
Abstract
Background:
Healthcare workers (HCWs) have shown increased adherence to infection control practices during the COVID-19 pandemic. However, there is a need to assess their adherence to and attitude toward COVID-19 guidelines after being vaccinated. The purpose of this pilot study is to assess the adherence to and attitudes toward the adherence to COVID-19 guidelines among HCWs who have been vaccinated.
Methods:
A retrospective cross-sectional design was employed. One hundred and eight participants were recruited via email from a medical center in the Midwest United States. The participants completed online surveys measuring the level of adherence to and attitudes toward the adherence to COVID-19 guidelines. The response rate was 5.4%.
Findings:
Most participants were female (73.1%) and white (82.4%). The participants adhered to COVID-19 guidelines 79.7% of the time. The most frequently followed guidelines were performing hand hygiene, wearing a respirator or well-fitting mask in areas where patients may be present, and wearing eye protection when entering the room for a patient with suspected or confirmed COVID-19 infection. The least performed precautions were performing COVID-19 testing after exposure to a suspected or confirmed COVID-19 case and maintaining social distancing. There was a significant decrease in the perceived importance of adherence to COVID-19 precautions post-vaccination (p <.001, 95% CI [−0.78, −0.35]).
Conclusions:
The increased perception of safety after receiving COVID-19 vaccination may negatively influence HCWs’ adherence to COVID-19 precautionary guidelines. Continuous education and monitoring of HCWs’ safety practices are important to influence HCWs’ attitudes to adhere to COVID-19 precautions, particularly after vaccination.
Background
Healthcare workers (HCWs) were at higher risk of being infected with SARS-CoV-2 virus and experiencing the consequences of the disease compared with the general population (Zakeri et al., 2021; Zheng et al., 2020). Between February and April 2020, the number of COVID-19 cases in the United States that were reported to the Centers for Disease Control and Prevention (CDC) was 315,531. Data related to occupation were reported for 49,370 cases (16%). Of those, 9,282 (19%) were HCWs (CDC COVID Response Team, 2020). The increased patient burden, personal protective equipment (PPE) shortage, and inability to maintain a safe distance from patients while providing care contributed to the high rate of infection among HCWs (Barranco & Ventura, 2020; Parmasad et al., 2021). Besides the health risks of COVID-19 on HCWs’ health, spreading COVID-19 infections among HCWs is costly to the whole healthcare system and results in decreasing HCWs’ productivity due to illness and time spent in quarantine (Yaghoubi et al., 2022). Furthermore, HCWs with asymptomatic COVID-19 placed their patients at risk of acquiring the infection (Alserehi et al., 2021). To ensure safety and protect the health of HCWs, the CDC published guidelines to prevent SARS-CoV-2 transmission among HCWs (CDC, 2021, 2022).
In December 2020, COVID-19 vaccinations became available to HCWs to provide protection against the infection (Dooling et al., 2021). Despite being vaccinated, the evolving state of the disease transmission continues to predispose even those who are vaccinated to acquiring the disease (Guedes et al., 2023). In fact, several surges of COVID-19 cases occurred globally and new variants that transmitted more rapidly than the original strain of the virus appeared in the period post-vaccination (Iftekhar et al., 2021). Thus, ensuring that HCWs remain adherent to all recommended guidelines after being fully vaccinated is important, especially in areas where COVID-19 virus transmission is high (CDC, 2021). However, the perceived sense of being protected against the virus following vaccination might result in decreasing adherence to COVID-19 guidelines among HCWs, which increases their risk for infection. It has been found that HCWs demonstrated a decreased level of adherence to COVID-19 protective practices after the first dose of COVID-19 vaccination compared to before taking the first dose of the vaccine (Zewude et al., 2021). Therefore, there is a need to assess HCWs’ adherence to COVID-19 guidelines and their attitudes toward guideline adherence, specifically after being fully vaccinated. The purpose of this pilot study is to assess the adherence to and attitudes toward the adherence to COVID-19 guidelines among HCWs who have been fully vaccinated. The specific aims are to (1) measure the level of adherence to COVID-19 precautionary guidelines among fully vaccinated HCWs post-vaccination and (2) examine if there is a significant difference in the attitudes toward adherence to COVID-19 precautionary guidelines among fully vaccinated HCWs before and after being fully vaccinated.
Methods
We implemented a cross-sectional design from one medical center. Online surveys were used to collect the data.
