
Abstract
Background:
According to the Total Worker Health® framework, safety culture including a reasonable workload among healthcare workers is essential to the security and well-being of patients, staff, and healthcare organizations. Evaluating the impact of the pandemic on the nursing workforce in different practice areas is critical for addressing workforce health and sustainability. The purpose of this study was to compare work and selfcare experiences among Alabama nurses between practice areas and the early pandemic years (2020 vs. 2021).
Methods:
A secondary analysis of cross-sectional Alabama State Nurses Association (ASNA) survey data was conducted. Kruskal–Wallis analysis of variance, Wilcoxon rank, and false discovery rates were examined.
Results:
There were 1,369 and 2,458 nurse survey responses in 2020 and 2021, respectively. By 2021, nurses reported worsening staff shortages, a greater need for retired and new graduate nurses to help with the workload burden, and perceptions of heavier emergency department workloads. Lower proportions of nurses reported the ability to engage in self-care activities and satisfaction with state and federal crisis management. Intensive care nurses were more likely to report staffing shortages while also reporting the lowest ability to engage in self-care.
Conclusions:
Overall, the Alabama nursing workforce perceived worsening work conditions in 2021 compared to when the pandemic began. Practice areas varied greatly in their responses, with acute and intensive care areas perceiving more difficult work conditions. Total Worker Health® programs should be designed to promote and support nurses’ well-being based on their experience and the needs of specific practice areas.
Background
The COVID-19 pandemic has challenged healthcare delivery systems around the globe (Jabarulla & Lee, 2021). Because the many different settings in which nurses work each have their own unique set of stressors, cultures, and milieus, examining the impact of the COVID-19 pandemic on the nursing workforce in different practice areas is critical for addressing workforce health and sustainability (Chan et al., 2021; Daly et al., 2020; Haas et al., 2020; Poortaghi et al., 2021). As frontline providers, nurses are qualified to provide critique of working conditions, identification of barriers and facilitators to the delivery of quality care, and early recognition of system-level failures that became increasingly evident during the pandemic (Daly et al., 2020; Haas et al., 2020).
As the COVID-19 pandemic began, hospitals around the world experienced a shift in healthcare delivery demand with nursing workforce resources that were already in a state of short supply (Andel et al., 2022; Kiekkas et al., 2019; Lasater et al., 2021; Twigg et al., 2015). Less is understood about how nurses who worked in different practice areas or work settings experienced the onset and early COVID-19 variant surges of the pandemic. Some nurses reported furloughs or cuts in work hours (Norvell & O’Donnell, 2020), while others reported understaffed or unsafe staffing levels (Andel et al., 2022; Lasater et al., 2021). There is limited evidence comparing nurses’ experiences and perceptions among different practice settings, specifically related to nursing shortages, the extent to which their emergency departments (EDs) were overwhelmed, their ability to engage in self-care, and their trust in state and federal elected officials.
Alabama trails other states in attention to nursing workforce issues (e.g., retention, recruitment, educational capacity, and the distribution of nursing workforce resources). Across the United States, other states have legislatively established and funded nursing workforce centers to continuously collect and analyze data about fluctuations in this largest segment of the healthcare workforce. For example, the Georgia Nursing Workforce Center was established to research, address, and monitor issues of supply and demand for nursing and distribute nursing workforce resources (Emory University, 2024). During the pandemic, a decline in workforce supply, increasing patient care demands, nurse burnout, and inequitable compensation of nurses in Alabama made headline news (Poitevint, 2021). However, the problems identified were not new, rather they were exacerbated by the COVID-19 pandemic (Dick et al., 2023; Montgomery et al., 2021, 2022).
Findings from a pre-pandemic 2019 to 2020 study (Dick et al., 2023) suggested that Alabama hospitals were experiencing critical nursing workforce shortages at that time. Chief Nursing Officer (CNO) perceptions of the acute care registered nurse (RN) labor market were concerning as 68% of CNOs survey respondents reported high RN demand and difficulty filling positions. The need was especially great for experienced nurses; 80% of participating CNOs reported high demand for seasoned RNs. These CNOs reported the most difficult to fill acute care RN positions were medical-surgical (72%), ED (72%), operating room (36%), and adult critical care (28%). The top factor impacting facility demand for RNs, as reported by the CNOs, was higher turnover and less retention of RNs than the year before (56%) while 24% also reported an anticipated increase in hospital bed capacity at their facility during the year following the study (Dick et al., 2023).
