
Abstract
Background:
Statistics from the Centers for Disease Control indicate that the use of e-cigarettes, vaping, and other electronic nicotine delivery systems (ENDS) are increasing although data on their safety is limited. While most employers ban smoking in the workplace, tobacco-free policies do not always extend specifically to e-cigarette products.
Methods:
An IRB approved exploratory, cross-sectional study was conducted to investigate occupational health professionals’ (OHPs) knowledge of e-cigarettes, vaping and ENDS and the ability to create change in tobacco-free workplace policies. A 91-item electronic survey was sent via email to 3248 OHPs who were members of the American Association of Occupational Health Nurses.
Findings:
A total of 299 surveys were returned, but only 230 completed the entire survey. Of those who completed the entire survey, those with advanced education had higher attitude toward change summary scores (p = .043) and those with lower years of practicing had low scores for transformational leadership (p = .039). Approximately 40% of individuals did not have or were unsure that a tobacco-free program was in place that included e-cigarettes, but the majority (90%) perceived their organizational leaders as interested in safety changes.
Conclusions:
The majority of respondents understood the health issues inherent in e-cigarettes, were open to implementing policies that included e-cigarettes but needed education and both managerial and employee support to implement policy changes.
Application to Practice:
OHPs are well positioned to be advocates for workplace education, policy development, and worker health promotion for smoking and vaping cessation by leading organizational change.
According to the Centers for Disease Control and Prevention (CDC), e-cigarettes, or vaping devices are known by many different names and may be referred to as e-cigs, vapes, vape pens, dap pens, tanks, mods, pod-mods, or electronic nicotine delivery systems (ENDS) (CDC, 2024a, 2024b). The use of e-cigarettes or vaping products is sometimes referred to as “vaping” or “julling” (CDC, n.d.). In this article, the products or devices are interchangeably referred to as e-cigarettes or ENDS and the use of the product is referred to as vaping or juuling. In 2021, according to the CDC, approximately 18.7% of (46 million) adults in the United States (U.S.) used any tobacco product (Cornelius et al., 2023). Tobacco product users reported the use of cigarettes most frequently, with an overall prevalence of (11.5%), followed by e-cigarettes (4.5%). During 2020–2021, a decrease in cigarette smoking prevalence from 12.5% to 11.5% was observed (p < .01); however, the prevalence of e-cigarette use increased from 3.7% to 4.5% (p < .01) (Cornelius et al., 2023). In the United States, it translates to an estimated 11.1 million adults who currently use ENDS, also referred to as e-cigarettes (Cornelius et al., 2023). Among those adults aged 25 to 45 years, 30.6% were current smokers, 45.8% were former smokers, and 23.6% had never smoked cigarettes (National Center for Health Statistics, 2023). For those adults aged 45 years and older, 42.7% were current smokers, 50.1% were former smokers, and 7.2% had never smoked cigarettes (National Center for Health Statistics, 2023). Clearly, the data suggest that a proportion of working adults are current smokers while their use of ENDS has increased.
Background
As ENDS use has increased consistently among younger adults who never smoked combustible cigarettes, the health risks for nicotine addiction and respiratory risks with ENDS use also rose (Bandi et al., 2023). In a large cohort study, current
Applying Research to Occupational Health Practice
Statistics from the Centers for Disease Control (2019) indicate that the use of e-cigarettes, vaping, and other electronic nicotine delivery systems (ENDS) are increasing, but research is still needed on the long-term health consequences that these products have on workers or workers that have secondhand exposure. While most employers ban smoking in the workplace, tobacco-free policies do not always extend specifically to e-cigarette products. Currently there are 37 states, and the District of Columbia, that prohibit smoking in the workplace, but most of these states do not include vaping in the non-smoking ruling (Lally, 2023). Organizations such as the American Nonsmokers’ Rights Foundation and Society for Human Resource Management have tools available to assist in employee education and policy development. Occupational health professionals are well positioned to be advocates for workplace education, policy development, and worker health promotion for smoking and vaping cessation. Below is a list of resources that can be utilized to begin policy development and implementation:
American Association of Occupational Health Nurses. (2019). AAOHN research priorities. www.aaohn.org/Portals/0/AAOHN%20Research%20Priorities_FINAL.pdf?ver=MsBuvVEe4aNNShJLNGLOfQ%3d%3d AAOHN drafted nine research priority areas that are consistent with and adapted from research priorities identified by the NIOSH Total Worker Health program.American Nonsmokers’ Rights Foundation. (2023a). Overview list—Number of smokefree and other tobacco-related laws.https://no-smoke.org/materials-services/lists-maps/#1555694220625-13093c40-f073 The American Nonsmokers’ Rights (ANR) Foundation is dedicated to promoting prevention and education about smoking/vaping and assisting with public health policy development. This site is a resource for statistical data associated with second hand smoke exposure and access to training resources and advocacy materials.Centers for Disease Control and Prevention [CDC]. (2021). Secondhand smoke exposure and the impact of smokefree policies.https://www.cdc.gov/tobacco/data_statistics/evidence/pdfs/secondhand-smoke-smokefree-policies-508.pdf This document provides the scientific evidence to support secondhand smoke exposure risks and also the impact of smokefree policies.Society for Human Resource Management. (2023). Smoke and vape-free workplace policy.https://www.shrm.org/resourcesandtools/tools-and-samples/policies/pages/smoke-vape-free-workplace-policy.aspx Full access to a sample smoke and vape-free workplace policy is available on this site for guidance on policy development.U.S. Preventative Services Task Force (2021, January 19). Tobacco smoking cessation in adults including pregnant persons: Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/tobacco-use-in-adults-and-pregnant-women-counseling-and-interventions The USPTF recommendations for tobacco smoking cessation in adults. Practice considerations, as well as supporting evidence for the benefits of tobacco cessation interventions is discussed, as well as identified research needs and gaps.