Participants were recruited from a large medical center in the Midwest United States, in which COVID-19 vaccines were required for all employees unless an exemption was provided for medical or religious reasons. COVID-19 policies at this medical center were based on CDC guidelines. The medical center is located in an area where COVID-19 transmission was high, as defined by the CDC during the data collection period in July 2022 (Sutherland, 2022). Inclusion criteria were being 18 years of age or older, having worked as an HCW for at least one year, providing direct care to patients (physicians, nurses, physiotherapists, respiratory therapists, etc.), having received the primary series of COVID-19 vaccinations, and having access to computer and the internet. The exclusion criterion was having a medical condition preventing or limiting the ability to use any COVID-19-related PPE.
To recruit participants, the administrators at the medical center were contacted and asked to forward the recruitment email to potential participants. The administrators in the participating institution sent out the recruitment email to all HCWs who provided services and direct care to patients (approximately 2000 HCWs). The study email contained the study title, the institutional review board (IRB) study number, study purpose, inclusion and exclusion criteria, and link to the study surveys. REDCap (Research Electronic Data Capture), a secure online software (Harris et al., 2009, 2019), was used to design and distribute the questionnaires and collect participant responses. After reaching the required sample size, the surveys were closed in REDCap. Each participant was paid a $15 e-gift card as compensation for the time spent completing the surveys.
Measures
Participants completed a demographic questionnaire. The demographic questionnaire collected information regarding age, race (African American, Asian, Native Hawaiian, White, and other), gender (female, male, and other), level of education (Diploma, Associate degree, Bachelor’s degree, Master’s degree, post-Master’s degree or certification), number of years of nursing experience, average hours worked per week, whether the HCW takes care of COVID-19 patients, type of COVID-19 vaccine received (Pfizer-BioNTech, Moderna, Johnson & Johnson’s Janssen), number of COVID-19 vaccine doses received, number of months from the date when the last dose of COVID-19 vaccine was received, and reason for receiving COVID-19 vaccine (to protect self against the infection or voluntarily, required by the current employer, other).
Adherence to COVID-19 precautionary guidelines was measured using the 18-item Adherence to COVID-19 Precautionary Guidelines Questionnaire, an investigator-developed instrument. The items in this instrument reflected COVID-19 precautionary behaviors based on the recommended guidelines by CDC for HCWs (CDC, 2021, 2022). The responses were measured using a 5-point Likert-type scale reflecting the percentage of the time HCWs adhered to each behavior (Never, 1–25%, 26–50%, 51–75%, 76–99%, and Always). This response scale was used in a similar instrument that measures nurses’ adherence to chemotherapy handling precaution guidelines (Polovich & Clark, 2012).
The attitudes toward adherence to COVID-19 precautionary guidelines were measured using the Attitudes toward the Adherence to COVID-19 Precautionary Guidelines Questionnaire, an investigator-developed instrument. This questionnaire contains two items. It measures the level of the perceived importance of adherence to COVID-19 guidelines before and after receiving COVID-19 vaccines. The response scale ranged from 0–10, where a higher score indicates an increased level of the perceived importance of following COVID-19 guidelines.
Assessing the Content Validity of the Study Instruments
The investigator-developed instruments (Adherence to COVID-19 Precautionary Guidelines Questionnaire and Attitude toward the Adherence to COVID-19 Precautionary Guidelines Questionnaire) were sent to experts for content validation. Three experts (two PhD-prepared researchers in occupational health and a clinician specializing in occupational health holding a Master’s degree) were contacted to review the questionnaires’ item content. An email was sent to the experts containing the questionnaires and instructions on how to assess content validity. The content validity for each item was rated on a relevance scale from 1 to 4; where 1: not relevant, 2: unable to judge the relevance of the item without revision, 3: relevant, needs minor modifications, and 4: very relevant and succinct (Lynn, 1986). The content validity index for each item was calculated by dividing the number of experts who rated the item as having 4 or 3 on the relevance scale over the total number of experts (Lynn, 1986; Polit & Beck, 2006). Moreover, the total scale content validity index was calculated by generating the mean of the content validity indices of the retained items (Polit & Beck, 2006). The minimum required content validity index for each item and the whole scale is 0.83 (Lynn, 1986). Further, the experts were asked to provide feedback on the comprehensiveness and wording of the items (Lynn, 1986).
