
Abstract
Background:
Excessive heat stress led to more than 400 deaths in the United States from 2011 to 2021. Common methods for heat injury prevention revolve around measurements of the environment and fail to account for the unique individual response to stressors.
Methods:
An observational approach was utilized with nine helicopter-based emergency medical services personnel during emergency flights to compare core temperature readings obtained from an ingestible temperature monitoring pill and the estimated core temperature reading of the Slate Safety Band V2 wearable device. Comparison of data was conducted within Microsoft Excel programming to determine the mean square error (MSE), root mean square error (RMSE), mean absolute error (MAE), mean biased error (MBE), and Bland–Altman plot development.
Findings:
A significant bias (t = 17.58, p < .001) toward the Slate Safety device reading higher with an average difference of −0.48°C (−0.86°F) was found, meaning the average temperature reading is 0.48°C (−0.86°F) higher with the Slate Safety device. A significant correlation of .26 (p < .001) was noted between the ingestible pill and the wearable device with a 95% confidence interval of 0.23 to 0.29. Aggregate core temperature data demonstrated an MSE of 0.43, an RMSE of 0.65, an MAE of 0.54, and an MBE of −0.48.
Conclusions/Application to Practice:
The ability to monitor the physiological parameters of a worker remotely adds safety tools relative to the risks of heat stress. The slightly higher reading associated with the Slate Safety wearable device provides an added safety margin to protect our workers.
Background
Excessive heat stress caused 436 deaths between 2011 and 2021 in the United States. These deaths overlap with 69,374 heat-related worker injuries between 1992 and 2016 (Bureau of Labor Statistics, U.S. Department of Labor, 2023; Sabrin et al., 2021). Exposure to environmental heat can lead to hyperthermia, heat cramps, and heat stress, causing a decline in cognitive function and an increased risk for physical injury. According to the Centers for Disease Control and Prevention (CDC), the common signs and symptoms of heat exhaustion include, but are not limited to, headache, nausea, dizziness, elevated body temperature, heavy sweating, and weakness (Jacklitsch et al., 2016). Prolonged heat stress is linked to long-term illnesses such as chronic kidney disease, cardiovascular disease, and respiratory dysfunction (Milner, 2022). Given the common symptoms and long-term implication of heat stress, it can be assumed that the actual number of injuries related to heat stress is much higher than reported (Xiang et al., 2014).
Helicopter-based emergency medical services (HEMS) crews often respond to critical incidents, including motor vehicle accidents, farm and industrial accidents, and other critical trauma and medical incidents, and then transport these high-acuity patients to a receiving hospital. Helicopter-based emergency medical services crews wear a flame-resistant flight suit, helmet, and often other impermeable personal protective equipment (PPE). While the flight suit provides protection from flame exposure and PPE provides an impermeable barrier of protection against many pathogens, they both place limitation on the ability for sweat to evaporate from the skin surface, the most common and effective means for cooling the body (Foster et al., 2020). Research suggested that this lack of ability to remove the heat produced based on both the environmental and situational dimensions of nursing care creates physical and psychosocial discomfort while impacting the nurses’ physical well-being and cognitive function, compromising the safety of the provider and patient (Byrne & Ludington-Hoe, 2021).
While all air medical transports pose a risk to flight crews, helicopter-based crews represent the majority (72.4%) of all reported fatalities (Shekhar & Blumen, 2023). The leading cause noted for the crashes of air medical units has been various human factors, including pilot error, pilot disorientation, impairment, fatigue, weather misestimation, and maintenance errors (Shekhar & Blumen, 2023). While this is not an exhaustive list of human factors contributing to crashes, all controls that do not impede helicopter crew performance must be implemented to enhance the units’ safety. Helicopter-based emergency medical services crews face exposure to high temperatures while in the aircraft with limited air conditioning capabilities or on an emergency scene with uncontrollable environmental condition. The combination of these environmental factors with their required flight suit and PPE places HEMS crews at risk for heat stress leading to heat illness, putting the safety of the crew, the well-being of the patient being transported, and the communities in the flight path at risk.
Core temperature is a measure indicating the effectiveness of thermoregulation and can be an indicator of hypothermia or hyperthermia in a worker (Yousef et al., 2024). Core temperature is an indication of the temperature of internal organs and is most accurately measured using a pulmonary artery catheter or esophageal temperature probe (Hymczak et al., 2021). The invasive nature of these measurement methods makes them impractical options for monitoring temperatures in the workplace. Ingestible core temperature monitoring pills (Figure 1A) have been shown reliable and accurate in measuring the gastrointestinal (GI) temperature which is highly indicative of the core temperature (Bongers et al., 2015). When swallowed, the crystals inside the pill vibrate at a frequency relative to the temperature producing a signal stored within the pill (NASA, 2006); this signal is then transmitted via Bluetooth technology to the reader device to report the temperature in the intestinal tract (Linton Instrumentation, 2018). Previous research has demonstrated a hesitancy to ingest the pill due to the introduction of the device into the body and delayed results reporting when the monitor is greater than 1 to 3 m from the pill, which leaves a gap in real-time continuous monitoring of the core temperature of workers (Callihan et al., 2023).
