
Abstract
Background
Healthcare workers (HCWs) faced substantial risk of infection during the COVID-19 outbreak. This study aims to determine the prevalence of anti-SARS-CoV-2 antibodies in a cross-sectional sample of HCWs as well as risk factors associated with exposure to SARS-CoV-2.
Methods
The study was conducted between March and May 2021 at the American University of Beirut Medical Center (AUBMC), a tertiary hospital located in Lebanon. Socio-demographic and clinical data, as well as data on exposure, PCR results, PPE adherence, and vaccination status, were collected using an online questionnaire. Sera were also collected to determine seropositivity using commercially available enzyme-linked immunoassay (ELISA) targeting the spike (S) and the nucleocapsid proteins (NCP) of SARS-CoV-2.
Findings
Among 92 recruited HCWs, 72.3% received PPE training, more than 70% were adherent to using appropriate PPEs, and around 80% were vaccinated. Nurses in this study population were at higher risk of exposure compared to medical doctors, technicians, and other HCWs. Among the HCWs who performed a PCR test, 28.6% were infected with SARs-CoV-2 with workplace exposure not associated with COVID-19 infection. All vaccinated HCWs were seropositive for anti-S IgG with high titer (≥384 BAU/mL), with a significantly higher median anti-S IgG titer compared to unvaccinated HCWs with previous infection (384 vs. 140.1 BAU/mL; p = .0043).
Conclusions
Our study highlights the importance of implementing strict infection control policies among HCWs and deploying an effective COVID-19 vaccination strategy. More studies are needed in Lebanon to assess risk factors of SARS-CoV-2 exposure in the workplace.
Background
Since its emergence in December 2019, the COVID-19 pandemic rapidly spread across the globe causing more than 572,239,451 confirmed cases and 6,390,401 deaths as of July 29, 2022 (World Health Organization, 2022). In Lebanon, more than one million confirmed COVID-19 cases and 10,000 deaths have been reported since the first case was identified in February 2020 (World Health Organization, 2022).
The structure of the Lebanese healthcare system had a major impact on the national response to the COVID-19 pandemic (Khoury et al., 2020). The majority of healthcare facilities in Lebanon (84%) are owned and managed by the private sector with only 15% of hospital beds belonging to public hospitals (El-Jardali et al., 2020). Due to limited budget allocated to the public sector, most public hospitals are not well equipped, are understaffed, and are underfunded. These factors, along with the financial crisis that Lebanon has been facing since October 2019, exerted a heavy burden on healthcare facilities and hospital staff (World Health Organization, 2021). Despite national and international efforts to equip hospitals with beds and medical supplies, most hospitals in Lebanon suffered from a significant shortage in personal protective equipment (PPE) and medical supplies (Bou-Karroum et al., 2020; El-Jardali et al., 2020). The American University of Beirut Medical Center (AUBMC) was among the few Lebanese hospitals that had sufficient PPE and implemented strict infection control policies. HCWs have been at the frontline in the fight against this pandemic (Sabetian et al., 2021). According to the World Health Organization (WHO) and prior to the administration of the COVID-19 vaccines, 14% of the total reported COVID-19 cases were among HCWs (World Health Organization, 2020a) with 11-fold increased positive test rates among frontline HCWs compared to the general population (Nguyen et al., 2020). In an attempt to protect HCWs from COVID-19, hospitals imposed different policies, which included providing adequate PPE, frequent COVID-19 screening, and other infection prevention and control (IPC) measures (Al-Tawfiq et al., 2020; Barranco & Ventura, 2020). Several studies assessed adherence to PPE among HCWs during the COVID-19 pandemic. The former varied with shortage in PPE supply being the main factor contributing to lower adherence (Badran et al., 2021; El-Sokkary et al., 2021; Nasrabadi et al., 2021; Panayi et al., 2020). HCWs were identified as a high-priority group for COVID-19 vaccination by the WHO Strategic Advisory Group of Experts (SAGE) framework for the allocation and prioritization of COVID-19 vaccination and the Advisory Committee on Immunization Practices (ACIP) (Dooling et al., 2021; World Health Organization, 2020b). Similarly, HCWs were among the high-priority targeted groups in the national vaccination campaign in Lebanon; the latter started on February 14, 2021 (Ministry of Public Health, 2021a). The BNT162b2 mRNA COVID-19 vaccine, an mRNA vaccine encoding the SARS-CoV-2 full-length spike (S) protein (Polack et al., 2020), was the first administered vaccine in Lebanon.
Prior to the introduction of COVID-19 vaccines (January 1, 2020, to December 31, 2020), a meta-analysis including 49 studies (127,480 HCWs) reported an estimated overall seroprevalence of SARS-CoV-2 antibodies among HCWs of 8.7% (Galanis et al., 2021). SARS-CoV-2 seropositivity among HCWs was 10-fold higher compared to national seroprevalence (Amer et al., 2022). In Lebanon and prior to the introduction of COVID-19 vaccines, a nationwide seroprevalence study conducted between December 2020 and January 2021 estimated an overall seroprevalence of SARS-CoV-2 antibodies at 18.5% in the general population (Hoballah et al., 2022).
To our knowledge, current data on SARS-CoV-2 seroprevalence among HCWs in Lebanon are limited. Assessing seroprevalence of SARS-CoV-2 antibodies among HCWs is important to better estimate the cumulative incidence of SARS-CoV-2 infection and thus improve IPC measures. Our study aimed to investigate the prevalence of anti-SARS-CoV-2 antibodies in a cohort of HCWs as well as risk factors associated with exposure to SARS-CoV-2.