Data Analysis
Sample Size Calculations
In a two-tailed t-test with a Cohen’s d effect size of 0.3 and alpha 0.05, we needed at least 90 HCWs to participate in this study to achieve a power of 80%. Sample size calculation was done using G Power 3.1.9.7 (Faul et al., 2009).
Statistical Analysis
The Statistical Package for Social Sciences (SPSS) version 27 (IBM Corp., 2020) was used to conduct the analysis. Missing value analysis revealed that the percentage of missing values in each variable was less than 10%. For Aim 1, we used descriptive statistics (frequency, mean, standard deviation, percent, and minimum and maximum values) to measure the level of HCWs’ adherence to COVID-19 precautionary guidelines. Pearson correlation was calculated to test the relationships between the adherence to the guidelines and the continuous demographic variables, while the independent t-test and ANOVA were used to test the relationships between the adherence to the guidelines and the categorical demographic variables. In addition, the Pearson correlation was used to test the relationship between adherence to the guidelines and the attitude toward adherence to the guidelines among HCWs. For Aim 2, a dependent sample t-test was computed to assess if there was a significant difference in the attitudes toward adherence to COVID-19 precautionary guidelines among fully vaccinated HCWs before and after being fully vaccinated (Field, 2018).
Ethical Considerations
The University of Cincinnati Institutional Review Board determined the study was exempt on March 17, 2022. In lieu of signed informed consent, participants were provided with a study information sheet before being directed to complete the electronic surveys. A waiver for consent documentation was granted, and completing the surveys indicated consent to participate.
Results
Content Validity
Based on the experts’ review, 13 of the 17 items in the Adherence to COVID-19 Precautionary Guidelines Questionnaire met the minimum level for content validity (0.83). The item content validity indices (I-CVIs) for the items ranged between 0.67 and 1.00. Four items that did not meet the minimum level of content validity (I-CVIs = 0.67) were kept because they reflected significant guidelines to prevent COVID-19 virus transmission. Several items were re-worded based on the experts’ feedback. One item that reflected the correct procedures to remove the PPE without cross-contamination was added. The final instrument contained 18 items with a total scale content validity index (S-CVI) = 0.92. Each item in the Attitudes toward the Adherence to COVID-19 Precautionary Guidelines Questionnaire had an I-CVI = 1.00, and an S-CVI = 1. Both items were re-worded per experts’ suggestions. No items were added to this instrument.
Sample Demographics
A total of 108 HCWs participated in this study with a calculated response rate of 5.4%. Seventy-nine participants (79%) were females, and 21 (21%) were males. The mean age of respondents was 41.8 (SD = 9.4) years. The majority were White (n = 89; 87.3%) and had post-Master’s degrees or certifications (n = 79; 76.7%). Overall, the average years of clinical experience was 15.5 years (SD = 9.6), and the mean number of hours worked per week was 41.3 hours (SD = 8.2).
Most participants (n = 82; 79.6%) received three doses of the COVID-19 vaccine, and the average number of months from the date when the last dose of the COVID-19 vaccine was received was 7.6 months (SD = 3.3). Eighteen participants (17.5%) reported that they received the Pfizer-BioNTsech vaccine, and 85 participants (82.5%) reported that they received the Moderna vaccine. The majority of the participants (n = 99; 96.1%) reported that they voluntarily received COVID-19 vaccine to protect themself against the infection. Seventy-six HCW participants (74.5%) provided direct care to COVID-19 patients. Table 1 presents the detailed demographic, work, and vaccination status variables of the study participants.
