
Abstract
Background:
Workers’ reporting of work-related injuries or illnesses is important for treatment and prevention, yet research often focuses on reporting barriers. This study aimed to identify factors related to work-related musculoskeletal disorder (WRMSD) reporting attitudes and their connection to reporting intention and behavior.
Methods:
We analyzed data from 377 direct care workers employed in 19 long-term care facilities in South Korea. A self-administered questionnaire collected demographics, job characteristics, physical and psychosocial factors, musculoskeletal symptoms, reporting attitudes, and WRMSD reporting intentions and behavior between May and August 2022. We used a generalized linear mixed model with a random intercept by employers to identify factors influencing reporting attitudes. To explore the relationship between reporting attitude and reporting intention and behavior, simple logistic regression was also conducted.
Results:
We achieved an 86% response rate. The majority of the study participants were female (87.2%), married (95.9%), and non-immigrant (72.8%). Of the study participants, 48.9% had no intention to report WRMSDs, and 44.3% held negative reporting attitudes. Among 200 workers with WRMSDs, 86.5% did not report them. Attitudes were associated with work duration, safety training, management safety priority, WRMSD experience, and symptom severity and frequency. Management safety priority did not moderate this relationship. Significant links existed between attitudes and reporting intention and behavior.
Conclusions/Applications to Practice:
This study highlights the vital influence of workers' attitudes on reporting work-related injuries and illnesses. Occupational health providers should employ strategies, such as tailored safety training and management commitment, with a focus on addressing the unique needs of long-tenured and musculoskeletal-exposed workers. Fostering a safety culture that promotes open and timely reporting is crucial, and implementing these strategies can significantly enhance workplace safety and health.
Introduction
The International Labour Organization estimates that approximately 350 million occupational accidents occur annually, resulting in high mortality rates (International Labour Organization, 2015). However, researchers have pointed out that the true extent of occupational health issues remains concealed due to the significant underreporting of occupational injuries and illnesses (Kyung et al., 2023). According to the Occupational Safety and Health Administration (OSHA) in the United States, it is mandatory for workers to promptly report all workplace incidents, hazardous conditions, and near misses to their management (Occupational Safety and Health Administration [OSHA], 2022). In an effort to encourage worker injury reporting, OSHA also safeguards workers’ rights to report injuries without fear of retaliation, and it prohibits employers from taking any adverse actions against workers who report incidents (OSHA, 2016). Despite these measures, many workers still encounter obstacles when attempting to report work-related problems to their management (Kyung et al., 2023). A recent review study revealed that U.S. workers, ranging from 20% to 74% across various job types, chose not to report their work-related injuries or illnesses to their management (Kyung et al., 2023).
According to behavioral theories such as the Theory of Planned Behavior, personal attitudes play a pivotal role in shaping behavioral intentions and behaviors (Ajzen & Fishbein, 1977; Gavaza et al., 2011; Jiang et al., 2018; Pfeiffer et al., 2010). In a study involving U.S. transportation workers, Jiang et al. (2018) observed that instances of underreporting workplace aggression and near-miss events were more prevalent among workers with unfavorable attitudes toward safety-related reporting (Jiang et al., 2018). Attitudes are believed to be malleable and subject to change based on individual experiences and work environments (Petty & Cacioppo, 1986). However, there is a dearth of research investigating factors that influence attitudes toward reporting work-related injuries or illnesses.
Direct care workers face an elevated risk of work-related musculoskeletal disorders (WRMSDs), but a significant number of these injuries go unreported (Caponecchia et al., 2020). Siddharthan et al. (2006) noted that nursing personnel often tolerated WRMSDs, regarding them as a natural part of their job, unless these issues interfered with their work activities, ultimately leading to the underreporting of WRMSDs (Siddharthan et al., 2006). Recognizing the crucial role of reporting attitudes in injury reporting, gaining a comprehensive understanding of these attitudes can offer valuable insight for further development of effective interventions aimed at motivating workers to report such incidents. However, existing research has primarily focused on identifying barriers to reporting occupational injuries or illnesses. This study aimed to (1) describe WRMSD reporting attitudes among direct care workers in long-term care facilities, (2) identify factors associated with WRMSD reporting attitudes, and (3) investigate the relationship between WRMSD reporting attitudes and reporting intentions and reporting behavior.