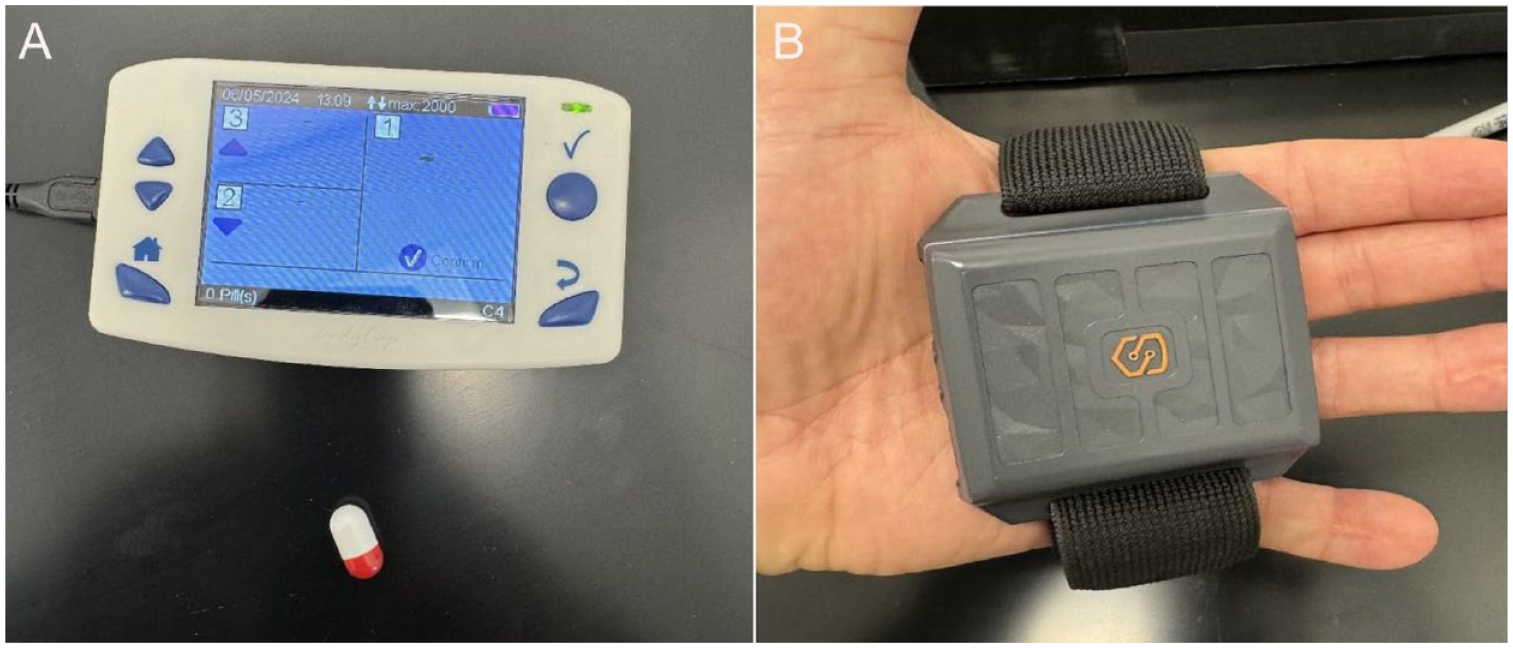
Temperature Monitoring Devices Used for Study: (A) eCelsius Ingestible Temperature Monitoring Pill and Monitoring Device and (B) Slate Safety Wearable Device
The wearable technology used in this study, the Slate Safety Band V2, allows for real-time monitoring of workers and was compared for accuracy to the gold standard ingestible temperature monitoring pill in this study. The real-time monitoring of workers’ physiological parameters provides a means for early detection of changes related to heat stress, allowing for mitigation prior to the development of heat-related illnesses (Council, 2022). Recent work has explored the ability of wearable technology to monitor physiological changes among workers (Callihan et al., 2023; Ibrahim et al., 2023). Wearable technology is typically attached to the surface of the skin with a band to the wrist, forearm, or upper arm. The technology utilized in these wearable devices is typically some sort of red or green light-emitting diodes (LEDs) that can detect changes in the blood vessels below the skin (Alugubelli et al., 2022). Wearable technology, specifically the Slate Safety Band V2 (Figure 1B), attached to the outer aspect of the upper arm provides a comfortable option for remotely monitoring the core temperature and heart rate of a worker with a clinically acceptable accuracy (Callihan et al., 2023; Ibrahim et al., 2023). Callihan et al. (2023) noted an accuracy of the Slate Safety device of 0.13% and 0.09% for the peak and average core temperatures, respectively, when compared with an ingestible pill with a bias error of 0.03°C. Similar findings were made by Ibrahim et al. (2023) that a strong correlation existed between the ingestible pill, p (421) = 0.543, p < .001, and a bias error of 0.20°C. The use of wearable technology to accurately predict current body temperatures on the job can help prevent injury from extreme heat by intervening before temperatures get too high for the body to sustain.
