
Abstract
Background:
Healthcare professionals work in challenging environments with extended working hours and excessive workloads to provide high-quality care. However, they hardly get the time to care for themselves. Online mindfulness-based interventions—which are not restricted by time or location—can be a powerful strategy to help healthcare professionals.
Objectives:
This scoping review aims to explore the current evidence about online mindfulness-based interventions for healthcare professionals.
Design:
A scoping review was conducted.
Methods:
A literature search was conducted to retrieve articles published between October 2016 and March 2023 in seven databases, including backward and forward citation tracking from the included articles. Among 1,278 articles retrieved, 33 met the criteria for review.
Results:
Two-thirds of the studies utilized commercialized mindfulness programs (n = 22). Duration of the mindfulness interventions varied from 1 week to 4 months, and half of the studies used audio-guided programs. Online mindfulness-based intervention studies were targeted to reduce burnout (n = 26), and the majority reported reduction in burnout (n = 18).
Conclusion:
Most studies used individual audio-guided programs that warrant the use of diverse delivery methods such as video media, simulation, and virtual reality for interactions in the future. Although the literature has accumulated evidence for commercialized online mindfulness-based interventions, further studies are needed to develop and test tailored interventions for healthcare professionals.
Background
The working environment of healthcare professionals such as nurses and doctors is known to be very challenging. This is because these professionals experience excessive workloads; patient deaths; unjustified demands such as responding promptly to individual, specific, and trivial requests from patients and caregivers; and conflicts with colleagues (Stodolska et al., 2023). The provision of high-quality medical services is affected significantly by the international phenomenon of healthcare professional burnout (Salyers et al., 2017; Shanafelt et al., 2009). In previous research, 51% of medical residents reported experiencing burnout (Low et al., 2019), and the prevalence of nurse burnout in various settings, such as hospitals, clinics, and industrial sites, was high, ranging from 29% to 36% (Gómez-Urquiza et al., 2017; Membrive-Jiménez et al., 2020). The experience of burnout can result in clinical errors (Shanafelt et al., 2009) and turnover intent (Scanlan & Still, 2019) and is ultimately detrimental to patient safety and the quality of healthcare (Salyers et al., 2017). In addition, healthcare professionals are vulnerable to developing secondary traumatic stress due to their constant exposure to distressing experiences experienced by their patients (Melinte et al., 2023). To make matters worse, healthcare professionals have been affected by extended working hours, sleep difficulties, exhaustion, and risk of infection due to the COVID-19 pandemic (Moazzami et al., 2020). As a result, 51% of healthcare professionals in 33 countries have experienced burnout during the pandemic (Morgantini et al., 2020). This is an increase from previous studies showing that 30% to 45% of healthcare professionals experienced burnout before the COVID-19 pandemic (Shanafelt et al., 2009, 2012).
Mindfulness-based interventions are an effective method for reducing burnout (Luken & Sammons, 2016). Mindfulness refers to paying attention to the present moment and accepting the sensations, emotions, and thoughts that come to mind (Kabat-Zinn, 2003). By using mindfulness to view one’s problems or relationships with others, one can escape the pain caused by subjective judgment and excessive concentration of the way of thinking (Park, 2017). In a previous study, engaging in mindfulness-based stress reduction (MBSR) decreased depression, anxiety, and stress along with burnout in physicians (Fortney et al., 2013). Mindfulness training significantly reduces the signs and symptoms of burnout among nurses (Mackenzie et al., 2006), and MBSR programs have been effective in reducing job stress and burnout among healthcare professionals (Luken & Sammons, 2016).
Even if mindfulness-based interventions are successful in reducing healthcare professionals’ burnout, it may be difficult to provide in-person interventions owing to time and location restrictions. The participation time limit was highlighted in the intervention research on healthcare professionals (Shapiro et al., 2005), and medical staff generally complained about not having enough time to attend programs (Coster et al., 2020). In addition, due to COVID-19, health-related arbitration is often carried out virtually through online and smartphone applications (Bossi et al., 2022). This has increased the adoption of digital health technologies (Mbunge et al., 2022). Consequently, research that combined in-person and non-face-to-face interventions started to appear in mindfulness-based intervention studies (Nguyen et al., 2020). In a meta-analysis of mindfulness-based interventions for physicians, 7 of 25 studies involved mixed in-person and non-face-to-face interventions (Fendel et al., 2021), indicating a movement away from in-person interventions toward non-face-to-face interventions.