Methods
This study employed a cross-sectional design, utilizing a convenience sample comprised of 377 direct care workers from 19 long-term care facilities in South Korea. These facilities represented 5.4% of all long-term care facilities located in Gyeonggi-do, the most populous province in Korea (Ministry of Health and Welfare, 2022). In South Korea, long-term care facilities are categorized as either long-term care hospitals or nursing homes. Long-term care hospitals provide in-patient services, and extended care for individuals requiring longer rehabilitation stays. They are obligated to staff healthcare professionals such as medical providers and nurses (H. Kim et al., 2015). On the other hand, nursing homes primarily offer social services to individuals aged 65 or older who cannot live independently but do not generally need the level of medical care provided in long-term care hospitals (H. Kim et al., 2015). For the purposes of this study, direct care workers were defined as trained staff responsible for delivering direct patient care, such as feeding, bathing, dressing, and toileting (J.-Y. Kim & Tak, 2018). Eligibility criteria included that direct care workers had been employed in their current positions for a minimum of 3 months and were able to read, write, and understand Korean. The initial 3 months of employment were considered a probationary period during which workers acclimated to their new roles and assessed whether the job was a suitable fit (Borofsky et al., 1995).
Recruitment and Data Collection
A flyer containing contact information was posted on the bulletin boards of the respective department in all 19 long-term care facilities after obtaining the necessary permissions. Data collection occurred between May and August 2022, utilizing a self-administered questionnaire that had been pilot-tested with 20 direct care workers in a long-term care hospital. The study’s questionnaire was distributed and collected during each institution’s monthly staff meetings or training programs, which were provided by the National Health Insurance Service. Informed consent was obtained from all participants, and a token of appreciation in the form of $10 (12,000 won) was provided to each participant upon completion of the survey. A total of 403 direct care workers participated in the survey, resulting in a response rate of 86% (ranging from 70% to 81% in three long-term care hospitals and from 86% to 95% in 16 nursing homes). After excluding 11 direct care workers who had been employed for less than 3 months and 13 direct care workers who had not responded to 5% or more of the questionnaire items, the final sample included 377 direct care workers. Ethical approval for the study was granted by the Committee on Human Research of the University of California, San Francisco, and the Public Institutional Review Board in South Korea.
Study Variables and Instruments
Demographic and Job Characteristics
Demographic characteristics encompassed age, sex (male or female), immigration status (immigrant or non-immigrant), marital status (married or single), and education (elementary school, middle school graduate, high school graduate, and college 1 year or more). Job characteristics included the type of long-term care facility (long-term care hospital or nursing home), duration of employment as a direct care worker, and work arrangement (permanent, temporary, or independent).
Physical Work Factors
Physical work factors comprised physical exertion and the number of assigned patients. For physical exertion, respondents were asked to rate the physical demands of their current job on a scale from one (“not strenuous”) to five (“extremely strenuous”) (Neupane et al., 2020).
Psychosocial and Organizational Factors
Psychosocial and organizational factors were assessed using job stress and management safety priority. Job stress was evaluated using the Korean version of the Effort-Reward Imbalance (ERI) Questionnaire, which included effort (six items), reward (10 items), and overcommitment (six items) (Eum et al., 2007; Siegrist, 1996). Effort reflects the job demands or obligations placed on workers and reward refers to something that workers can acquire from their work such as monetary compensation, esteem, career opportunities, and job security (Van Vegchel et al., 2005). Overcommitment defines a set of attitudes, behaviors, and emotions reflecting excessive striving for approval and appreciation (Hasselhorn et al., 2004). In the ERI model, a lack of reciprocity between efforts spent and rewards received at work arouse emotional distress and subsequent adverse health outcomes (Siegrist, 1996). All items in these scales used a four-point Likert-type scale ranging from one (“strongly disagree”) to four ( “strongly agree”), with higher values indicating higher effort, reward, or overcommitment. The effort, reward, and overcommitment scores were calculated as the sum of item responses: the ERI ratio was obtained by dividing effort by reward, with a correction factor of 3/5 applied to adjust for the unequal number of items in the effort and reward scales (Siegrist et al., 2004). For management safety priority, respondents were asked to indicate whether the health and safety of workers were considered a high priority by the management in their workplace, with response options of “yes” or “no” (Kines et al., 2011). In regard to safety training for injury reporting, respondents were also asked to indicate if they had ever received training regarding the reporting of workplace injuries or illnesses from their organization.