Real-time monitoring of physiological parameters related to heat stress among HEMS crews is necessary for the safety of the flight crews and the patients in their care. To date, minimal information is available related to the impact of the heat on the flight crews. This paper explores the research question: can the Slate Safety Band V2 accurately predict the core temperature of HEMS crews remotely when compared with the gold standard ingestible temperature monitoring pill? The ability to remotely monitor the physiological parameters of heat stress among HEMS crews will improve the safety and health of this highly needed and at-risk work group.
Methods
Participants
A cross-sectional design with observational methods was utilized for this pilot study. Data were collected during normal working conditions of HEMS crews. Data collection occurred with a Private Helicopter Service in Central Alabama while the crew was performing emergency flight operations between May and August 2023. Participants were recruited from a single helicopter-based EMS service in a rural part of the state. Potential participants served as a nurse, paramedic, or pilot for the HEMS company with the only inclusion criteria for the pilot study of being actively employed with the host helicopter service and able to read and speak English. The only exclusion criteria for the pilot study were having an active GI issue or concern due to the use of the ingestible pill. Sixteen helicopter-based EMS crew members were recruited for participation with nine agreeing to take the ingestible core temperature measuring pills.
The Institutional Review Board (IRB) at the University of Alabama approved the pilot study (22-12-6226-A) prior to commencing any research activities. Participants met with the principal investigator (PI), or one other member of the research trained, and IRB approved the evening before collection to provide written informed consent and to take the ingestible pill. Participants read the informed consent, had any questions answered by member of the research team, and signed consent. Participants were then given the pill to take at that time to ensure the pill had passed from the stomach into the GI tract in time for collections the next day. When participants came on shift the next morning, the protocol was reviewed with a member of the research team and any new questions were addressed.
Procedures
All data collections for the pilot study were conducted during live flight situations between May and August 2023 for the flight crews utilizing the eCelsius ingestible core temperature monitoring pill and the Slate Safety Band V2 as described above. Given the emergency nature of the flight service, no controls were able to be put in place regarding temperature or humidity inside the helicopter except for the normal operating onboard air conditioning unit. The air conditioning units were utilized by the flight crews according to their normal operating procedures during the flights.
Data Analysis
Core temperature measurements were collected using the eCelsius ingestible core temperature pills (sample frequency 15 seconds), an emerging gold standard, and the Slate Safety band V2 wearable device (sample frequency 1 minute) for comparison during emergency response flights. Data were time matched to the 1-minute mark for analysis (Figure 2). Comparison of data was conducted within Microsoft Excel programming to determine the mean square error (MSE), root mean square error (RMSE), mean absolute error (MAE), mean biased error (MBE), and Bland–Altman plot development. The SPSS version 27 software package was utilized for bivariate Pearson correlations between the average and peak values of the pill and Slate Safety Band V2 device conducted for each participant and for the aggregate of all the participants. Bland–Altman plots were completed with linear regressions performed. Accuracy was determined as a percentage of the expected value for both peaks and averages, with the ingestible pill serving as the expected value. Data were collected at 1-minute intervals during emergency flights from nine different participants and included 4,135 minutes of time-matched data points for core temperature as measured by the ingestible pill and the Slate Safety wearable device.
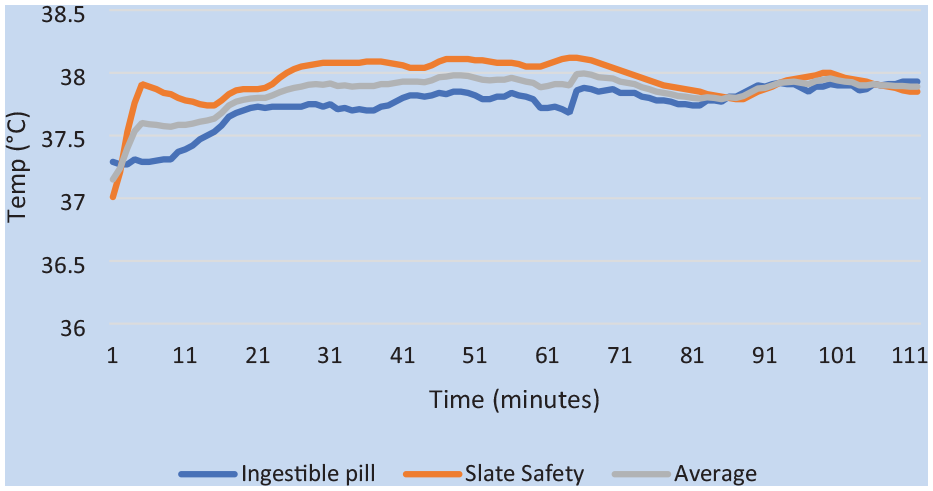
Time Series Plot of Temperature as Measured by eCelsius Pill and Slate Safety and the Average of the Two for Participant 1
Further analyses were conducted based on temperature range measured by the ingestible pill to include 36°C to 37°C (96.8°F to 98.6°F), 37°C to 38°C (98.6°F to 100.4°F), and 38°C to 39°C (100.4°F to 102.2°F). Mean square error, RMSE, MAE, and MBE were determined for each temperature range with comparison of accuracy completed between groups.
