
Abstract
Background:
Firefighters face many inherent occupational health hazards and increased risk for several cancers, making peak health essential. However, cardiac events and stroke continue as leading causes of on-duty deaths. Healthy diets promote prevention of cardiovascular disease and cancers. While some dietary interventions have been undertaken, sustained improvements have not been observed. Understanding firefighters’ occupational influences on dietary behavior is vital for implementation of effective interventions to improve nutrition.
Methods:
The Theoretical Domains Framework (TDF) guided this qualitative study. Nine focus groups of firefighters who work 24-hour shifts and one interview with a fire administrator (N = 34) were conducted in 2018 across South Carolina, United States.
Findings:
Predominant TDF domains of influence for workplace dietary behaviors included social/professional role and identity; social influences; environmental context and resources; knowledge; beliefs about consequences; memory, attention, and decision processes; and emotion. Four emergent themes mapped to TDF domains: “We are family”: Firefighters feel a strong identity in their work and with peers; “If you are a firefighter, you’ve got a second job”: Firefighters experience many limitations in personal and workplace resources; “That kills us”: Firefighters were knowledgeable about most all occupational health and safety risks except dietary risks; and “You’re tired, wore out”: Occupational stress influenced nutritional choice making.
Conclusions:
Firefighters experience many barriers to healthy eating while at work due to unique occupational influences. The findings from this study highlighted specific behavioral domains and barriers to be intervened upon that may increase the likelihood of long-term adoption of healthier dietary practices by firefighters.
Background
Firefighting is an essential public service that has been challenged by a nationwide shortage of firefighters (Fahy et al., 2022). A notoriously dangerous occupation with extensive hazards (e.g., physical, ergonomic, biological, and chemical), firefighting requires a heightened level of physical fitness and endurance. Yet overweight and obesity are common among firefighters, increasing risks for developing chronic diseases including cardiovascular disease (CVD), diabetes, hypertension, and various types of cancers (Bode et al., 2021; Jalilian et al., 2019; Khaja et al., 2021; Ras et al., 2023; Smith et al., 2020).
Sudden cardiac death has been the leading cause of on-duty fatalities since the National Fire Protection Association (NFPA) began recording on-duty deaths in 1977 (Fahy & Petrillo, 2022). Mitigation measures to improve firefighter safety have decreased overall on-duty injuries and deaths over time; however, the proportion of on-duty deaths due to myocardial infarction (MI) and stroke have increased (Kahn et al., 2019). Underlying CVD can contribute to on-duty cardiac events (Khaja et al., 2021; Ras et al., 2023; Smith et al., 2022). Furthermore, an additional unknown number of off-duty cardiac events are likely given the high incidence of predisposing factors in firefighters (Fahy & Petrillo, 2022). Cancer is another major health concern for firefighters, as they suffer a higher incidence of various cancers including testicular, bladder, brain, colorectal, prostatic, non-Hodgkin’s lymphoma, and skin melanoma than the general population (Soteriades et al., 2019). The higher incidence of cancers among firefighters can, in part, be attributed to occupational environmental carcinogenic exposures (Demers et al., 2022).
Lifestyle practices, including nutrition, may contribute to firefighters’ overall health and risk of developing cancer and other chronic diseases such as CVD, diabetes, and hypertension (Christodoulou et al., 2022; Lan et al., 2020; Santos, 2022; Sidossis et al., 2023). The standard American diet, which is low in fruits, vegetables, whole grains, legumes, and nuts, is considered one of the most important risk factors for death and disability in the United States (Aune, 2019; Di Fusco et al., 2024; Masoudkabir et al., 2023). In addition to workplace safety procedures that minimize hazardous exposures for firefighters, improving firefighter nutrition may mitigate the development of dietary-related chronic diseases. Several dietary interventions have been undertaken to improve firefighters’ dietary health with observed improvements in diet quality, body weight status, and cardiometabolic biomarkers (Hershey et al., 2023; Joe et al., 2022). Most interventions provided education and counseling on healthy food choices without intervening upon firefighter-specific workplace influences (Joe et al., 2022). For a more targeted approach to promoting sustainable dietary and food culture changes, future interventions should address firefighter-specific occupational influences on dietary behaviors. The purpose of this study was to identify the predominant workplace influences on firefighters’ dietary practices and to recommend interventions that decrease barriers and encourage healthy eating while at work.
Methods
This qualitative descriptive study was informed by the Theoretical Domains Framework (TDF), a theory-based guide used in implementation science to examine a behavior within the context of an organizational setting with particular interest in implementation of solutions to create greater adherence to behavior change (Atkins et al., 2017). The TDF is not a theory with testable relationships, but a consolidated framework consisting of 14 domains of influence derived from 33 behavioral theories (Atkins et al., 2017). TDF domains include: knowledge; skills, social/professional role and identity; beliefs about capabilities; optimism; beliefs about consequences; reinforcement; intentions; goals; memory attention and decision processes; environmental context and resources; social influences; emotion; and behavioral regulation (Atkins et al., 2017). Used across various disciplines to examine a wide range of behaviors, the TDF is comprehensive enough to capture many possible influences on a behavior and provides a theoretical framework for identifying the prominent influences for targeted intervention in a specific group and setting.