ENDS use was associated with current traditional cigarette use, current marijuana use, history of lung cancer, nonstroke cerebral vascular disease, and chronic obstructive pulmonary disease (COPD) (Scott et al., 2023). E-cigarettes are not without potential negative health consequences such as nicotine addiction, exposure to toxicants, and respiratory symptoms (American Cancer Society [ACS], 2019; Li et al., 2020). The National Academies of Sciences, Engineering, and Medicine (2018) concluded that e-cigarettes are harmful to physiological activity in humans, including bystanders, and the implications for long-term effects on morbidity and mortality are not yet clear. The American Industrial Hygiene Association (AIHA) recommends that e-cigarettes should be considered a source of aerosols, volatile organic compounds (VOCs), and particulates in the indoor environment (Marcham & Springston, 2019).
Initially, ENDS were marketed to aid in the cessation of traditional combustible cigarette smoking. However, ENDS are not approved as a cessation aid by the Food and Drug Administration (FDA) and approximately 25% of those who use ENDS have never used traditional combustible cigarettes (Scott et al., 2023). Few randomized trials have evaluated the effectiveness of e-cigarettes in increasing tobacco cessation and “the balance of benefits and harms cannot be determined” (Krist et al., 2021, p. 265). Therefore, the full implications of vaping on long-term health, the magnitude of health and safety hazards that vaping may present to both users and nonusers, including bystanders, remains unclear.
The CDC reviewed the e-cigarette policy landscape in the United States (2017) and found that only eight states, the District of Columbia (DC), and Puerto Rico specifically prohibited indoor e-cigarette use and smoking in indoor areas (Marynak et al., 2017). As of July 2023, 1,035 municipalities and 26 states, along with the District of Columbia, Puerto Rico and the United States. Virgin Islands have laws that restrict e-cigarette use in 100% smoke-free venues such as nonhospitality worksites, restaurants, and bars (American Nonsmokers’ Rights Foundation, 2023a). However, since most local and state smoke free laws were enacted before e-cigarette’s were on the market, many smoke-free laws do not explicitly mention e-cigarettes. While most employers ban smoking in the workplace, their policies do not always extend specifically to e-cigarette products. Employers need to examine state and local laws addressing the use of these products in the workplace (Nagele-Piazza, 2019). The use of e-cigarettes in workplaces and public places is a significant public health concern (CDC, 2022) because of the potential health impact on users and bystanders such as nicotine addiction, and exposure to toxicants, VOCs, and aerosoled particles (CDC, 2024). The impact of e-cigarette usage is compounded because of the potential confusion or lack of clarity as to where smoking and vaping are allowed, resulting in compliance problems with smoke-free laws and ongoing exposures (American Nonsmokers’ Rights Foundation, 2023b).
The e-cigarette mode of nicotine delivery raises concerns about the safety of the product, the health effects of exposure on users and bystanders, relevance of current tobacco-free and smoke free air policies to their use, how e-cigarette use affects tobacco cessation programs, and other initiatives to prevent and control tobacco use in the workplace (Syamlal et al., 2019). Semple et al. (2022) noted that restrictions and policies on use of e-cigarettes require more research, and Hammond and Phillips (2020) noted that scientific evidence on e-cigarettes is needed so nurses can accurately educate their workforce. However, evidence suggests little is known about ENDS knowledge among U.S. healthcare professionals (Loewen & Relich, 2019), specifically occupational health professionals (OHPs) and nurses, who can be greatly effective in workplace education, policy development, and worker health promotion (Graham, 2024).
