
Abstract
Background:
Firefighters are at increased risk of developing cancer due to occupational exposures, but they may also face increased risk due to their lifestyle, such as the quality of their diet and physical activity. Cancer beliefs and screening behavior could also influence their cancer risk. The current study aimed to identify individual differences associated with lifestyle behaviors, cancer screening, and cancer beliefs among firefighters; to describe the strategies firefighters use to adapt to their work schedule; and to describe topics firefighters believe are the most important to address in their workplace.
Methods:
Career firefighters (N = 171) in a medium-sized U.S. city completed an online survey.
Findings:
Logistic regression analyses identified age, education, racial identity, years of fire service, perceived stress, and rank as predictors of responses to items addressing cancer screening, lifestyle behaviors, and cancer beliefs. Although results varied, age, education, and racial identity were associated with most of the outcomes. Strategies related to sleep such as getting the right amount and napping, exercise, and getting family/roommate support were selected as the top adaptive strategies for work. Sleep, mental health/well-being, and work-life balance were selected most often as the most important topics to address in the fire service, with topics related to reducing occupational exposures receiving less attention.
Conclusions/Application to Practice:
The findings suggest individual differences, such as age, education, and racial identity, should be considered when developing occupational health interventions for firefighters. Interventions related to mental health, work-life balance, and sleep may be desired most by those in the fire service.
Introduction
Firefighters face many health risks. They are exposed to chemicals and toxins that are either known or probable human carcinogens (International Agency for Research on Cancer [IARC], 2022), and have elevated rates of cancer incidence and mortality relative to the general population (Tsai et al., 2015). Night shiftwork has been classified as a “probable carcinogen” by IARC (Barul et al., 2019; Ward et al., 2019). When considering the combined risk of occupational exposures and night shiftwork, IARC recently declared firefighting as a carcinogenic occupation (Demers et al., 2022).
Due to firefighting demands, it may be difficult to maintain a healthy lifestyle that prevents cancer (Dobson et al., 2013). Lifestyle behaviors such as physical activity, diet, and sleep are cancer risk factors (Lugo et al., 2019; Markt et al., 2015; Sillah et al., 2018). Nearly half of firefighters do not meet recommended levels of physical activity, and the prevalence of obesity and hypertension among firefighters is similar to the general population (Barry et al., 2019; Kales et al., 2009). Thus, despite the need to maintain good physical fitness, many firefighters have lifestyles and behaviors that increase cancer risk.
Antecedents to lifestyle behaviors in non-firefighter populations have been explored. Physical activity has been shown to vary by race, with Black individuals being less physically active than White individuals (Hawes et al., 2019). Higher education levels are associated with engagement in healthier lifestyle behaviors, such as not having obesity (A. K. Cohen et al., 2013). Both younger and higher-educated individuals take more daily steps than older and less educated individuals (Bassett et al., 2010). Among employees, higher levels of stress have been found to be associated with an unhealthy diet and cigarette use (Ng & Jeffery, 2003; Okechukwu et al., 2014).
Studies have addressed ways to increase firefighters’ cancer screening rates (Walsh et al., 2014). Although research among the general population has found age, education, race, and income are associated with cancer screening (Cullati et al., 2009; Shokar et al., 2008), there is limited research among firefighters. Cancer beliefs are also possibly linked to lifestyle behaviors (Niederdeppe & Levy, 2007). There has been research examining firefighters’ beliefs about cancer (Anderson et al., 2017); however, there is a lack of research examining individual differences associated with firefighters’ cancer beliefs.
In addition, no studies have explicitly asked firefighters about the strategies they use to adapt to their work schedule or the specific topics they believe are the most important to address in the fire service. By explicitly asking firefighters what strategies they use to adapt to their job demands and what issues they think are most important, researchers, occupational health practitioners, and fire service managers can use this information to develop interventions. The current study had the following aims: (a) determine individual differences associated with lifestyle behaviors, cancer screening, and cancer beliefs among firefighters; (b) describe the strategies firefighters use to adapt to their work schedule; and (c) describe topics firefighters think are the most important to address in their workplace.
Methods
Design
An observational cross-sectional study in which participants completed a self-report survey was conducted. Ethical approval was attained from the Institutional Review Board at Virginia Commonwealth University.
Participants and Data Collection
Firefighters in the Fire and Emergency Services (F&ES) department of a medium-sized U.S. city (population >220,000) completed a survey. During survey instrument development, meetings were held with leaders from the F&ES department and the Firefighter Cancer Support Network (FCSN). The survey instrument was pilot tested on several local firefighters and feedback was incorporated into a final survey using Research Electronic Data Capture (REDCap; P. A. Harris et al., 2009, 2019). During Spring 2022, all firefighters employed by the F&ES department (N = 446) were contacted via email to complete the survey. Study investigators attended local firefighter meetings to advertise the survey. All members of the department were full-time career firefighters with varying work schedules. About half (51%) of the participating firefighters reported working a second job, although no information was collected on the specific type of job. As an incentive, each fire station with at least one participant was entered into a raffle. The winning station received a healthy eating workshop presented by a local professional chef, who visited the winning fire station and used the fire station’s kitchen for the workshop. The workshop was positive, with the hope of additional workshops in the future.
Measures
Independent Variables
Participants were asked to report their racial identity (White; Black; American Indian or Alaska Native; Asian; Native Hawaiian or Other Pacific Islander; Multiple race), gender (female; male; transgender female; transgender male; gender-variant/non-conforming), age, education (less than 8 years to postgraduate), fire service years, and current department rank (i.e., Firefighter, Lieutenant, Captain, or Chief Officer). Due to the relatively small number of battalion chiefs, assistant chiefs, deputy chiefs, and fire chiefs, this group was consolidated into a Chief Officer category, as recommended by the F&ES department and FCSN leaders to ensure anonymity. Participants also completed the Perceived Stress Scale 4 (PSS-4; S. Cohen et al., 1983). Response options ranged from never to very often. Each item was scored on a 0 to 4 scale, with higher scores indicating more perceived stress. The items were summed to create a composite PSS-4 score, with the range of possible scores being 0 to 16. The reliability of the PSS-4 in this sample was acceptable (Cronbach’s α = .76).