Study conduct was guided using COnsolidated criteria for REporting Qualitative research (COREQ) guidelines (Tong et al., 2007).
Setting and Sample
Participants were full-time and part-time firefighters working in South Carolina, who worked 24-hour shifts. South Carolina is a coastal state in the southeastern region of the United States with population of approximately 5.1 million.
Data Collection
Nine in-person focus groups consisting of three or more on-duty firefighters and one interview with a fire administrator were conducted using a semi-structured interview guide with open-ended questions based on the TDF domains. Research team members facilitated focus groups after receiving interview and research protocol training. Focus groups were conducted from June to November 2018 in three urban counties and one rural county across South Carolina and ranged from 35 to 69 minutes. All sessions were held at fire stations and were audiotaped and transcribed verbatim by trained research assistants. No incentives were offered for participation by the employer or research team.
After initial contact with Fire Chiefs via email and phone calls, sessions were scheduled, and participants were recruited in-person and on-site. Information about the study, potential risks, potential benefits, confidentiality procedures, and contact information for the investigators were provided prior to participation. Basic demographic information was obtained including age, race, gender, height, weight, years firefighting experience, and county. Body mass index (BMI) was calculated using self-reported height and weight. Participant BMI was categorized into normal weight for BMI 18.5 to 24.9, overweight for BMI 25 to 29.9, and obese for BMI greater than 30.
Data Analysis
Data analysis was conducted by two PhD-prepared nurses with expertise in qualitative research methods and took a theory-informed thematic analysis approach. Thematic Analysis (Braun & Clarke, 2006, 2019) follows a practical, six-phase iterative approach that allows for flexibility in focus and scope of addressing the research question. Using the TDF to guide the data analysis process allowed for (a) a better understanding of the multifactorial influences on firefighters’ workplace dietary behaviors; and (b) identification of the most relevant influences so that future interventions could be tailored to enhance behavior change adherence in this specific context. Themes were organized by TDF domains and illustrated by participant quotes which were lightly edited for clarity (e.g., removal of dysfluencies) and contextualization (in brackets); no names were used in this report to protect participants’ privacy.
Results
Firefighters in this sample (N = 34) were 100% male, 90% White, and 87% had either overweight or obesity. Sixty-one percent of participants worked in a rural county with an average of 13.5 years firefighting experience. See Table 1 for demographics.
Demographics of Firefighter Participants
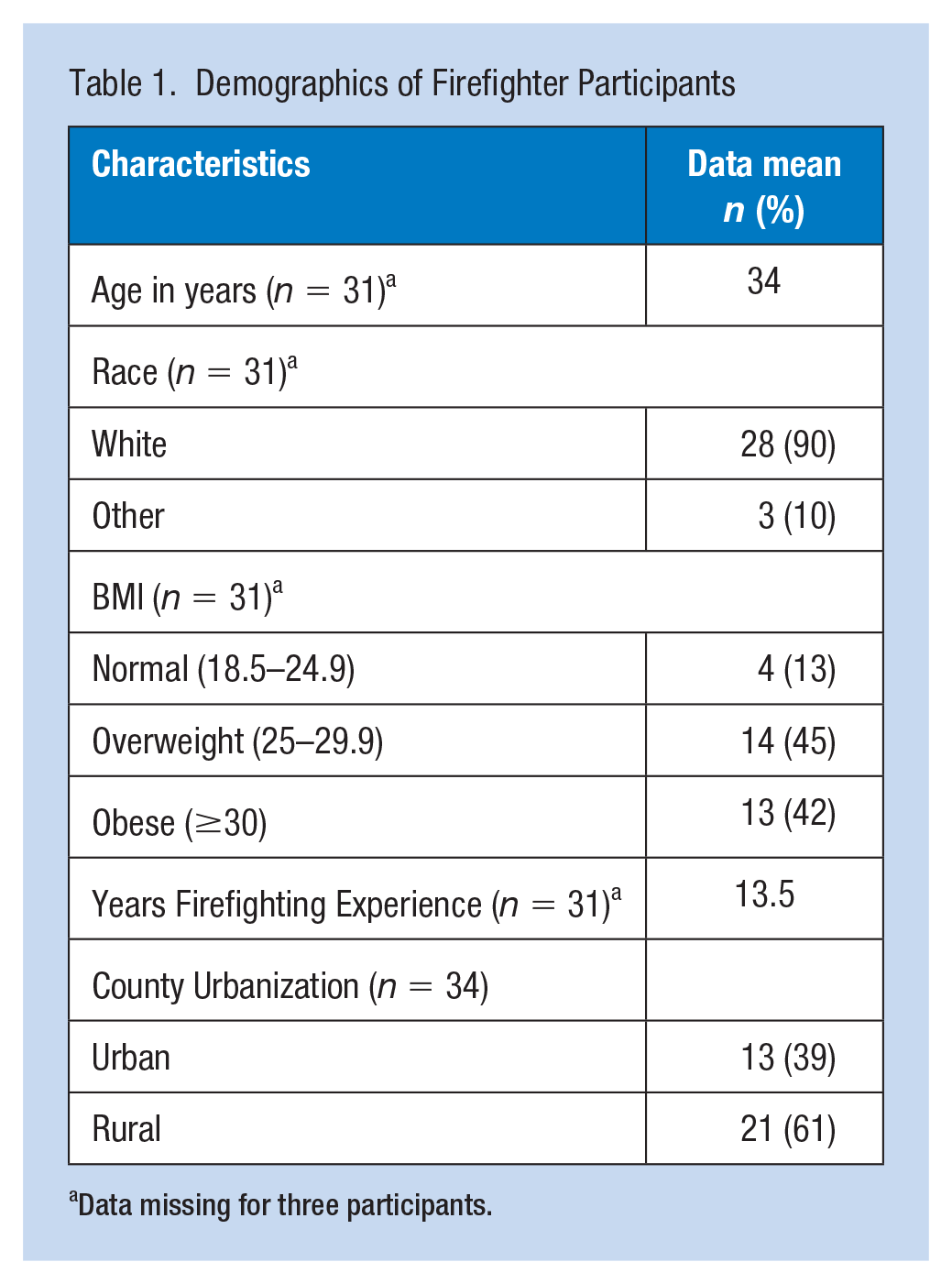
Data missing for three participants.