Musculoskeletal Symptoms
The assessment of musculoskeletal symptoms encompassed various aspects, including the experience of WRMSDs, the frequency of musculoskeletal symptoms, and the severity of pain. These aspects were evaluated using a modified questionnaire originally employed and validated in the Nurses’ Work Life and Health Study (J. A. Lipscomb et al., 2002). This modified questionnaire, featuring a single item for each question, adhered to the definition of musculoskeletal symptoms as outlined in the Nordic Musculoskeletal Questionnaire, which includes pain, aching, stiffness, burning, numbness, or tingling in various body regions. To collect relevant data, respondents were queried about their encounters with musculoskeletal pain or discomfort in the neck, shoulder, back, upper extremities, or lower extremities, within the past 12 months. They were also asked to indicate whether this pain or discomfort was either aggravated or caused by their work. Subsequently, participants who reported experiencing symptoms within the prior 12 months were presented additional inquiries regarding frequency and severity of these symptoms. To assess the frequency of musculoskeletal symptoms, a six-point Likert-type scale ranging from one (“never”) to six (“daily”) was employed. The severity of pain was evaluated using a five-point Likert-type scale, ranging from one (“none”) to five (“extreme”).
Reporting Attitudes
Reporting attitudes were gauged using a modified version of a four-item questionnaire developed and validated by Probst and Graso (2013) with a Cronbach’s alpha of 0.76 (Probst & Graso, 2013). The original questionnaire was adapted for direct care workers in long-term care facilities by changing “accidents and injuries” to “work-related injuries or illnesses.” The modified English version of the questionnaire was translated and back-translated into the Korean language by two independent bilingual people and the Korean version of questionnaire was finalized through consultation with a third bilingual person. Respondents were asked to indicate their injury reporting attitudes as follows: “Work-related injury or illness investigations are mainly used to assign blame,” “Nothing gets fixed, so why bother reporting an injury or illness,” “Reporting a work-related injury or illness hurts my chances for job-related rewards,” and “Injury or illness is a normal part of my job. They can’t all be prevented.” Participants used a 7-point Likert-type scale, ranging from one (“strongly disagree”) to seven (“strongly agree”), with higher scores indicating more positive attitudes toward reporting. Reporting attitudes scores were calculated as the mean of item responses. Reporting attitudes were also dichotomized into two groups using a cutoff at the median score of four. The Korean version of the questionnaire used in this study had a Cronbach’s alpha of 0.80, indicating its reliability.
WRMSD Reporting Intention and Reporting Experience
Reporting intention was assessed using a single question “If you experience work-related injuries or illnesses, would you be willing to report the disorders to your management?” Responses to this question were recorded as “yes” or “no” (Conner & Heywood-Everett, 1998). For individuals who had experienced WRMSDs within the past 12 months, they were asked whether they had reported WRMSDs to their management. Respondents were also queried about their experience witnessing the injury reporting behaviors of their colleagues or co-workers.
Data Analysis
Data analyses were conducted using STATA version 16.0 (Stata Corporation, College Station, TX). Descriptive statistics were employed, including frequency and percentage for categorical variables and means with standard deviation for continuous variables. To handle missing data, responses missing 5% or more of the questionnaires were initially excluded from the study. For multi-item measures, multiple imputation was used to address missing data effectively. A generalized linear mixed model was utilized, with a random intercept by employers, to identify significant factors influencing reporting attitudes. This model incorporated demographic and job characteristics, physical work factors, psychosocial work environments, musculoskeletal symptoms, and the experience of witnessing injury reporting, as guided by the literature on injury reporting behavior. Subsequently, the interaction effect of management safety priority was introduced into the model to assess whether the influence of management safety priority on injury reporting attitudes remained consistent across different long-term care facilities. The results were reported by Beta coefficients. Simple logistic regression analysis was employed to explore the relationship between reporting attitude and intention to report, as well as the behavior of reporting WRMSDs. Odds ratio (OR) and 95% confidence interval (CIs) were calculated to measure these relationships. Statistical significance was defined as a p-value less than .05.