According to previous studies, mindfulness-based interventions delivered through smartphone applications significantly increase mindfulness levels, such as by paying attention to the present moment and accepting the sensations, emotions, and thoughts that come to mind (Wen et al., 2017). The data have shown that online mindfulness-based interventions have helped reduce stress and improve mindfulness (Y. Zhang et al., 2020). Thus, online interventions may be as effective as in-person interventions owing to technological advancements (A. Zhang et al., 2019). In-person mindfulness interventions involve MBSR, movement meditation, and mindfulness meditation (Spinelli et al., 2019). Online mindfulness-based interventions also consist mainly of MBSR and mindfulness meditation (Y. Zhang et al., 2020). This suggests that there are no restrictions in providing the existing mindfulness programs online.
Although a literature review that identifies the effect of mindfulness-based interventions on burnout for healthcare professionals has been conducted, it only targeted in-person interventions, and research on online interventions tailored to the current trend is insufficient. Therefore, this study identified the effectiveness of online mindfulness-based interventions for healthcare professionals through a scoping review.
Objectives
This scoping review aimed to explore the body of knowledge on the online mindfulness-based interventions for healthcare professionals. Specifically, it examined the study characteristics, intervention characteristics (core components, mode of delivery, duration, and dropout rate), measured variables, and effects of the intervention.
Methods
Study Design
A scoping review maps the relevant literature in the field and is useful to identify gaps in the existing literature (Arksey & O’Malley, 2005). Arksey and O’Malley’s framework was adopted for this review: (a) stating the research question, (b) identifying the relevant literature, (c) selecting the literature, (d) charting the data, and (e) collating, summarizing, and reporting the results. These five stages were followed and provided a structured approach to explore the current evidence through an examination of the existing literature. Quality of the included papers was not rated as scoping studies do not require evaluation of the quality of the literature (Levac et al., 2010). Therefore, a scoping review is suitable to provide a broader perspective on current research on the topic and map the relevant literature on the effect of online mindfulness-based interventions on healthcare professionals.
Stating the Research Question
The research question for this scoping review was, “What is the current evidence on the characteristics, measured variables, and effects of online mindfulness-based interventions for healthcare professionals?”
Identifying the Relevant Literature
The search strategy involves identifying relevant studies, including published and unpublished work, with an emphasis on being as comprehensive as possible (Arksey & O’Malley, 2005; Gottlieb et al., 2021). In 2023, literature was searched in the following nine databases: five global search engines in English (PubMed, Embase®, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature, and ProQuest Dissertations & Theses Global) and two domestic Korean search engines (Korean Studies Information Service System and Research Information Sharing Service). Various combinations of search terms (see Box 1) were used to either broaden or narrow the search depending on the results in a specific database. Furthermore, reference lists of the articles were searched manually. Finally, gray literature such as doctoral theses, research institute reports, non-peer-reviewed literature and academic conference presentations, relevant letters, and editorials were searched.
Query Box
Selecting the Literature
Articles published between October 2016 and March 2023 were selected. Articles retrieved from the literature search were reviewed by four researchers using the following inclusion and exclusion criteria:
Inclusion criteria: (a) Studies that tested the effect of online mindfulness-based interventions, including online–offline mixed interventions if the online components consisted of mindfulness (e.g., 6-week program: 4-week online and 2-week offline); (b) participants of the studies were licensed healthcare professionals, physicians/surgeons, dentists, doctors, and registered nurses or licensed practice/vocational nurses who treated patients directly in hospitals; and (c) articles were written in English or Korean.
Exclusion criterion: Participants of the studies included nonlicensed healthcare professionals such as hospital administrative staff.
A total of 1,278 articles were retrieved from the initial database search (Figure 1). After removing duplicates, 946 articles remained. The titles and abstracts were reviewed, and 806 articles were excluded, leaving 140 articles for a full-text review. Thirty-one articles were identified as fully meeting the inclusion criteria. Reference lists were then reviewed, which yielded 11 additional articles, of which two met the inclusion criteria. Finally, 33 articles were included in this scoping review.
Flowchart
Throughout the review process, two researchers took the lead in data extraction, and all researchers reviewed the contents. Uncertainties and disagreements were resolved through weekly meetings. The literature review software Covidence (https://covidence.org), an article-managing tool for collaborating researchers (Babineau, 2014), was used to manage the retrieved studies and screen for redundant studies.