The purpose of this study was to examine OHPs’ current level of knowledge regarding e-cigarettes, vaping, and ENDS; the status of workplace tobacco-free policies that include e-cigarettes; and the factors related to how policy change is perceived by professionals in the workplace. This study aimed to describe OHPs’ (a) current knowledge level regarding e-cigarettes, vaping, and ENDS, (b) current status of e-cigarette inclusion in their workplace smoke-free policies, (c) attitude toward change, (d) resistance to change, (e) organizational readiness to change, (f) leadership commitment to safety, and (g) transformational leadership ability. The information obtained from the study is relevant to OHPs and those who support OHPs in developing educational opportunities for greater understanding of e-cigarettes, vaping, and ENDs and in implementing policies in the workplace that address e-cigarettes.
Methods
A cross-sectional study was conducted during June through August 2020 using convenience sampling. A 91-item electronic survey was administered via email to 3,248 OHPs who were active members of the American Association of Occupational Health Nurses in 2020 to assess OHPs’ current level of knowledge regarding e-cigarettes, vaping, and ENDS; to explore how many workplace organizations included e-cigarettes in tobacco-free policies, and how factors related to policy change were perceived by the OHPs and the organization in which they were employed. Bloomsburg University’s Institutional Review Board (IRB) determined this research study (Study #2020-20) to be exempt.
Data Collection
The study population included OHPs working in a variety of organizations and healthcare environments. Nurses or OHPs ages ≥18 years of age; of all races and ethnic groups; regardless of educational level, level of expertise, or years of experience were welcome to participate in the study. This broad population was requested to participate to obtain a diverse and representative sample. OHPs were introduced to the study via email invitation distributed in 2020 by the American Association of Occupational Health Nurses (AAOHN) to their 3,248 members. Participation in the survey was voluntary and no incentives were offered or given to participate.
The Director of AAOHN emailed the study invitation to members that included a hyperlink/URL to the survey. The invitation stated that by accessing the hyperlink/URL, individuals that completed the survey consented to take part in the study. The invitation also stated that no personal identifiable information would be requested and that respondents would be able to exit the survey at any time if they so wished to do so. The Director of AAOHN sent at least one reminder to members regarding the survey during the time the survey was active. The electronic survey was available for an 8-week period in June and July 2020, and the survey was estimated to take approximately 30 to 40 minutes to complete. There was no personal identifiable data collected, thus preserving the respondents’ anonymity to the researchers.
Data obtained from the electronic survey was initially stored on the Qualtrics software database system which is identified as being secure through the use of username and password at the primary researcher’s university. Once the study was completed, the primary researcher retrieved the data from Qualtrics and stored the data in an excel spread sheet saved on the primary researcher’s work computer which was secured by a username and password and locked within their private office of which only the researcher had the key. The data collected for this study was managed and stored securely by the primary researcher. The primary researcher employed specific measures, such as secure digital storage solutions and restricted physical access, to safeguard the data and ensure its confidentiality and integrity throughout the research process. The primary researcher shared the anonymous data with the co-researchers using encrypted electronic methods.
Study Instruments
The 91-item electronic survey consisted of seven sections: (a) demographic and professional information of the respondent; (b) general knowledge of e-cigarettes, vaping, and ENDS; (c) attitude to change; (d) resistance to change; (e) organizational readiness to change; (f) leadership commitment to safety; and (g) transformational leadership ability.
The first section of the survey, demographic and professional characteristics, were measured by 10 multiple choice or yes/no questions including general information about the workplace and employees, such as occupational role in the setting, educational preparation, total years in occupational health, and characteristics of the workplace. The second section of the survey, knowledge of e-cigarettes, vaping, and ENDS, were measured with a set of 18 multiple choice or yes/no questions specifically examining the respondent’s general knowledge regarding e-cigarettes, the health risks associated with e-cigarettes, as well as questions about the existence and creation of tobacco-free policies’ inclusion of e-cigarettes at their facilities. Each e-cigarette knowledge question in this section had only one correct answer. The first two survey sections described above, demographic characteristics and general knowledge of e-cigarettes, vaping, and ENDS, were self-developed questions created by the researchers. Several experts including the AAOHN leadership and OHPs reviewed the survey questions for face validity to confirm that the survey content was appropriate, clear, and all-inclusive.