Results
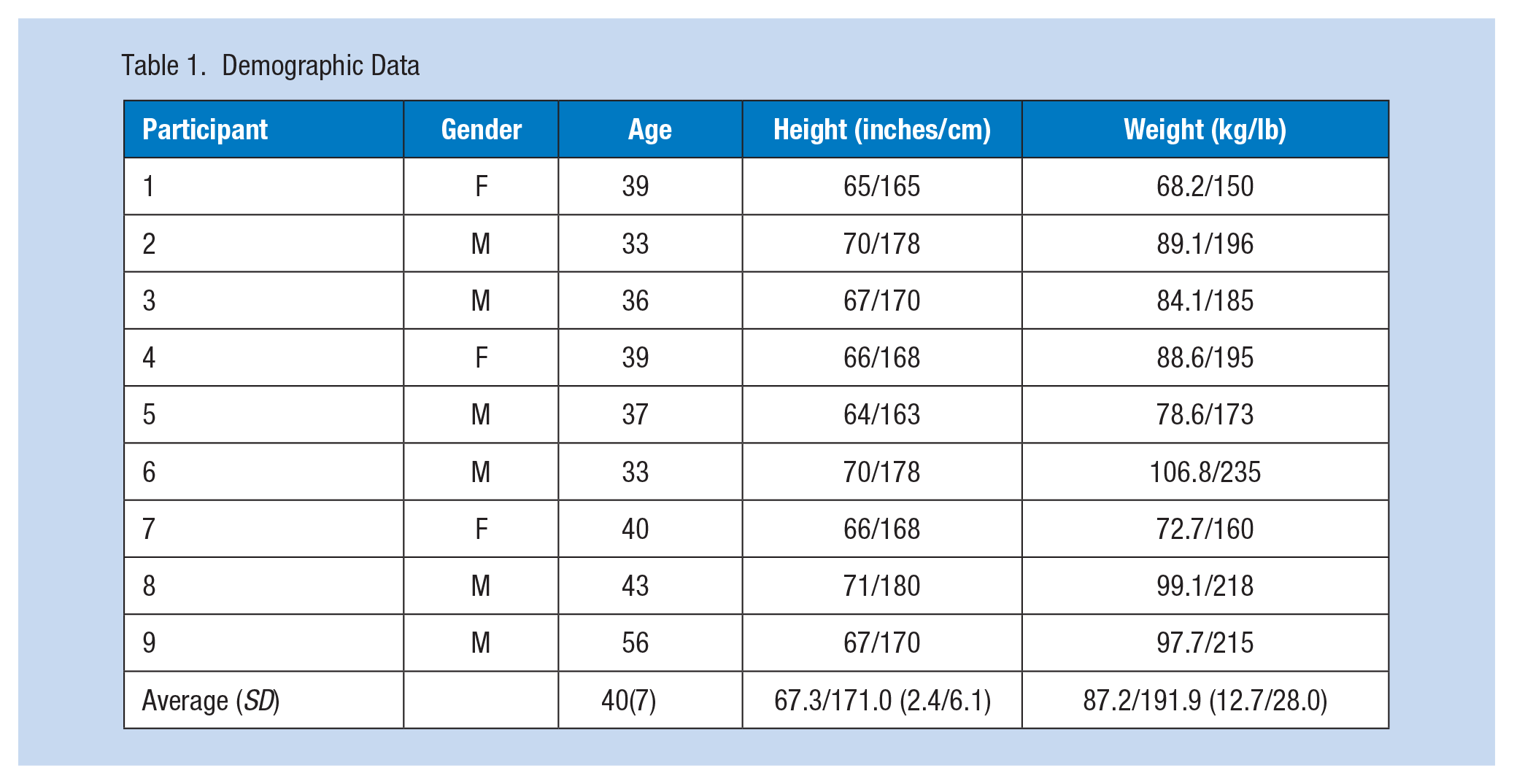
The nine helicopter-based EMS crew members (Table 1) participated in the pilot research study by consuming the ingestible core monitoring pill (eCelsius) and wearing the Slate Safety band V2 during emergency flights. Cabin temperature for the flights ranged from 23.9°C to 35.5°C (75°F to 95.9°F). For unknown reasons, there were 37 missing data points spread randomly across the span of the collection with no data obtainable through the Slate Safety wearable device, for a total of 37 minutes combined for all participants. Missing data accounted for 0.009% of the data and did not account for more than three consecutive data points throughout the time span, thus these data points were removed from the analysis. The differences and mean differences between ingestible pill measurements and Slate Safety measurements can be seen in the Bland–Altman plot (Figure 3). Linear regression demonstrated a significant bias (t = 17.575, p < .001) toward the Slate Safety device reading higher with an average difference of −0.48°C (−0.86°F), meaning the average temperature reading is 0.48°C (0.86°F) higher with the Slate Safety device.