Results
Characteristics of the Study Participants
The study included a total of 377 direct care workers, with 139 individuals in long-term care hospitals and 238 in nursing homes (Table 1). Approximately 87% of the participants were female, and 27% were immigrants. The majority of the respondents were married (95.9%), had a high school education (68.6%), and held temporary or independent work arrangements (73.3%). On average, the participants had a mean age of 60.7 years and had worked as direct care workers for an average of 5.9 years. Two-thirds of participants (68.5%) perceived that worker safety was a priority in their organization, and 91.2% had received safety training related to injury reporting. More than half of the respondents (59.1%) had witnessed the injury reporting of others, within the past 12 months, 54.6% had experienced WRMSDs. Nearly half of the participants (48.9%) expressed no intention to report their WRMSDs, and the majority of those who had experienced WRMSDs did not report them to their management (85.5%). The mean score for WRMSD reporting attitudes was 3.8.
Demographic, Job, Psychosocial, and Health Characteristics Among Direct Care Workers in Long-Term Care Facilities in Korea (N = 377).
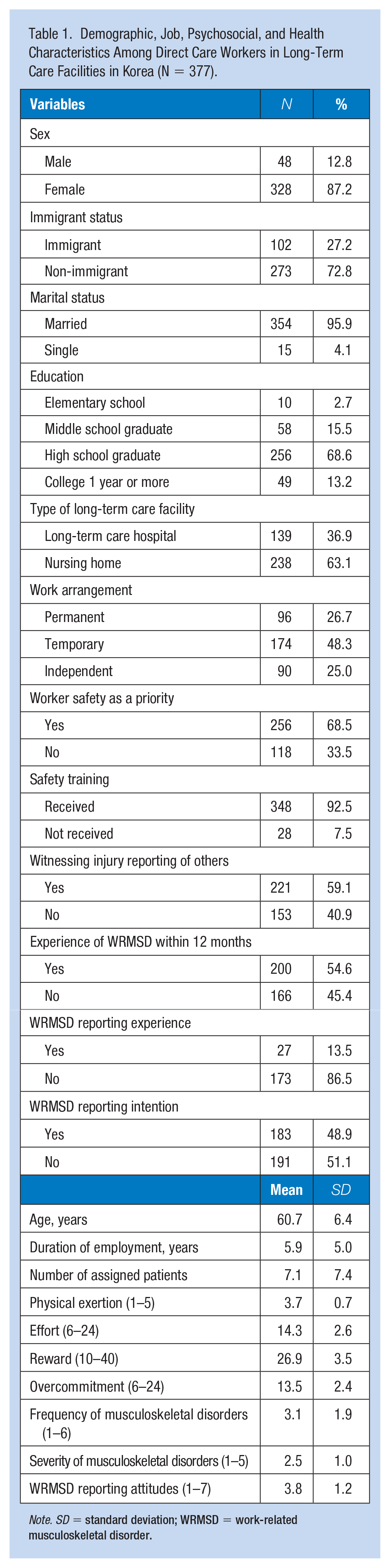
Note. SD = standard deviation; WRMSD = work-related musculoskeletal disorder.
Factors Associated With Reporting Attitudes
Table 2 presents the results of a generalized linear mixed analysis examining the factors associated with direct care workers’ attitudes toward reporting WRMSDs. Direct care workers with a longer duration of employment (coefficient = −0.01, p = .01) and a higher frequency of musculoskeletal disorders (coefficient = −0.18, p < .01) were less likely to hold positive reporting attitudes. Reporting attitudes were positively associated with safety training for injury reporting (coefficient = 0.65, p = .03), experience of WRMSDs (coefficient = 0.71, p = .01), higher severity of musculoskeletal disorders (coefficient = 0.20, p = .03), and management prioritizing worker safety (coefficient = 0.5, p = .001). A moderating effect of management safety priority was added to the model, but no significant effect was observed (data not shown).