Methods
Study Design, Population, and Data Collection
We conducted a cross-sectional study between March 2021 and May 2021 among HCWs at AUBMC; the latter hosts approximately 3,100 HCWs. The study protocol was approved by the Institutional Review Board (IRB) at the American University of Beirut (AUB). Flyers and posters were distributed throughout AUBMC to recruit voluntary participants. Written informed consent was obtained from each participant. The questionnaire completed by the study participants was based on previous tools and adapted according to the aims of the study (Sakr et al., 2022). The questionnaire included the following sections: demographic characteristics, polymerase chain reaction (PCR) test results, occupational and community-related exposure to SARS-CoV-2, work history, PPE training and use, self-reported past medical history, and COVID-19 vaccination history. We followed the U.S. Centers for Disease Control and Prevention (CDC) public health guidance for community-related exposure, which defines the latter as any close contact with confirmed or suspected COVID-19 case within 1.8 meters (6 feet) for ≥15 minutes (CDC, 2021).
ELISA
Whole blood was collected for isolation of sera from participating HCWs. SARS-CoV-2-specific IgG antibodies against SARS-CoV-2 spike (S) protein were quantified using an anti-SARS-CoV-2-QuantiVac ELISA (IgG) (Euroimmun, Lübeck, Germany) according to the manufacturer’s instructions. Results were interpreted in Binding Antibody Units (BAU/mL) as follows: <25.6 negative, ≥25.6 to <35.2 borderline and ≥35.2 positive. To assess previous exposure to SARS-CoV-2 among vaccinated and unvaccinated HCWs, we also tested IgG against SARS-CoV-2 nucleocapsid protein (NCP) using anti-SARS-CoV-2-NCP ELISA (IgG) (Euroimmun, Lübeck, Germany) according to the manufacturer’s instructions. Anti-NCP IgG is only induced after natural infection but not after receiving the BNT162b2 mRNA COVID-19 vaccine and can be used as a biomarker of natural exposure to SARS-CoV-2 (Assis et al., 2021). IgG levels were calculated as ratios defined as the absorption of the patient’s sample divided by the absorption of the calibrator. Ratios <0.8 were negative, ≥0.8 to <1.1 were borderline, and ≥1.1 were positive. All samples in both ELISA assays were run in duplicates.
Statistical Analysis
Statistical analysis was performed using STATA SE 13. Descriptive statistics were calculated for all study variables. Means, ranges, and standard deviations were reported for continuous variables, while counts and frequencies were reported for categorical variables. Fisher’s exact test was used to assess the association between job categories (medical doctors, nurses, technicians, and others) and exposure factors. Mann–Whitney U test was used to compare the levels of anti-S IgG between vaccinated and unvaccinated study participants as well as between those with previous SARS-CoV-2 infection. A bivariate analysis was done to evaluate the association of RT-PCR test result as the dependent variable with exposure factors using Fisher’s exact test. We also performed a multivariate linear regression for each of the anti-S and the anti-NCP IgG using the following variables: COVID-19 vaccination, previous infection, and occupational exposure to SARS-CoV-2; selection of independent variables included in the model was based on statistical significance. A multicollinearity check was performed to check the correlation between independent variables used in the multivariate model. Missing data were not included in the analysis. The level of statistical significance was set at p < .05.
Results
Characteristics of Study Participants
A total of 92 HCWs participated in this study out of 3,100 (3% response rate). The low response rate could be attributed to the method of recruitment as well as the workload facing HCWs at the time. The majority of study participants were 25 to 45 years old (79.5%) and females (69.7%) (Table 1). Medical doctors and nurses constituted 58% of study participants, whereas 6.8% were technicians (laboratory technicians and phlebotomists), and the remaining were distributed between clerks, administrative, and others. The vast majority (75%) did not report any pre-existing medical condition. Twenty HCWs (28.6%) tested positive for SARS-CoV-2 via PCR. Approximately, 80% of participants were fully vaccinated against COVID-19 (i.e., received two doses of the BNT162b2 mRNA vaccine) at the time of participation. Among the vaccinated, 88.1% received their second dose ≥14 days before participating in this study.
Demographic Characteristics, Training, and Adherence to PPE Among Study Participants (n = 92)
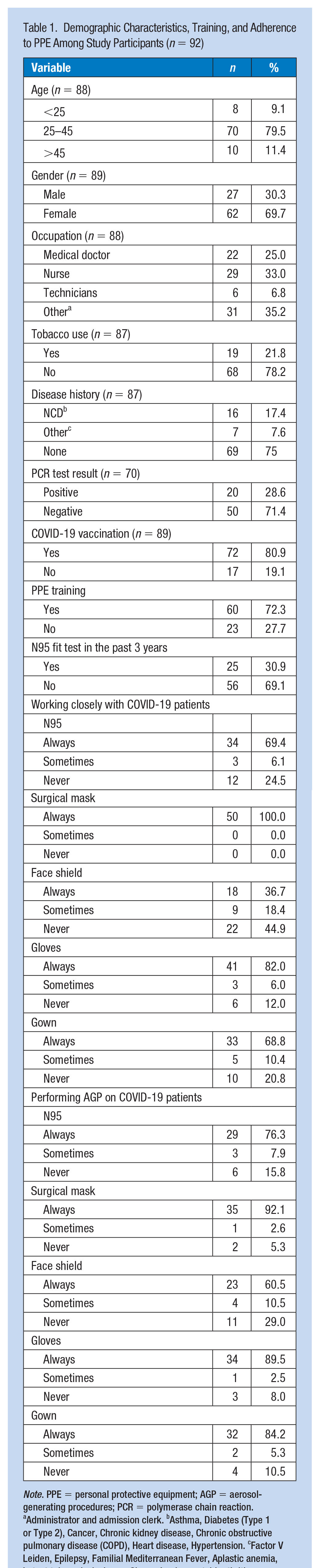
Note. PPE = personal protective equipment; AGP = aerosol-generating procedures; PCR = polymerase chain reaction.
Administrator and admission clerk. bAsthma, Diabetes (Type 1 or Type 2), Cancer, Chronic kidney disease, Chronic obstructive pulmonary disease (COPD), Heart disease, Hypertension. cFactor V Leiden, Epilepsy, Familial Mediterranean Fever, Aplastic anemia, Latent tuberculosis, lupus, Sjogren’s, rheumatoid arthritis.