Firefighters reported influences on workplace dietary behaviors that corresponded to 13 of the 14 TDF domains. However, seven domains were identified as predominantly influential on firefighters’ workplace eating habits and included social/professional role and identity; social influences; environmental context and resources; knowledge; beliefs about consequences; memory, attention, and decision processes; and emotion (Atkins et al., 2017). See Table 2 for the predominant TDF domains of influence, TDF domain definitions, and corresponding study findings.
Predominant TDF* Domains of Behavioral Influence for Firefighters’ Workplace Dietary Practices
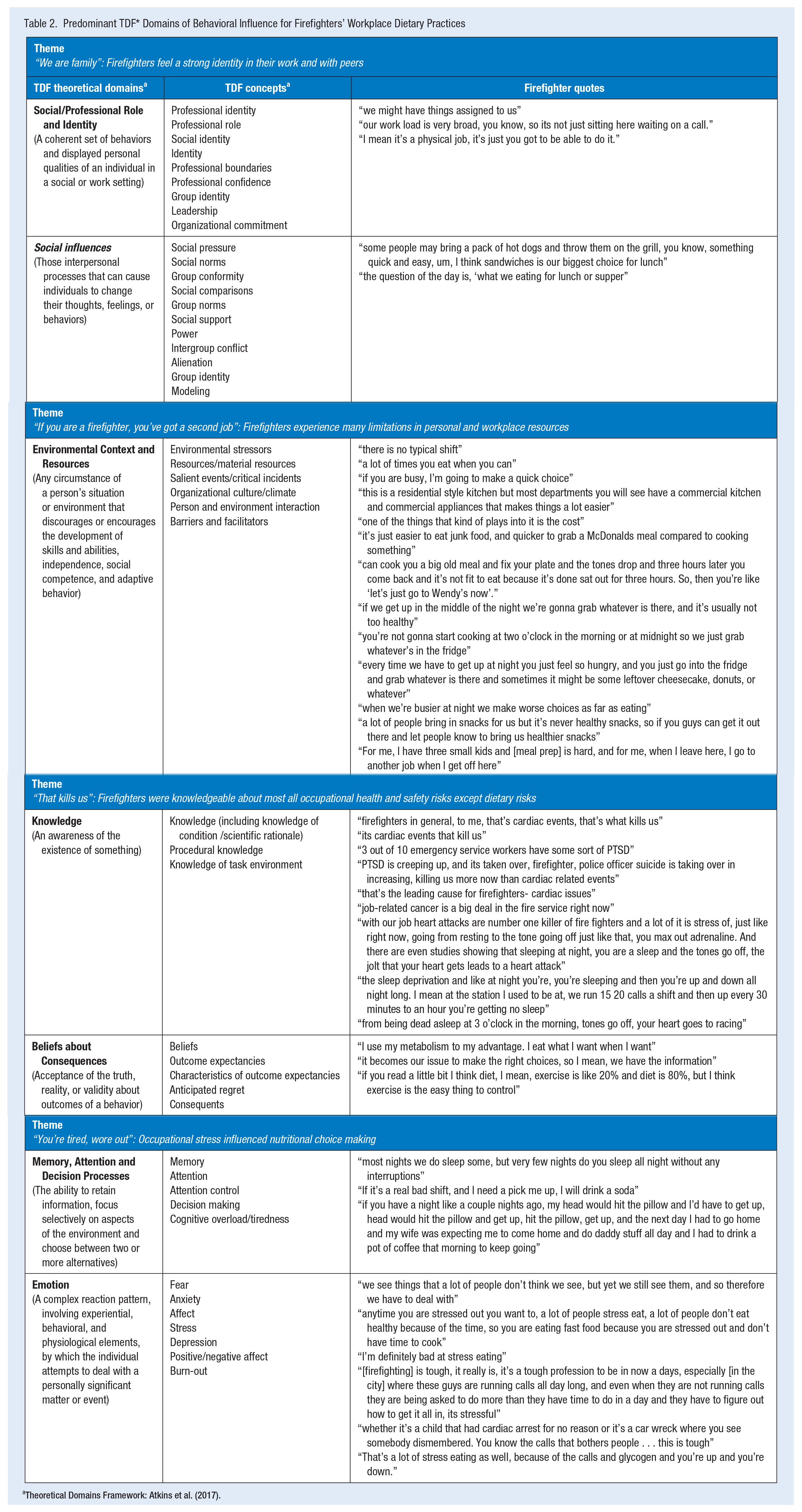
Theoretical Domains Framework: Atkins et al. (2017).