Demographic, Work, and Vaccination Status Variables of the Study Participants and the Relationship With Adherence to COVID-19 Guidelines (n = 108)
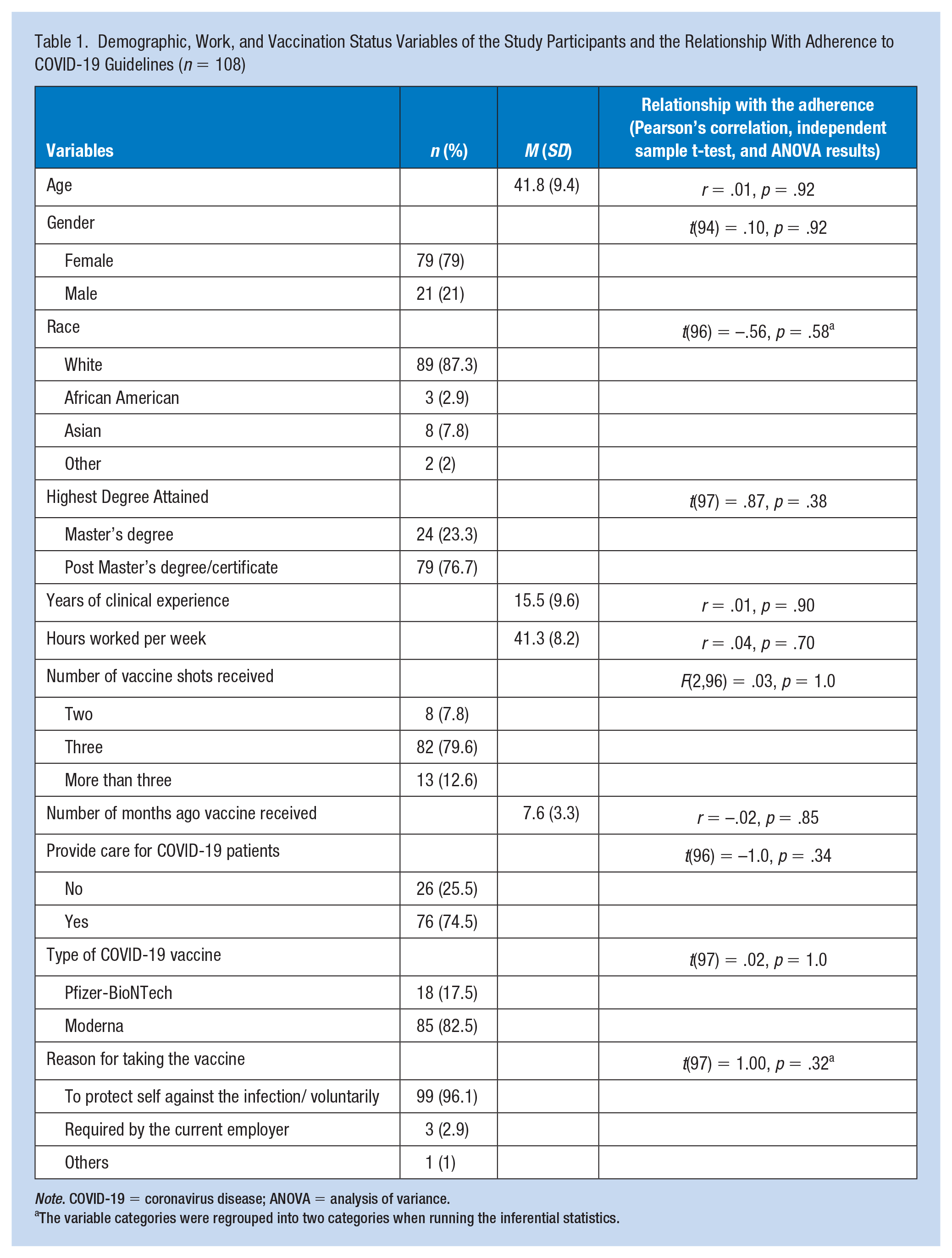
Note. COVID-19 = coronavirus disease; ANOVA = analysis of variance.
The variable categories were regrouped into two categories when running the inferential statistics.
Adherence to COVID-19 Guidelines
The participants reported the frequency of their adherence to COVID-19 guidelines in terms of the percentage of the time they adhered to each of the guidelines. In general, the participants adhered to COVID-19 guidelines 79.7% of the time (SD=11.6; range 46.7%–100%). The most frequently followed guideline was performing hand hygiene before and after entering a patient room (96% of the time), followed by wearing a respirator or well-fitting mask in areas where patients may be present (95.2% of the time) and wearing eye protection when entering the room for a patient with suspected or confirmed COVID-19 infection (94.6% of the time). The recommended guideline least performed by the participants was performing COVID-19 testing after 5 to 7 days of exposure if the first test was negative (44.8% of the time), followed by performing COVID-19 testing after 24 hours of exposure to a suspected or confirmed COVID-19 case (52% of the time) and maintaining social distancing with others when possible (61.4% of the time). In terms of the adherence to wearing PPE when entering a room for a patient with suspected or confirmed COVID-19 infection, PPE most frequently used to least frequently used were as follows: eye protection (e.g., face shield, eye goggles; 94.6% of the time), gloves (89.4% of the time), isolation gowns (86.6% of the time), and N95 mask or higher-level respirator (69.2% of the time). The internal consistency reliability for the scale was acceptable (Cronbach’s alpha = 0.79). The attitude toward adherence to COVID-19 guidelines was positively and significantly correlated with the percent of the time the participants adhered to COVID-19 precautionary guidelines (r = .39, p < .001). None of the demographic, work, and vaccination status variables were significantly associated with the percentage of the time the participants adhered to guidelines. Table 1 presents the results of the inferential statistics on the relationships between each of the demographic, work, and vaccination status variables and adherence to COVID-19 precautions. Table 2 represents the percentage of time the participants adhered to each of the COVID-19 precautionary guidelines.