Adherence to PPE
Our data showed that most of our participants (72.3%) received PPE training, while only 30.9% underwent N95 fit testing in the past 3 years (Table 1). All participants reported adherence to face masks when in direct COVID-19 patient care, and the majority reported adherence to the use of gloves (82%), N95 respirators (69.4%), and gowns (68.8%) (Table 1). More than 90% were always adherent to using a surgical mask while performing aerosol-generating procedures (AGPs) on COVID-19 patients, followed by 89.5%, 84.2%, 76.3%, and 60.5% of participants who were always using gloves, gowns, N95 masks, and face shields, respectively (Table 1). We did not collect data on HCWs solely performing AGPs; thus, we were not able to compare adherence to PPE between the two groups. Our data did not reveal any significant difference between vaccinated and unvaccinated HCWs and between participants with and without previous SARS-CoV-2 infection in relation to PPE adherence (data not shown).
Risk of Exposure to SARS-CoV-2 Among HCWs
We next assessed the risk of exposure to SARS-CoV-2 among HCWs by occupation. We divided the latter into four groups based on the risk of exposure: medical doctors, nurses and laboratory/radiology technicians (i.e., high-risk and involvement in direct patient care), and others; the latter includes administrators and admission clerks (i.e., low risk and no direct patient care involvement) (Table 2). Our data revealed a significant difference between the following exposure variables: working with a suspected or confirmed COVID-19 cases (p<.001), time spent with patients in the Emergency Department (ED) (p = .006), time spent in Intensive Care Unit (ICU) with COVID-19 patients (p = .039), and frequency of performing a medical procedure on COVID-19 patients (p = .014) and the occupation categories (medical doctors, nurses, technicians, and others). The majority of participating nurses (96.2%) and all medical doctors (100.0%) worked with suspected or confirmed COVID-19 cases. Our results showed that nurses spent more time with patients in the ED and the ICU compared to other categories of HCWs. Moreover, more than 50% of nurses reported frequently performing medical procedures (e.g., physical exam, blood withdrawal) on COVID-19 patients compared to 19% of medical doctors, and none among other occupations. Importantly, the results of the bivariate analysis revealed that none of the exposure variables (inside and outside the workplace) were significantly associated with SARS-CoV-2 infection in our cohort (Table 3).
Exposure of HCWs to SARS-CoV-2 by Occupation
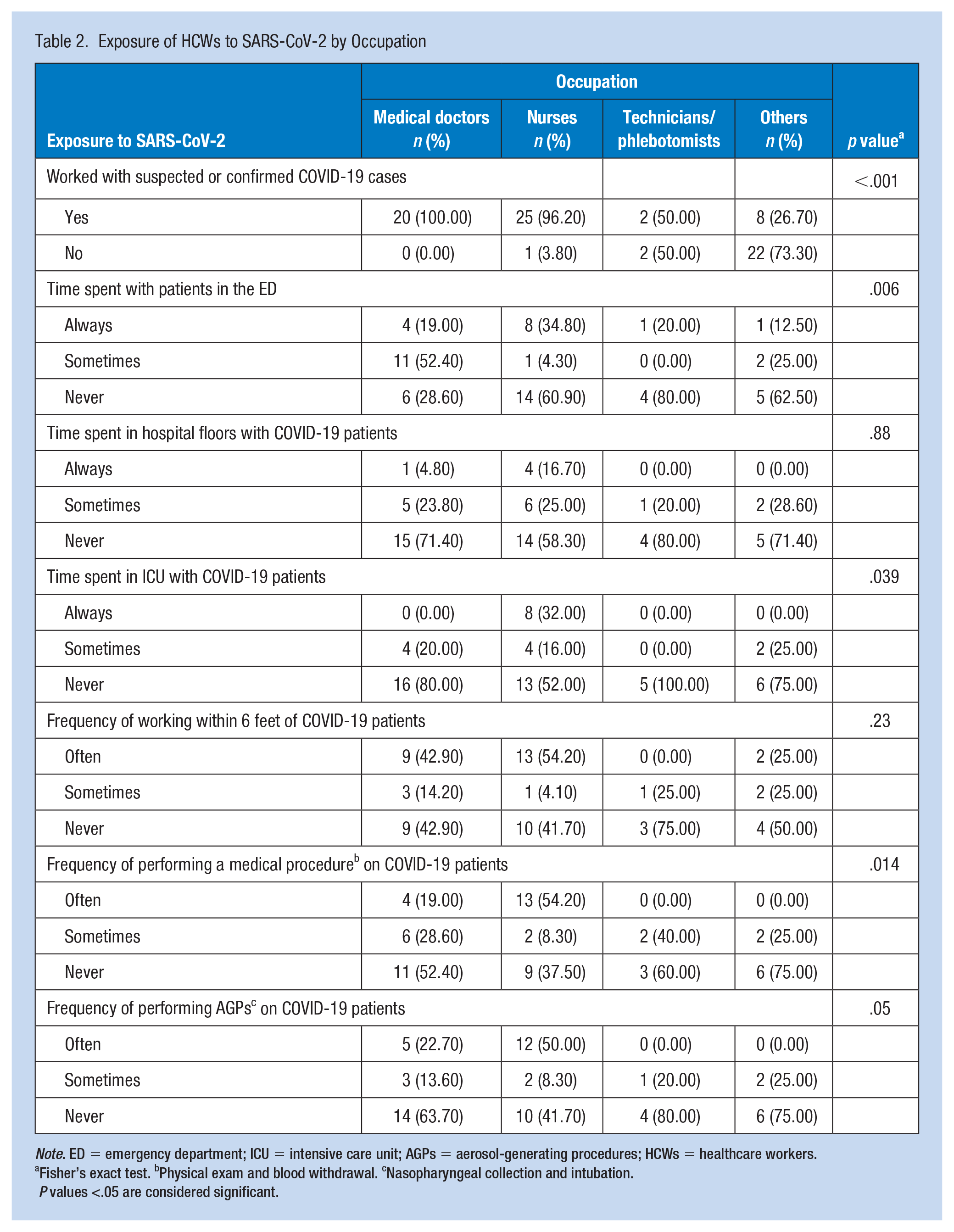
Note. ED = emergency department; ICU = intensive care unit; AGPs = aerosol-generating procedures; HCWs = healthcare workers.