Demographic Data
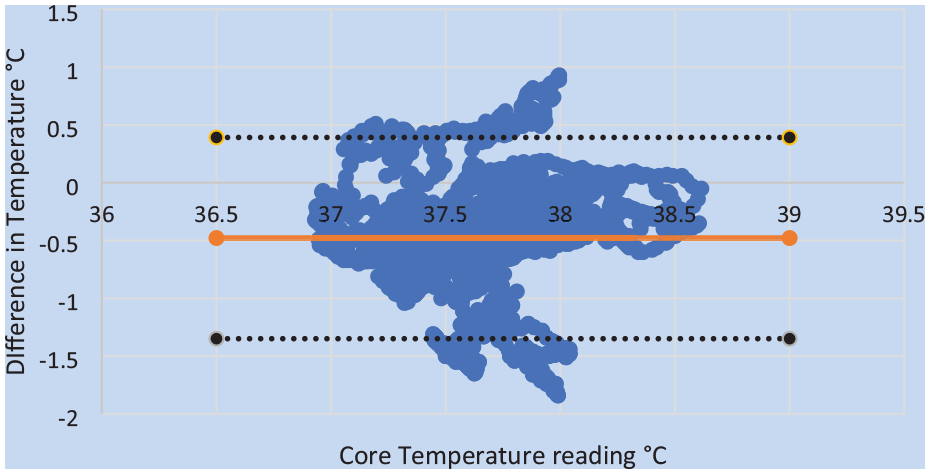
Bland–Altman Plot of the Differences Between Measured Temperature With Slate Safety Device and Ingestible Core Temperature Measuring Pill
Participant temperatures ranged from 36.68°C to 38.59°C (98.02°F to 101.46°F) and 36.89°C to 38.91°C (98.40°F to 102.04°F) as read by the ingestible pill and wearable device, respectively. Individual participant correlations between the core temperature measurements using the ingestible pill and the wearable device are included in Table 2. A significant correlation of .26 (p < .001) was noted between the ingestible pill and the wearable device with a 95% confidence interval of 0.23 to 0.29. Aggregate core temperature data demonstrated an MSE of 0.43, an RMSE of 0.65, an MAE of 0.54, and an MBE of −0.48. Accuracy for both peaks and averages are presented in Table 2, with an overall accuracy of −0.61% and −0.56%, respectively, across the nine participants.
Correlation and Accuracy Data Comparing Ingestible Pill to Slate Safety Wearable Device
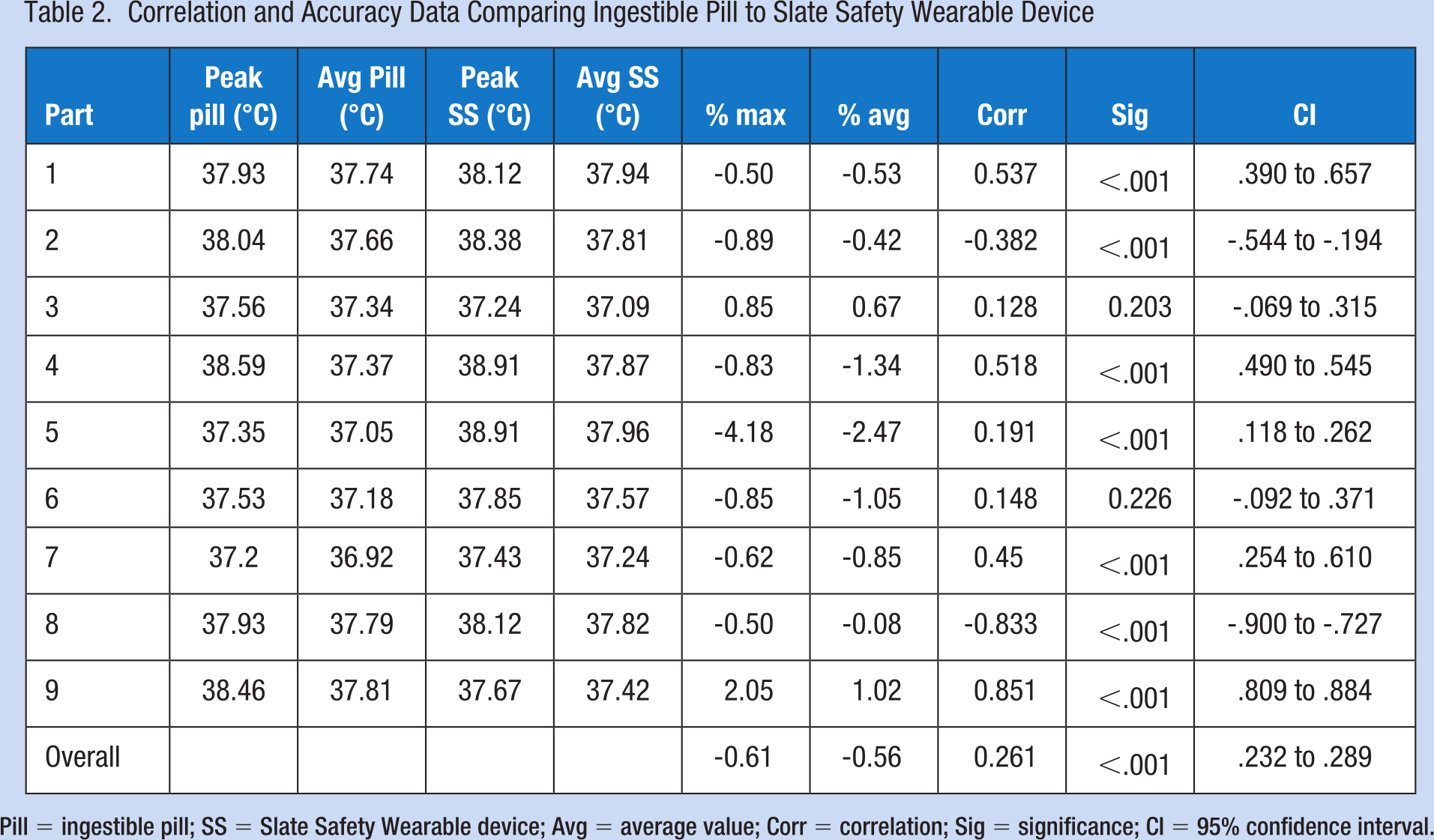