The thematic analysis process also yielded four theoretically relevant emergent themes representing firefighters’ experiences of occupational influences on their dietary decision-making and each was characterized by different TDF domains.
Social/Professional Role and Identity and Social Influences
“We Are Family”: Firefighters Feel a Strong Identity in Their Work and With Peers. Firefighters identified with the role deeper than on an occupational level. They felt it important to embody the role through physical fitness and emotional toughness. The importance of physical fitness and normal cardiometabolic markers were reinforced through required annual workplace evaluations. Physical fitness was also recognized as a responsibility to one another and the community. They frequently spoke of peers as “brothers” and highlighted an individual’s responsibility toward the group: From a fire safety issue, it does bother me in a sense that if we go in with a big dude and he goes down, how am I going to save him? How am I going to move a 300-pound guy with gear through a scene? I mean, he’s responsible for me, I’m responsible for him. We are all on a team together.
Another added, With our job, what the job requires of us, I want to be my best for my brothers and my sisters that I work with, and then I want to be my best for the people that are out there.
This conceptualization of “brotherhood” extended to nutritional choice making, including for the few that reported following a “healthy diet.” For example, a few firefighters reported meal prepping ahead of scheduled shifts and bringing one or two meals to eat during their 24-hour shift. For the third meal, however, they would usually go along with the other crew members to either pick up food from a restaurant or when cooking together, eat what was prepared, even if it did not align with their healthy diet: Where they go, I go. We stick together. We are always in a team here, so where they’re going, that’s where I’m going.
Similarly, many were influenced by peer behaviors and crew preferences when eating meals together: The fire service is a brotherhood anyway so, you don’t want to be the only guy sitting over here eating a salad when everybody else is eating the same meal.
Twenty-four-hour shifts at the fire station were usually staffed by the same group, or crew, of firefighters. Firefighters formed strong bonds with their crew overtime and after encountering dangerous and emotionally challenging scenarios in daily work together. The social norms of eating were most influenced by crew members that regularly worked together on the same shifts. As noted by one firefighter who regularly worked at different stations with different crews, “every shift and every station has its own personality.” Like family dynamics, social norms were established within crews by the interactions of individual preferences with group needs and environmental limitations. Because firefighters work 24-hour shifts, all meals and snacks during shifts were consumed in the presence of fellow crew members. Meals eaten together further strengthened feelings of comradery, thus raising the level of social influences on eating: Meals are an important time at the fire station. At the firehouse during a shift, that’s a lot of comradery built, a lot of the brotherhood aspect of it. That’s your family, and you try to sit down together and eat. That’s what we try to do.
Although norms differed between crews, most agreed that breakfast was usually individualized, lunch was typically something quick and eaten on the run, and dinner was a group decision. Dinner was the most peer-influenced meal, because whether dinner was a group prepared meal, pick-up from a restaurant, or each brought their own, they decided together.
In addition to peers, fire service leadership also played an important role in setting social norms. Firefighters had respect for chain-of-command and authority, thus station leaders such as Captains and Chiefs had notable influence on station culture. Firefighters spoke of local fire leaders that influenced firefighters’ behaviors through role-modeling (both healthy and unhealthy dietary practices), setting priorities for educational offerings, and financial resource allocation: [Our Chief] brought in a fitness guy from [another] county [for fitness education] but then that morning before he got here, he [Chief] also brought grits, eggs, bacon, sausage, homemade biscuits and all that stuff.
Participants reported modeling their behaviors based on their administrators’ nutrition choices: “Since I came here, watching Chief eat, I’ve picked up on some of his [healthy] meals.”
Another added, “[Shift supervisor] is pretty good at his diet and it makes me think, ‘I should probably be on the same page,’ so, I think that is a good thing.”
The participants also reported the influence of less healthy options offered by administrators: “Near Christmas season, our Chief always gives us a big box of station cookies,” and approached the health status of these administrators as a cautionary influence: Our administration, I can’t speak for them, but I don’t know if their diet is as good as it could be . . . we’ve got some administration that all of us just look at each other like “we are not going to end up like them,” so, they are bigger guys . . . that is actually, I think, a huge influence as far as the whole entire department. Even guys that are a little bit heavier-set, even on the line, they are like “I don’t want to end up like him.”