Fisher’s exact test. bPhysical exam and blood withdrawal. cNasopharyngeal collection and intubation.
P values <.05 are considered significant.
Association Between SARS-CoV-2 Positivity Rates Among HCWs and Exposure Inside and Outside the Workplace
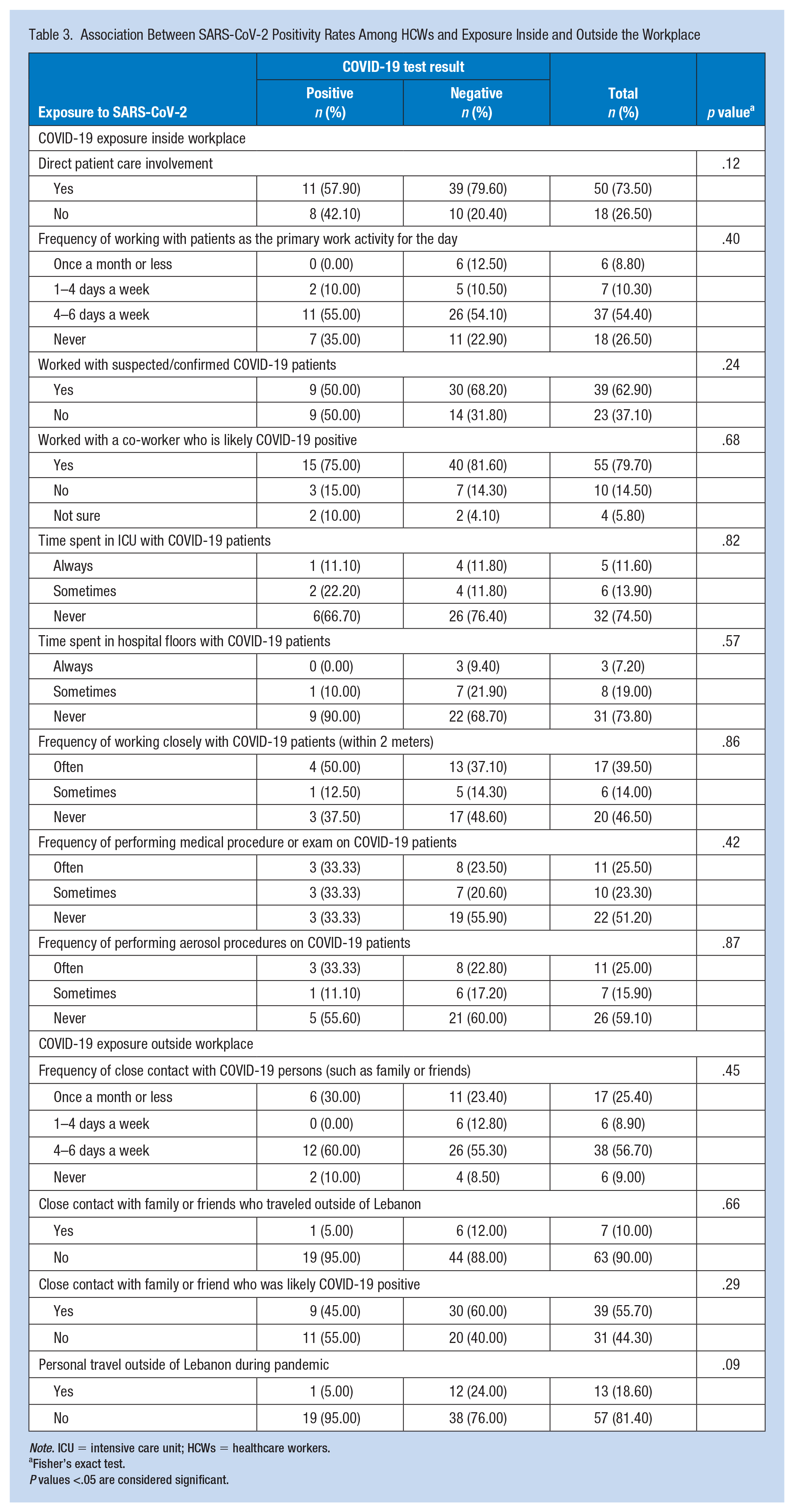
Note. ICU = intensive care unit; HCWs = healthcare workers.
Fisher’s exact test.P values <.05 are considered significant.
Anti-S and Anti-NCP SARS-CoV-2 IgG
To assess previous exposure to SARS-CoV-2 among vaccinated and unvaccinated HCWs, we determined anti-S IgG and anti-NCP IgG in sera of study participants. As expected, all vaccinated participants were seropositive for anti-S SARS-CoV-2 IgG (≥35.2 BAU/mL) compared to 58.8% of the unvaccinated (p<.001) (Table 4). The majority of our vaccinated participants (89.2%) tested negative for anti-NCP IgG compared to 64.7% of the unvaccinated (p = .023). Among the vaccinated group, 10.7% had positive or borderline (9.2% and 1.5% respectively) result for anti-SARS-CoV-2 NCP IgG, confirming a previous infection. The vast majority of the former (85.7%) reported to have been in a close contact (within 6 feet) with a positive COVID-19 case (family member or a friend) and 71.4% reported having experienced COVID-19-like symptoms in the past 2 months (data not shown); thus supporting the results of the anti-NCP assay indicating previous infection. Among unvaccinated HCWs with borderline (n = 1; 5.9%) or positive (n = 10; 58.8%) anti-S IgG, six HCWs tested positive for anti-NCP IgG, confirming a previous COVID-19 infection (Table 4).