A 2018 Alabama Hospital Staff Nurse Study described patient-to-nurse ratios as reported by Alabama nurses. The average patient-to-nurse ratios were 2:1 in intensive care units (ICU) (min = 1:1, max = 9:1), 3:1 in pediatric units (min = 1:1, max = 7:1), 4:1 in surgical units (min = 1:1, max = 11:1), 5:1 in medical units (min = 1:1, max = 21:1), and 7:1 in rehabilitation units (min = 3:1, max = 18:1) (Prapanjaroensin et al., 2020); not every state reports required nurse-to-patient ratio. However, California has mandated patient-nurse ratios including 2:1 for ICU, 4:1 for pediatric units, 5:1 for medical/surgical, and no unit has over 6:1 patient-nurse ratios (National Nurses United, 2024), and Pennsylvania has proposed patient-nurse ratios as 2:1 for ICU, 3:1 for pediatric units, 4:1 for medical/surgical, and 5:1 for rehabilitation units (The General Assembly of Pennsylvania, 2021). Research indicates that a greater number of patients per nurse has been correlated to overall missed nursing care which is the amount of care that was not completed by nurses (e.g., ambulation, feeding, turning, and hygiene) during the last seven recent shifts (Campbell et al., 2020). In addition, the majority of Alabama staff nurses reported moderate to high levels of Personal, Work-, and Client-related Burnout domains (89%, 88%, and 64%, respectively) of the Copenhagen Burnout Inventory even before the pandemic (Montgomery et al., 2021, 2022). The Staffing and Resources Adequacy subscale of the Practice Environment Scale of the Nursing Work Index (Lake, 2002) had the highest correlations to all burnout subscales (Personal, Work-, and Client-related Burnout) (Montgomery et al., 2021), indicating that insufficient staff and other human and material resources available to provide patient care was strongly associated to burnout.
To promote nurse well-being, the Total Worker Health® (National Institute for Occupational Safety and Health [NIOSH], 2016) approach prioritizes a hazard-free work environment to keep nurses safe and healthy by considering staffing and resource adequacy, e.g., workload, stress level, and interactions with coworkers and supervisors. Total Worker Health® for healthcare workers can be defined as policies, interventions, and evidence-based practices that protect healthcare workers including staff nurses from work-related mental and physical problems and enhance their well-being (NIOSH, 2016). This is reflected by a positive safety culture in healthcare that is essential to the security and well-being of patients, staff, and healthcare organizations (UMass, 2024). Job stress (e.g., long working hours, high workload, burnout, working conditions, and fatigue) is impacted by safety culture (Zabin et al., 2023). Lower patient-to-nurse ratios results in higher quality of patient care, lower workload, fewer nurse turnover, and shorter patient length-of-stay in the hospital (Aiken et al., 2014; de Véricourt & Jennings, 2011). Individual leaders and/or organizations that wish to start an effective workplace program should understand the current state of work, the workforce, and the workplace (UMass, 2024). This paper provides a baseline finding on the Alabama nursing workforce in the early COVID-19 pandemic years by using the Total Worker Health® approaches (NIOSH, 2016).
In April 2020, the Alabama State Nurses Association (ASNA) began deploying a series of surveys for nurses across the state of Alabama to record nurse experiences and concerns throughout the COVID-19 pandemic. The specific aims of this study were to compare Alabama nurses’ perceptions of the nursing shortage, the need for retired and new graduate nurse help, perceptions of the ED workload, their ability to engage in self-care, and their satisfaction with state and federal crisis management between practice areas (inpatient acute care, intensive care, long-term care assisted living, outpatient care, and others) and the early pandemic years (April 2020 vs. February 2021).
Methods
Study Design and Setting
A secondary analysis of cross-sectional survey data was conducted. A number of potential survey respondents could not be estimated because the survey link could be forwarded or shared by anyone that received the initial link. In addition, records were not kept by the organization about the number of email addresses that received and/or rejected the invitation to participate in the survey. Therefore, the response rate could not be calculated. Two datasets (from 2020 to 2021) were obtained from the ASNA. The data sets were previously derived by ASNA via a SurveyMonkey® electronic survey that consisted of six Likert-type scale survey items and an open-text question to collect information about the survey respondents’ primary practice areas. The survey was distributed to all nurses, both RNs and LPNs, in Alabama who had email addresses on file with ASNA, although we were unable to access those data.