Outcomes
Lifestyle behavior questions were obtained from the Health Information National Trends Survey (HINTS; Nelson et al., 2004), which is administered by the National Cancer Institute. When possible, pre-established guidelines were used to categorize firefighter behavior. For physical activity, firefighters were asked the number of days and minutes per day of at least moderate-intensity physical activity (henceforth referred to as physical activity). Firefighters were not asked to distinguish between physical activity during firefighting duties versus non-firefighting physical activity as the purpose was to assess overall physical activity, irrespective of the context. The days and minutes were multiplied together to calculate weekly physical activity minutes. The number of days of muscle-strengthening activities was also assessed. Those who engaged in at least 150 minutes of physical activity and engaged in at least 2 days of muscle-strengthening activities were considered to meet the Department of Health and Human Services’ physical activity guidelines for Americans (Piercy et al., 2018).
Cigarette use was measured by asking “Have you smoked at least 100 cigarettes in your life?” Firefighters who answered No were considered never smokers, while those who answered Yes were considered ever smokers (Bondy et al., 2009). Fruit and vegetable consumption was measured by asking firefighters how many fruit and vegetable servings they had per day. Those who had a combined serving of at least 5 per day were categorized as meeting the fruit and vegetable guidelines (World Health Organization, 2020). Firefighters were asked how many hours of sleep they got per night. Firefighters who responded at least “7 hours” were categorized as getting adequate sleep (Centers for Disease Control and Prevention, 2022). Firefighters were asked to subjectively rate their sleep quality over the past 7 days: very good, fairly good, fairly bad, or very bad. Those who answered at least fairly good were considered to have good sleep quality. Firefighters reported how many days per week on average they drank alcohol. Firefighters who reported drinking 0 days per week were considered to abstain from drinking and those who reported drinking at least 1 day per week were considered drinkers. Body mass index (BMI) was calculated by the author by using the formula: weight (kg)/[height (m)]2. Self-reported height and weight were used in the calculations. Firefighters were classified as having obesity if they had a BMI of 30 or higher and normal/overweight with a BMI less than 30.
Questions related to cancer fatalism and beliefs from HINTS were used. Firefighters were asked: “There are so many different recommendations about preventing cancer, it’s hard to know which ones to follow,” “There’s not much you can do to lower your chances of getting cancer,” and “It seems like everything causes cancer” and responded strongly agree, somewhat agree, neither agree nor disagree, somewhat disagree, or strongly disagree. The three items are sometimes combined to create a cancer fatalism composite score (Chung & Lee, 2019). However, the Cronbach’s alpha of the three items was low (α = .52), similar to Sinky et al. (2018). Thus, the three items were examined individually. In order to code for firefighters who agreed with the statement compared with those with did not, firefighters who responded at least somewhat agree were coded as agreeing with the statement, while those who disagreed or were neutral were coded as expressing indifference/disagreeing with the statement. Recommended by the FE&S department and FCSN leaders, firefighters were also asked if they had undergone screening for breast, colorectal, prostate, and skin cancer.
Firefighters were asked to rate the top five strategies they used to adapt to their fire service work, and also five important topics needing to be addressed. In order to develop lists of adaptive strategies and topics, the research team held meetings with the leaders from the F&ES department and the FCSN who provided input regarding adaptive strategies used and topics to add to the survey. Adaptive strategies included sleep and sedation, alcohol, tobacco, stimulants/caffeine, diet, exercise, family/friends or supervisor support (e.g., selecting my schedule, getting days off), and other. Important topics included physical activity and muscle-strengthening exercises (excluding cardio exercises), diet, sleep, smoking/alcohol/substance use, work-life balance, mental health/well-being, financial management, infectious agents, hazardous materials/toxins produced, aqueous film-forming foams or other flame suppressants, policy for post-fire on scene decontamination, PPE cleaning/decontamination, and other. All items are listed in Tables 4 and 5.
Analysis Strategy
Descriptive statistics were first calculated. Race was categorized into two groups: White (reference category) and Black or Other race. Education was categorized into two groups: do not have college degree (reference category) and have college degree. Firefighter rank was categorized into two groups in order to compare those with administrative responsibilities versus those without administrative responsibilities: Firefighter (reference category) and Lieutenant or higher. Due to the small number of female firefighters (10), gender was not included as an independent variable. The results did not differ if female firefighters were removed and were retained for the final analyses given the percentages (5%) in the current study are representative of the U.S. population of female firefighters (U.S. Fire Administration, 2023).
Individual logistic regression models were conducted for the following outcome variables: met physical activity and muscle-strengthening guidelines, adequate sleep, good sleep quality, met fruit/vegetable guidelines, having normal/overweight BMI status, never smoker, abstain from drinking, agreement with the statements “everything causes cancer,” “not much can be done to lower cancer risk,” “it is hard to know which cancer preventive recommendations to follow,” and screened for colorectal cancer, skin cancer, and prostate cancer. Breast cancer screening was not included as an outcome as all female firefighters had reported being screened. Lifestyle behaviors were coded so that 1 was the healthy behavior, while 0 was the health-risk behavior for consistency across the models. For the cancer beliefs, agreeing with the statement was coded as 1, while not agreeing was coded as 0. For cancer screening, getting screened was coded as 1, while not getting screened was coded as 0. The following independent variables were included in each regression model: age, years of fire service, race, education, rank, and perceived stress. Age, years of service, and perceived stress were included as continuous variables. Age, years of service, and rank were correlated with each other (r’s ranging from .28 to .77). However, the variance inflation values for each independent variable were less than 5, lower than the standard cutoff of 5 or 10 used for characterizing potential multicollinearity (i.e., correlation between multiple independent variables in the regression model). Thus, all variables were retained for the analyses. Listwise deletion was used for all regression models.