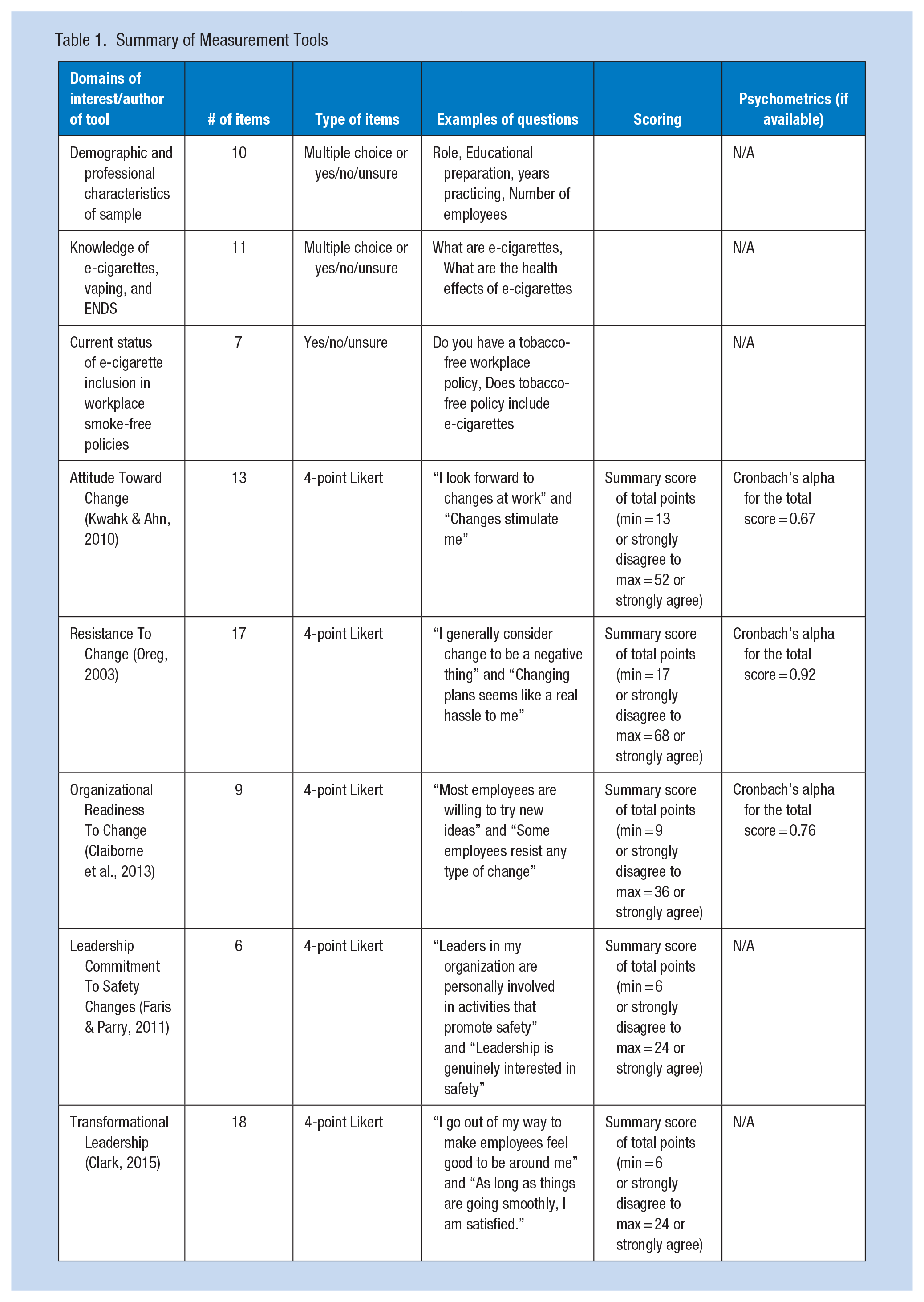
The five remaining sections of survey questions, excluding the demograhic and professional information and knowledge of e-cigarettes questions, were obtained from the PsycTESTS database system with permission. The PsycTESTS instruments in this study were modified to make wording applicable to the study respondents; for example, changing the word “staff” to “employees.” These survey sections measured the domains of interest such as the respondents’ attitude toward change (Kwahk & Ahn, 2010), resistance to change (Oreg, 2003), organizational readiness for change (Claiborne et al., 2013), organizational leadership commitment toward safety changes (Faris & Parry, 2011), and transformational leadership (Clark, 2015). The survey responses to each of these five sections of questions were measured using a 4-point Likert-type scale where 1 = Strongly Disagree, 2 = Disagree, 3 = Agree, and 4 = Strongly Agree. These survey measures were also used in a previous study of workers’ perceptions of Total Worker Health using the same occupational health adult population sample and reported elsewhere (Olszewski et al., 2021). See Table 1 for a summary of measurement tools used in this study.