Environmental Context and Resources
“If You Are a Firefighter, You’ve Got a Second Job,”: Firefighters Experience Many Limitations in Personal and Workplace Resources. Firefighters had financial and time limitations both inside and outside of work which influenced workplace food choices. Many firefighters in this study reported working a second job largely due to low salary. One firefighter noted the prevalence of second jobs among peers, relating that, “if you are a firefighter, you’ve got a second job.” Another added, “If this job paid well enough where I didn’t have to work my part-time [job] I wouldn’t work a part-time [job].” Due to working multiple jobs, firefighters had reduced personal time which limited their ability to plan, shop, and prepare for healthy eating.
Financial limitations due to low salary also impacted food choice. As one firefighter explained, “you can eat a lot of meat and bread and cheese for several days off a pack and a loaf of bread.” Related another: “We try to eat for not more than five to eight dollars per person, eating on a budget obviously.”
During shifts, firefighters often experienced busy days with scheduled station and truck maintenance duties, building inspections, and training. Meals were quick events, eaten between scheduled duties and emergency calls. Firefighters made food choices that were quick and easy to prepare or pick up from a restaurant or grocery store. Sandwiches were a commonly cited choice for mid-day meals: “You’ve got to eat when you can, and grab it where you can, and eat it and go.”
Another said, “We might eat fast food at night just because of the time constraints, but we do try to cook at least once a shift.”
The built environment both inside and outside the fire station also influenced firefighters’ workplace dietary choices. Proximity of the station to restaurants, especially where food could be picked up or delivered, increased the likelihood of eating out rather than cooking. Some of the stations were within walking distance to various restaurants, making eating out the primary choice at those stations: “I’ve worked on crews where we cooked a lot and then, like out here, there’s a lot of food in walking distance, so we eat out a lot.” Some rural stations were far from grocery stores and the restaurant choices nearby were fast food franchises: It goes back to our location in our district, we are in a limited area, which limits our choices obviously. But then again, we’ve got a couple different grocery stores that we can go to for options, but convenience kind of ties into that too, as far as cooking time and preparation and things like that.
Firefighters were also influenced by the foods that were readily available at the station, particularly at night. Sugary cereals, potato chips, and cookies were often stored in the station kitchen, and firefighters would find themselves mindlessly snacking on whatever was available: “If I’m up at two in the morning and that box of butter cookies is there, I’m fixing to get into butter cookies.”
Another source of free food at the station came from community members, who often dropped off meals and baked goods for the firefighters. Whenever free foods were available, firefighters would surely partake: [Community member] brings us a dessert every shift, literally, she brings ice cream in here, and it’s a miracle we don’t all weigh 600 pounds, to be honest with you, and she is the nicest lady ever, and it’s never healthy.
The station kitchen also influenced food choices and the probability of cooking. All stations (N = 6) represented in this study had basic kitchen appliances of refrigerator, microwave, electric stove/oven, and coffee maker. Food storage facilities limited choices for many. Food kept in the refrigerator or pantry would be eaten by those on other shifts and therefore, firefighters did not stock more groceries than were needed for their shift: “If it’s in the fridge, it’s pretty much free game, like there was some ice cream sandwiches and somebody came in here earlier and said, ‘I don’t care who’s these are’ and took one out.”
One firefighter described the benefits of a commercial-grade kitchen at another station he often worked at: They’ve got two ovens, a griddle in the center, and they’ve got the gas eyes on the sides, and they’ve got a whole big huge island and it has two sinks and each [shift] has their own pantry with refrigerators with their own food that they can lock up and it’s all locking pantry and I don’t think I ever heard of, our shift anyway, going out and getting food.
Shift workflows also impacted eating choices. Busy shifts, especially when interrupted by emergency calls, lead to eating “grab-and-go” options rather than cooking. One reason firefighters avoided cooking at the station was due to stove/oven automatic shut off when emergency calls alarmed. This safety feature, though necessary, ruined half-cooked meals: When you’re trying to cook, and then you’ll get a call in-between, and then you’ll have to cut your dinner off, and then hopefully get back in enough time where it’s not ruined to finish cooking it. That’s the main problem. You’re cooking spaghetti and then leave, go to a call, and then who knows if your spaghetti noodles are gonna be fine when you come back.
The constant possibility of being called away resulted in frustration and rapid consumption: That’s very frustrating to be enjoying a good meal, or starting to, and just very hungry, and then all of a sudden you hear “beep,” and then you walk back in and start again and alarm goes off again, that’s very frustrating.
Another added, “The quicker you can eat, and the quicker you can prepare it and eat the food, the less chance you run of being interrupted, because it’s a small timeframe.”
Knowledge and Beliefs About Consequences
“That Kills Us”: Firefighters Were Knowledgeable About Most All Occupational Health and Safety Risks Except Dietary Risks. Firefighters were well-educated on occupational health and safety risks and mortality rates and expressed worry over the leading cause of on-duty deaths: “who’s gonna have a heart attack next?” Many participants were able to cite specific statistics regarding sudden cardiac death, cardiovascular disease, cancer, and post-traumatic stress disorder, which were gleaned from workplace education, training, and annual physical screenings. One participant related, “The knowledge that we have industry-wide is that heart attacks are killing firemen, and cancer, so, people are paying attention.”