Linear Mixed Model Analysis of Factors Associated With Attitude Toward Work-Related Musculoskeletal Disorder (WRMSD) Reporting (N = 288)
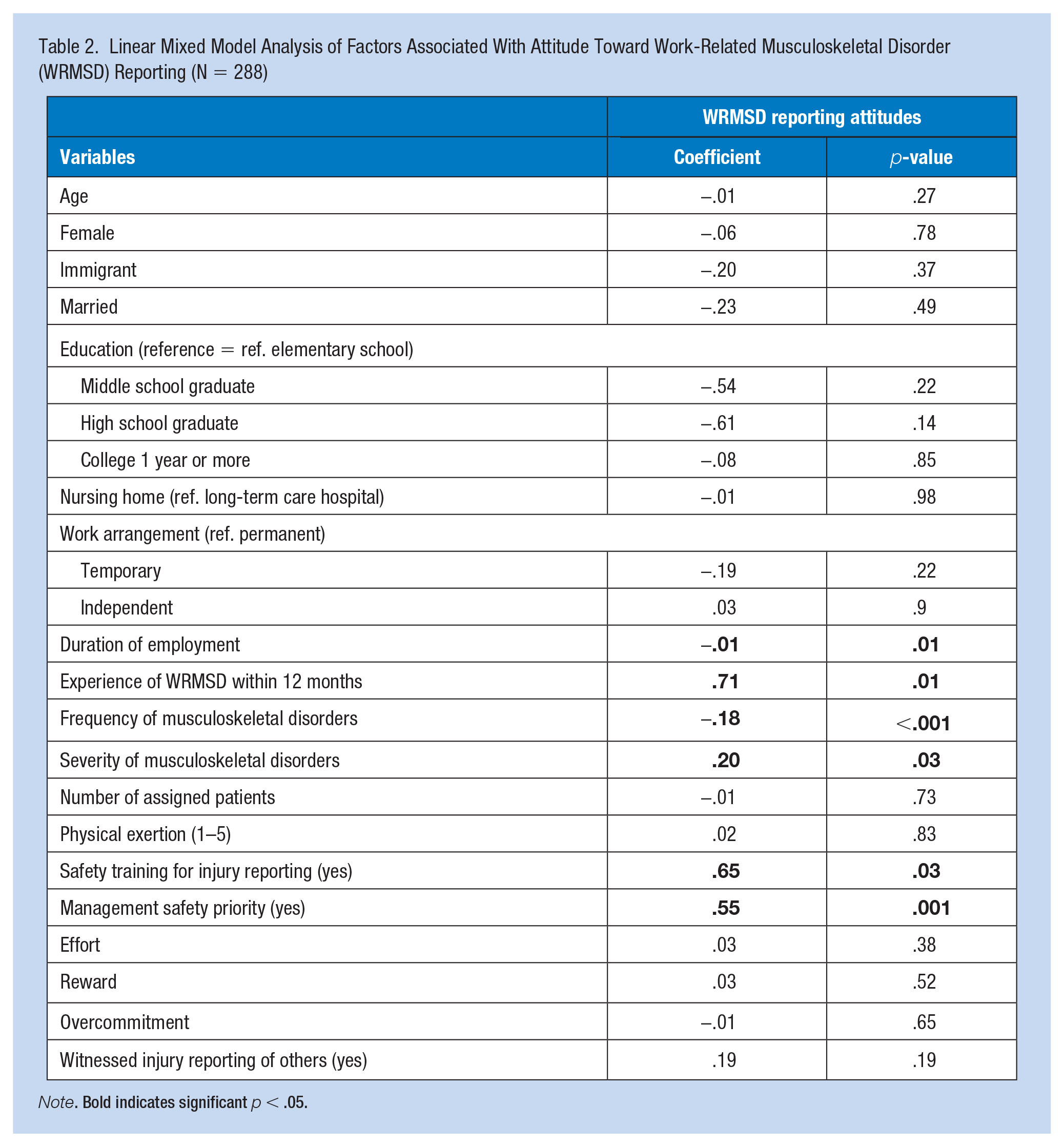
Note. Bold indicates significant p < .05.
The Relationship Between Reporting Attitudes and Reporting Intention and Behavior
Table 3 illustrates the association between WRMSD reporting attitudes and both WRMSD reporting intention and actual reporting. Direct care workers who held positive reporting attitudes were significantly more likely to express an intention to report WRMSDs to their management (OR = 13.17, 95% CI = 7.76–22.36). Direct care workers with positive attitudes toward WRMSD reporting also had 2.88 times greater odds of actually reporting WRMSDs when compared to those with negative attitudes (OR = 2.88, 95% CI = 1.26–6.61).