Adherence to COVID-19 Precautionary Guidelines With the Guidelines Ranked From the Highest to the Lowest Level of Adherence to These Guidelines by HCWs
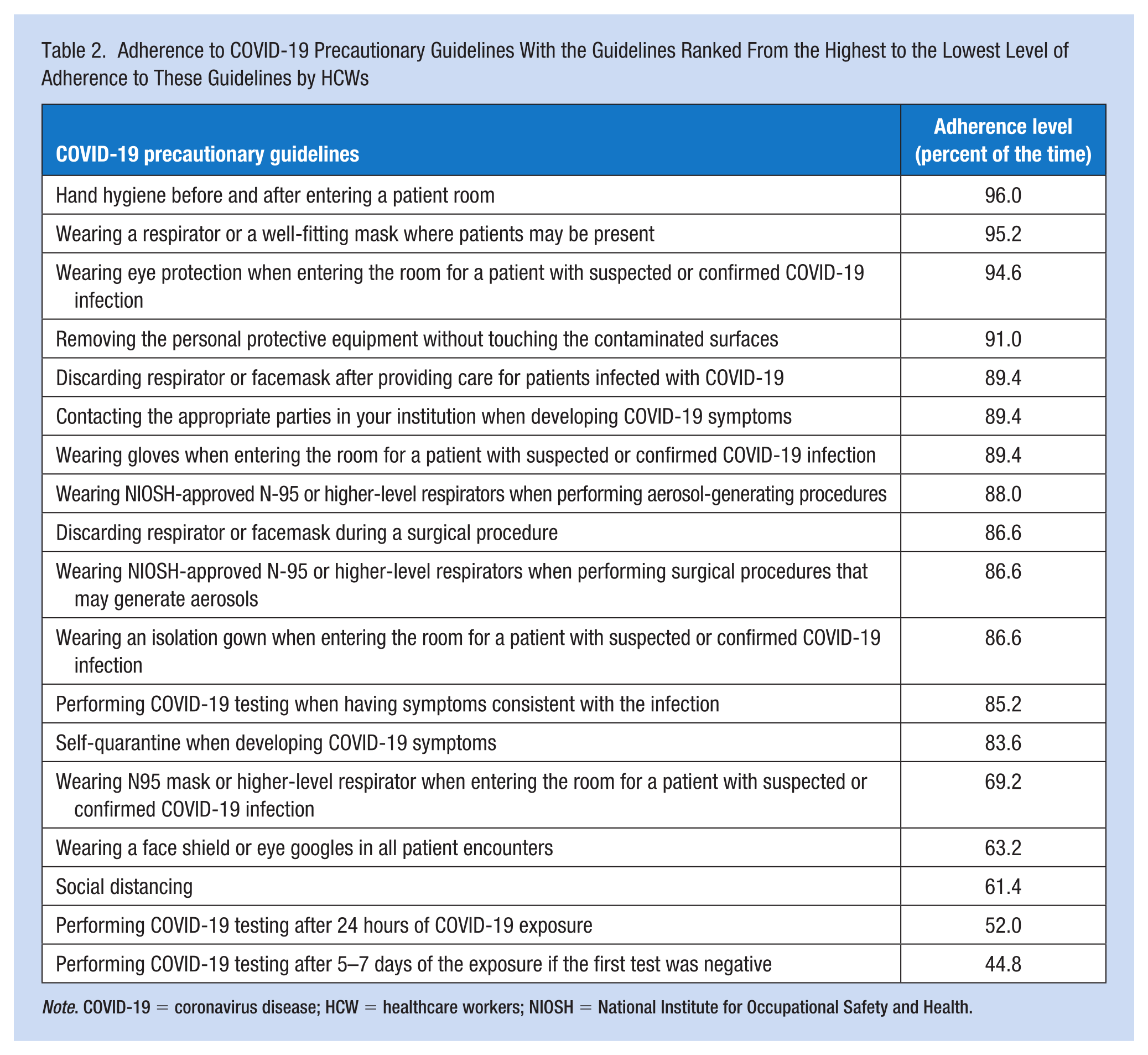
Note. COVID-19 = coronavirus disease; HCW = healthcare workers; NIOSH = National Institute for Occupational Safety and Health.