Firefighters were well-aware of work-related hydration needs, the importance of cardio-pulmonary fitness, and proper handling of contaminated equipment to mitigate some occupational risks. In general, however, firefighters did not place emphasis on dietary health as a means of preventing CVD or cancer. Particularly in reference to cardiac events, firefighters believed sleep deprivation and the adrenaline-rush of late-night calls to be stronger factors than any personal predisposing health conditions such as CVD: I believe studies have shown that the number one killer of firefighters is a heart attack, just because we go from zero miles-per-hour to 100 miles-per-hour in a matter of seconds. It’ll be the middle of the night and you’re completely asleep, and you just gotta get up and go to do your work, so I think it’s something very stressful on the heart, and I think you should just stay physically fit.
While firefighters acknowledged that healthy eating was important for health, most reported they focused more on exercise to achieve physical fitness. Many firefighters used “moderation” to describe a healthy diet. Firefighters recognized their personal diets as acceptable or unhealthy but did not express a strong desire to change eating habits to improve health. Most were aware of normal biometric parameters (e.g., blood pressure, blood glucose, and cholesterol) and reported personal measurements to be within acceptable ranges. However, firefighters identified obesity as a primary health concern for self and peers: “Obesity mainly, I mean, myself as well, we all need to become a lot healthier.”
Few firefighters were knowledgeable about what constitutes a healthy diet or how to achieve one, and most viewed healthy foods as lacking flavor. Salads and grilled fish or chicken were commonly cited examples of healthy foods. Firefighters viewed healthy eating as a personal choice that was arrived at only by willpower: “[It] goes back to your own convictions. You can’t be told, you have to make the decision yourself.” Yet these participants didn’t know strategies or recipes for making their diets healthier. Given that workplace education on health, safety, and physical fitness were common, firefighters welcomed the prospect of workplace educational training on healthy eating: Everyone has different ideas about what [food] is good and what [food] is bad and some people just don’t know or some people know a little bit, so maybe just education on healthy choices.
And another suggested easy healthy recipes and meal plans: “If it was laid out per day, like our first shift, first day of our rotation this month, this is what we are making for lunch, this is what we are making for dinner and that’s already decided.”
Memory, Attention, and Decision Processes and Emotion
“You’re Tired, Wore Out”: Occupational Stress Influenced Nutritional Choice Making. Attention and decision-making efforts for food choices were influenced by firefighters’ level of tiredness while at work. When physically tired from long calls, firefighters chose quick, easy meals that did not require any thought or preparation: “After a busy shift, I could fix something up that is good but at that point in time I just want some chips and salsa.”
Firefighters experienced sleep disruption and poor sleep quality while working 24-hour shifts. Tired firefighters engaged in snacking, especially late at night, to keep awake or to refuel after exertions. Foods chosen late at night typically consisted of ready-to-eat processed foods or baked goods that required no preparation, because “when you get back you don’t wanna have to cook again because you’re tired, wore out.” Lack of sleep from frequent nighttime calls caused additional tiredness and firefighters to seek out caffeine and high-energy snacks: “I definitely drink too much coffee because of [being tired].” Lasting effects of fatigue from firefighting influenced decisions regarding food planning and preparation during personal time.
In addition to being physically demanding, firefighting and responding to various types of emergency calls requires intense mental capacity and attention control, thus, mental and emotional stress from firefighting also played significant roles in decision-making on food choices. Foods high in processed sugars, fats, and/or sodium were preferred after stressful events and late at night as a comfort measure. Firefighters also reported eating large quantities of comfort foods when stressed: Look at EMS, and fire, and police, you know, it’s a lot of comfort eating and a lot of stress eating. It’s two in the morning and you just had a rough call, yeah, you’re going to go get a bag of Taquitos and knock them back with a big salty, sweet, and crunchy because it’s a pleasurable thing.
Sharing unhealthy foods was an easy and common way to deal with emotional, mental, and physical stress: “If you have a real rough [call], you’re like, let’s go grab a burger, let’s grab an ice cream, let’s knock back, quiet down and have that moment, that bonding, like let’s go get milkshakes after this [call].”
Discussion
To better understand the full scope of influences on dietary choices for firefighters within the context of the workplace, TDF-guided focus groups and one interview were conducted with firefighters in South Carolina, United States. Through thematic analysis, the intricate interactions between workplace influences on healthy eating for firefighters were identified and described. TDF domains of influence most relevant to firefighters highlighted through this research can be targeted for implementation of interventions to decrease workplace barriers to healthy eating and enhance behavior change.