Ethics Approval
Exempt institutional review board (IRB) approval was obtained (No. IRB-300009006) from the first author’s organizational IRB for conducting this study.
Measurements
Survey items were created by ASNA and included verbatim the following:
My perception is that my facility has a shortage of nurses (called “perceptions of nursing shortage”),
We need retired nurses and new grads to fill needs in certain practice areas (called “the need for retired and new graduate nurse help”),
Our ED has been overwhelmed (called “perceptions of the ED workload”),
I have been able to maintain a reasonable amount of self-care, diet, exercise, relaxation and sleep (called “ability to engage in self-care”),
Our state elected officials have done a great job dealing with this crisis (called “satisfaction with state crisis management”), and
Our federal elected officials have done a great job dealing with this crisis (called “satisfaction with federal crisis management”).
These six items were rated with a five-point Likert-type scale range from 1 (Strongly disagree) to 5 (Strongly agree). The practice area question was an open-text item. Two researchers independently categorized each practice area response into one of five practice areas, then compared their categorization and adjudicated any differences. The practice settings used for this study included: (a) inpatient acute care, (b) intensive care (ICU), (c) long-term care/assisted living (LTC), (d) outpatient care, and (e) other. Respondents who did not designate a practice setting were deleted from analyses and responses that were not clearly specified (e.g., “pediatrics”) were categorized as “other.”
Data Collection and Data Analysis
Data were exported into a comma split value file and analyses were performed using R Studio statistical software version 4.1.2. To compare the perceptions between the practice areas, Kruskal–Wallis analysis of variance was conducted, except for the perceptions of ED workload item, where Wilcoxon rank sum tests were conducted to compare between inpatient acute care and ICU nurses. To compare the perceptions between years, Wilcoxon rank sum tests were conducted. Furthermore, effect sizes (Eta2 [η2] and Cohen’s d) were conducted for all comparisons. With multiple comparison tests, the probability of a type I error grows with the number of the tests. Therefore, the Benjamini-Hochberg False Discovery Rates (FDR) were calculated to assess the expected proportion of type I errors (false positive) (Benjamini & Hochberg, 1995).
Results
For 2020 and 2021, respectively, a total of 1,618 and 2,561 participants responded to the online survey; however, only 1,369 (85%) and 2,458 (96%) provided the practice area information for each of those years, respectively. Table 1 presents the descriptive statistics of each item by year and practice area. In 2020, LTC nurses reported highest scores on perceptions of nursing shortage (M = 4.3), the need for retired and new graduate nurse help (M = 3.9), and satisfaction with federal crisis management (M = 3.0). They also reported the lowest engagement in self-care (M = 2.7). Intensive care nurses reported the highest perceptions of ED workloads in their respective facilities (M = 2.8), while outpatient nurses were more likely to engage in self-care (M = 3.2) and be satisfied with state crisis management (M = 2.9). In 2021, LTC nurses most frequently reported the need for retired and new graduate nurse help (48%) and satisfaction with state crisis management (27%). Intensive care nurses reported the highest perceived nursing shortage in their respective facilities (76%) (M = 4.7), and lowest ability to engage in self-care (2%) (M = 2.3) and satisfaction with state (M = 2.3) and federal (M = 2.2) crisis management. Outpatient nurses reported the greatest ability to engage in self-care (M = 2.9) and highest levels of satisfaction with federal crisis management (M = 2.5). Inpatient acute care nurses reported perceptions of highest ED workloads (M = 4.4).