Charting the Data
Data were presented in tables, summarized, and synthesized qualitatively according to the purpose and research question of this review.
Collating, Summarizing, and Reporting the Results
The final stage of a scoping review involves collating, summarizing, and reporting the results (Arksey & O’Malley, 2005). For this scoping review, data related to the study characteristics included the author, publication year, study participants, interventions, follow-up time points, and measurement tools. Data related to intervention characteristics included the core content of the intervention, mode of delivery, duration, and dropout rate. Moreover, measurement variables of the online mindfulness-based interventions were presented. Four researchers were divided into two groups of two. The two groups independently extracted data by viewing all full texts. Inconsistencies between the researchers were discussed and agreed upon.
Results
Characteristics of the Retrieved Studies
Characteristics of the retrieved articles are described in Table 1. Most studies were conducted in the United States (n = 27), followed by the United Kingdom (n = 2), Australia (n = 1), Brazil (n = 1), Kuwait (n = 1), and Mexico (n = 1). More than half of the studies were implemented during the COVID-19 pandemic (n = 19), while some were implemented before the pandemic (n = 11). The remaining studies did not mention the implementation period (n = 3).
Study Characteristics
Note. aMBI = abbreviated Maslach Burnout Inventory; ACE = adverse childhood experiences survey; BAI = Beck Anxiety Inventory; BCSQ = Burnout Clinical Subtypes Questionnaire; BDI = Beck’s Depression Inventory; BRS = Brief Resilience Scale; C = control group; CAMS-R = Cognitive and Affective Mindfulness Scale–Revised; CBI = Copenhagen Burnout Inventory; CCCS = Confidence in providing Calm, Compassionate Care Scale; CD-RISC = Connor-Davidson Resilience Scale; CFS-CPV = Caring Factor Survey–Care Provider Version; CFST = Compassion Fatigue Self-Test; CPSS = Cohen Perceived Stress Scale; DRS = Dispositional Resilience Scale; E = experimental group; FFMQ = five facet mindfulness; FMI = Freiburg Mindfulness Inventory; GAD = General Anxiety Disorder Scale; HSRQ = Headspace® Self-Report Questionnaire; LEC = Life Events Checklist; MAAS = Mindfulness Attention Awareness Scale; MBI = Maslach Burnout Inventory; MBI & AWS = Maslach Burnout Inventory Areas of Work-Life Survey; MBI-HSS = Maslach Burnout Inventory Human Services Survey; MBI-HSSMP = Maslach Burnout Inventory Human Services Survey Medical Personnel; MBSR = Mindfulness-Based Stress Reduction Program; MICU = medical intensive care units; MMBI-EE = Modified Maslach Burnout Inventory; MNPJSS = Misener Nurse Practitioner Job Satisfaction Scale; NA =not available; NPRS = Numeric Pain Rating Scale; OLBI = Oldenburg Burnout Inventory; OSUWMC = Ohio State University Wexner Medical center; PANAS = Positive and Negative Affect Schedule; PCE = Positive Childhood Experiences Survey; PCL-C = Posttraumatic Stress Disorder Checklist Civilian; PHQ = Patient Health Questionnaire; PERMA Profiler = Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment; PNAS = Positive and Negative Affect Schedule; ProQOL = Professional Quality of Life Scale; PSS, Perceived Stress Scale; PSQI = Pittsburgh Sleep Quality Index; PWBI = Physician Well-Being Index; RMRS = Rushton Moral Resilience Scale; RSES = Response to Stressful Events Scale; SBRS = Smith’s Brief Resilience Scale; SCS = Self-Compassion Scale; SCS-SF = Self-Compassion Scale–Short Form; SD = standard deviation; SICU = surgical intensive care units; UK = United Kingdom; USA = United States; WBI = Well-Being Inventory; WEMWBS = Warwick-Edinburgh Mental Wellbeing Scale.
A large number of studies adopted quasi-experimental designs (n = 28); these were followed by randomized controlled trial studies (n = 3), a development study (n = 1), and a prospective cohort study (n = 1). A small number of studies had both intervention and control groups (n = 4), while the remaining studies had only intervention groups (n = 29). The number of participants varied among the studies, with the smallest sample size being 3 (Ruiz, 2020) and the largest being 643 (Cepeda-Lopez et al., 2023). Participant types included nurses (n = 15), doctors (n = 13), nurse practitioners (n = 2), nurse leaders (n = 1), and a combination cross occupation (n = 2).