Only firefighters aged 40 and older were included for the colorectal cancer screening analysis and male firefighters aged 40 and older were included for the prostate cancer screening analyses to match the recommendations of the International Association of Fire Chiefs (IAFC) (Sparer & Health Communication Core, 2022). Only Yes or No responses were considered for the cancer screening analyses. For the ranking of adaptative workplace strategies and the most important topics to address in the fire service, respective tables were created to show how many times a strategy or topic was ranked. All analyses were conducted using R (version 4.3.1), which is a free software environment for statistical analyses (R: The R Project for Statistical Computing, 2024).
Results
Descriptive Statistics
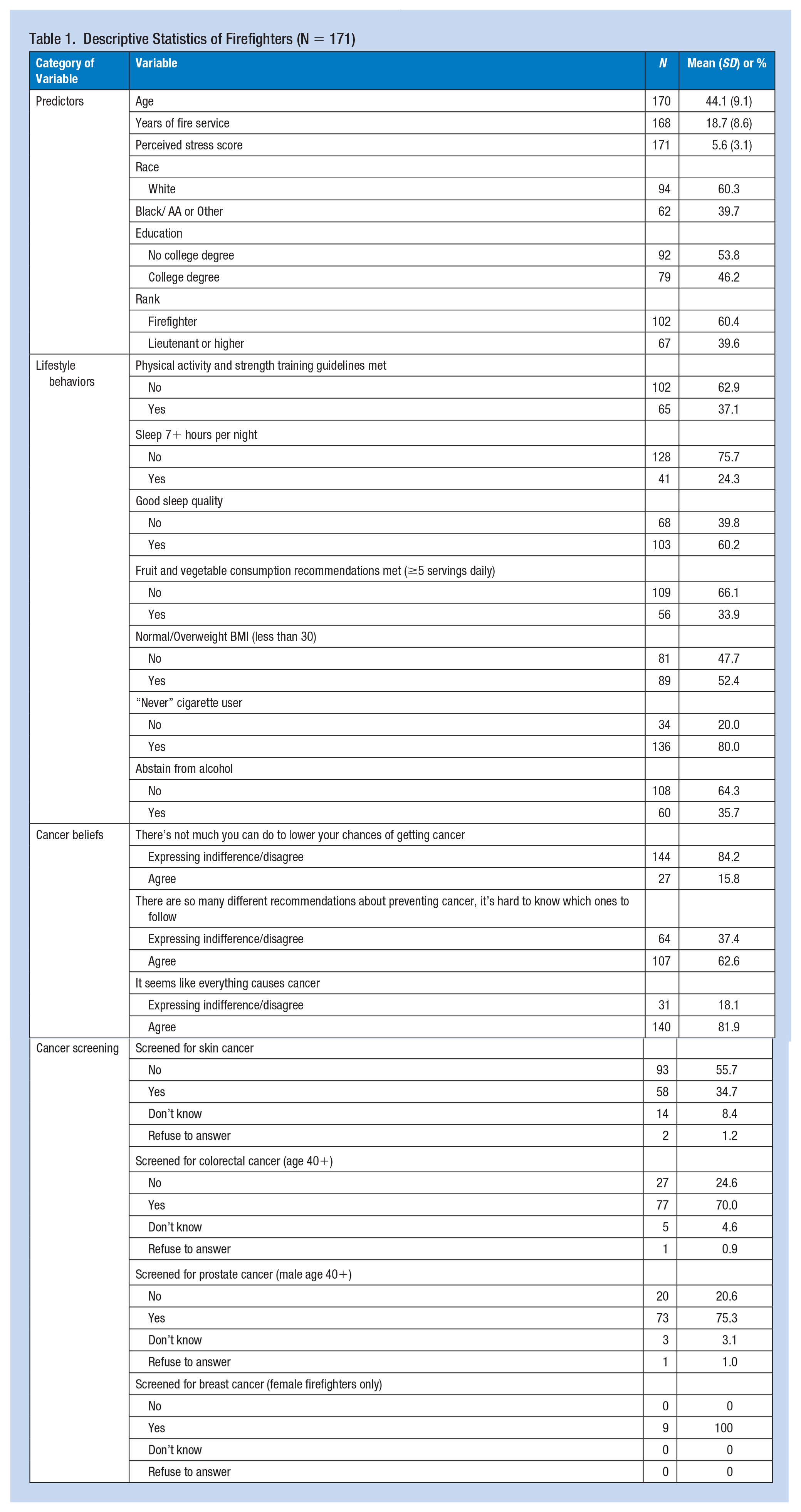
A total of 171 firefighters completed the survey (38% response rate). Table 1 includes descriptive statistics, including the percentage of those who met the lifestyle behavior recommendations, who agreed with the cancer belief statements, and had been screened for the different cancer types. The average age of participants and duration of firefighter service was 44.1 and 18.7 years, respectively. The average PSS-4 score was 5.6. The majority of firefighters reported their race as White (60%). Approximately half of the firefighters had a college degree (46%). A majority (60%) held a rank of Firefighter. When considering the lifestyle behaviors of the firefighters, 37% met the physical activity and strength training guidelines, 24% slept at least 7 hours per night, 60% reported at least good sleep quality, 34% reported eating at least 5 servings of fruit and vegetables, 52% had normal/overweight BMI, 80% were “never” cigarette users, and 36% abstained from alcohol.
Descriptive Statistics of Firefighters (N = 171)
Logistic Regression Results
Table 2 includes the logistic regression results for the lifestyle behaviors. Firefighters who reported their race as Black or Other were less likely to get adequate sleep (OR = 0.30, 95% confidence interval [CI] = [0.10, 0.84], p = .028), while firefighters with a college degree were more likely to get adequate sleep (OR = 3.51, 95% CI = [1.42, 9.34], p = .008). Firefighters who reported more perceived stress were less likely to report good sleep quality (OR = 0.81, 95% CI = [0.71, 0.91], p < .001). Firefighters who reported their race as Black or Other were less likely to have normal/overweight BMI (OR = 0.42, 95% CI = [0.19, 0.90], p = .029). Firefighters who reported their race as Black or Other and firefighters who were ranked Lieutenant or higher were more likely to be never smokers: OR = 4.76, 95% CI = [1.53, 18.68], p = .013 and OR = 3.31, 95% CI = [1.11, 11.51], p = .042, respectively. No individual differences were associated with physical activity, diet, and alcohol consumption.