Summary of Measurement Tools
Data Analysis
The data analysis plan included the use of descriptive statistics to analyze the sample demographics. The frequency of responses to each of the demographic items on the questionnaire were described using counts and percentages. Responses to questions regarding general knowledge of e-cigarettes were compared against the correct responses and a total score for the number of correct responses was calculated. The number of correct responses was categorized using tertiles including low (0–6 correct questions), medium (7 correct questions), and high (8–11 correct questions). Each of the five sets of PsycTESTS questions (Likert-type-scale questions) including attitude toward change, resistance to change, organizational readiness, leadership commitment toward safety, and transformational leadership were combined. The association of the mean PsycTESTS summary scores and selected demographic characteristic (advanced education/role in occupational health versus other role, <6 years in practice versus ≥6 years in practice, hospital/academic environment versus industrial/corporate environment, and English-only language at facility versus other language at facility) were evaluated using two-sample t-tests. Finally, the mean PsycTESTS summary scores were compared between number of correct general knowledge questions (low versus medium versus high) using linear regression trend tests. For each test, p—values < .05 were considered significant.
Results
Demographics and Characteristics of the Respondents
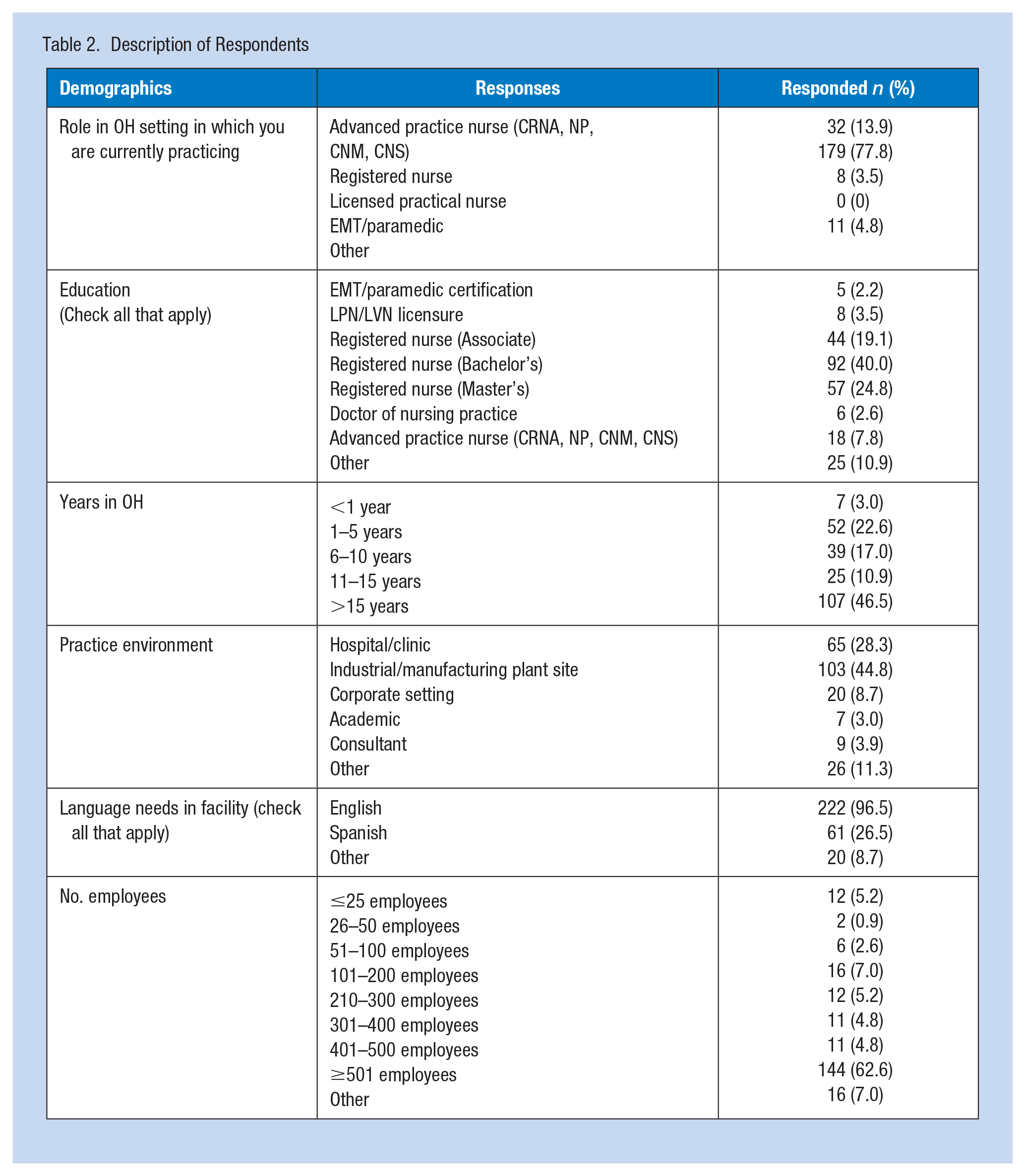
From the total number of 3,248 OHPs with active membership in AAOHN, a total of 299 OHPs responded, but only 230 completed the entire survey for a response rate of 9.2%. Sixty-nine respondents were excluded for various issues of incompleteness of the survey. The results presented here include only those from 230 respondents who completed surveys. The basic respondent was a registered nurse (77.8%), with a BSN (40%), with greater than 15 years’ experience (46.5%), employed at an industrial/manufacturing organization (44.8%), with greater than 500 employees (62.6%), with 60% of those employed aged >36 years old (Table 2).