In this study, TDF domains of social/professional role and identity and social influences weighed heavily on firefighters’ workplace eating habits. Firefighters share strong social bonds with peers and cultural norms of the firehouse are deeply ingrained into daily activities, including food culture (Sidossis et al., 2023; Sotos-Prieto et al., 2019). Decisions regarding food during 24-hour shifts are made together and often override personal preferences or goals (Hershey et al., 2023; Joe et al., 2022). Social influences between co-workers on healthy eating practices have been identified in other workplace settings (van der Put & Ellwardt, 2022). Firefighters in this study confirmed that peers influenced eating practices through role-modeling (both healthy and unhealthy behaviors) and social norms. Therefore, group-focused dietary interventions may better address the social influences on diet experienced by firefighters and station-wide interventions are recommended (Joe et al., 2022; Sotos-Prieto et al., 2019). Taking into consideration the firehouse food culture, a few dietary intervention studies have included firefighter tailored education and recipes, group education sessions, firefighter exemplars of successfully adhering to healthy eating patterns, and peer nutrition leaders at each fire station (Day et al., 2019; Hershey et al., 2023; Sotos-Prieto et al., 2020). However, most utilized individual-level education, counseling, implementation, and reporting (Joe et al., 2022). An individual-level nutrition education and one-on-one coaching intervention that compared firefighters with civilians found lower Mediterranean diet adherence for firefighters than civilians and suggests the need to address workplace barriers for firefighters and incorporate more group-level interventions (Almeida et al., 2022). Introducing interventions that leverage peer support and accountability for adhering to healthy eating while at work may improve outcomes. As in various workplace settings, firefighters reported building comradery by sharing food during mealtimes which could be used as an advantageous setting for introducing healthy recipes and habits (Horton Dias et al., 2021).
In addition to peer-to-peer influences on food choices, fire leaders have inherent authority to improve firehouse food culture due to firefighters’ respect for the traditional leadership hierarchy (Sotos-Prieto et al., 2019). Through decisions on workplace educational topics, policy implementation, and fund allocation, fire leaders set firehouse priorities and can effectively change culture. Leadership support and participation in developing workplace intervention programs for improving dietary behaviors could result in better adherence and outcomes and should be integral to implementation. Given that healthy dietary patterns, are associated with healthier cardiometabolic markers, body weight status, and less heart disease and cancers, more attention from leadership to improving firefighters’ dietary health is needed (Christodoulou et al., 2022; Lan et al., 2020; Sidossis et al., 2023).
The TDF domain of environmental context and resources was another predominant influence on firefighters’ dietary practices in the workplace. Particularly, lack of financial resources, both personally and departmentally, created barriers to healthy eating for firefighters in this study. Low salary impacted individuals’ ability to purchase healthier foods but also infringed on personal time as many held second and third jobs outside of the fire service, which hindered their ability to plan and prepare healthy foods to bring to work. Fire leaders and occupational health practitioners should consider this factor heavily when implementing changes to improve firefighters’ dietary health. Innovative approaches, such as partnering with local food producers, merchants, and community members, to provide healthy foods at fire stations could address several barriers to healthy eating for firefighters while at work. Sotos-Prieto et al. (2020) attempted to diminish financial barriers in a Mediterranean diet intervention by partnering with a grocery chain for discounts and coupons for use both while at work and at home. In addition, through partnerships with product distributors, supplies of almonds, avocados, and extra virgin olive oil were provided at intervention fire stations (Sotos-Prieto et al., 2020). In this study, firefighters reported frequently consuming foods that were free and available while at the firehouse, though the available foods were typically unhealthy. Having free food available at work may influence consumption due to ease of access and no personal financial cost (Horton Dias et al., 2021). Workplace food programs, including worksite meal provision and take-home groceries, have been used in several countries and industries as a benefit of employment and often resulted in positive improvements in diet (Peñalvo et al., 2021; Rachmah et al., 2022).
In addition to lack of funds and time, firefighters’ reported frequently consuming foods that were easy to obtain, prepare, and consume due to influences related to the TDF domains of memory, attention, and decision processes and emotion. Firefighters need assistance to make healthy eating choices the default due to workflow barriers. Busy workflows and stress during shifts cause firefighters to forgo food planning and make choices based on what is easy to obtain and consume. Ready access to sweets at the firehouse increased consumption for many firefighters in this study. Typically, fast foods and unhealthy snacks are consumed during busy shifts and late at night (Christodoulou et al., 2022; Sotos-Prieto et al., 2019). Occupational stress and fatigue drain firefighters of the energy needed to plan and prepare healthy foods while at work. Due to 24-hour shifts, firefighters can be exposed to fire station environments for longer than workers in other settings, making the station food environment an important location for intervention. Structuring the built environment by providing additional food prep tools/appliances and healthy ready-made meals/snacks and reducing unhealthy foods available in firehouse vending machines or free foods provided by others could encourage healthier food choices as has been seen in various work environments (Peñalvo et al., 2021; Rachmah et al., 2022).
As illuminated through this research, the TDF domains of knowledge and beliefs about consequences influenced firefighters’ adherence to healthy dietary practices. Firefighters were knowledgeable about most occupational health risks but lacked knowledge about dietary risks associated with CVD and cancers. Although firefighters are acutely aware of CVD and cancer as primary risks to their health, knowledge about prevention through lifestyle methods is primarily focused on exercise and physical fitness. Many wellness programs for firefighters have been exercise focused though most included nutrition education to varying degrees (MacMillan et al., 2020). Firefighters are frequently updated on occupational health risk statistics and procedures to decrease their environmental exposures, such as proper handling of contaminated safety gear. Including information on prevention of CVD and cancers through healthy diet could increase firefighters’ knowledge and beliefs about the importance of diet for health. Through annual required physical exams firefighters are made aware of personal risk factors based on assessed biomarkers, however, realistic strategies for improvements through diet changes are seldom provided. Some dietary interventions aimed at improving healthy diet adherence and cardiometabolic markers have incorporated firefighter tailored education, firehouse cooking demonstrations, and healthy recipes for firefighters’ favorite meals (Day et al., 2019; Hershey et al., 2023; Sotos-Prieto et al., 2020). Firefighters need leadership support for on-the-job nutritional education to include easy, low-cost recipes, specific strategies for including more healthy foods in the diet, food prep/cooking skills, and tips for choosing healthier options when eating at restaurants.