Anti-SARS-CoV-2 S1 IgG and Anti-SARS-CoV-2 NCP IgG Among Vaccinated and Non-Vaccinated HCWs
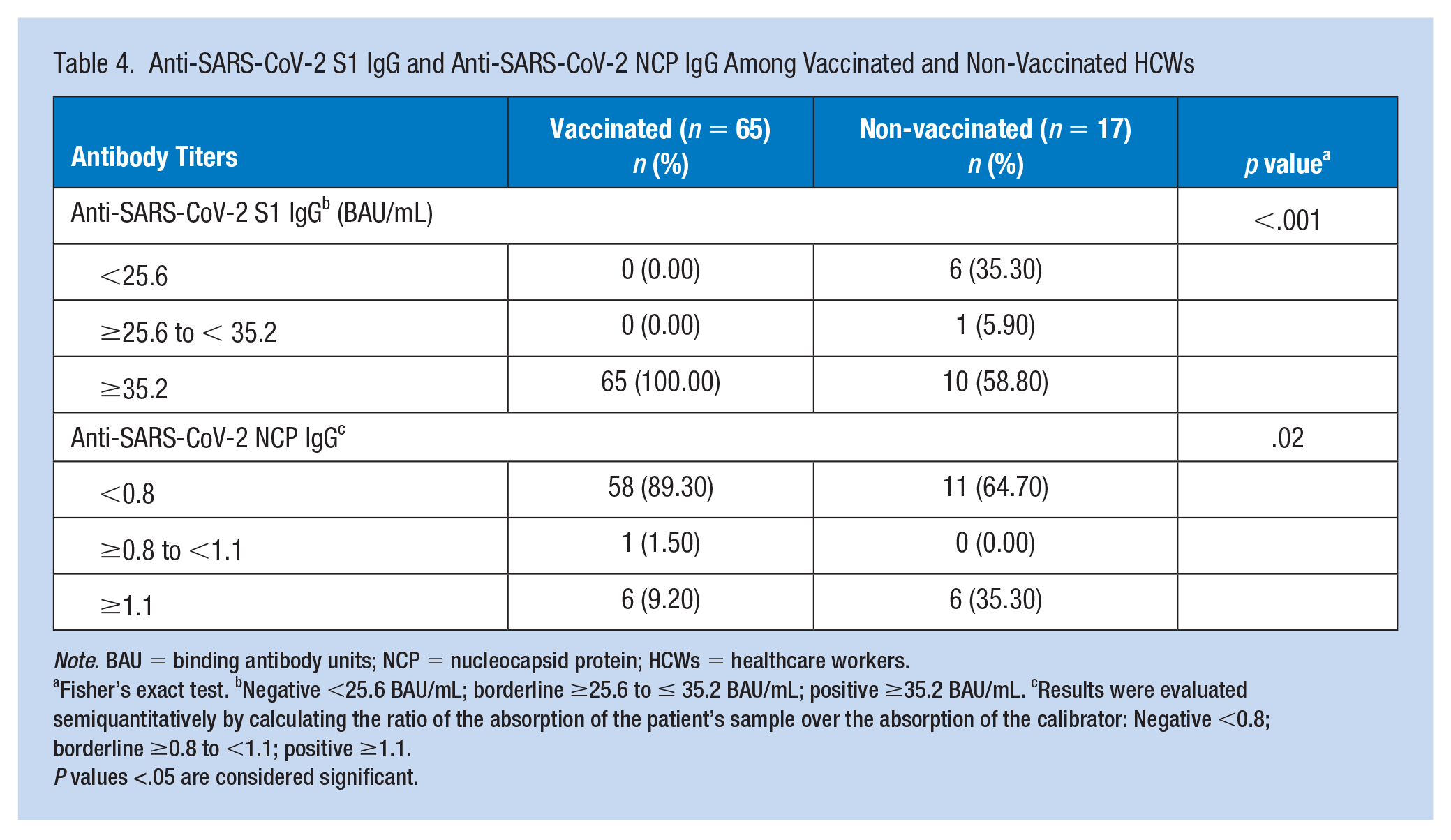
Note. BAU = binding antibody units; NCP = nucleocapsid protein; HCWs = healthcare workers.
Fisher’s exact test. bNegative <25.6 BAU/mL; borderline ≥25.6 to ≤ 35.2 BAU/mL; positive ≥35.2 BAU/mL. cResults were evaluated semiquantitatively by calculating the ratio of the absorption of the patient’s sample over the absorption of the calibrator: Negative <0.8; borderline ≥0.8 to <1.1; positive ≥1.1.
P values <.05 are considered significant.
We then assessed anti-S IgG titers among vaccinated and unvaccinated HCWs with and without previous SARS-CoV-2 infection using Mann–Whitney U test (Figure 1). As expected, unvaccinated HCWs with no previous infection had negative anti-S IgG titer. Importantly, vaccinated HCWs with or without previous infection had significantly higher median anti-S IgG titer compared to unvaccinated HCWs with previous infection (384 vs. 140.1 BAU/mL; p = .0043). These results indicated that HCWs in our study who received two doses of the BNT162b2 mRNA vaccine irrespective of previous SARS-CoV-2 infection have significantly higher anti-S IgG levels compared to unvaccinated HCWs with previous infection.