Description of Respondents
Knowledge of E-cigarette, Vaping, and ENDS
Analysis of the respondent’s general level of knowledge regarding e-cigarettes were favorable with the majority answering most of the questions correctly >64% (Table 3). Only 17% of respondents were aware of the total number of adults who reported vaping or using e-cigarettes, and 57% of respondents did not know FDA covered all tobacco products including e-cigarettes. Analysis of general knowledge level was not associated with respondent’s education/role in occupational health, years practicing, or the occupational health environment.
General Knowledge Response
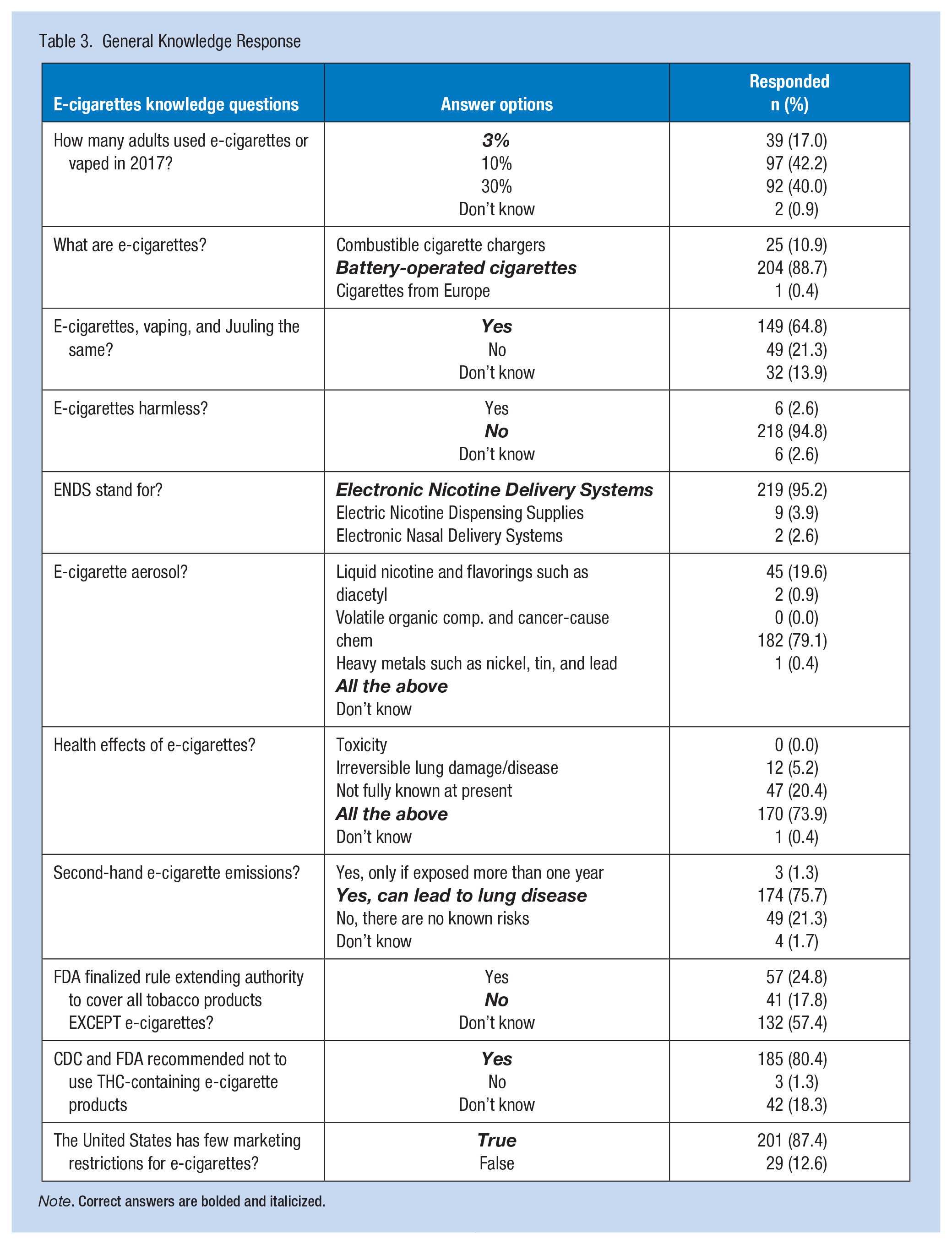
Note. Correct answers are bolded and italicized.
