
Abstract
Background:
9-1-1 telecommunicators are frequently exposed to indirect traumatic events that impact their mental and physical health and are often required to work overtime with rotating shifts. Previous studies reported various harmful effects of overtime on the health and well-being of workers, such as musculoskeletal injuries, burnout, low job satisfaction, fatigue, and intent to leave. However, there is limited research on the impact of overtime hours on 9-1-1 telecommunicators’ stress symptoms, especially mandatory overtime hours. This study aimed to examine the relationship between overtime hours—mandatory and voluntary—and the level of stress symptoms among 9-1-1 telecommunicators.
Methods:
We used secondary data from the surveys of the “Multi-tasking to hyper-tasking: Investigating the impact of Next Generation 9-1-1” study for analysis. Linear mixed-effects regression was applied to examine the association of overtime hours with the stress level.
Results:
Of the 403 participants, 47.6% reported that they were required to work mandatory overtime, and the mean mandatory overtime was 7.51 (SD = 12.78) hours in the past month. 58.3% reported working voluntary overtime, and the mean voluntary overtime was 11.63 (SD = 17.48) hours. This study found that mandatory overtime hours were associated with an increase in self-reported stress symptoms (β = 0.30, p = .002), whereas no significant association was found between voluntary overtime and the level of stress symptoms (β = −0.01, p = .885).
Conclusion/Application to Practice:
Study results highlight the importance of reducing mandatory overtime in call centers as one possible strategy for reducing stress levels among this critical workforce.
Background
9-1-1 Telecommunicators play an essential role in emergencies for the public as they receive and respond to incoming emergency and non-emergency calls by providing medical instruction to callers while dispatching first responders to the scene (Meischke et al., 2018). Due to the nature of their work, 9-1-1 telecommunicators are frequently indirectly exposed to traumatic events that impact their mental and physical health (Meischke et al., 2020). Even though the traumatic events they deal with are physically distant, they frequently experience feelings of fear, helplessness, frustration, and horror due to the calls they receive, and those feelings could potentially lead to the development of post-traumatic stress disorder (PTSD) (Birze et al., 2022; Carleton et al., 2020; Pierce & Lilly, 2012). Given these working conditions, it is unsurprising that 9-1-1 telecommunicators experience high work-related stress (Shakespeare-Finch et al., 2015). In one study, cortisol levels, a physiological measure of stress, were noted to be highest when 9-1-1 telecommunicators received incoming calls (Bedini et al., 2017).
Along with the stressful nature of their work, telecommunicators are also frequently required to work overtime due to staff shortages and difficulties in recruiting and retaining qualified and long-term employees (LeBlanc, 2017; Moore, 2019). 9-1-1 Telecommunicators work long, non-typical shifts (Meischke et al., 2015). The U.S. Fair Labor Standards Act (FLSA) defines overtime as working more than 40 hours per week (U.S. Department of Labor, 2016). However, the law does not limit the maximum number of hours employers can require their employees to work if employees are paid at a rate of time and a half for any hours worked beyond the regularly scheduled 40 hours. A study by LeBlanc (2017) reported that a dispatcher in Ingham County, Michigan worked 1,121 hours of overtime consecutively in 2016, 955 hours in 2015, and 967 hours in 2014.
An early review of studies from multiple industry sectors found that work overtime was associated with increased injury rates, illnesses, or mortality and feelings of decreased alertness and fatigue, lower cognitive function, and declines in vigilance on task measures (Caruso et al., 2004). Several studies in nursing also reported that long working hours (e.g., 12 hours/shift and more than 40 hours/week) were adversely related to the health and well-being of nurses, such as musculoskeletal injuries, obesity, absenteeism, burnout, reduced job satisfaction, fatigue, intent to leave, emotional disorders, and lack of time for housework (Bae & Fabry, 2014; Barker & Nussbaum, 2011; Han et al., 2011; Portela et al., 2005; Stimpfel et al., 2012, 2015; Trinkoff et al., 2006). Even though these results are from nursing, some of the negative impacts of overtime could occur among 9-1-1 telecommunicators because 9-1-1 telecommunicators also work irregular shifts (e.g., day, evening, and night shifts) and deal with life-threatening situations frequently. A recent study of 9-1-1 telecommunicators by Chae and Meischke (2021) reported a significant relationship between individual-level factors (e.g., mindfulness and overcommitment), organizational-level factors (e.g., job requirements and social support), and stress symptoms using a multilevel model. In that study, the total number of overtime hours was not significantly associated with symptoms of stress in a multivariable analysis, but the overtime variable did not differentiate between mandatory and voluntary overtime.