Attitudes Toward the Adherence to Guidelines Before and After COVID-19 Vaccination
Participants reported the level of perceived importance of adhering to COVID-19 precautionary guidelines before and after receiving COVID-19 vaccination. Out of 10, the average perceived level of importance to follow COVID-19 guidelines before vaccination was 9.77 (SD=0.6; range: 7–10), while the average perceived level of importance to follow COVID-19 guidelines after vaccination was 9.20 (SD=1.2; range: 3–10). There was a significant decrease in the perceived importance of adherence to COVID-19 precautionary guidelines after receiving COVID-19 vaccination, t(102) = −5.24, p < .001, 95% CI [−0.78, −0.35]. The effect size of Cohen’s d was −0.52.
Discussion
The results of this study indicate that the adherence to COVID-19 precautionary guidelines among HCWs post-vaccination is suboptimal. Also, the study results show that the perceived importance of adhering to the guidelines influences the actual adherence behaviors among HCWs. In addition, HCWs’ perceived importance of following COVID-19 precautionary guidelines after being vaccinated is significantly lower compared to before receiving COVID-19 vaccination.
HCWs’ adherence to COVID-19 precautionary guidelines was and still is essential to protect their health and prevent the transmission of the virus to others. Although previous studies show that HCWs’ adherence to infection control practices was improved during the pandemic (Albeladi et al., 2021; Nimer et al., 2021), the present study’s findings indicate that HCWs adherence to COVID-19 guidelines is lower than the recommended level. In addition, this study shows that HCWs adhere to some COVID-19 precautionary guidelines more than others. For example, in most instances, HCWs adhere to performing hand hygiene before and after entering a patient room, wearing a respirator or a well-fitting mask in areas where patients may be present, and wearing eye protection when entering the room for a patient with suspected or confirmed COVID-19 infection. These patterns of adherence behaviors are similar to that in Latif et al. (2022) study, where HCW participants indicated that they mostly adhere to wearing masks, washing hands before and after a patient encounter, and wearing PPE when caring for a patient with COVID-19.
On the contrary, the current study shows that performing COVID-19 testing after exposure to a suspected or confirmed case of COVID-19 and maintaining social distancing with others were the least performed COVID-19 preventive behaviors. In the medical center where this study was conducted, HCWs, at the time of the study, were required to perform COVID-19 testing after exposure to the COVID-19 virus if they experienced COVID-19 symptoms. This could interpret the low percentage of HCW respondents who performed COVID-19 tests after the exposure. In agreement with this study’s findings regarding the adherence to social distancing at work, Latif et al. (2022) study shows that maintaining social distancing with others was the least performed behavior among HCWs. The latter study did not assess the adherence to performing COVID-19 testing after exposure to a suspected or confirmed case of COVID-19. Previous studies identified barriers to adhering to social distancing among HCWs in clinical settings. Examples are the physical structure of the environment in clinical settings and the need to provide direct patient care, work within teams, protect patient confidentiality when communicating patient information, and sustain good relationships with co-workers (Hobbs et al., 2021; Keller et al., 2022) unlike the studies by Alhumaid et al. (2021) and Zewude et al. (2021), which indicate that there are relationships between HCWs’ demographic characteristics and the adherence to COVID-19 preventive behaviors, no relationships between HCWs’ demographic characteristics and adherence behaviors were found in this study.
This study demonstrates that HCWs do not adhere to using all PPE when encountering a patient with COVID-19 infection. This is supported by the findings from previous studies by Neuwirth et al. (2020) and Latif et al. (2022). Several factors affect the adherence to wearing PPE among HCWs during the pandemic such as high workload, PPE shortage, knowledge and attitude toward using PPE, discomfort from wearing them, and desire to appear indifferent (Savoia et al., 2020; Zewude et al., 2021). The least used PPE by the participants in this study when entering a room for a patient with confirmed or suspected COVID-19 infection was wearing an N95 or higher-level respirator. This could be interpreted by using other types of masks (e.g., surgical masks) while at work (95.2% of the time). According to Peres et al. (2022), compared to surgical masks, using respirators by HCWs during the pandemic is more associated with discomfort, headache, dyspnea, skin reactions, difficulty in communication, and hindering optimal task performance.