Descriptive Statistics of Items by Practice Areas and Years
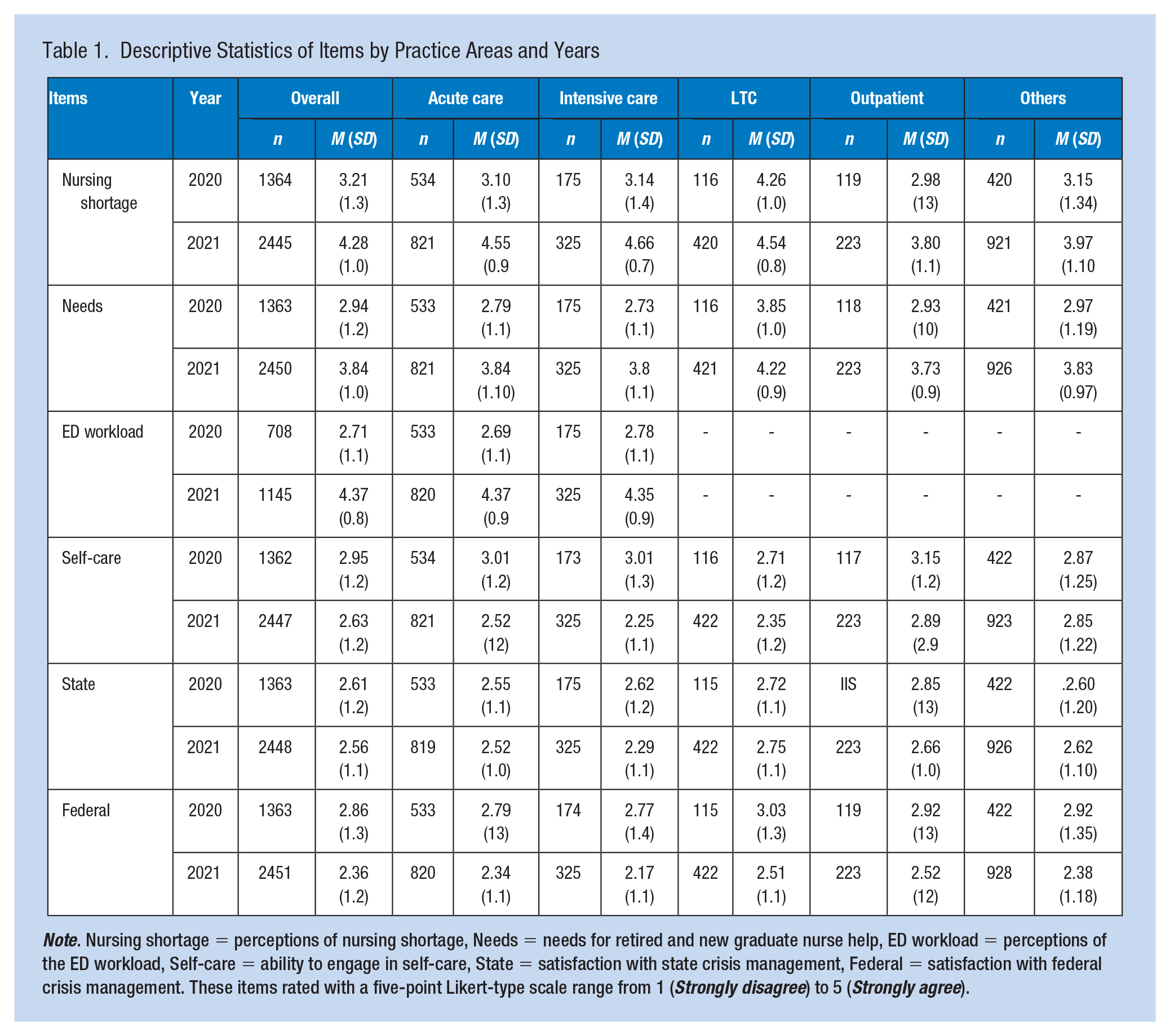
Note. Nursing shortage = perceptions of nursing shortage, Needs = needs for retired and new graduate nurse help, ED workload = perceptions of the ED workload, Self-care = ability to engage in self-care, State = satisfaction with state crisis management, Federal = satisfaction with federal crisis management. These items rated with a five-point Likert-type scale range from 1 (Strongly disagree) to 5 (Strongly agree).
Table 2 presents the comparison between the years 2020 and 2021. Overall, nurses’ perceptions of nursing shortage, the need for retired and new graduate nurse help, and perceptions of the ED workload were significantly higher in 2021 compared to 2020 (BH-FDR < .001, Cohen’s d = 0.841–1.281). The ability to engage in self-care, and satisfaction with federal crisis management was rated significantly lower in 2021 (BH-FDR < .001, Cohen’s d = 0.260–0.413). Nurse satisfaction with state crisis management was not significantly different between years 2020 and 2021.