Analysis of questions that explored existing tobacco and e-cigarette policies in the workplace found approximately 52.2% of respondents’ workplaces did not allow the use of e-cigarettes or smoking in any indoor or outdoor areas and 46.5% allowed only in outdoor areas. Interestingly, 77% of respondents had a tobacco-free workplace policy in place, but only 59.6% included e-cigarettes or vaping. For respondents who did not have a policy in place, 49% indicated they were interested in implementing one, but noted the top three challenges to implementing a policy as gaining employee interest (19.6%), having management commitment (18.7%), and needing personnel to implement a program (11.7%).
Attitude Toward Change
Those with advanced degree had a mean Attitude Toward Change of 40.7 (SD = 4.8). For those with other degree types, the mean Attitude Toward Change score was 39.3 (SD = 5.2). When using a two-sample t-test, this difference was significant (p = .043). This is a relatively small difference, but it was significant and might be interpreted as those with advanced degrees had “better attitudes toward change.” Attitude toward change was not associated with years practicing, occupational health environment, language needs at facility, or general knowledge.
Resistance to Change
The resistance to change score was not associated with education/role in occupational health, years practicing, occupational health environment, language needs at facility, or general knowledge.
Organizational Readiness to Change
The organization readiness to change score was not associated with education/role in occupational health, years practicing, occupational health environment, language needs at facility, or general knowledge.
Leadership Commitment to Safety Change
Those in a hospital/academic setting had a mean leadership commitment toward safety score of 18.2 (SD = 4.0). For those working in industrial, corporate, consulting, or other settings, the mean leadership commitment toward safety score was 19.3 (SD = 4.0). When using a two-sample t-test, this difference was significant (p = .046). This is a relatively small difference, but it was statistically significant and might be interpreted to mean that those in hospital/academic settings felt that their leadership has lower commitment toward safety. The leadership commitment toward safety score was not associated with education/role in occupational health, years practicing, language needs at facility, or general knowledge.
Transformational Leadership
The transformational leadership score was positively associated with years of practice (linear regression trend test p value = 0.039). This score increased with years of practice (mean score for <6 years = 56.6 [SD = 6.0]), mean score for 6 to 15 years = 57.4 [SD = 6.96], and mean score for 15+ years = 58.8 [SD = 6.0]. This might be interpreted as higher years of practice was associated with increased comfort in transformational leadership. The transformational leadership score was not associated with education/role in occupational health, occupational health environment, language needs at facility, or general knowledge.
Discussion
As vaping and electronic cigarettes continue to gain popularity, attitudes and perceptions about these products have also changed. Alduraywish et al. (2023) explored attitudes and knowledge regarding e-cigarette use among first-year students at a university in Saudi Arabia. This cross-sectional design explored knowledge and attitudes toward e-cigarette use. The online, self-administered questionnaire was completed by 467 students. The results indicated that the mean age of smoking initiation was 16.4 years of age. Of e-cigarette users, 31.3% reported that they smoked daily, and 86.7% reported that they used a flavored e-cigarette. The users of e-cigarettes (22.5%) to regular cigarettes (48.4%) reported that e-cigarettes carry the same risk as regular cigarettes due to the chemical components. The students indicated significant gender differences in that the women who participated in the study had better knowledge of e-cigarettes (p > .001). Male participants reported a higher-income status (p < .013), were current smokers (p < .001), and indicated intention for future use (p < .001) that were strong predictors of future e-cigarette use. The researchers concluded that more educational campaigns and tighter regulations are needed to positively impact this increased trend of e-cigarette use. Similarly, in this study, the research results indicated an overall need for increased education on e-cigarette use and regulatory information, as 57% of respondents did not know FDA covered all tobacco products including e-cigarettes.
Healthcare providers play a significant role in patient education and health promotion. Hwang et al. (2020) explored the knowledge of healthcare providers as it related to the health implications of e-cigarette use. The study was conducted over a 4-month period in 2018. Participants included medical attendings (n = 15), residents (n = 15), medical students (n = 33), and nursing students (n = 28). The research was conducted in two steps: free listing interview and a brief survey. The results indicated that the perceptions among e-cigarette use varied across the study participant groups. Gaps in knowledge were identified among all participants regarding FDA regulations of e-cigarettes, and attending physicians were less aware than their junior colleagues regarding prevalence of use. All participants indicated a variable or low response regarding familiarity with evidence-based consequences. In addition, the majority of study participants indicated that their knowledge about e-cigarette use came from news outlets or social media sites versus professional platforms. The researchers concluded that formal training and knowledge should be incorporated into nursing and medical school training as it relates to the health impact of e-cigarette use so this knowledge can be applied to patient education. The present research study supported the need for increased knowledge, training, and policies needed regarding e-cigarette use. Our results indicated that 49% of respondents were interested in implementing a smoking/vaping policy but noted the top-three challenges to implementing a policy as gaining employee interest (19.6%), having management commitment (18.7%), and needing personnel to implement a program (11.7%).