Pill = ingestible pill; SS = Slate Safety Wearable device; Avg = average value; Corr = correlation; Sig = significance; CI = 95% confidence interval.
Data were separated into temperature ranges as read by the ingestible core temperature pill to include the ranges of 36°C to 37°C (96.8°F to 98.6°F), 37°C to 38°C (98.6°F to 100.4°F), and 38°C to 39°C (100.4°F to 102.2°F). Mean square error, RMSE, MAE, and MBE for each temperature range are displayed in Table 3. Of note, all participants recorded a temperature within the 37°C to 38°C (98.6°F to 100.4°F) range, six had temperatures that were in the 36°C to 37°C (96.8°F to 98.6°F), and only three participants achieved a temperature above the 38°C (100.4°F) mark. Specificity and sensitivity of the Slate Safety device to predict a core temperature greater than 38°C were 80.4% and 74.2%, respectively, with a positive predictive value (PPV) of 26.7%.
Results for MSE, RMSE, MAE, and MBE Based on Core Temperature as Measured by Ingestible Core Temperature Monitoring Pill
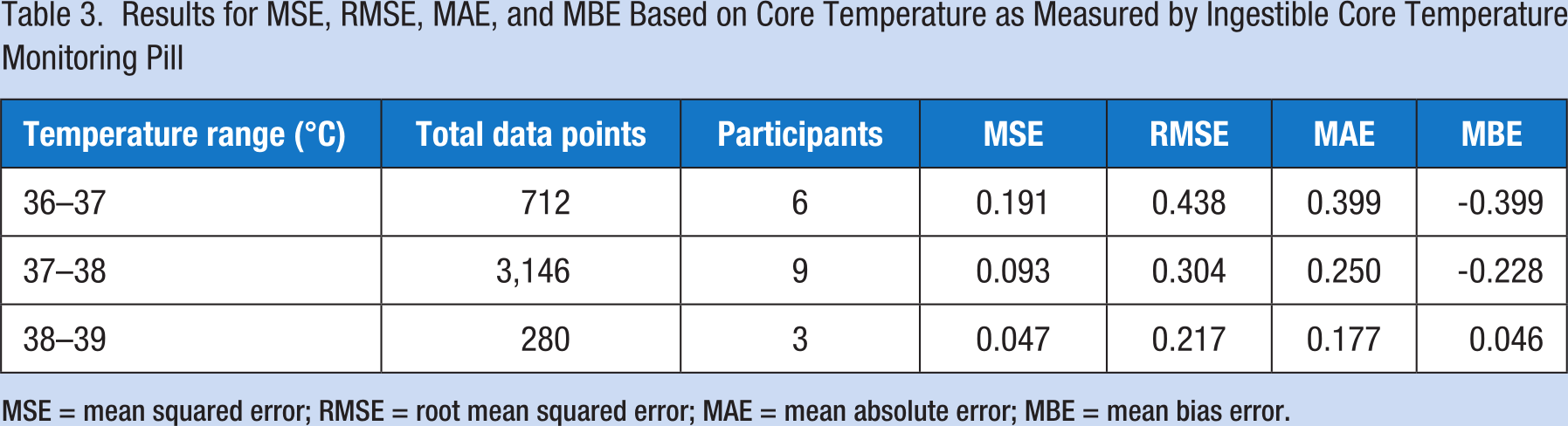
MSE = mean squared error; RMSE = root mean squared error; MAE = mean absolute error; MBE = mean bias error.