Two studies collected qualitative data: In one study, open-ended survey questions via a website were used to evaluate burnout postintervention (Khalid, 2021), and in the other study, online interviews via Zoom were conducted to obtain participant feedback on the intervention (Gbeddy, 2021). One study collected biological biomarkers such as serum cortisol levels and pulse rate (Valluri, 2022).
Online Mindfulness-Based Interventions
A description of the interventions is presented in Table 2. Among the 33 studies, two-thirds (n = 22) utilized previously developed mindfulness programs, and 6 studies developed a program tailored to the participants directly. In five studies, the previously developed program was modified slightly.
Intervention Characteristics
Note. C = control group; DP = depersonalization; E = experimental group; EE = emotional exhaustion; FMI = Freiburg Mindfulness Inventory; MAAS = Mindful Attention Awareness Scale; MBSR, mindfulness-based stress reduction; NA, not available; PA, personal accomplish; PAS, positive affect score; VR, virtual reality.
The core components of the interventions included a combination of meditation, informal practice, and movements. The type of meditation used in the studies included awareness such as through a body scan, breathing (n = 26), loving-kindness (n = 4), self-compassion (Pandit et al., 2022), and cognitive behavioral therapy (Counson et al., 2021). The movements included sitting, walking, adopting yoga postures, and stretching. In three studies, journaling or writing was included in the interventions. One study included a practice that could solve job-related difficulties (Hanson et al., 2022).
The modes of delivery used in the retrieved studies were mobile applications (n = 21) and a web-based platform (n = 6). In three studies, mindfulness-based interventions were guided through videoconferencing software such as Zoom, and in two studies, they were guided through email. One study used a sound machine and virtual reality (VR) device (Muir et al., 2022). About half of the studies adopted a voice-guided method for delivery (n = 18), and a video-guided method was also adopted (n = 5). In one study, the program was delivered through VR (Weitzman et al., 2021), and in another study, the program was delivered through both VR and video and was voice-guided (Muir et al., 2022). In the remaining studies, the delivery method was not mentioned (n = 8).
The duration of the intervention varied: 1 week (Ruiz, 2020), 10 days (Taylor et al., 2016), 2 weeks (n = 3), 3 weeks (n = 2), 4 weeks (n = 8), 6 weeks (n = 9), 2 months (n = 2), 3 months (n = 5), and 4 months (n = 2). Interventions in approximately half of the studies were provided daily (n = 18); in one study, it was provided 5 days a week (Haskins, 2018), and in some, it was provided weekly (n = 4). Some studies encouraged participants to do as much as they could, such as self-assessments after the course or Zoom meeting (n = 4). The remaining studies did not mention the interventions’ frequency (n = 6). Each session lasted for less than 30 minutes (n = 20) or between an hour and 2 hours (n = 4). Some did not describe the length of their program sessions (n = 4) or flexibility regarding the time for participation (n = 5).
The dropout rate also varied which included more than 50% (n = 3), 30% to 50% (n = 12), 10% to 30% (n = 6), less than 10% (n = 4), and none (n = 9). Some studies described their strategies to enhance participant engagement and reduce dropout, and the most frequently used strategy was giving rewards (n = 5), and sending messages and/or emails to remind participants (n = 5). Strategies from other studies included making phone calls (Gbeddy, 2021), asking participants to be self-motivated by using journaling (Best et al., 2020), and using calendars (Khalid, 2021).
Measured Variables of the Interventions on Healthcare Professionals
Measured variables of the interventions on healthcare professionals are presented in Table 3. The most commonly used outcome measure was burnout (n = 26), followed by mindfulness (n = 11), stress (n = 10), resilience (n = 7), anxiety (n = 5), compassion satisfaction (n = 5), depressive symptoms (n = 5), secondary trauma (n = 5), well-being (n = 5), self-compassion (n = 3), compassion fatigue (n = 1), job satisfaction (n = 1), and sleep quality (n =1).