Logistic Regression Models: Lifestyle Behaviors
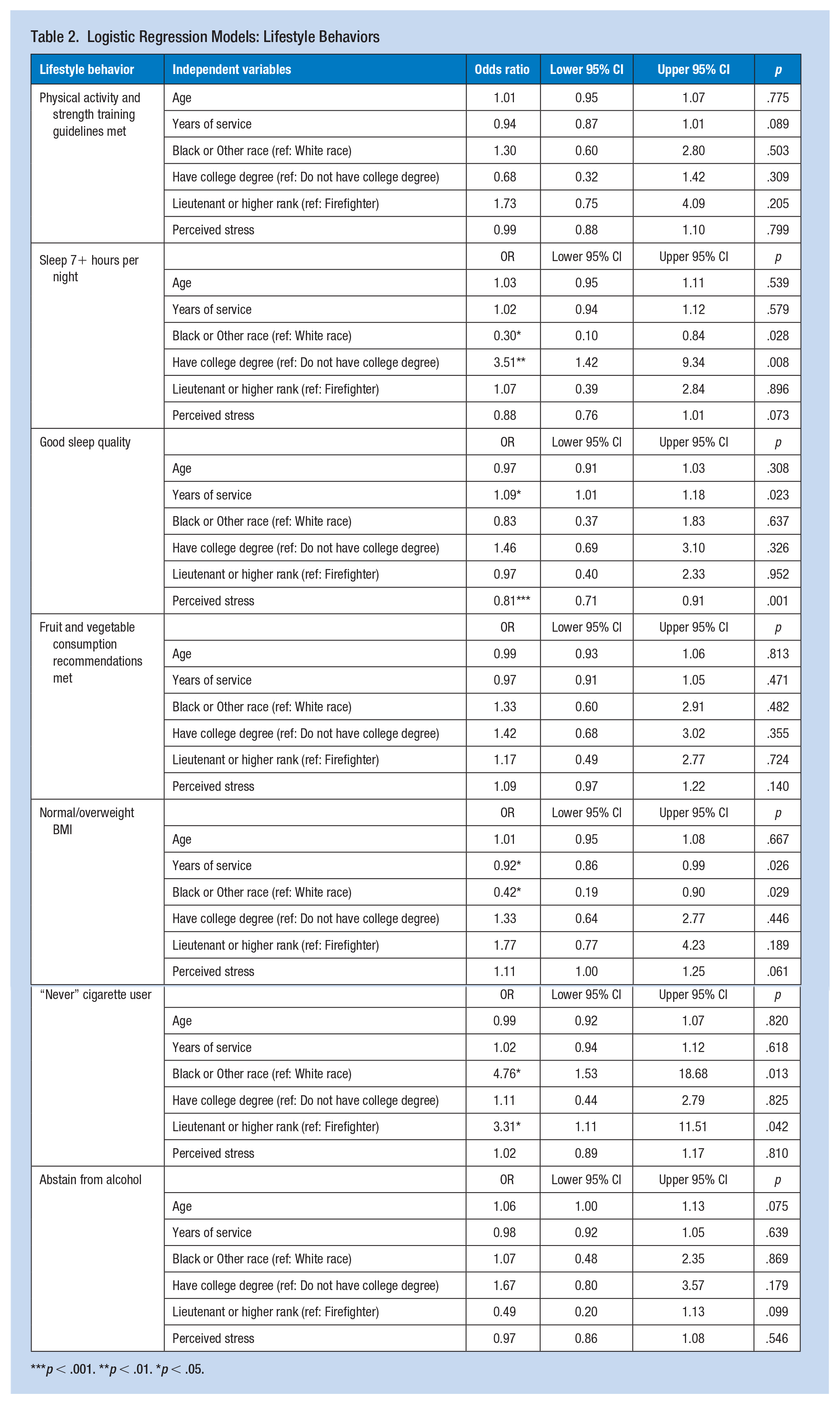
p < .001. **p < .01. *p < .05.
Table 3 includes the logistic regression results for the cancer and screening. Firefighters who reported their race as Black or Other and firefighters with a college degree were less likely to agree that it seems like everything causes cancer: OR = 0.23, 95% CI = [0.08, 0.61], p = .004 and OR = 0.29, 95% CI = [0.10, 0.74], p = .013, respectively. However, firefighters who were ranked Lieutenant or higher were more likely to agree that it seems like everything causes cancer: OR = 3.20, 95% CI = [1.07, 10.72], p = .046. Firefighters who reported their race as Black or Other and firefighters with a college degree were less likely to agree there’s not much you can do to lower your chances of getting cancer: OR = 0.12, 95% CI = [0.02, 0.49], p = .009 and OR = 0.30, 95% CI = [0.09, 0.92], p = .045, respectively. No individual differences were associated with agreeing that “there are so many recommendations about preventing cancer, it’s hard to know which ones to follow.” Screening for skin cancer increased with increasing age (OR = 1.11, 95% CI = [1.03, 1.20], p = .008), while firefighters who reported their race as Black or Other were less likely to be screened for skin cancer (OR = 0.15, 95% CI = [0.15, 0.39], p < .001). Screening for colorectal cancer increased with increasing age (OR = 1.46, 95% CI = [1.23, 1.84], p < .001), while firefighters with a college degree were less likely to ever to be screened for colorectal cancer (OR = 0.13, 95% CI = [0.02, 0.51], p = .007). Firefighters who reported more perceived stress were less likely to be screened for prostate cancer (OR = 0.75, 95% CI = [0.58, 0.94], p = .017).
