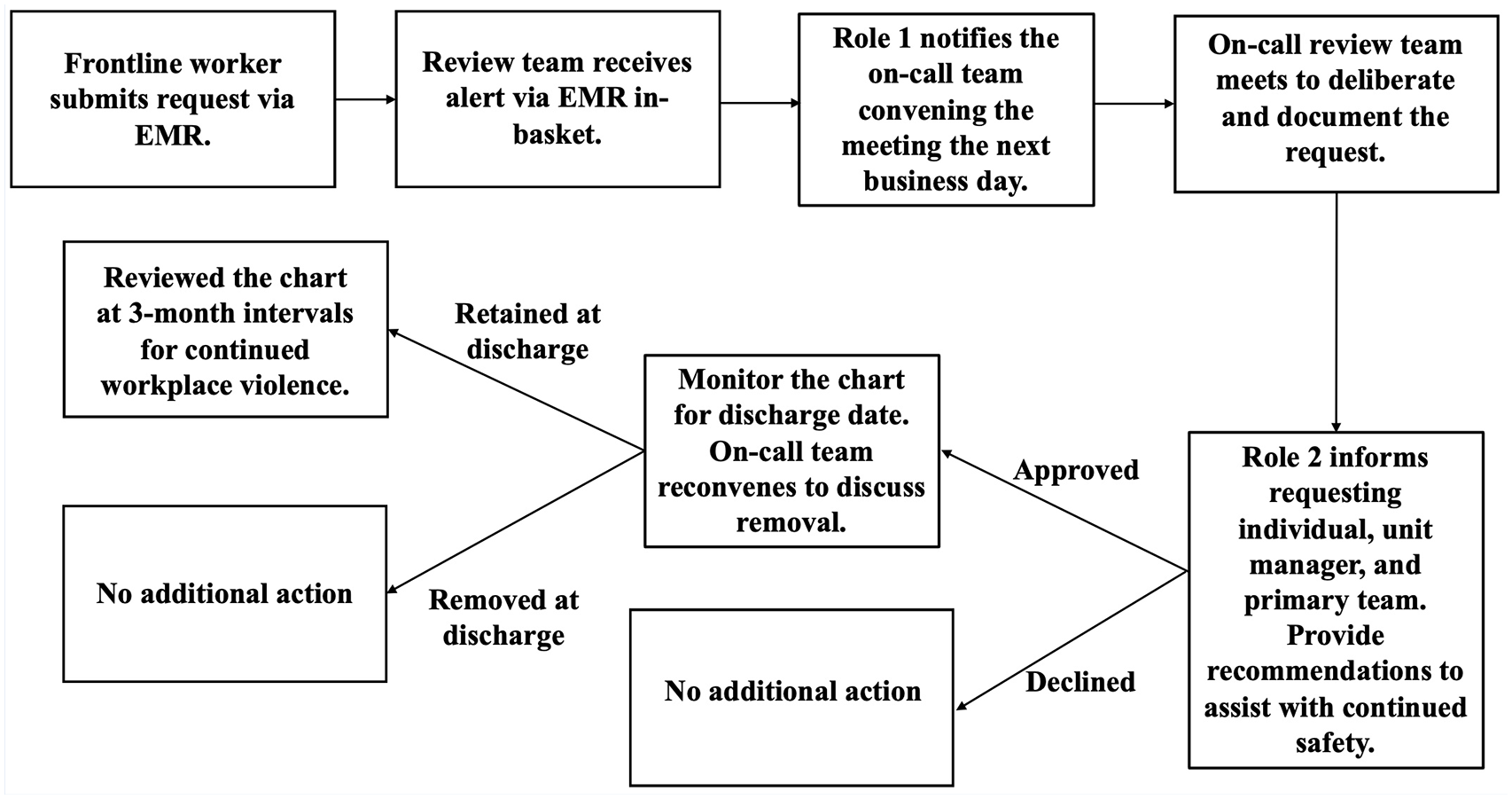
Workflow Depicting Process of Approving Banner Requests
This work was considered exempt by the institutional review board (IRB).