The Relationship Between Reporting Attitudes and Reporting Intention and Actual Reporting of Work-Related Musculoskeletal Disorders (WRMSDs): Using Bivariate Logistic Analysis
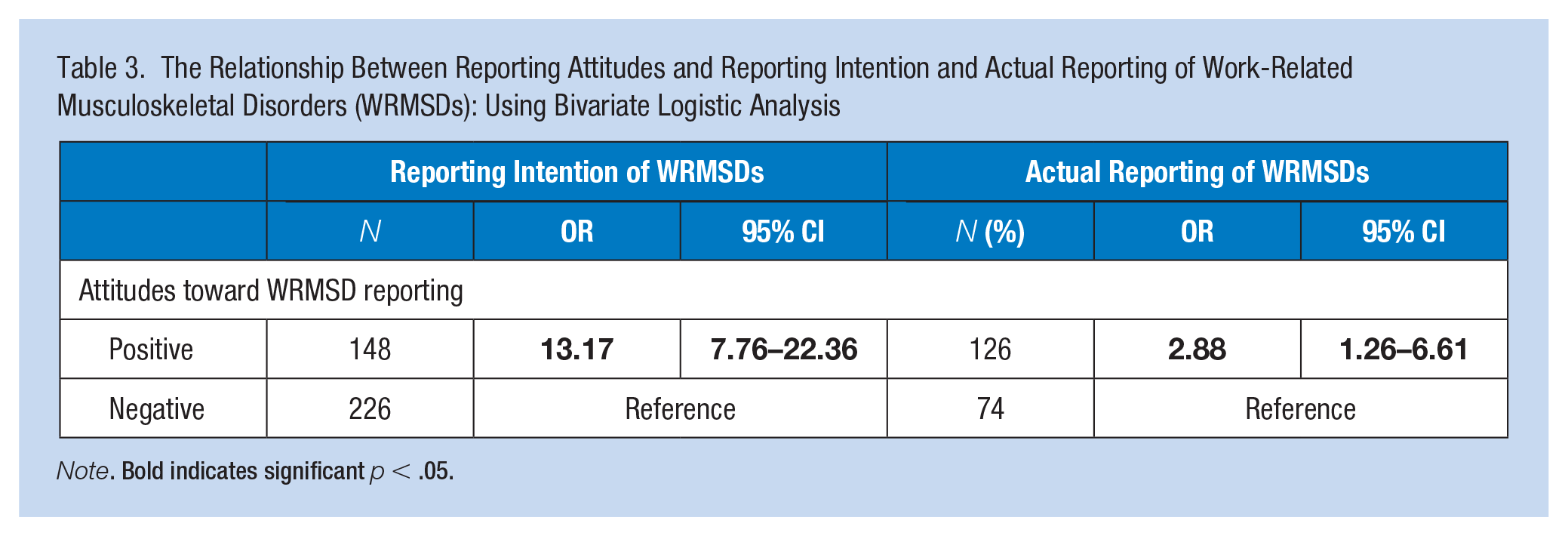
Note. Bold indicates significant p < .05.
Discussion
This study investigated the factors associated with WRMSD reporting attitudes among direct care workers in long-term care settings in South Korea. Several key findings emerged from this study. A significant proportion of direct care workers expressed a lack of intention to report WRMSDs (51.1%), and only a small fraction of those who experienced WRMSDs actually reported them to their management (13.5%). This highlights the presence of barriers to reporting within this population. Furthermore, WRMSD reporting attitudes were found to be significantly associated with both reporting intention and actual reporting behavior, underscoring their critical role in shaping reporting practices.
This study found that direct care workers with longer length of tenure tended to have less positive reporting attitudes. These findings are in line with previous research among pharmacists, suggesting that individuals with more years of experience may have less favorable attitudes toward incident reporting (Gavaza et al., 2011). They observed a negative correlation between incident-reporting attitudes and years of experience in pharmacy practice (r = −0.136, p = .008). One possible explanation for this trend is that workers with longer job tenure may have witnessed or experienced punitive disciplinary actions in response to injury reporting in the past. In earlier years, there was a prevailing perception that work-related injuries or illnesses were often attributes to individual negligence (Frederick & Lessin, 2000; Gavaza et al., 2011). This historical context may have led to a sense of frustration among direct care workers with longer experience in the field. They may recall instances where injury reporting led to negative consequences, such as reprimands or disciplinary actions, and this could contribute to their less favorable attitudes toward reporting. Overcoming the legacy of punitive measures and ensuring that reporting is met with support and solutions rather than blame is essential for promoting positive reporting attitudes among all workers, regardless of their tenure.