Comparison Tests for All Items Between Year 2020 and 2021
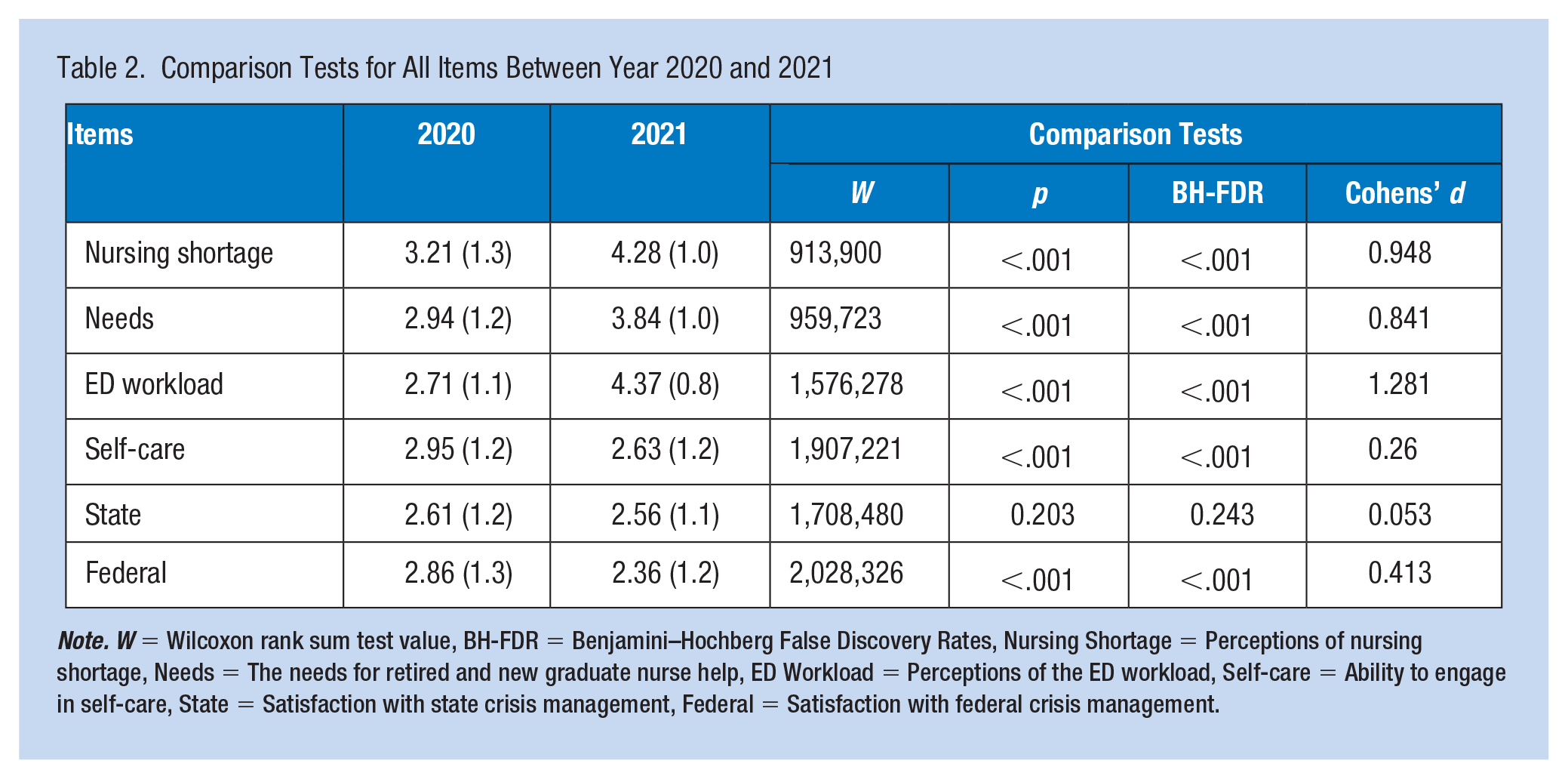
Note. W = Wilcoxon rank sum test value, BH-FDR = Benjamini–Hochberg False Discovery Rates, Nursing Shortage = Perceptions of nursing shortage, Needs = The needs for retired and new graduate nurse help, ED Workload = Perceptions of the ED workload, Self-care = Ability to engage in self-care, State = Satisfaction with state crisis management, Federal = Satisfaction with federal crisis management.
Table 3 presents the comparison tests between the practice areas in years 2020 and 2021. In 2020, perceptions of nursing shortage, the need for retired and new graduate nurse help, and ability to engage in self-care were significantly different between the practice areas (BH-FDR < .05, η2 = 0.008–0.063). In 2021, perceptions of nursing shortage, the need for retired and new graduate nurse help, ability to engage in self-care, and satisfaction with state and federal crisis management were significantly different between the practice areas (BH-FDR < .05, η2 = 0.007–0.107). ED workload was not significantly different between ICU and inpatient acute care in 2020 and 2021 (BH-FDR = 0.44; 0.92; Cohen’s d = −0.075; 0.024), resoectively.