Logistic Regression Models: Cancer Beliefs and Cancer Screening
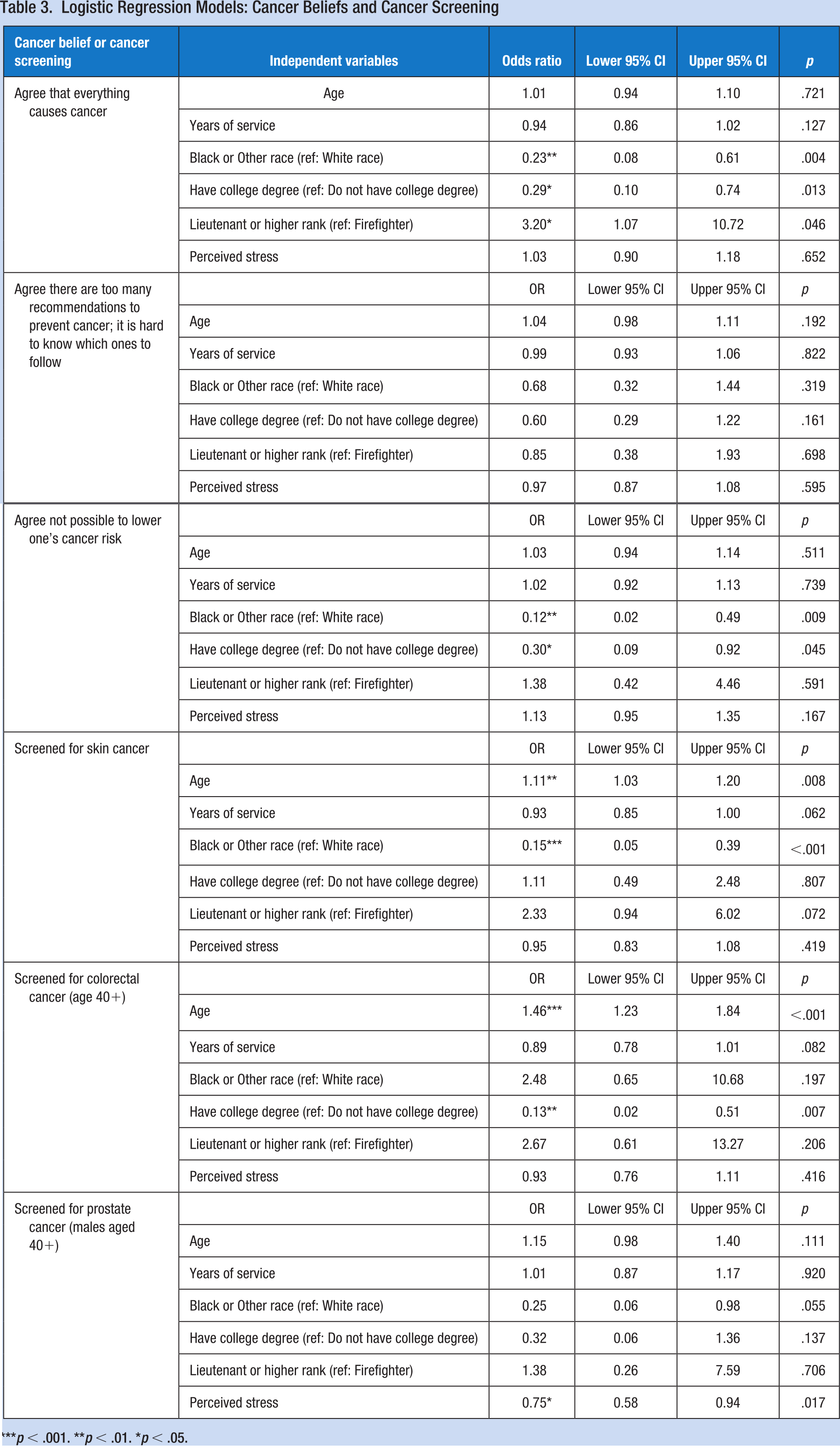
p < .001. **p < .01. *p < .05.
Ranking of the Adaptive Strategies and Topics of Importance
Table 4 includes the number of times an adaptive strategy was ranked by the firefighters. Sleep (getting the right amount) received the most first-place votes (66) and was ranked in the top 5 of 123 participants, which was the first overall highest-ranked strategy by total number of votes. Sleep environment received the second most overall votes (101) and Napping and Exercise both received 93 votes. Conversely, Use of alcohol (24), Use of tobacco products or other forms of nicotine (9), and Other (4) received the lowest overall votes.