There is limited research on the impact of overtime hours, specifically mandatory overtime hours, on 9-1-1 telecommunicators’ levels of stress symptoms. Considering the work characteristics of 9-1-1 telecommunicators, this study examined the relationship between overtime hours—mandatory and voluntary—and the level of self-reported stress symptoms among a sample of 9-1-1 telecommunicators across the United States and Canada. The specific aims of this study were to (a) describe the voluntary and mandatory overtime hours and level of stress symptoms among 9-1-1 telecommunicators and (b) examine the relationship between the overtime hours—mandatory and voluntary—and the level of stress symptoms among 9-1-1 telecommunicators.
Methods
Study Design and Data Collection
We conducted a secondary data analysis of surveys collected from a randomized controlled trial (RCT) entitled, “Multi-tasking to hypertasking: Investigating the impact of Next Generation 9-1-1 (2016–2017)” that included evaluation of an online mindfulness training in addition to an observational cohort study (January 2015–June 2017) that evaluated stress associated with implementing Next Generation 9-1-1 (commonly referred to as NG911), which is a digital, internet protocol (IP)-based system that will replace the analog 911 infrastructure that has been in place for decades (Baseman et al., 2018; Kerr et al., 2019; Lilly et al., 2019). The parent study conducted baseline, post, and follow-up surveys with two different samples of telecommunicators for each of the study arms (RCT and observational study). The targeted 9-1-1 telecommunicators were those who had completed training, worked at any emergency call center, and were over age 18. For this study, we used data from the baseline surveys of both study samples. The data were collected through an online survey between April 2013 and November 2017 from full-time 9-1-1 telecommunicators at 49 call centers in the United States and two call centers in Canada. The 9-1-1 telecommunicators were recruited using convenience sampling through outreach campaigns, staff announcements, recruitment flyers, email, and word-of-mouth. The managers of call centers were approached to invite their 9-1-1 telecommunicators. Then, 9-1-1 telecommunicators were invited to participate in the survey by email after completing an electronic informed consent form (Baseman et al., 2018; Meischke et al., 2018). This study was approved by the institutional review board (IRB) at the University of Washington for its research ethics exemption because of its use of secondary, de-identified data (IRB number: STUDY00008583).
Measurements
Demographic Variables
Participants were asked to provide information on their age category, gender (female/male), marital status (yes/no), having children under the age of 18 years (yes/no), and countries and states where the call center belonged to.
Mandatory, Voluntary, and Total Overtime Hours
For mandatory and voluntary overtime hours, participants were asked if they had been required to work mandatory or voluntary overtime in the past month in a yes or no question and if they answered yes, they were then asked to enter mandatory and voluntary overtime hours they had worked in the past month (Meischke et al., 2018). For total overtime hours, we combined mandatory and voluntary overtime hours. If they answered no to mandatory and voluntary overtime, we determined they did not work overtime in the past month.
Stress Symptoms
The level of stress symptoms was measured by the Calgary Symptoms of Stress Inventory (C-SOSI). The C-SOSI measures physical and psychological symptoms of stress and was selected for the parent study outcome because it had been used in research evaluating the impact of a mindfulness intervention on stress in a different population (Carlson & Thomas, 2007). The C-SOSI is a 56-item scale comprising eight subscales: depression, anger, muscle tension, cardiopulmonary arousal, sympathetic arousal, neurological/gastrointestinal disorders, cognitive disorganization, and upper respiratory symptoms. Each item was answered on a 5-point Likert-type scale ranging from 0 (never), 1 (infrequently), 2 (sometimes), 3 (often), to 4 (very frequently) during a designated timeframe (e.g., during the last week). Internal consistency for the C-SOSI score in the parent study was α = .953 (Lilly et al., 2019). Cronbach’s alpha reliabilities for the subscales ranged from .80 to .95 (Carlson & Thomas, 2007). The total score of C-SOSI was calculated by summing the points for each item and used for the analysis.
Data Analysis
Descriptive statistics were performed on demographic variables and overtime hours, including frequency, mean, and standard deviation. To test the hypothesis of this study, linear mixed-effect regression was used to explore (a) the association of mandatory and voluntary overtime hours on the total C-SOSI score and eight subscales of C-SOSI, and (b) the association of any overtime (yes or no) on the total C-SOSI score while considering the “call centers” variable as a random effect. For the random effect, we included both a random intercept and random slope because data for participants nested within the organizations they belong to. Hypothesis testing set the p-value of .05 as statistical significance with adjustment of multiple testing comparisons using the Bonferroni correction (Noble, 2009). All analyses were conducted using STATA 17.0 (STATA Corp., College Station, TX, USA).