Overall Comparison Tests for All Items Between Different Practice Areas in Each Year
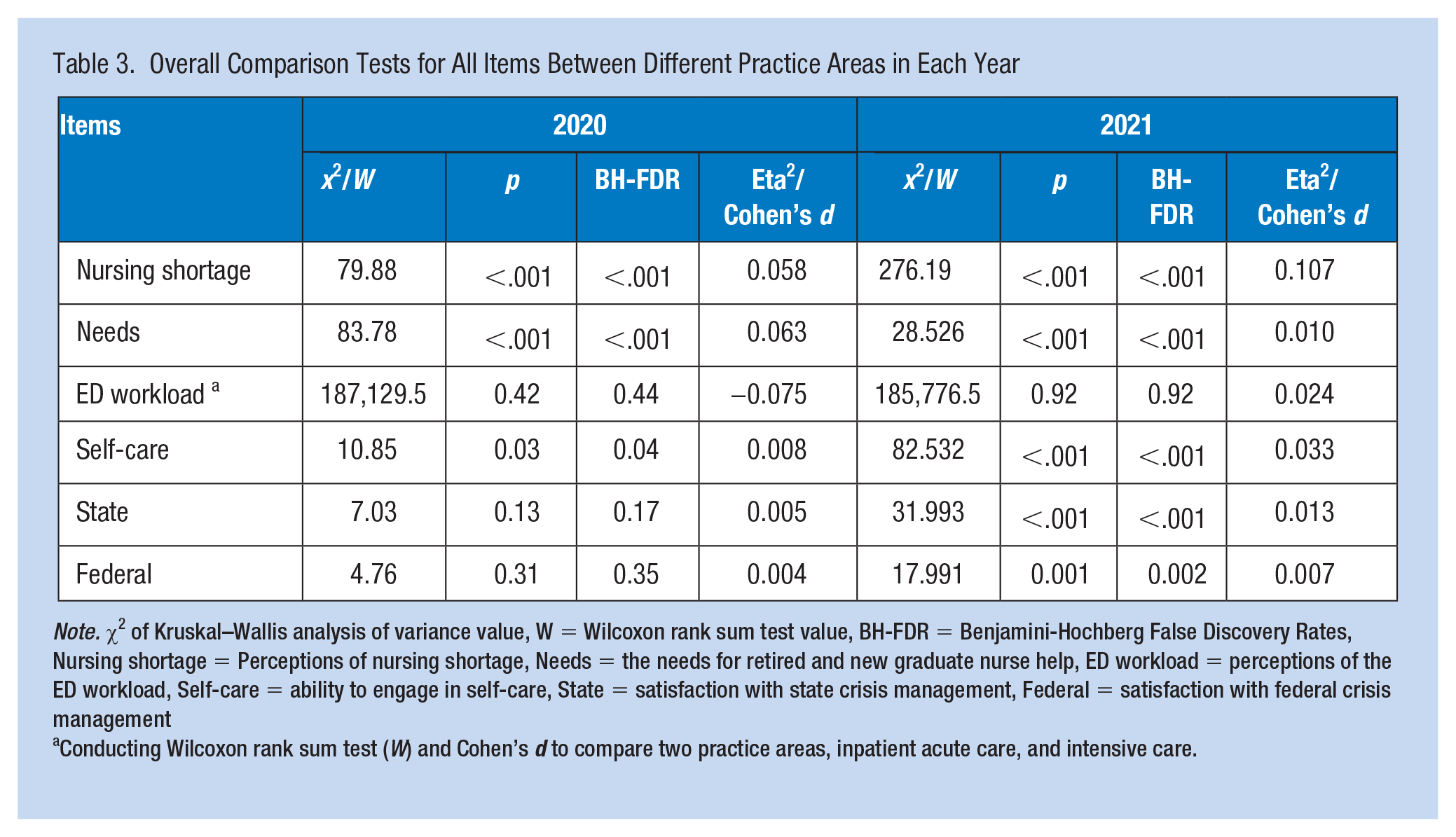
Note. χ2 of Kruskal–Wallis analysis of variance value, W = Wilcoxon rank sum test value, BH-FDR = Benjamini-Hochberg False Discovery Rates, Nursing shortage = Perceptions of nursing shortage, Needs = the needs for retired and new graduate nurse help, ED workload = perceptions of the ED workload, Self-care = ability to engage in self-care, State = satisfaction with state crisis management, Federal = satisfaction with federal crisis management
Conducting Wilcoxon rank sum test (W) and Cohen’s d to compare two practice areas, inpatient acute care, and intensive care.