Measured Variables of the Online Mindfulness-Based Interventions Among Healthcare Professionals
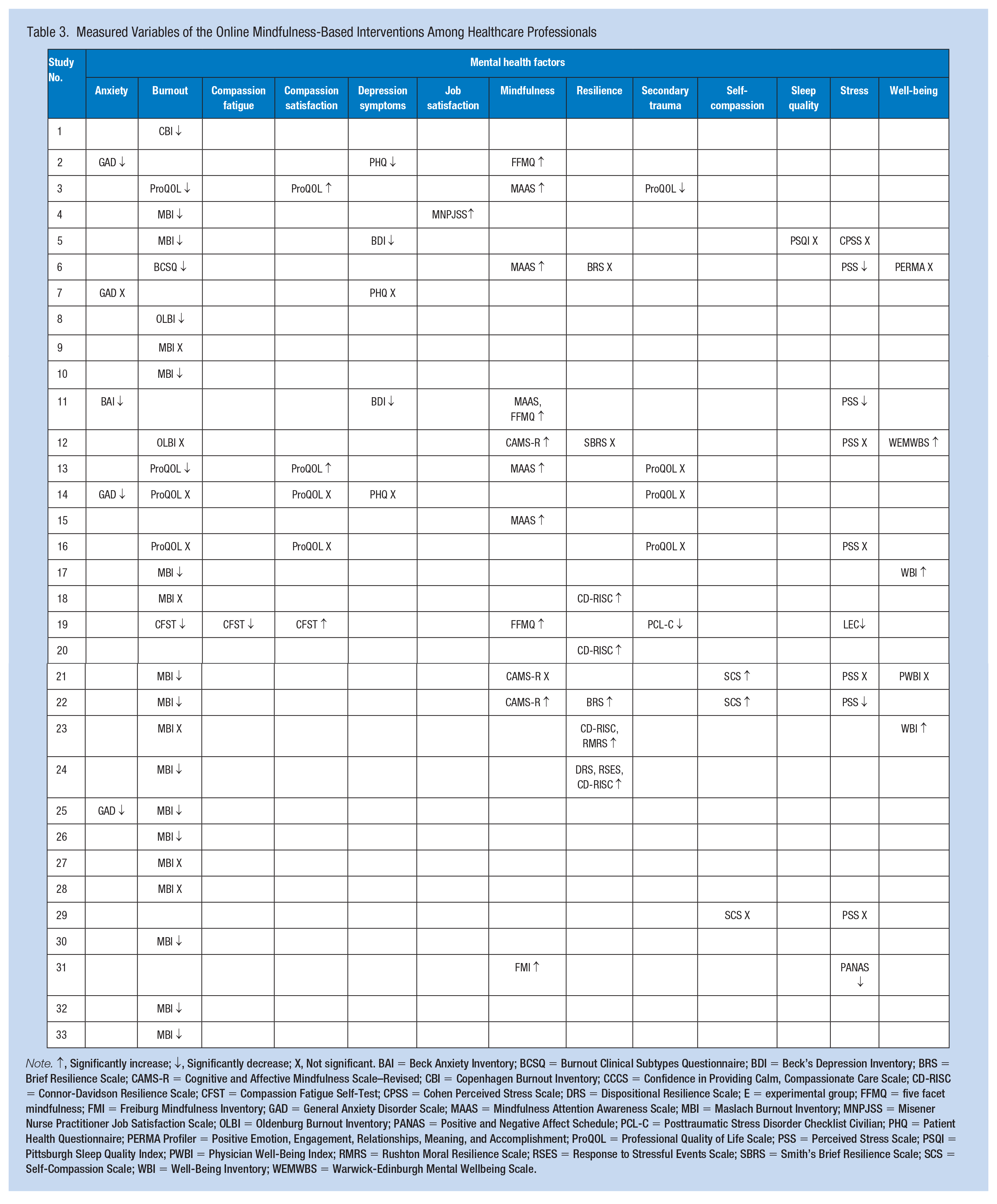
Note. ↑, Significantly increase; ↓, Significantly decrease; X, Not significant. BAI = Beck Anxiety Inventory; BCSQ = Burnout Clinical Subtypes Questionnaire; BDI = Beck’s Depression Inventory; BRS = Brief Resilience Scale; CAMS-R = Cognitive and Affective Mindfulness Scale–Revised; CBI = Copenhagen Burnout Inventory; CCCS = Confidence in Providing Calm, Compassionate Care Scale; CD-RISC = Connor-Davidson Resilience Scale; CFST = Compassion Fatigue Self-Test; CPSS = Cohen Perceived Stress Scale; DRS = Dispositional Resilience Scale; E = experimental group; FFMQ = five facet mindfulness; FMI = Freiburg Mindfulness Inventory; GAD = General Anxiety Disorder Scale; MAAS = Mindfulness Attention Awareness Scale; MBI = Maslach Burnout Inventory; MNPJSS = Misener Nurse Practitioner Job Satisfaction Scale; OLBI = Oldenburg Burnout Inventory; PANAS = Positive and Negative Affect Schedule; PCL-C = Posttraumatic Stress Disorder Checklist Civilian; PHQ = Patient Health Questionnaire; PERMA Profiler = Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment; ProQOL = Professional Quality of Life Scale; PSS = Perceived Stress Scale; PSQI = Pittsburgh Sleep Quality Index; PWBI = Physician Well-Being Index; RMRS = Rushton Moral Resilience Scale; RSES = Response to Stressful Events Scale; SBRS = Smith’s Brief Resilience Scale; SCS = Self-Compassion Scale; WBI = Well-Being Inventory; WEMWBS = Warwick-Edinburgh Mental Wellbeing Scale.