This study sheds light on the relationship between WRMSD experience and reporting attitudes among direct care workers. It is evident that workers who have experienced a WRMSD within the past 12 months were more likely to hold positive reporting attitudes. This connection can be understood by considering the criteria for reporting injuries and complaints under the OSHA. In Korea, workers have the right to report work-related injuries or illnesses (Oh, 2014). However, for reporting to be valid, the injuries must be proven to be work-related (Oh, 2014). In such cases, workers who have suffered from work-related injuries or illnesses are responsible for providing evidence of the work-relatedness themselves (Oh, 2014). Consequently, those who meet these criteria may perceive reporting as beneficial, leading to more positive attitudes.
Severity and frequency of musculoskeletal symptoms also played a role in shaping injury reporting attitudes, but their influence differed. Severity of musculoskeletal symptom had a positive relationship with reporting attitudes in this study, consistent with findings that highlight symptoms severity as a significant factor contributing to actual injury reporting (Kyung et al., 2023). In the context of South Korea’s Serious Accidents Punishment Acts, severe symptoms may prompt workers to recognize the necessity of taking action (Korea Legislation Research Institute, 2021). They may feel compelled to report their condition to management to explore potential solutions, such as requesting sick leave or seeking job modification or intervention to mitigate the risk of further injury. Conversely, symptom frequency was inversely associated with injury-reporting attitudes in this study. This finding aligns with prior research that identified symptoms frequency as a barrier to actual reporting (Siddharthan et al., 2006). Siddharthan et al. (2006) revealed that workers who already reported more than three injuries were nearly twice as likely to avoid reporting additional work-related injuries compared to those who had reported three or less injuries. This may be linked to a fear of negative repercussions. Workers who experience recurrent injuries or illnesses may worry about being stigmatized as negligent workers and believe that injury reporting is primarily used to assign blame. Frequent injuries may also contribute to a sense of normalcy within the workplace, leading workers to perceive such incidents as routine and not worthy of reporting.
Safety training was another significant factor affecting reporting attitudes. The study’s findings regarding the positive impact of safety training on workers’ reporting attitudes are consistent with previous research conducted by Green et al. (2019). These studies demonstrated the effectiveness of educational interventions in improving attitudes toward injury reporting. Green et al. (2019)’s study involving janitors showed that the intervention group experienced a significant reduction in barriers related to injury reporting, such as perceiving injuries as a part of the job (reduced from 8% to 2%) and fearing negative consequences (reduced from 8% to 2%). This suggests that educational programs can effectively address misconceptions and fears that may hinder reporting. Similarly, Jansma et al. found that workers who received patient safety education showed significant improvement in incident reporting attitudes and intentions. This improvement persisted even 16 days after the education was provided, indicating that the positive effects of training can endure over time. In light of these findings, it becomes clear that safety and health training should be considered an essential component of any organization’s effort to create a safe workplace. Providing workers with knowledge about their rights and the importance of injury reporting can contribute to a culture of safety where employees feel empowered to report incidents without fear of negative consequences (Green et al., 2019).
This study’s findings highlight the critical role that organizational safety culture and management priorities play in shaping workers’ attitudes toward injury reporting, which aligns with earlier research (H. J. Lipscomb et al., 2015; Probst & Graso, 2013). Probst and Graso (2013)’s study among copper mining workers stressed the importance of a safe climate. Workers who perceived that their organization prioritized the safety of workers tended to have more positive attitudes toward injury reporting. This suggests that an organizational culture that emphasizes worker’s safety can contribute to fostering a more favorable reporting environment. H. J. Lipscomb et al. (2015)’s research provided further evidence of the impact of safety climate on injury reporting. Their study showed that when management did not prioritize worker’s safety, both the prevalence of non-reporting and non-reporting without fear increased significantly (H. J. Lipscomb et al., 2015). Specifically, workers who perceived a low priority on worker safety were 1.7 times more likely to experience underreported injuries and 1.4 times more likely to feel unable to report without fear compared to workers with a high emphasis on worker's safety (H. J. Lipscomb et al., 2015). The safety climate within an organization can send clear signals to workers about whether reporting incidents will be encouraged or met with punitive measures. When management actively promotes a safety-oriented culture and provides the necessary resources and support, workers are more likely to see the value in reporting injuries and feel comfortable doing so without fear of reprisal.