Finally, this study indicates that positive HCWs’ attitudes are associated with adherence behaviors. Similar findings were reported by Alhumaid et al. (2021) and Latif et al. (2022). However, comparing the attitudes toward the adherence to COVID-19 precautionary guidelines before and after being vaccinated, HCW participants in this study reported a significant decrease in the perceived importance of following COVID-19 precautionary guidelines after being vaccinated. This could be interpreted by the increased perception of safety from exposure to the COVID-19 virus after being vaccinated (O’Donohue et al., 2022), which would lead to a decreased level of adherence to COVID-19 precautionary guidelines. For example, Zewude et al. (2021) showed that there was a significant decrease in adherence to following COVID-19 precautionary guidelines (e.g., wearing masks and hand hygiene) among a sample of HCWs when comparing preventive behaviors before and after receiving the first dose of COVID-19 vaccination.
Limitations
This study employed a cross-sectional survey design, which cannot prove or detect causal relationships. Another limitation is the potential for social desirability bias. This is when the participants provide responses that are favorable rather than what reflects their actual adherence behaviors and attitudes. Moreover, the recruited sample might not represent the demographic of the HCWs in the United States due to the low response rate and the homogeneity of participant characteristics (i.e., most participants were female and white, and all of them had a Master’s degree or higher). In addition, the participants were recruited from a single health center, which limits the generalizability of the study findings.
Implications for Occupational Health Practice and Future Research
The findings of this pilot study could help in developing intervention programs for increasing adherence to safety practices against COVID-19 among HCWs. The findings provide insights into the level of adherence to different behavioral practices among HCWs including using the required PPE. This provides guidance on specific practice areas that warrant focus when developing these intervention programs. The measures used in this study could be employed to evaluate the effectiveness of the developed interventions. Equally important, healthcare institutions should find ways to emphasize the importance of HCWs’ adherence to COVID-19 guidelines and monitor the adherence to these guidelines especially following vaccination. These and similar strategies could protect HCWs from acquiring COVID-19 infection, reduce the healthcare costs associated with HCWs being infected with COVID-19, and protect the health of patients from acquiring nosocomial COVID-19 infection.
Future research should be conducted with a more representative sample of HCWs from multiple recruitment sites. Also, research is needed to investigate the factors that influence the perceived importance of adhering to safety practices after a protection measure is adopted by healthcare institutions. Moreover, strategies targeted to promote adherence and attitudes toward adherence to infection control practices among HCWs at the personal and workplace levels should be investigated.
Conclusion
HCWs’ adherence to COVID-19 guidelines is essential to protect them from acquiring the infection. Unfortunately, the increased perceptions of safety from exposure to the COVID-19 virus after receiving COVID-19 vaccination negatively influenced HCWs’ adherence to COVID-19 precautionary guidelines in one large Midwest United States medical center. Continuous education and monitoring of HCWs are recommended to influence HCWs’ attitudes toward adherence to COVID-19 precautionary guidelines, particularly after vaccination.
Applying Research to Occupational Health Practice
This study findings provide insights on the level of adherence to different behavioral practices against COVID-19 infection among healthcare workers including using the required personal protective equipment. This helps in developing intervention programs aiming at increasing the adherence to these practices among healthcare workers. Equally important, this study suggests that healthcare institutions should find ways to emphasize the importance of healthcare workers’ adherence to COVID-19 guidelines and monitor the adherence to these guidelines especially following vaccination.
Footnotes
Authors’ Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by:
1. Medique Research Grant and the American Association of Occupational Health Nurses Foundation.
2. National Institute for Occupational Safety and Health through the Targeted Research Training Program of the University of Cincinnati Education and Research Center Grant #T42OH008432.
3. The National Center for Advancing Translational Sciences of the National Institutes of Health, Award number UL1TR001425. The content in this project is the authors’ responsibility and does not reflect the official views of the National Institutes of Health.
Human Subjects Review
The university Institutional review board approval was obtained on March 17, 2022. The study was determined as exempt (IRB ID 2022-0102).