Results
Program Metrics
Our intervention program was piloted for 6 months on 21 of 45 units that qualified, with these 21 units selected due to their history of high reporting of WPV incidents to University of Maryland Medical Center's (UMMC) internal safety reporting system. In these past 6 months, 57% of the units (12 of 21) filed official requests for a safety alert banner, with multi-trauma intermediate care submitting the most at five requests in total (Table 1) (Supplementary Appendix B). To note, more requests were denied than approved by the steering committee (61.9%: 38.1%, declined: approved) (Table 1) (Supplementary Appendix B). Twenty-three percent of the cases filed were of patients within ages 35 to 44, 71% were Black American, and 81% were male (Table 2) (Supplementary Appendix B).
Units With Submitted Staff Safety Alert Banners
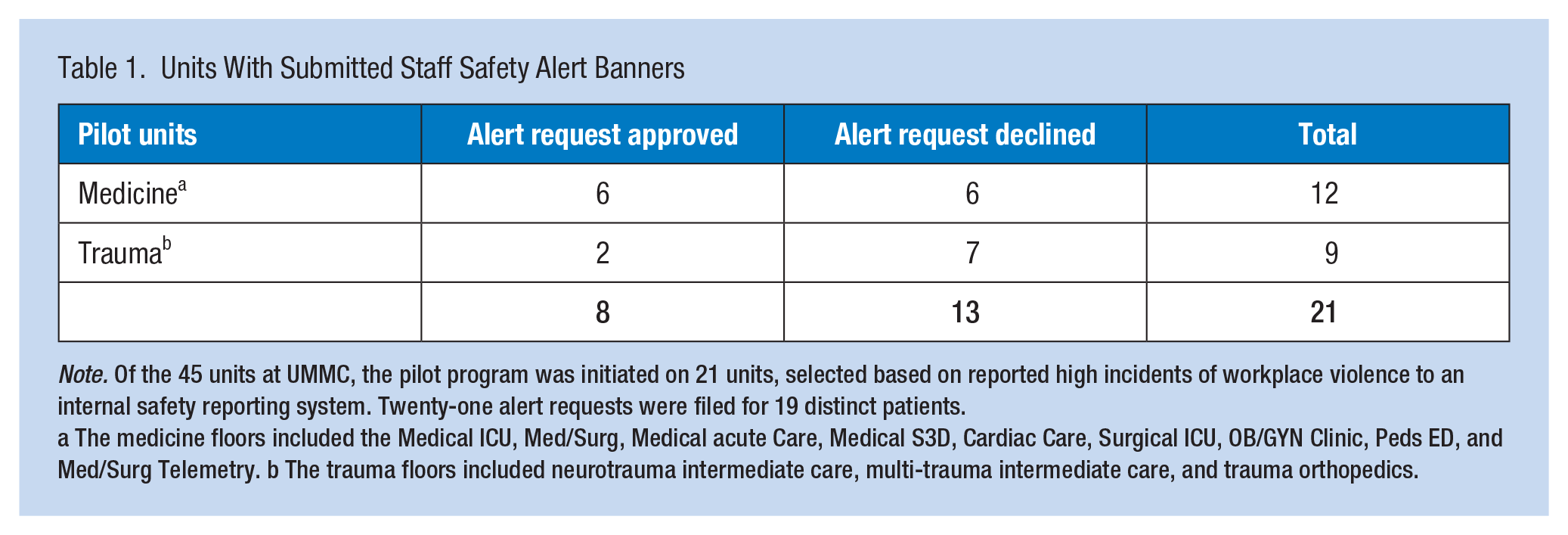
Note. Of the 45 units at UMMC, the pilot program was initiated on 21 units, selected based on reported high incidents of workplace violence to an internal safety reporting system. Twenty-one alert requests were filed for 19 distinct patients.
a The medicine floors included the Medical ICU, Med/Surg, Medical acute Care, Medical S3D, Cardiac Care, Surgical ICU, OB/GYN Clinic, Peds ED, and Med/Surg Telemetry. b The trauma floors included neurotrauma intermediate care, multi-trauma intermediate care, and trauma orthopedics.