Discussion
Alabama’s ICU nurses’ strong agreement with perceptions of a nursing shortage, low self-care ability, and low satisfaction with state and federal officials’ crisis management align with findings from a national survey of critical care nurses through the American Association of Critical Care Nurses. Across the United States, critical care nurses reported burnout (85%), moral distress (50%), and risk for post-traumatic stress disorder (47%) (Guttormson et al., 2022a). Guttormson et al. (2022b) also asked nurses using open-ended questions about their experience during the COVID-19 pandemic. Nurses perceived inadequate staffing levels, low satisfaction with federal government leadership, and low hospital leadership support, which are consistent with Alabama nurses’ perceptions (Guttormson et al., 2022b). These findings are not surprising given the increased burden of critically ill COVID-19 patients, resource shortages, and exposure to patient death (Foli et al., 2021) in critical care units across the country.
Nurses working in long-term care and assisted living facilities expressed a need for retired and new graduate nurses’ help, spotlighting staffing shortages in Alabama LTC facilities. A significant proportion of LTC staff is comprised of unlicensed assistive personnel (UAP) and licensed practical nurses (LPN)/ licensed vocational nurses (LVN). During the first year of the pandemic, UAPs and LTC facilities had the highest turnover rates of any health occupation and workplace, respectively (Frogner & Dill, 2022). While other practice areas are recovering, LTC staff turnover rates are the slowest to recover and have worsened over time (Frogner & Dill, 2022). In 2020, the number of NCLEX-PN test takers was the lowest in 10 years (NCSBN, 2022). Although the majority of LPNs/LVNs still work in LTC settings, the proportion of LPNs/LVNs employed by hospitals has increased from 13.5% (2018) to 14.7% (2021) (NCSBN, 2022), further compounding the LTC staffing shortage.
Alabama nurses working in inpatient acute care settings were more likely to strongly agree that their EDs are overwhelmed compared to nurses from other practice areas. Across the United States, ED visits decreased drastically in the early phases of the pandemic (down 42% in April 2020 from April 2019) (Hartnett et al., 2020). ED visits increased from December 2020 to January 2021, albeit 25% lower than the previous year (Adjemian et al., 2021). Although ED visit encounters were down overall, increased COVID-19 admissions, limited bed capacity, hospital overcrowding, and staffing shortages resulted in extended ED lengths of stay, overwhelming the ED capacity in many cases (Lucero et al., 2021).
In 2021, Alabama nurses in all practice areas implicated staffing and heavy workload concerns as well as limited health promoting behavior. Our findings mirror those of the American Nurses Foundation (ANF). In their initial COVID-19 Survey from March to April 2020, 68% (n = 21,760) of U.S. nurses voiced concern over short-staffing (ANF, 2020a). Throughout the first year of the pandemic, less than half of U.S. nurses reported using self-care techniques such as regular exercise, balanced diet, and relaxation, while over half of the nurses reported difficulty sleeping or sleeping too much (ANF, 2020b, 2020c). In 2021, most nurses agreed that consistent and better national health policies and public intervention plans (74%) and increased staffing (67%) would prepare the health workforce for future health crises (ANF, 2021).
In 2020, 20% of U.S. nurses surveyed by Smiley et al. (2021) reported an intent to retire or leave the nursing profession in the next 5 years. To help alleviate the immediate staffing crisis, nursing schools and state legislators found creative ways to educate and graduate nursing students during the pandemic, such as through virtual simulation-based training, practice-academic partnerships (facilitating clinical experiences as paid or unpaid “essential personnel”), and allowing supervised practice of pre-licensed nursing students and recent graduates (NCSBN, 2022). Presently, nursing schools in regions across the country are experiencing full-time faculty vacancies (7%, Midwest; 8.1%, South; 8.3%, North Atlantic; 9%, West) (American Association of Colleges of Nursing, 2022). It is imperative to the health of U.S. citizens and the nursing workforce that nursing schools are well-equipped with funding and faculty to educate the next generation of nurses to replace retirees and those leaving the profession.
The results of this study provide a baseline snapshot of how Alabama nurses perceived their workload, leadership, and state and federal crisis management. Based on the Total Worker Health® framework, this paper reports on important concerns regarding the health of the Alabama nursing workforce and provides initial evidence for healthcare leaders to prioritize and plan for enhancement of nurse well-being. Interventions or programs that will enhance nurses’ well-being are needed especially for ICU nurses.