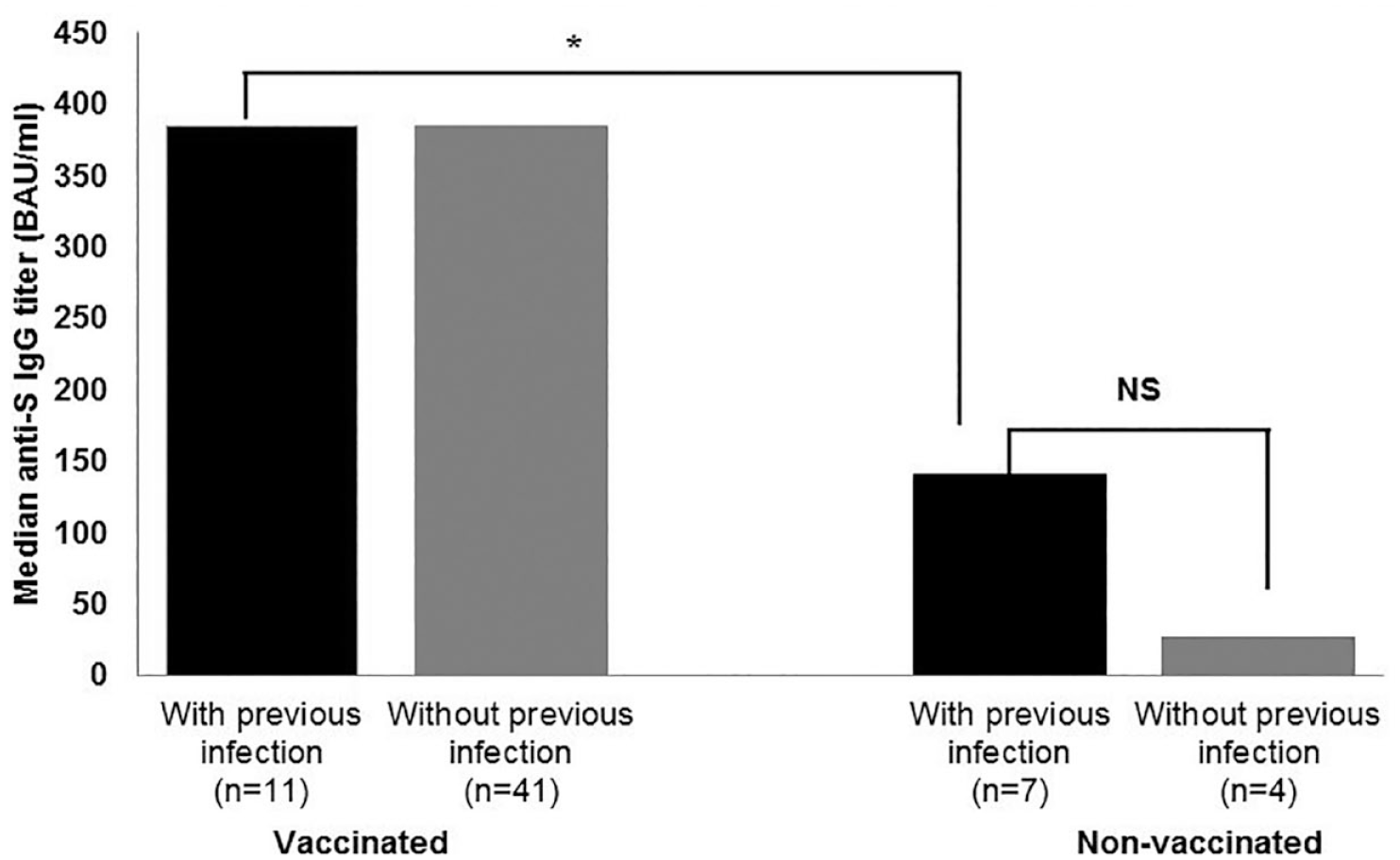
Anti-SARS-CoV-2 Spike IgG Titer in Among Vaccinated and Non-Vaccinated HCWs.
We also performed a multivariate linear regression for each of the anti-NCP and anti-S IgG while adjusting for the following variables: COVID-19 vaccination, previous infection, and significant occupational exposure variables (working with suspected or confirmed COVID-19 cases, time spent in the ED, time spent in the ICU with COVID-19 patients, and frequency of performing medical procedures on COVID-19 patients) (Table 5). Our results showed that there was a positive correlation between anti-NCP IgG levels and previous COVID-19 infection, close contact with COVID-19 cases, time spent in the ICU with COVID-19 patients, and performing medical procedures on COVID-19 patients. However, a negative correlation between anti-NCP IgG levels and COVID-19 vaccination and the time spent in the ED was detected. In addition, we detected a significant positive correlation between anti-S IgG and COVID-19 vaccination (p value < .001) as well as anti-S IgG and time spent in the ICU with COVID-19 patients and performing medical procedures on COVID-19 patients.
Multivariate Linear Regression and Multicollinearity Test for Anti-SARS-CoV-2 S1 IgG and Anti-SARS-CoV-2 NCP IgG Levels Among HCWs
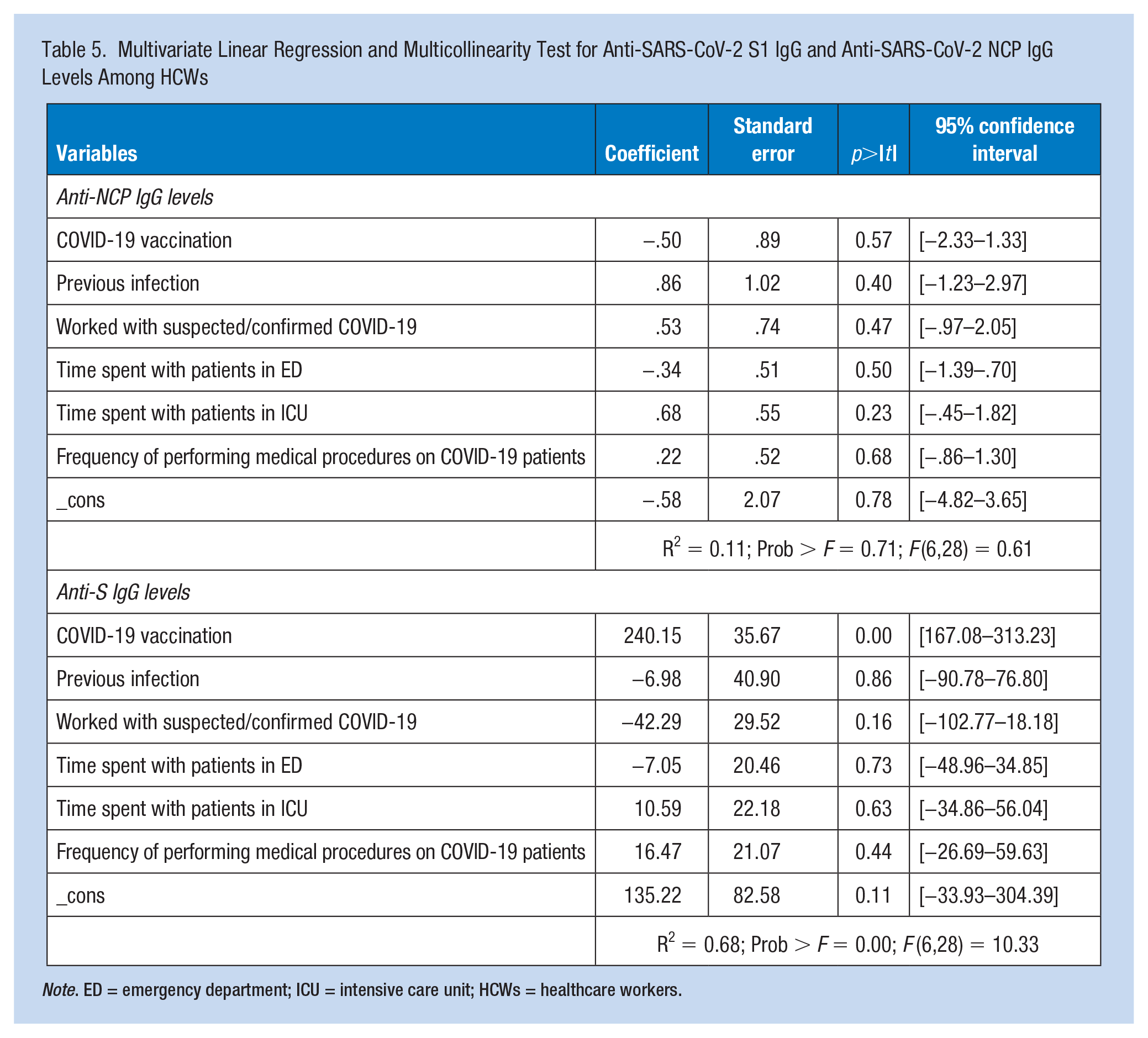
Note. ED = emergency department; ICU = intensive care unit; HCWs = healthcare workers.
Discussion
Our results showed that the vast majority of HCWs were highly compliant with and adherent to using PPE while caring for COVID-19 patients and performing aerosol procedures. Although HCWs are at significant risk of SARS-CoV-2 infection, the use of PPE and infection control training are associated with decreased risk of infection (Chou et al., 2020). The high level of PPE adherence among HCWs may be attributable to the ability of AUBMC to secure enough quantities of PPEs in times of national shortage and the continuous training of AUBMC staff on infection control measures. Our results are consistent with previous reports from the region (Alajmi et al., 2020; Al Marzouqi et al., 2023; Elshaer & Agage, 2022; Nasrabadi et al., 2021; Zangoue et al., 2021). Our results are also in agreement with previous studies reporting that working in a high-risk versus general department, suboptimal handwashing before or after patient contact, longer working hours, improper PPE use, and having a family member diagnosed with COVID-19 were associated with increased risk of SARS-CoV-2 infections among HCWs (Chou et al., 2020).