Anxiety, burnout, compassion fatigue, depression symptoms, secondary trauma, and stress were variables that decreased after applying online mindfulness-based interventions. Providing the interventions significantly reduced burnout in 18 studies but not in 8 studies. Among the 18 studies that showed reduction on burnout, the Maslach Burnout Inventory (MBI; n = 12) was the most used, followed by the Professional Quality of Life (ProQOL; n = 2), Oldenburg Burnout Inventory (n = 1), Burnout Clinical Subtypes Questionnaire (n = 1), Copenhagen Burnout Inventory (n = 1), and Compassion Satisfaction/Fatigue Self-Test (CFST; n = 1). The intervention reduced stress in half of the studies (n = 5) that measured stress. Moreover, among the tools that reduced stress in these studies, the Perceived Stress Scale (n = 3) was the most common, followed by the Life Events Scale (n = 1) and Positive and Negative Affect Schedule (n = 1). Anxiety was decreased in four studies, leaving one study with no significant change. The tools used to reduce anxiety in these studies included the Generalized Anxiety Disorder Assessment (n = 3) and Beck Anxiety Inventory (n = 1). Depressive symptoms were decreased in three studies, while in two studies the result was not significant. The tools used to reduce depressive symptoms in these studies were the Beck Depression Inventory (n = 2) and Patient Health Questionnaire (n = 1). For secondary trauma, more studies reported that the intervention did not result in a significant change (n = 3) compared with those reporting a reduction in symptoms (n = 2); compassion fatigue decreased in one study (n = 1).
Compassion satisfaction, job satisfaction, mindfulness, resilience, self-compassion, and well-being were variables that significantly increased after applying the online mindfulness-based interventions. Mindfulness was significantly increased in 10 studies, while the intervention led to no change in one study. Among the 10 studies that showed increased mindfulness, the Mindful Attention Awareness Scale (MAAS; n = 4) was used the most, followed by the Five Facet Mindfulness Questionnaire (FFMQ; n = 2), Cognitive and Affective Mindfulness Scale–Revised (n = 1), Freiburg Mindfulness Inventory (n = 1), and co-measurement of MAAS and FFMQ (n = 1). Resilience increased in five studies but not in two studies. Among the 10 studies that showed increased resilience, the Connor-Davidson Resilience Scale (CD-RISC; n = 2) was used the most, followed by the Brief Resilience Scale (n = 1), co-measurement of the CD-RISC and Rushton Moral Resilience Scale (n = 1), and co-measurement of the CD-RISC, Dispositional Resilience Scale, and Response to Stressful Experiences Scale (n = 1). Compassion satisfaction increased in three studies but not in two studies. The tools that increased compassion satisfaction in the studies were ProQOL (n = 2) and CFST (n = 1). Well-being increased in three studies, while it was not significant in two studies. In these studies, the tools that showed increased well-being were the Well-Being Inventory (n = 2) and Warwick-Edinburgh Mental Wellbeing Scale (n = 1). Self-compassion increased in two studies, but not in one study, and job satisfaction increased in one study (n = 1).
Finally, the intervention did not affect sleep quality in one study (Carullo et al., 2021).