Demographics
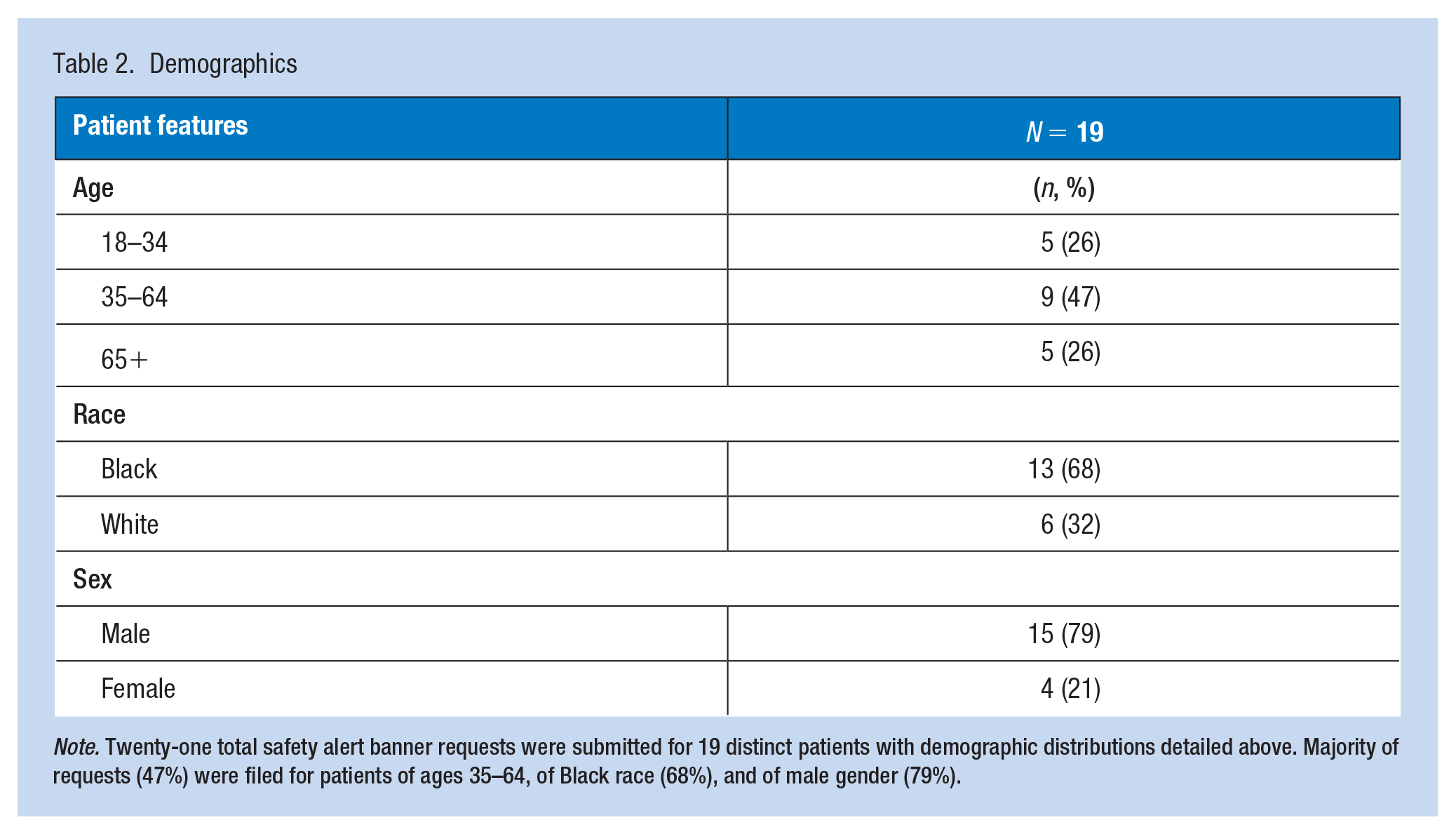
Note. Twenty-one total safety alert banner requests were submitted for 19 distinct patients with demographic distributions detailed above. Majority of requests (47%) were filed for patients of ages 35–64, of Black race (68%), and of male gender (79%).
Operational Results
The steering committee considers each banner request for one of three conclusions: approved with banner active on EMR until discharge, approved with banner permanently active on EMR, or declined. As mentioned, more cases were declined (61.9%) than approved (38.1%), which is due to the consideration of a range of contributing factors surrounding the safety event (Tables 3 and 4).