While the Occupational Safety and Health Administration (OSHA) in the US requires healthcare facilities to maintain a respiratory protection program that includes annual fit testing for respirators before being used in the workplace (D’Alessandro et al., 2020), fit testing during pandemics has several barriers. The latter is related to shortages in times of high demand, of N-95 masks and fit test kits, as well as time constraints (D’Alessandro et al., 2020). Although only 30.9% of the study participants reported being fit tested, HCWs at AUBMC performed N-95 seal check by self-assessment in place, as recommended by the CDC to achieve the best respirator fit during crisis (D’Alessandro et al., 2020). This mitigated the risk of exposure at the workplace and decreased SARS-CoV-2 transmission rates among HCWs. When performing AGP, most of our participants reported wearing a respirator (i.e., N95) or face masks. Compliance with wearing a face mask or respirators during AGP is critical to significantly reduce the risk of SARS-CoV-2 transmission (Fawcett et al., 2023). Although wearing eye protection is recommended during AGP, the relative risk of transmission through the ocular route is thought to be low (Barnett et al., 2020; Fawcett et al., 2023).
Nurses were at higher risk of exposure compared to medical doctors and technicians; this is also reflected by the results showing that nurses spent more time with patients in the ED and the ICU, and performed more medical procedures and AGPs compared to medical doctors, technicians, and others. This finding contradicted with the results of a recent meta-analysis indicating that physicians were at higher risk of SARS-CoV-2 exposure compared to nurses (Gholami et al., 2021). This might be explained by the fact that nurses spend more time caring for COVID-19 patients in the COVID-19 unit, the ICU and the ED compared to physicians. Moreover, nurses are closely involved in performing medical procedures and AGPs on patients.
Our study reported SARS-CoV-2 infection in 27.8% of HCWs who performed a PCR test between July 2020 and April 2021. This result is similar to what has been previously reported among this population, whereby a third of the workforce got infected between the beginning of the pandemic in February 2020 and the start of the vaccination campaign in February 2021 (Sakr et al., 2022). Exposure assessments, testing recommendations, as well as periods of isolations and quarantine were based on the CDC guidelines issued for HCWs and were handled by the Employee Health Unit staff. During the same period of the study, the average positivity rate per month among the general population ranged between 1.53% and 20.07% (Abou Hassan et al., 2023). The infection rate in our study population is also relatively high compared to other studies in the region where the reported percentages were 7.4% in Riyadh city (Alroqi et al., 2021), 13.5% in Egypt (Al Maskari et al., 2021), and 21.2% in Oman (Kassem et al., 2020). The high infection percentages reported in this study may be attributable to the fact that Lebanon was facing a COVID-19 surge at the beginning of the year 2021, during which 1,000 to 6,000 new COVID-19 cases were reported daily until the month of April (Abou Hassan et al., 2023; Ministry of Public Health, 2021b).