Number of Times a Strategy Was Ranked as the Top First, Second, Third, Fourth, and Fifth Strategy Firefighters Used to Adapt to Their Work Schedule
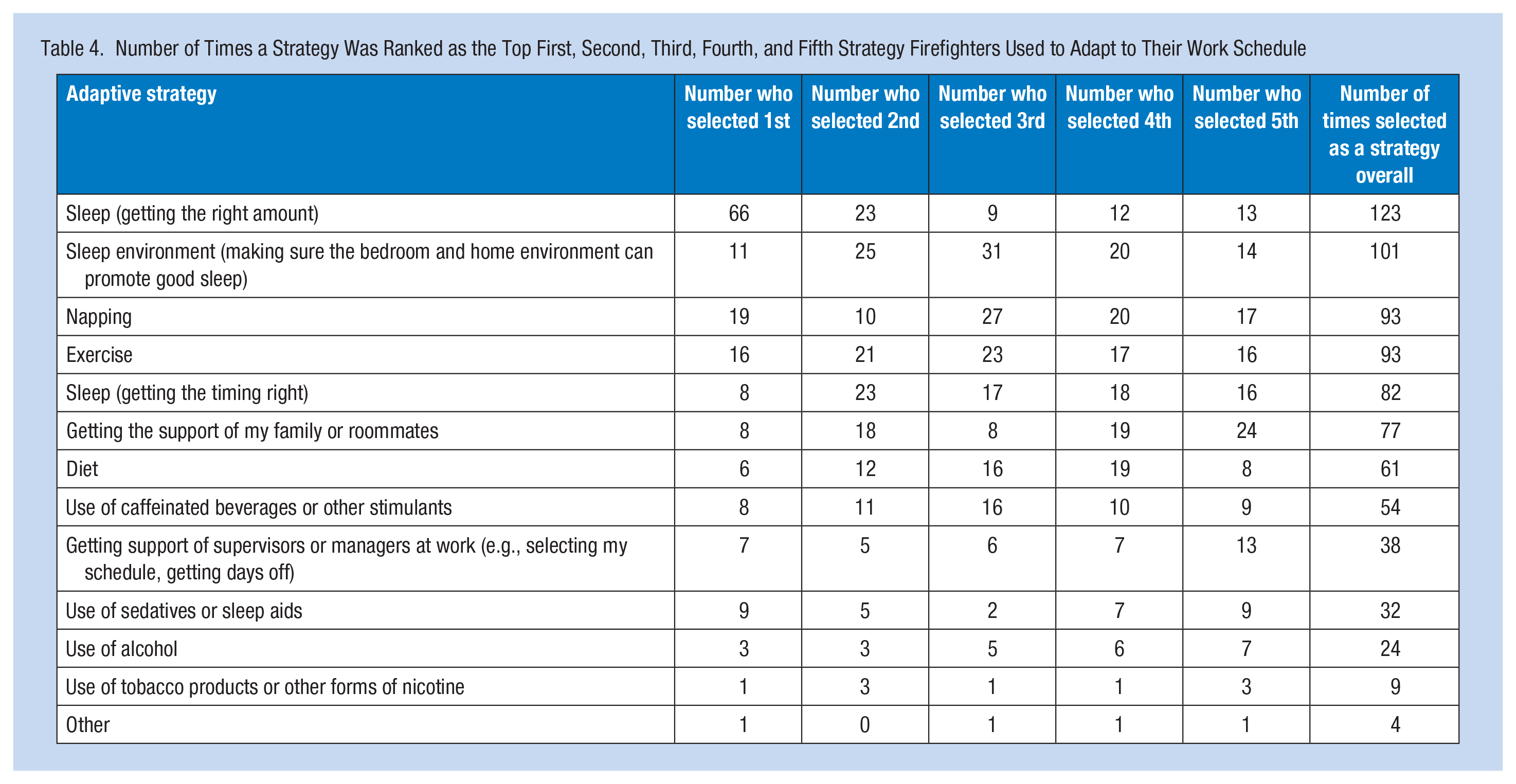
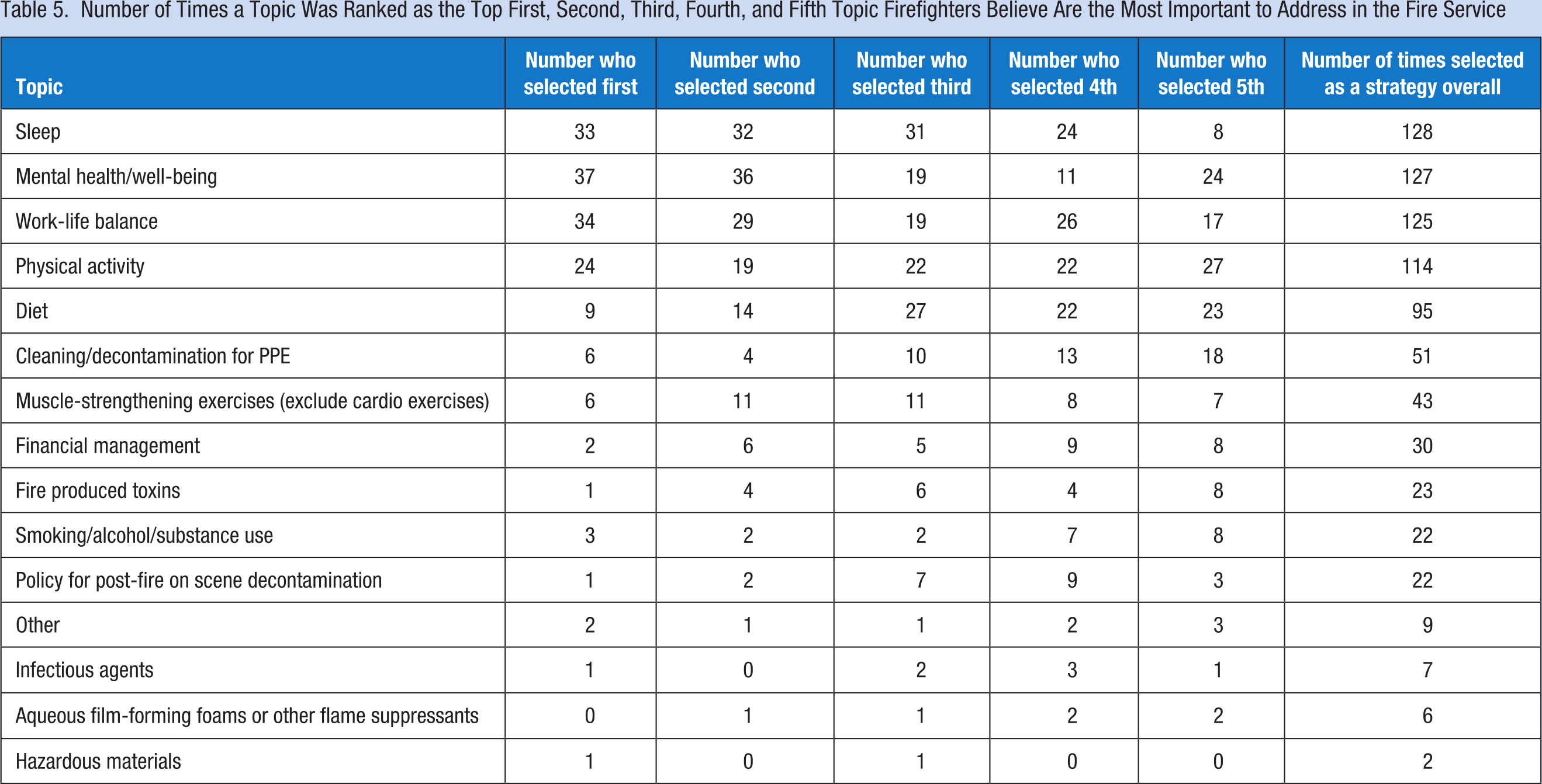
Table 5 includes the number of times a topic was ranked by the firefighters. Mental health/well-being received the most first place votes (37) and was ranked in the top 5 of 127 participants, which was the second overall highest-ranked topic by total number of votes. Sleep received the most overall votes (128), Work-life balance received the third most (125), Physical activity received the fourth most (114), and diet received the fifth most (95). Conversely, Infectious agents (7), Aqueous film-forming foams or other flame suppressants (6), and Hazardous materials (2) received the lowest overall votes.