Operational and Patient Results
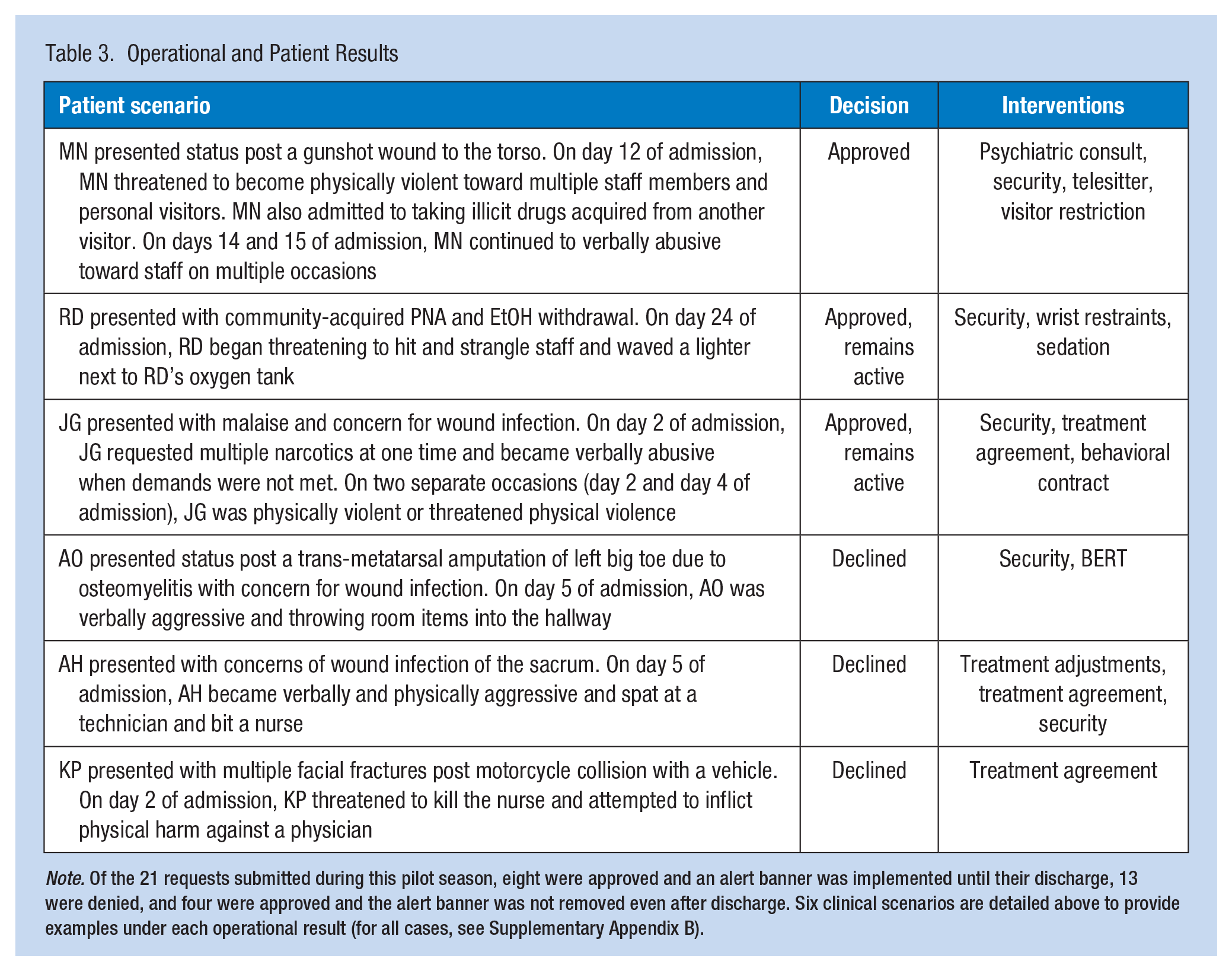
Note. Of the 21 requests submitted during this pilot season, eight were approved and an alert banner was implemented until their discharge, 13 were denied, and four were approved and the alert banner was not removed even after discharge. Six clinical scenarios are detailed above to provide examples under each operational result (for all cases, see Supplementary Appendix B).