Discussion
A significant correlation was found between the ingestible pill reading and the Slate Safety wearable device estimation (.26) slightly less than the (.595) found in previous studies from Callihan et al. (2023) and the (.543) by Ibrahim et al. (2023). This weaker correlation, while still statistically significant, raises concern with the ability of the Slate Safety wearable device to track the temperature with as much accuracy and precision as possible. Given the variability in each participant, temperature and humidity of the environment, and job tasks being performed during the flights, caution should be exercised when instituting a wearable device in different work environments. While the exact algorithm used with the Slate Safety Device is not known by the research team, due to LED technology typically focusing on heart rate and blood flow (Alugubelli et al., 2022), it is assumed that heart rate is the main variable that contributes to the estimation. Environmental factors (radiant heat sources, air flow) and individual characteristics of the employee (body mass, sweat production, inflammation, edema) can lead to barriers for accurate measurement of these variables (Bent et al., 2020). Beyond these, it is speculated that limitations may exist related to the proprietary algorithm which are unknown. Testing should occur to validate accuracy in each variable.
This pilot study found that on average the temperature reading for the Slate Safety wearable was 0.48°C (0.86°F) higher than the ingestible pill. In previous research, Callihan et al. (2023) found the average temperature 0.04°C higher while Ibrahim et al. (2023) found the temperature 0.20°C higher. The differences noted may be attributed to either the temperature ranges or the wearing of flame-resistant flight suits by the flight crews. With a reported acceptable bias error of ±0.5°C in previous work, the bias noted in the wearable device is important but is acceptable and as indicated in the Bland–Altman plot (Figure 3) could be considered small (Ibrahim et al., 2023). Nonetheless, the overestimation of the wearable device provides a safety factor ranging from 0.03°C as seen in the Callihan et al. (2023) to the 0.478°C (0.861°F) seen in the current pilot study, in the estimation of the core temperature for the worker.
When separating the data based on measured core temperature, we found that the lowest and middle temperature range (i.e., 36°C–37°C, and 37°C–38°C) had higher variability compared with the highest temperature range (i.e., 38°C–39°C) as indicated by MSE, RMSE, and MAE values. Moreover, the lowest and middle temperature range contributed to the overall underestimation with the Slate Safety device (MBE value = −0.48°C) while the highest temperature range demonstrated the only MBE with a positive value, indicating a slight temperature overestimation (0.046°C). Given the imbalanced sample size between temperature groups, future research should focus on larger sample sizes with more control on temperature ranges and activities performed.
The ability of the Slate Safety device to predict core temperatures higher than 38°C (100.4°F) was examined and demonstrated a sensitivity of 74.2% and a specificity of 80.4% despite the PPV of only 26.7%. This finding demonstrates the ability of the Slate Safety wearable device to predict the higher core temperature as high, with the PPV explained by the higher level of false-positive results. This higher level of false-positive results (Slate Safety being greater than 38°C with pill reading less than 38°C) would be considered acceptable in that the occupational health professional would be able to evaluate an individual who was approaching being at risk.
The study conducted by Callihan et al. (2023) had a set temperature value of either 21.7°C or 29°C (71°F or 84°F) while the Ibrahim et al. (2023) study maintained a temperature of 33°C (91.4°F). The temperature could not be controlled for in this pilot study and ranged between 23.9°C and 35.5°C (75°F to 96°F), with an average of 30.4°C (86.7°F). These temperature differences may account for the differences noted in the average bias error between systems. Future work should provide for more controlled temperature and humidity conditions to compare devices. A second factor that may account for the difference is the lack of ability to monitor and control the relative humidity and temperature within the flight suit of the worker during data collection for this pilot study. The PPE being worn does not allow for the environment, the skin, and, in turn, the Slate Safety wearable device to be monitored or controlled. Skin contact may also encounter interference between the participant and the monitoring device due to excessive sweat that is not able to evaporate efficiently inside the restrictive flight suit. Future studies should explore this variable more in-depth to determine the impact on the Slate Safety wearable device.