Number of Times a Topic Was Ranked as the Top First, Second, Third, Fourth, and Fifth Topic Firefighters Believe Are the Most Important to Address in the Fire Service
Discussion
Summary of the Findings
In this study, the associations between individual differences and lifestyle behaviors, cancer screening, and cancer beliefs were examined among firefighters. Consistent with other firefighter studies (Savall et al., 2021), only a quarter of participants in the current study reported adequate hours of sleep per night. After further investigation, while 60% of firefighters were in the at least fairly good sleep quality group, only six of these firefighters reported their sleep was very good. This corroborates prior findings of poor sleep health among those in the fire service (Carey, Al-Zaiti, Dean, et al., 2011).
Although more firefighters (37%) met guidelines for both physical activity and muscle-strengthening than U.S. adults (24%) (Elgaddal et al., 2022), it is still concerning since firefighting requires high levels of physical fitness. Others have found physical inactivity to be common among firefighters (Barry et al., 2020; Bugajska et al., 2007). Almost half (49%) of the firefighters in the study had obesity. High rates of obesity are common in fire departments along with hypertension and other chronic disease risk factors (Kaipust et al., 2019; Smith et al., 2012). Interestingly, firefighters reported eating more fruits and vegetables than participants in other studies. However, there have been recent efforts to improve the nutrition of firefighters through educational materials and interventions (Carey, Al-Zaiti, Liao, et al., 2011; Donahue et al., 2022), which could possibly explain the increased consumption of fruits and vegetables. One out of five (20%) firefighters were ever cigarette users, which is lower than the estimated U.S. adult population of 33% from the HINTS 6 survey conducted in 2022 (Health Information National Trends Survey [HINTS], 2023b). This corroborates with U.S. national reports of lower rates of cigarette use among firefighters compared with the general adult U.S. population (Jitnarin et al., 2015). In addition, 36% of firefighters reported not drinking at all during the week, which is less than the estimated 49% of U.S. adult population from HINTS 6 (HINTS, 2023a). Other studies of U.S. firefighters have found high rates of alcohol consumption, with moderate/heavy and binge drinking common one among firefighters (Angleman et al., 2022; Carey, Al-Zaiti, Dean, et al., 2011; Choi et al., 2017).
Prior research has found demographic variables to be associated with lifestyle behaviors (Mathur Gaiha et al., 2021; Rai et al., 2019). In our study, firefighters who reported their race as Black or Other were less likely to get adequate sleep, while those with a college degree were more likely to get adequate sleep. These findings align with prior research finding Black adults and adults with lower levels of education in the United States reporting shorter sleep durations (Cunningham et al., 2015; Jackson et al., 2013). Firefighters with more years of service were more likely to report good sleep quality, while firefighters who reported higher levels of perceived stress were less likely to report good sleep quality. In contrast, Mehrdad et al. (2013) examined the association between years of service and sleep quality among firefighters in Iran and found firefighters with more years of service were less likely to report good sleep quality. Similar to the current study, other studies of firefighters have found higher stress to be associated with poorer sleep quality (Abbasi et al., 2018; Yook, 2019).
Firefighters with more years of service and firefighters who reported their race as Black or Other were less likely to have a normal/overweight BMI. In general, non-White adults have been found to have higher percentages of obesity when compared with White adults (Petersen et al., 2019). Regardless of age, firefighters with more years of experience compared with those with fewer years may be more sedentary and have poorer diets because of the firehouse’s kitchen culture that may promote unhealthy eating (Anderson et al., 2017). Firefighters who reported their race as Black or Other and firefighters ranked as Lieutenant or higher were more likely to be never smokers. While Poston et al. (2014) did not find any racial differences in cigarette use, they found White firefighters were more likely to use smokeless tobacco. It is unclear why those ranked Lieutenant or higher were more likely to be never smokers. No differences emerged for meeting the physical activity and muscle-strengthening guidelines, fruit and vegetable recommendations, and alcohol consumption, indicating individual differences may be less important for these outcomes.
There were also several differences when assessing cancer screening and beliefs. Black or Other race firefighters and those with a college degree were less likely to agree that “there’s not much you can do to lower your chances of getting cancer” and that “it seems like everything causes cancer.” These findings are similar to an analysis of HINTS, in which Black and more educated Americans were less likely to endorse cancer fatalistic beliefs (Niederdeppe & Levy, 2007). However, firefighters ranked Lieutenant or higher were more likely to agree that “it seems like everything causes cancer.” It is unclear why higher-ranked firefighters would agree with the statement. It is possible higher ranked firefighters with administrative responsibilities are involved with handling work-related cancer claims and this could lead to higher fatalism among higher-ranked firefighters; however, further research will be needed to better understand the association. Skin cancer screening increased as the age of the firefighters increased, while firefighters who reported their race as Black or Other were less likely to be screened, similar to prior studies (Rodriguez et al., 2007). Colorectal cancer screening increased as the age of the firefighters increased, while those with a college degree were less likely to be screened. While the findings on age corroborate with findings among the general population, the finding that those with a college degree were less likely to be screened does not align with prior research (Cullati et al., 2009). In addition, firefighters who reported higher levels of perceived stress were less likely to be screened for prostate cancer, similar to a finding that higher levels of perceived stress were associated with lower odds of regularly getting screened for cancer (Hajek et al., 2017). Hajek et al. argue that higher levels of stress are associated with engagement in less health-promotion behaviors, which could explain why higher stress is associated with being less likely to get screened for cancer.