Strengths and Limitations
Participants represented both rural and urban settings, thus giving a rich understanding of South Carolina firefighters’ experiences. The sample was predominantly White and all male. Although reflective of the U.S. Fire Service demographics, the lack of diversity limits the cultural perspective and generalizability of the results to groups with more racial, cultural, and gendered diversity. Data were collected prior to the COVID19 pandemic which may have altered the work environment for firefighters and subsequent results.
Implications for Occupational Health Practice
Efforts to decrease firefighter risks for CVD and cancer should include interventions to improve nutritional health. The TDF domains of particular importance for firefighters’ dietary choices highlighted by this research should be targeted for intervention to potentially improve effectiveness. Due to firefighters’ strong group influences on food-related decision-making, creating a culture of health with an emphasis on a healthy diet could be a powerful mechanism to establish long-term behavior changes. Using a team approach to improving diet offers built-in benefits of accountability and peer support, both important to firefighters’ ability to consistently make healthy choices while at work. Fire leadership support is imperative to the success of any workplace program and of particular importance in setting workplace priorities. Occupational health professionals should seek partnerships with fire leadership when developing any intervention plan. For example, leaders could recruit volunteers and assign shopping and cooking duties according to healthy meal plans just as other routine station duties are assigned. By providing meal plan schedules ahead of time, the typical time and effort spent on food-related decision-making that occurs during shifts could be alleviated.
Firefighters engage in frequent on-the-job education regarding occupational health and safety risks. Because firefighters have many time constraints both while at work and at home, nutrition education should be included with other on-the-job trainings to increase awareness of the importance of a healthy diet in the prevention of many chronic diseases including CVD and cancer. Training could include specific strategies for choosing healthy foods on a budget, sample meal plans with recipes, recommendations for making healthy choices at restaurants, and cooking skills.
Alterations to the firehouse food environment could diminish some occupational barriers to healthy eating for firefighters. Providing healthy snacks (e.g., low-sodium nuts, fruits, vegetables, hummus) at the firehouse and on trucks would increase access to healthy foods and could make consuming healthy foods the easiest, most convenient choice. Fire leaders and occupational health professionals could harness community partnerships to schedule healthy meal and grocery donations to fire stations. Providing an inviting space for cooking and storing ingredients could address some additional barriers. The U.S. Fire Administration has set forth recommendations for firehouse kitchens which include stainless steel commercial-grade appliances, separate locking cabinets, and refrigerators/freezers for each shift (US Fire Administration, Federal Emergency Management Agency, US Department of Homeland Security, 2018), all of which were cited by firefighters as promoters of cooking and storing healthy foods. Whenever possible, fire leaders could advocate for upgrading firehouse kitchens to support firefighters’ ability to cook healthy meals while at work. Potentially, making additional prep tools/appliances such as high-powered blenders, pressure cookers, and slow cookers available could aid firefighters in preparing healthy foods more often.
Applying Research to Occupational Health Practice
Cardiovascular disease and cancer are common in firefighters, yet few dietary interventions have focused on firefighter-specific occupational influences on dietary behaviors. This descriptive study highlighted workplace influences on dietary behaviors for firefighters in the southeast United States. Firefighters face many barriers to healthy eating, particularly related to workplace food culture, workflow uncertainty, financial restraints, and physical and emotional stress. By harnessing the firefighter culture of comradery, group-focused on-the-job dietary interventions may provide additional efficacy for improved dietary behaviors. Fire leadership support is essential to initiating culture change and implementing workplace programs that focus on decreasing barriers and improving nutritional health of the group. Innovative programs that include workplace food provision alongside group-focused nutrition education and skills training could help decrease firefighters’ occupational barriers to healthy eating while at work.
Footnotes
Acknowledgements
We would like to thank all the firefighters who participated in this study. We would like to acknowledge Dr. Michael Wirth for making initial introductions for this research. We would like to acknowledge our research team: Heather Miles, Kristen Dibello, Molly Melton, Mary Bethea, Vanessa Grout, and Sara Kailey Miller.
Author Contributions
Conception and design in collaboration by CHD and RMD. CHD, CC, and RMD collected and analyzed data. CHD completed the literature review and wrote the first draft with contributions from RMD. All authors reviewed, revised, and commented on subsequent drafts of the manuscript. All authors gave final approval for submission.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cynthia Horton Dias and Courtney Catledge received no financial support for the research, authorship, and/or publication of this article. Robin M. Dawson was supported by National Heart, Lung, and Blood Institute (NHLBI)/National Institutes of Health (NIH) (1 K23 HL133596-01A1). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the NHLBI/NIH.
Human Subjects Review
The University of South Carolina IRB deemed this study exempt status (Pro00077143).