The significant relationship found in this study between injury reporting attitudes and injury reporting intention reinforces the notion that attitudes play a pivotal role in shaping reporting behavior. This consistency with earlier research underscores the importance of attitudes in influencing the intention to report incidents (Gavaza et al., 2011; Pfeiffer et al., 2010). Given these findings, Pfeiffer et al. (2010) integrated attitudes into a psychological framework that explains factors influencing the intention to report incidents. According to the theory of planned behavior, individual behavioral intention is assumed to be affected by attitudes and is considered a primary contributor to actual behavior (Ajzen, 1991). This finding highlights the notion that influencing reporting behavior begins with shaping attitudes.
This study found a significant relationship between injury reporting attitudes and actual reporting behavior, aligning with previous research that demonstrated a positive correlation between favorable reporting attitudes and increased rates of reporting occupational accidents (Probst & Graso, 2013). Many studies underscore the role of negative attitudes as obstacles to injury reporting (Evans, 2006; Pompeii et al., 2016). While researchers have been examining the complex interplay between attitudes and behavior for many years, the evidence regarding the attitudes-behavior association has exhibited variability and mixed results (Glasman & Albarracín, 2006). To improve the prediction of behavior, it is advisable to focus on attitudes closely aligned with the specific behavior of interest.
To the best of our knowledge, this study is the first to explore WRMSD reporting attitudes in a sample of direct care workers in South Korea. Nonetheless, several limitations need to be acknowledged. First, the data were collected from a nonprobability sample of direct care workers, primarily in nursing homes, within a single province in Korea. This limited scope may affect the generalizability of our findings to other settings. However, it is worth noting that our sample comprised participants from 19 different long-term care facilities, and we achieved a high response rate (86%), which may enhance the generalizability of our results. Second, the small sample size, particularly for reporting behavior, could have limited the statistical power of our analysis. Third, as the data relied on self-reported questionnaires, responses may have been influenced by recall or reporting bias, potentially leading to underestimation or overestimation of results. Finally, due to the cross-sectional design of the study, we cannot establish causal relationships between variables.
Implications for Occupational Health Practice
Timely identification of work-related injuries or illnesses is crucial for promoting workplace safety and health, and workers’ willingness to report incidents to management represents the initial step in this process. This study highlights the significant role of workers’ attitudes toward injury reporting in shaping their reporting intentions and actual behavior, and these attitudes may be moderated or mediated by the safety culture within the organization. Various factors, including the duration of employment, safety training, management’s safety priorities, experience with WRMSDs, and the severity and frequency of musculoskeletal symptoms, were identified as influencing reporting attitudes. To improve workers’ attitudes toward injury reporting and facilitate actual reporting, organizations should demonstrate a strong commitment to worker safety. This includes providing safety training that emphasizes injury reporting, particularly for workers with extended tenures and those frequently exposed to musculoskeletal issues. Future research employing a longitudinal study design, is recommended to validate and expand upon these findings.
Applying Research to Practice
The tasks of direct care workers are often challenging while offering few extrinsic reward. Despite the high risk of work-related injury or illness, many direct care workers did not report it to their management and tended to normalize it. This study identified that injury reporting attitudes were associated with duration of work, safety training for injury reporting, management safety priority, work-related injury/illness experience, and severity and frequency of the symptom. Organizational commitment to the priority of worker safety and safety training focusing on injury reporting is needed for workers especially those frequently exposed to musculoskeletal problems and with longer duration of employment to improve workers’ attitude toward injury reporting and facilitate actual reporting.
Footnotes
Acknowledgements
The authors would like to thank the study participants and the data collection site managers for their assistance and support. The authors also thank the department manager of the National Health Insurance Service (Dong-Hwa Lee) for his contribution to data collection.
Author Contribution
Kyung conceived the study, obtained the funding, conducted data collection, analysis, and interpretation, and drafted this manuscript. Lee contributed to the development of the study and critical review of the manuscript. Wagner participated in the critical revision of the manuscript. Harris-Adamson contributed by providing feedback for the revision of the manuscript. Hong provided substantive feedback on findings from the analysis and guidance for interpretation of findings. All authors participated in revisions of the important content for publication and approved the final version of the manuscript. All authors agreed to be accountable for questions related to its accuracy or integrity.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received the funding from the 2023 AAOHN Foundation Research Grant
Institution and Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of the University of California, San Francisco (Date: May 20, 2022, Identification number: #22-36334) and the Public Institutional Review Board in South Korea Date: May 20, 2022, Identification number: P01-202205-01-036).