When asked to rank the top strategies they use to adapt to their work schedule, four of the five top strategies firefighters selected were sleep-related. Health-risk behaviors, such as the use of alcohol and tobacco products, were rarely used. Although most of the firefighters in the current study had relatively poor sleep health, most firefighters appear to use sleep to adapt to their work schedule, rather than engage in health-risk behaviors. Finally, firefighters ranked the topics they think are the most important to address in the fire service. Firefighters see lifestyle behaviors as important workplace issues to address with mental health and work-life balance as the most important followed by sleep, physical activity, and diet. Surprisingly, topics related to decontamination and exposure to hazardous materials received much less attention. While speculative, one possible explanation for why certain workplace policy topics received less first place votes is that there has been a very strong focus on reducing occupational exposures in the fire service over the years, from both IARC and fire service professional organizations. Although continued efforts to reduce firefighters’ occupational exposures are needed, firefighters are also increasingly aware that their lifestyle choices are modifiable factors that can alter cancer risk (Jitnarin et al., 2020). Firefighters may see their occupational exposures as “part of the job” and harder to control when compared with their lifestyle behavior engagement. However, additional research is needed in this area as other possible explanations, such as the firefighter culture, access to laundry facilities, and access to spare gear, could also explain the ranking.
Strengths, Limitations, and Future Directions
There are several strengths of the current study. Most firefighter research has focused on one or two lifestyle behaviors. This study included a wider range of lifestyle behaviors. Cancer beliefs and screening were also considered as outcomes. These variables have not been studied frequently among firefighters. In addition, key firefighter stakeholders aided in the development of the survey questions. However, limitations include the self-report nature of the lifestyle behaviors, which are subject to overestimation or underestimation (M. C. Harris, 2017). There are limitations in using BMI to assess obesity as it does not distinguish excess unhealthy weight from high lean mass, which may limit the interpretability of the current findings, as firefighters may have high muscle mass that contributed to higher BMI. Even though questions were mostly derived from HINTS, the use of single-item measures did not allow for exploration of the constructs in more detail, such as whether the firefighter was a binge or heavy alcohol drinker. The cancer screening questions only asked participants if they had ever been screened but did not ask specifically what type and the timing of the screening; so it was not possible to assess if firefighters were up to date in their cancer screening.
Although we were able to include female firefighters in our study, which are not always included in firefighter research, we were not able to assess differences between female and male firefighters due to the small sample of female firefighters. The response rate (38%) was lower than anticipated, but anecdotally, conversations with stakeholders indicated there were high levels of stress due to the increase in overtime shifts and the COVID-19 pandemic, which may have influenced the response rate. We did not assess interruptions in sleep during work shifts, which may be associated with sleep quality and overall hours of sleep. Also, the findings may only be generalizable to career and not volunteer firefighters.
There are several implications and future directions. Sleep is an important issue when discussing firefighter health given its association with cancer (Song et al., 2021). The findings suggest that most firefighters are not getting enough sleep, but believe it is important, and that represents an important intervention target. In general, evidence from the current study suggests that firefighters see lifestyle behaviors as important workplace issues to address. While topics related to occupational exposures are important, firefighters may believe that addressing topics related to their lifestyle behavior is more important and controllable. Mental health/well-being and work-life balance were also ranked highly. This is notable as suicide in the fire service is a public health concern (Healy & Vujanovic, 2021), along with high levels of depression, posttraumatic stress disorder, anxiety, and alcohol use (Carey, Al-Zaiti, Dean, et al., 2011; Haddock et al., 2017). Future research may wish to explore ways to improve the mental health and work-life balance of firefighters.
Implications for Occupational Health Practice
Individual differences, such as age, education, and race, were shown to be associated with lifestyle behaviors, cancer screening, and cancer beliefs. Firefighters ranked sleep and other lifestyle behaviors, mental health, and work-life balance as the most important topics to address in the fire service and as strategies they use to adapt to their work schedule. Occupational health professionals can work with fire service leadership to develop tailored interventions that consider not only firefighters’ individual differences but also the healthy strategies firefighters currently use to adapt to their work schedule and the topics firefighters believe are the most important to address. By considering what firefighters desire most, this could increase intervention effectiveness.
Applying Research to Occupational Health Practice
Firefighters are at increased risk of cancer due to occupational exposures. Having a better understanding of firefighters’ lifestyle behaviors, cancer beliefs, and cancer screening is important for the development of occupational health interventions. Additionally, assessing what firefighters think are the most important topics to address in their workplace and the current behaviors they engage in to adapt to their work schedule could better inform future interventions. Findings showed age, education, and racial identity were associated with most of the lifestyle behaviors, cancer beliefs, and cancer screening behaviors. Strategies related to sleep, such as getting the right amount and napping, exercise, and getting family/roommate support were selected as the top adaptive strategies for work. Sleep, mental health/well-being, and work-life balance were selected most often as the most important topics to address in the fire service, with topics related to reducing occupational exposures receiving less attention.
Footnotes
Acknowledgements
We would like to thank the Richmond Fire and Emergency Services Department and Virginia Chapter of the Firefighter Cancer Support Network for their help with developing the survey and helping recruit participants. We would also like to acknowledge that Virginia Commonwealth University REDCap is supported by the C. Kenneth and Dianne Wright Center for Clinical and Translational Research grant support (UL1TR002649).
Authors’ Contributions
TEG, BFF, and JBB conceived the study, developed the survey, and recruited participants. All authors contributed to the analysis of the data and interpretation of the results. TEG took the lead in writing the manuscript. All authors provided critical feedback and contributed to the final manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a Virginia Commonwealth University Massey Cancer Prevention and Control (CPC) Research Accelerator Monies (RAMs) Award (PI: JBB). This work was supported in part by a K12 National Institute of General Medical Sciences award (2K12GM093857) to TEG.
Ethical Considerations and Disclosures
This study was approved by the Institutional Review Board of Virginia Commonwealth University (HM20022904).