During this pilot study, data were collected while the participants were on emergency medical flights; however, the specific tasks being performed during the flights varied as is the nature of emergency work. The ability to remotely monitor the physiologic parameters of the participants regardless of their tasks was highly successful, with only 37 data points missing across the duration of the pilot study. Nearly 70 hours (4,139 minutes) of data were collected and only 37 minutes were missed. Remotely monitoring the worker is crucial for in-flight programs and any work environment where direct supervision is not possible. This pilot study found that the Slate Safety Band V2 can accurately measure core temperature in HEMS crews when compared with the ingestible core temperature monitoring devices, indicating this device is a valid and reliable tool in remotely monitoring the physiological status of HEMS crews. Continued research is needed to further validate this technology within other occupational settings.
Several limitations were noted for this pilot study, including the small sample size and lack of controls for participant size, actions being performed, and climate within the helicopter. Despite the sample size of participants being only nine, a total of 4,139 data points were examined for comparison between the ingestible core temperature monitoring pill and the Slate Safety device. To improve on this weakness, future studies should include a larger sample size with a more diverse sample to include different skin tones and body composition. The lack of ability to control the conditions within the helicopter, such as ambient temperature, humidity, and tasks being performed, was necessary for this observational pilot study but did not allow for analysis of the accuracy of the Slate Safety device with these variables. Future research should control for these variables during the assessment.
Implications for Occupational Health Practice
With the increase in global warming, heat stress is of great concern in the community and industry (Fotso-Nguemo et al., 2023; Wolkoff et al., 2021). Having a means to monitor heat stress among workers is a critical step in limiting the risk of developing heat injury or illness. While current practice is to monitor the conditions of the work environment, acclimate workers, and build in cooling mechanisms, the need remains for monitoring of individual workers (Jacklitsch et al., 2016). When working in a hot environment, physiological changes occur in the worker, including an increased metabolic rate, increased sweat production, an elevation in the core temperature, and an increased heart rate (Institute of Medicine, 1993; Periard et al., 2016). Monitoring individual physiological changes related to the hot environment could be instrumental in reducing the incidence of heat-related injury.
When selecting a monitoring device, one must look at cost, reliability, accuracy and precision, and the ability to remotely monitor the employee. While the standard of measurement of core temperature is the use of an ingestible pill or a rectal thermistor, these options are not always cost-effective and are often found invasive by workers. It was found that workers were more willing to participate in physiological monitoring studies when using the non-invasive wearable technology over the ingestion of the core temperature monitoring pill (Callihan et al., 2023). Despite the upfront investment necessary for the wearable technology, it may be more economical in the long run and yield better compliance with use among workers.
While current practice for managing heat stress risk factors hinges on environmental factors, it is critical to add individual monitoring as a tool in our efforts in limiting heat-related illness. The added ability to monitor the individual physiologic response to heat stressors will allow for more precision and individualization in heat illness prevention efforts. Wearable sensor technology can accurately monitor workers remotely (Callihan et al., 2023; Ibrahim et al., 2023; Moyen et al., 2021) as an additional tool in planning preventive measures on hot days or when working in hot environments. The occupational health worker should test these devices within their work environment to determine whether the use of wearable technology can improve the safety and wellness of the workers they serve.
Helicopter-based emergency medical services crews are subjected to high stress conditions in often high temperature environments. It is crucial that physiological monitoring be added to the continued efforts of ensuring adequate hydration, providing cooling areas or devices, and built in recovery times following flights. Helicopter-based emergency medical services crews risk their lives for the good of others, and it is vital to protect them from environmental risks.
In summary,
The ability to monitor the physiological parameters of a worker allows for the occupational health professional to recognize workers at risk for heat illness and take preventative measures before injury occurs.
Wearable technology adds the ability for occupational health professionals to remotely monitor the physiological parameters of workers, adding a layer of safety when working in a hot environment.
The Slate Safety Band V2 wearable device provides accuracy within 0.478°C (0.861°F) when compared with the ingestible core temperature monitoring pill in real time.
Wearable technology allows occupational health professionals to remotely monitor workers with minimal lost data.
Footnotes
Acknowledgements
Special thanks to Regional Air Medical Services, Jasper, Alabama, for allowing us to conduct this research study.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The financial support through the University of Alabama, 2023 Office for Research & Economic Development Small Grants Program.
Ethical Approval
Approval for this study was obtained through the University of Alabama IRB on March 30, 2023, protocol #22-12-6226.