Overall, no significant association between workplace or individual exposure and SARS-CoV-2 infection was found. However, a systematic review assessing the seroprevalence of SARS-CoV-2 antibodies and its associated factors in HCWs reported that workplace factors (working in a COVID-19 unit, patient-related work, frontline HCWs, healthcare assistants, shortage of PPE, self-reported belief of previous COVID-19 infection, previous PCR test) and household contact with suspected or confirmed cases of COVID-19 are all factors significantly associated with seropositivity (Galanis et al., 2021). The absence of this correlation in this study may be explained by the fact that the majority of our participants were highly compliant to all precautionary measures against COVID-19 inside and outside the hospital. This reduces the exposure risk inside the workplace, and consequently decreases the possibility of acquiring or spreading the infection. In addition, our small sample size might have added to the lack of correlation.
Our results showed that all vaccinated HCWs were seropositive for anti-S IgG with high titer (≥384 BAU/mL) with positive correlation between anti-S IgG levels and COVID-19 vaccination. This was expected since all vaccinated individuals received the BNT162b2 mRNA vaccine which encodes for the SARS-CoV-2 full-length S protein (Polack et al., 2020). Anti-NCP IgG was also detected in 10.7% of vaccinated individuals, who had been therefore previously infected with SARS-CoV-2. This was confirmed by the positive correlation between anti-NCP IgG and previous infection. We also observed significantly higher anti-S IgG titers among vaccinated individuals with or without previous infection compared to unvaccinated individuals with previous infection. The latter was in agreement with previously published data (Assis et al., 2021; Forgacs et al., 2021; Urlaub et al., 2021). Among unvaccinated participants with previously confirmed SARS-CoV-2 infection, the majority (6/7; 85.7%) were seropositive for anti-S IgG. This was in accordance with other studies reporting seropositivity of 91-100% among adults with previously confirmed SARS-CoV-2 by RT-PCR (Gudbjartsson et al., 2020; Long et al., 2020; Wajnberg et al., 2020). This study also showed that seropositivity for anti-NCP IgG did not coincide with the presence of anti-S IgG among unvaccinated HCWs with previous infection. This was in agreement with previous data reported among adults with confirmed SARS-CoV-2, showing a heterogeneous antibody response against the spike receptor binding domain (S-RBD) and NCP in addition to the lack of correlation between the detection of NCP binding antibodies and the presence of S-RBD neutralizing antibodies (Heffernan et al., 2021; McAndrews et al., 2020; Weidner et al., 2020).
Our results are hampered by several limitations. Our study is a cross-sectional study and recruitment started after the launch of the national COVID-19 vaccination. Consequently, we were unable to follow up participants and assess the durability of antibodies following natural infection and vaccination. Our study included a small sample of HCWs from a single healthcare facility in Lebanon; accordingly, our results cannot be generalized on all HCWs at AUBMC nor across other hospitals in Lebanon. This is especially true since AUBMC is a private university hospital and its characteristics likely differ from other private and public hospitals. Importantly, PPE adherence was self-reported rather than objectively assessed. This hampered our ability to adequately assess the adherence to IPC measures at the hospital level.
Conclusion
More studies including HCWs from several healthcare centers across the country are needed to assess SARS-CoV-2 seroprevalence and PPE adherence in this high-risk population. The use of PPE drastically reduces the risk of COVID-19 and should inform future recommendations to ensure stockpile of PPEs as well as adequate training to prevent occupational risk of exposure and consistent compliance during emergencies. Longitudinal studies on vaccine effectiveness and breakthrough infections among this high-risk group are needed in Lebanon to complement relevant compliance practices for occupational safety.
Applying Research to Occupational Health Practice
Our study investigated the prevalence of anti-SARS-CoV-2 antibodies and assessed the risk of exposure to SARS-CoV-2 in a cohort of HCWs in a tertiary healthcare facility in Lebanon. Our results showed that most HCWs were adherent to PPEs. Nurses were at higher risk of exposure to SARS-CoV-2 compared to other categories of HCWs (i.e. physicians, technicians). This is aligned with nurses reporting spending more time with patients in the ED and ICU as well as performing more clinical procedures. As expected, anti-S IgG titers were significantly higher among vaccinated participants; previous infection is suggested among unvaccinated HCWs with high titers of anti-S IgG. While anti-NCP IgG antibodies were detected among vaccinated (10%) and unvaccinated individuals (35%), these seropositivity rates did not coincide with the presence of anti-S IgG among unvaccinated HCWs with previous infection.
These results suggest the difference in detected antibodies following natural infection. Our findings advance the significance of the implementation of infection, prevention and control measures in healthcare settings specifically during public health emergencies in order to control viral spread. More research is needed in order to assess the ability of serological assays to differentiate anti-SARS-CoV-2 antibodies following vaccination or natural infection in order to support rapid clinical diagnosis.
Footnotes
Acknowledgements
We thank all HCWs for their participation.
Author Contributions
CJS participated in the study design; designed the exposure questionnaire, oversaw data collection, participated in data analyses, and edited the manuscript; FFAH performed laboratory experiments, data analysis, and wrote the first draft of the manuscript; LF performed data collection; MBH performed laboratory experiments, data analysis, and contributed to writing; SA performed data analysis and contributed to manuscript writing; DR participated in designing the exposure questionnaire, study analysis, and edited the manuscript; NMM designed the study, oversaw all aspects of the study, edited, and finalized the manuscript. CJS and FFAH equally contributed to the manuscript.
All authors reviewed, edited, and approved the final manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Lebanese National Council for Scientific Research (Award A103936).
Human Subjects Review
The study protocol was approved by the Institutional Review Board (IRB) at the American University of Beirut (AUB) (IRB ID: BIO-2020-0374; Date: December 21, 2020).