Overall, research from this study is consistent with other research findings regarding the lack of knowledge among healthcare professionals, including occupational health nurses, surrounding the health effects of e-cigarette use. Healthcare professionals require evidence-based, scientifically driven resources and education about the health effects of e-cigarette/ENDS use. This education should also be included in healthcare education programs (Hwang et al., 2020).
A power analysis was not completed for this study. The researchers indicated a possible limitation of this study related to a small sample size (9.2%) of responding OHPs from one occupational health organization (AAOHN). Those OHPs who were not members of AAOHN were not recruited for this study. Ultimately, participants in this study may not be representative of the larger occupational health population despite the AAOHN being an organization drawing members from across the United States and the fact that the study received participation from OHPs at different organizations across the United States.
AAOHN is the professional association of licensed nurses engaged in the practice of occupational and environmental health nursing (AAOHN, n.d). AAOHN’s research priorities were consistent with and adapted from the research priorities identified by the NIOSH Total Worker Health Program. Future studies could add to the AAOHN research priority agenda (2019) by exploring control of hazards, health air quality, total worker health, safe and clean environments (tobacco-free policies), and supporting environments that are safe and clean. Additional research on these topics could be conducted with other occupational health organizations such as Association of Occupational Health Professions, American Association of Nurse Practitioners, or the American College of Occupational and Environmental Medicine. This sample size would include a wider variety of medical professionals, such as physicians, administrators, and OHPs.
Application to Occupational Health Practice
Those who smoke are educated to quit for health improvement; however, many smokers may turn to vaping as it appears in the general media to be a safer alternative to smoking. Metcalf et al. (2022) indicated that vaping is considered an option to smoking versus alternative smoking cessation products approved through the FDA. Healthcare professionals, specifically OHPs, are well positioned to provide the needed education to employees on safe alternatives to vaping and vaping prevention. OHPs including occupational health nurses should educate employees on the health risks associated with vaping and encourage those workers to speak with younger family members about the risks of vaping (Hammond & Phillips, 2020). Workers who use ENDS should be encouraged to avoid smoking and pursue alternative cessation products such as counseling or FDA-approved smoking cessation medications.
Currently there are 37 states and the District of Columbia that prohibit smoking in the workplace, but most of these states do not include vaping in the nonsmoking ruling (Lally, 2023). There are currently only six states (Arkansas, Delaware, New Jersey, North Dakota, Oregon and Utah) that include e-cigarettes in their indoor smoking regulations. Lally (2023) indicated that employers such as CVS Caremark, Walmart, UPS, Starbucks, and Target have moved to including e-cigarettes in their smoking policies. OHPs can work with human resources to lead these efforts and encourage smoking policies that include e-cigarettes. The direction of legal counsel can assist in identifying state and local ordinances that may already restrict the use of e-cigarettes, or ordinances that restrict employers’ ability to prohibit them in the workplace. The Society for Human Resource Management (2023) has a free, with reusable permission, policy for smoke and vape-free workplace which can be a great starting point for policy implementation. OHP respondents to this study indicated a need for examples of written policies in multiple languages, educational offerings to review risks or vaping and policy development/templates to include vaping, and need for research on this issue to include additional organizations.
OHPs are in a unique position to impact the health and well-being of employees at work and families outside of the work environment. Olszewski et al. (2021) conducted a research study exploring occupational health nurses’ attitudes on change and organizational leadership in Total Worker Health initiatives. The 2021 study, conducted with the AAOHN, found that occupational health nurses had a positive attitude to change and that employers are supportive of change. Smoking and vaping cessation education and policy development is an example of a Total Worker Health initiative that would benefit the worker and worker families. OHPs and nurses are in a key position to lead organizational change and implement necessary policy changes to address the epidemic of smoking and vaping use within the workplace and the communities in which workers reside.
Footnotes
Acknowledgements
The authors thank the contribution of G. Craig Wood, MS, Biostatistician for support with the statistical data analysis.
Author Contributions
S.Q. conceived the study concept and design, developed the background and methodology, and drafted and edited the manuscript text. K.O. provided input on the study concept and design, designed the survey used to collect the data, assisted with distributing the survey, assisted with writing and editing of the manuscript. D.W. developed the study methodology and survey, provided data analysis and interpretation, and assisted with the writing and editing of the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
This research was reviewed by Commonwealth University (formerly Bloomsburg University), Institutional Review Board, Study #2020-20, and approved May 26, 2020 as Exempt.