Discussion
In the studies considered in this scoping review, online mindfulness-based interventions consisted of various activities such as mindful movement, walking meditation, mindfulness exercises, breathing exercises, cognitive behavioral therapy, and communication skills. These interventions were similar to the in-person mindfulness-based interventions reported in a recent review study (Suleiman-Martos et al., 2020). In their study, the components of online mindfulness-based interventions were body scans, physical activity, breathing exercises, cognitive training therapy, and communication skills; the interventions did not consider aromatherapy or music. However, if online mindfulness-based interventions that integrate multiple senses are developed by adding auditory elements such as music and olfactory elements like aromatherapy to the existing interventions, their content components will become more abundant.
More than half of the studies included in this review delivered the interventions through voice-guided messages, while only 7 of 33 used video guides or VR. However, for those with little experience in mindfulness, it might be challenging to determine whether attention and movement are being performed properly by just following the audio guides. Participants having difficulties in comprehending body movements might reduce their compliance (Navarro-Haro et al., 2019). Therefore, it is recommended that the limitations of existing meditation delivery methods be improved by adding visual interest elements into the process (Oh et al., 2018). For example, the intervention can include a background of natural environments such as rivers and forests or use a character as an instructor to guide movements. Virtual reality, a method of adding visual interest elements of mindfulness, has been shown to improve participant satisfaction due to its high level of immersion, providing the illusion of being there (Navarro-Haro et al., 2019). Mindfulness-based VR was developed and applied to various patients, such as those with an anxiety disorder, borderline personality disorder, or spinal cord injury, and it was reported that the intervention was effective in improving anxiety, depression, and reduced stress (Flores et al., 2018; Navarro-Haro et al., 2019). However, only two studies reported using mindfulness-based VR intervention for service providers in this study (Muir et al., 2022; Weitzman et al., 2021). Therefore, further studies should be conducted to develop mindfulness-based VR interventions for healthcare professionals.
According to the findings, 22 of 33 studies utilized previously developed commercial programs, while 6 studies developed interventions tailored to their participants. According to the previous research, a tailored mindfulness-based program developed for resident physicians resulted in 93% of the participants completing the program and thus lowered dropout rates (Aeschbach et al., 2022). Similarly, in this review, the dropout rate of participants using interventions that were not tailored varied from 10% to more than 50% of total participants, while the dropout rate of all tailored program participants was less than 10%. A tailored program could motivate participants to continue the program and reduce dropout rates. Therefore, it would be beneficial to develop tailored interventions that consider the uniqueness of the job characteristics of healthcare professionals.
One advantage of an online mindfulness-based intervention is that it is not limited by time and space. For this reason, online mindfulness-based interventions could be a good fit for healthcare professionals who often work shifts (Aikens et al., 2014). Even still, in this review, 15 of 33 studies had a dropout rate of more than 30%. Online-based approaches are difficult to manipulate because they require installing and accessing an online program (Gbeddy, 2021). Moreover, there is no direct contact with the project director; thus, adherence has proven challenging (Yogeswaran & El Morr, 2021). In this review, several strategies were utilized to improve adherence, including gift card drawings, phone calls, Zoom meetings, emails, and messages. In addition, in some studies, to increase participation rates, only the mindfulness components were conducted online, and offline meetings were held for introduction and discussion before and after the intervention. It has been reported that utilizing user interaction factors could reduce the dropout rate of participants (Oh et al., 2018). For example, if the metaverse, which interacts with people through avatars and VR technology, is used for intervention, it could improve not only adherence to the outcome but also the effect of a positive outcome (Yogeswaran & El Morr, 2021). Therefore, interaction between participants is a good alternative to reduce dropout rates.