Considerations for a Patient-Centered Approach
Note. Each reported incident was analyzed for contributing factors to better understand avenues of future prevention. Attempted interventions prior to banner requests were also documented to understand the level of de-escalation implemented.
Eight cases were approved and the safety alert banner was displayed until day of discharge. Here, we showcased MN due to the slow process to approve the banner request that was applied to this case. MN had three total banner requests submitted throughout MN’s hospital stay. The committee initially declined the first request, attributing MN’s agitation to being under the influence of outside drugs but after repeated reports of aggressive behavior, the banner request was approved and was displayed on MN’s EMR until discharge (Table 3).
Four cases were approved, and their safety alert banner status remains active (Table 3). The committee approves certain cases to remain active if patients of interest continue to meet the definition of WPV. We highlight RD and JG to display the range of behavior that necessitated an active alert. RD stated a goal and had the intent to follow through and commit violence that would result in widespread harm to staff, other patients, and destruction to property. JG’s case was initially declined due to the clinical picture of pain impacting JG’s judgment. Subsequently, JG’s care team was encouraged to establish shared decision-making regarding pain management and treatment plan. However, JG’s team continued to report instances in which JG began to escalate from verbal aggression to physical violence. This prompted the standing approval of an active banner as the escalation increased the credibility in JG’s intent to act violently.
Thirteen cases were declined the use of an alert banner. Specifically, we highlight AO, AH, and KP to portray the nuance in cases that did not qualify for a banner. AO’s banner request was declined because AO’s aggression did not appear to have a specific target and the verbal references/threats made were vague (Table 3). AH’s banner request was declined because upon further committee analysis of the situation, AH’s behavior was attributed to pain levels and embarrassment and AH’s care team was encouraged to adjust their approach to communicating and executing treatment plans. KP’s banner request was denied because KP’s behavior was concluded to be due to delirium which resolved.
Discussion
Workplace violence is an increasing concern in healthcare. More recently, there has been a paradigm shift to low if not zero tolerance to WPV. The University of Maryland Medical Center implemented the SSA initiative to escalate, in real time, during concerns of WPV and ensure appropriate resources to the team. As stated, of the 21 cases submitted for a banner request, only eight were approved. Once approved, the duration of banner display was continually reviewed, even after patient discharge. We highlight multiple cases that showcase the nuance in protocol given the holistic understanding of the individual patient. MN’s course highlights the slow and careful process our team undergoes to ensure patients continue to receive quality care while also considering the safety of the patient care team. The cases where the banner remains presently active, RD and JG, were highlighted to explain the emphasis placed on threat severity. Denied cases were scenarios in which patient factors played the foremost role and when patient needs were addressed, the case was resolved.
These cases highlight the importance of a review board to differentiate between cases in which de-escalation could be achieved upon further understanding of the patient’s clinical picture and cases in which intent to harm was clear despite patient circumstances. The rigorous unbiased review process in place avoids “framing” patients who demonstrate behavioral concerns, despite the potential unintentionality behind such behaviors. The review team serves the purpose of validating staff and reiterating the truth that WPV is not “part of the job” while advocating for patient needs and ensuring that patients continue to receive unbiased care.
To date, very few studies have evaluated the efficacy of behavioral flags. Drummond et al. (1989) implemented a flagging protocol in U.S. Veterans Health Administration (VHA) hospitals and found a 92% mean decline in violent events 1 year after implementation. Following studies revealed a mixed picture: one institution saw a decline in violent events during the duration of their flagging protocol program but increased once again when the pilot ended, and another institution saw that EMR flagging deterred only a percentage of patients, while encouraging more violent events in a small minority of patients (Kling et al., 2011; Paterson et al., 2019). From a staff perspective, flagging practices have been found to increase vigilance, which encourages the treatment team to proactively implement safety measures (Burkoski et al., 2019; Paterson et al., 2019; Seeburger et al., 2023). However, major concerns emerged from these studies, including the unintended consequences of stigmatizing patients, and the perception of patient privacy infringement (Ferron et al., 2022; Seeburger et al., 2023). Our program development seeks to address such concerns. Our approval process incorporates patient advocacy protocol by evaluating foremost if violence proceeded from unmet patient needs. Alert requests submitted for such cases were denied and on follow-up the situation was successfully de-escalated. Approved cases were continuously reviewed for any change in behavior, and if appropriate were discontinued or maintained. Upon discharge, the team would again review the safety alert to establish whether the alert should remain in place after discharge for the next clinical encounter in either the ambulatory, emergency department (ED), or hospital visit. The pilot administration team also remained an active role during the unit training period to ensure a robust transfer of information. Staff were trained in de-escalation techniques and informed of safety resources (Table 4). Safety alert implementation was reserved as a “last resort” escalation to prevent overuse and excess submissions in efforts to mitigate possible introductions of bias and to respect patient privacy.