Limitations
The first survey (2020) was launched early during the pandemic, and many nurses may have been too overwhelmed to respond to the survey; the number of responses was lower than the second survey (2021). Furthermore, there were 249 and 103 responses from years 2020 and 2021, respectively, that did not respond to the practice area question and were excluded in the analysis. Because this study was survey data collected from Alabama nurses only, the findings cannot be generalized to nurses employed in other parts of the United States. Finally, inherent to the nature of secondary data analysis of existing data, some variables that are potentially useful for this paper such as actual staffing level, nurse well-being, and burnout were not collected.
Recommendations and Implications for Occupational Health Practice
While the pandemic is ongoing, the most severe staffing shortages appear to be in the intensive and acute care settings. Total Worker Health® can be a framework for policies, programs, and practice that integrate workplace safety culture and enhance nurses’ well-being. Nurses may benefit from shift arrangements and supplemental staffing to help them maintain a reasonable amount of self-care, diet, exercise, relaxation, and sleep. Healthcare administrators must actively engage with frontline nurses to regain trust and take immediate steps toward improvement of staffing conditions and work environments.
System-level changes that support fundamental respect for the self-care needs of nurses must become a priority for organizations wishing to recruit and retain nurses in the workforce. Nursing education programs can learn from the experiences of frontline nurses during the COVID-19 pandemic and commit to educational preparation that results in an elevation of the status of nursing professionals. Nurses must feel empowered to not only advocate for patients, but also move policy and system-level changes toward the realization of work environments that support reasonable workloads, safe staffing levels, self-care practices, and mental health resources to help deal with the extensive amount of death during the pandemic. Finally, nursing professionals have the expertise and collective capacity to drive policy changes. Professional organizations have a responsibility and an opportunity at the current time to represent the nursing workforce effectively by driving a culture shift that not only values the quality of care for patients but also values the safety and self-care of healthcare providers.
Conclusion
Based on the Total Worker Health® framework, this study defined the concerns regarding the health of the Alabama nursing workforce. Although nationwide surveys include nurses from Alabama, their representation has been limited. To our knowledge, the 2020 and 2021 ASNA surveys represent the largest group of Alabama nurses’ COVID-19 experiences to date. The perceptions of Alabama nurses grew worse in 2021 relative to the nursing shortage, the need for retired and new graduate nurse help, perceptions of the ED workload, ability to engage in self-care, and satisfaction with state and federal crisis management. Findings from this study highlight important concerns regarding the health of the Alabama nursing workforce and priorities for health policy. Total Worker Health® can also be a framework for policies, programs, and practice that address these important concerns.
Applying Research to Occupational Health Practice
Our findings provide a baseline result of the nurses’ perceptions of their workplace which can impact their well-being. Alabama nursing workforce perceived worsening work conditions in 2021 compared to when the pandemic begacn. This underscores the importance of shared governance structures within organizations that empowers nurses to create healthy work environments. Our study also found that practice areas varied greatly in nurse responses, with acute and intensive care areas faring the worst. Occupational health providers and nurse leaders should design programs that help promote and support nurses’ well-being based on their concerns and needs, specifically in acute and intensive care settings; for example, an occupational health nurse can examine job roles, recognize health effects from hazardous exposure, and design programs that prevent hazardous exposures and promote well-being such as resilience training.
Footnotes
Acknowledgements
The authors would like to thank all participants for their great contribution to this study. Also, we would like to thank ASNA for providing the data.
Author Contribution
Concept and design: Aoyjai Montgomery, Patricia Patrician. Acquisition of the data: Patricia Patrician. Analysis and interpretation: Aoyjai Montgomery. Drafting of the manuscript: Aoyjai Montgomery, Courtney Sullivan, Tracey Dick, Charlene Roberson, Lindsey Harris, Patricia Patrician. Critical revision of the manuscript: Aoyjai Montgomery, Courtney Sullivan, Tracey Dick, Charlene Roberson, Lindsey Harris, Patricia Patrician. Final Approval: Aoyjai Montgomery, Courtney Sullivan, Tracey Dick, Charlene Roberson, Lindsey Harris, Patricia Patrician.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
The study was approved as non-human subjects research by the University of Alabama at Birmingham (No. IRB-300009006) on March 22, 2022.