The studies in our review used it in various ways for not only measuring the outcome but also evaluating each outcome. More than half of the studies included in this review reported measures for burnout after online mindfulness-based interventions for healthcare professionals. The most commonly used outcome measure of burnout was the MBI, which is the first scientifically developed burnout measurement method and is a widely used tool in various research (Williamson et al., 2018). This is consistent with the results of previous review studies that provided in-person mindfulness-based programs (Klein et al., 2020; Suleiman-Martos et al., 2020). In addition to burnout, stress, anxiety, and depression were measured. Online mindfulness-based interventions may reduce stress among healthcare professionals, which can reduce absenteeism and improve job satisfaction, benefiting employers, employees, and consequently patients and service users within the healthcare system (Burton et al., 2017). Moreover, online mindfulness-based interventions are increasing the level of mindfulness and resilience. This can benefit healthcare professionals’ not only hospital work and interpersonal relationships but also personal life (Lee & Jang, 2019). Therefore, prescribing a mindfulness-based program may be a strategy to prevent and reduce burnout, anxiety, depressive symptoms, and stress, as well as increase mindfulness, resilience, and self-compassion. However, reliability and validity of a measurement tool are important indicators of the quality of that measurement instrument (Kimberlin & Winterstein, 2008). Therefore, we suggest high-quality intervention studies that use validated and commonly used measurement methods to determine whether the instruments used help measure the desired effects of the intervention.
Limitations
This study has several limitations. First, nearly half of the selected studies were doctoral studies. As the proportion of dissertations without peer review accounted for half, the quality evaluation of the studies included documents with a high risk of bias. Second, in three studies, it was difficult to conclude that the results were the effect of online intervention. This is because there were cases in which an in-person discussion session was conducted in parallel after the online intervention. Third, 29 of 33 studies had external validity threats as they adopted a one-group pretest–posttest design without a control group, so there was no generalization of the significant derived results. To verify the efficacy of online mindfulness-based interventions, more randomized controlled trials should be conducted.
Conclusion
For this scoping review, 33 online mindfulness-based interventions implemented for healthcare professionals were described and explored. Most studies were implemented in the United States during the COVID-19 pandemic. Interventions used in the retrieved studies often utilized previously developed audio-guided online mindfulness-based programs to reduce burnout. Different tactics were used to compensate for the drawbacks of online interventions, such as a high dropout rate. As the evidence for online mindfulness-based interventions is accumulated, further studies are needed to develop and test tailored interventions for healthcare professionals. This review’s results indicated that interventions tailored to the characteristics of each participant’s job yielded positive outcomes. Moreover, the analysis was subdivided based on the outcome dimensions to identify participant characteristics and suggested the development of customized programs. In addition, it is important to prepare an alternative method of interaction between participants to reduce dropouts. There is also a need to compare in-person and online interventions, especially in terms of the dropout rate.
Implications for Occupational Health Practice
This review examined the effect of online mindfulness interventions for healthcare professionals. During the past 3 years, the COVID-19 pandemic has made face-to-face programs difficult. Thus, there was a need to evaluate the effectiveness of online mindfulness interventions. Online mindfulness programs are especially suitable for healthcare professionals because they are accessible and do not have time or location limitations. Moreover, healthcare professionals can readily incorporate any findings into practice. This scoping review discovered that online mindfulness interventions help reduce stress, burnout, anxiety, and depression and improve the emotional well-being of various healthcare professionals. However, research on tailored interventions was inadequate. Therefore, for effective interventions, tailored programs must be persistently developed and evaluated. This will improve the service level of healthcare professionals as well as patient safety in the long run. Finally, among the interventions commonly used in the literature in this review, “Headspace,” a mobile application which provides a guide to practice mindfulness and meditation (Headspace, 2023), stood out for its accessibility, making it a recommended option for implementation.
In Summary
The working environment of healthcare professionals, who come into direct contact with patients, is challenging due to excessive workloads, extended working hours, and infection risks. Mindfulness refers to paying attention to the present moment and accepting the sensations, emotions, and thoughts coming to mind. Online mindfulness-based interventions, unrestricted by time or place, can be a powerful strategy to reduce burnout and improve psychological health for healthcare professionals. Different tactics (e.g., Zoom meetings, emails, and messages) can compensate for the drawbacks of online interventions, such as a high dropout rate. Most online interventions used audio guidance and previously developed programs. Moreover, it would be beneficial to utilize video media and develop tailored interventions considering the uniqueness of healthcare professionals’ job characteristics.
Footnotes
Author Contributions
Chiyoung Cha & Miran Lee
Substantial contributions to the conception or design of the work. The acquisition, analysis, or interpretation of data for the work. Final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.Gumhee Baek & Aram Cho The acquisition, analysis, or interpretation of data for the work. Drafting the work and revising it critically for important intellectual content. Final approval of the version to be published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1A2C2008166).
Ethical Statement
This study, being a scoping review that does not directly involve human subjects, was exempt from the requirement to obtain approval from an institutional review board.