Limitations
Though this pilot initiative serves as one of the few, if not the first, published intervention programs for addressing WPV in healthcare through patient flagging, it is not without limitations. First, the program was only piloted for 6 months on select units in a 45-unit hospital. The long-term effects of this program on staff safety and WPV management have yet to be observed and analyzed. The program’s foundation is also built on careful and extensive staff education that requires extensive commitment from leadership to train every unit to be properly equipped in de-escalating procedures before submitting a banner request. The success of institution-wide implementation of this program also requires leadership to be properly trained in unconscious bias. Furthermore, the program created an extension off of UMMC’s EMR system. Therefore, another limitation restricting easy implementation at other institutions is the technological capabilities of the respective institutions.
In addition, patient education and involvement is an essential factor in the shared-decision-making model of patient care and should extend into violence prevention as it directly impacts patient perception of care quality. However, during this phase of our program development, patient education was not implemented. Moving forward, this is an important feature that future iterations should consider. Other next steps include implementing the pilot for longer durations to quantify rates of WPV on units with the pilot compared with units running at standard WPV precautions and analyzing cost-benefit for institution-wide safety alert program implementation. Measuring and analyzing specific outcome measures to assess the efficacy of our program is a necessary next step, as well as implementing feedback from participating units. Furthermore, in addition to this pilot, our institution is currently partnered with the Crisis Prevention Institute (CPI), an international leader in evidence-based de-escalation and crisis prevention training and dementia care services, to provide WPV training to all staff across our two campuses. Another next step would be to focus on the details of this training once completed across all staff.
Conclusion
Workplace violence in healthcare has remained a notable concern, and since the COVID-19 pandemic, WPV rates have only risen. There is a great need to design and implement robust solutions to maintain quality patient care while protecting the care team at an institutional level. Here, our SSA Banner program is designed to consider specific patient circumstances, culture, socio-economic background, and so on to avoid “framing” patients who demonstrate behavioral concerns but may not be intentional behaviors. Emphasizing this differentiation allows us to ensure the appropriate measures are provided to individual patients and, as a care team, we continue to prioritize patient-centered interventions.
Supplemental Material
sj-docx-1-whs-10.1177_21650799241280667 – Supplemental material for Staff Safety Alert Banner Program Against Workplace Violence at an Urban American Hospital
Supplemental material, sj-docx-1-whs-10.1177_21650799241280667 for Staff Safety Alert Banner Program Against Workplace Violence at an Urban American Hospital by Crystal Li, Stephanie Bentley, Mangla S. Gulati, Kristie Snedeker and Madeline R. Marks in Workplace Health & Safety
Supplemental Material
sj-docx-2-whs-10.1177_21650799241280667 – Supplemental material for Staff Safety Alert Banner Program Against Workplace Violence at an Urban American Hospital
Supplemental material, sj-docx-2-whs-10.1177_21650799241280667 for Staff Safety Alert Banner Program Against Workplace Violence at an Urban American Hospital by Crystal Li, Stephanie Bentley, Mangla S. Gulati, Kristie Snedeker and Madeline R. Marks in Workplace Health & Safety
Footnotes
Author Contribution
Crystal Li, Stephanie Bentley, Mangla Gulati, Kristie Snedeker, and Madeline R. Marks provided substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. Crystal Li, Stephanie Bentley, Mangla Gulati, and Madeline R. Marks drafted the article and revised it critically for important intellectual content. Crystal Li, Stephanie Bentley, Mangla Gulati, Kristie Snedeker, and Madeline R. Marks gave final approval of the version of the article to be published; and all authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Exempt.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.