Results
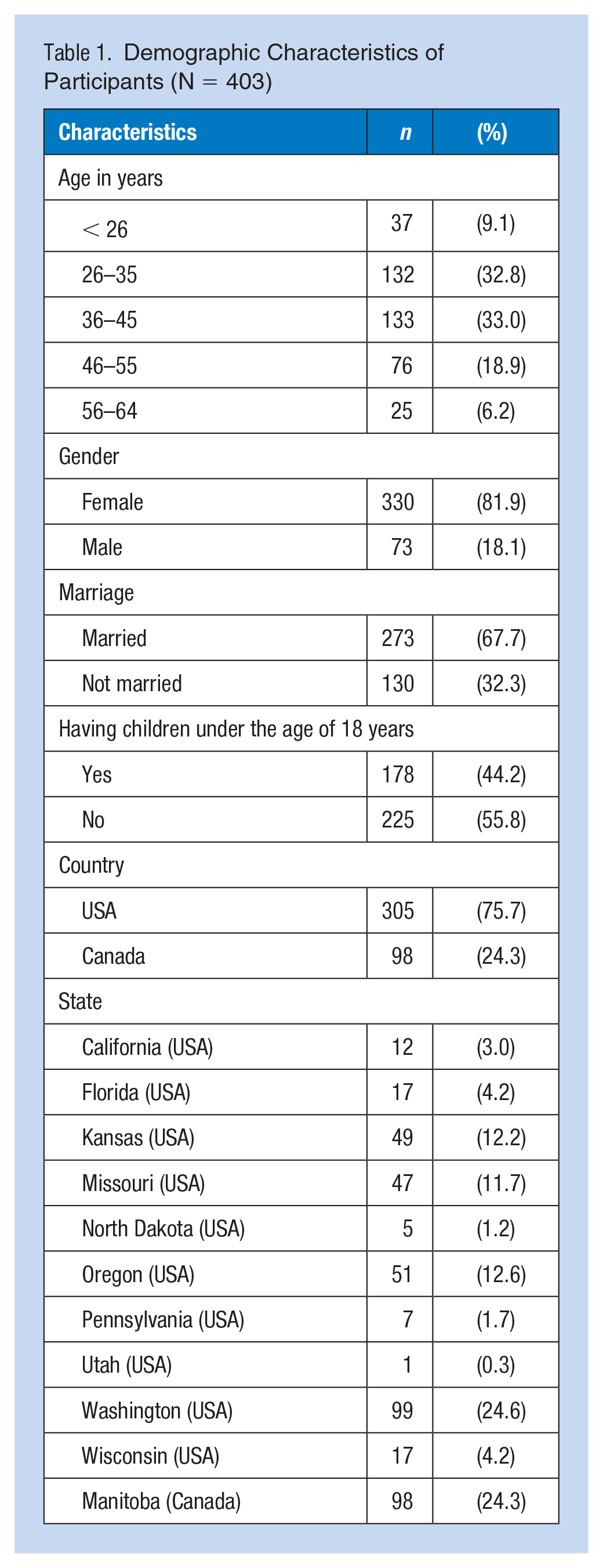
A total of 403 participants from the original study met the criteria for inclusion in our analysis. Of these, 32.8% were between 26 and 35 years old, and 33.0% were between 36 and 45 years old. Most participants were female (81.9%) and married (67.7%). About half of the participants reported having children under the age of 18 years (44.2%). Most of the participants were from the United States (75.7%). The other 24.3% were from Canada. The demographic characteristics of the study participants are summarized in Table 1.
Demographic Characteristics of Participants (N = 403)
Of the 403 participants, 47.6% reported that they had been required to work mandatory overtime. Among those who worked mandatory overtime, the mean mandatory overtime hours in the past month were 7.51 (SD = 12.78). The percentage of 9-1-1 telecommunicators who had worked voluntary overtime was 58.3%, and among those who worked voluntary overtime, the mean voluntary overtime hours in the past month were 11.63 (SD = 17.48). Overall, 75.45% reported that they had been required to work overtime in the past month. The mean overtime hours in the past month were 19.14 (SD = 22.43). The mean of the stress symptoms scores for the participants was 58.49 (SD = 30.59). Overtime hours, eight subscales, and total stress symptoms score are summarized in Table 2.
Overtime Hours and Stress Symptoms (C-SOSI) Score (N = 403)
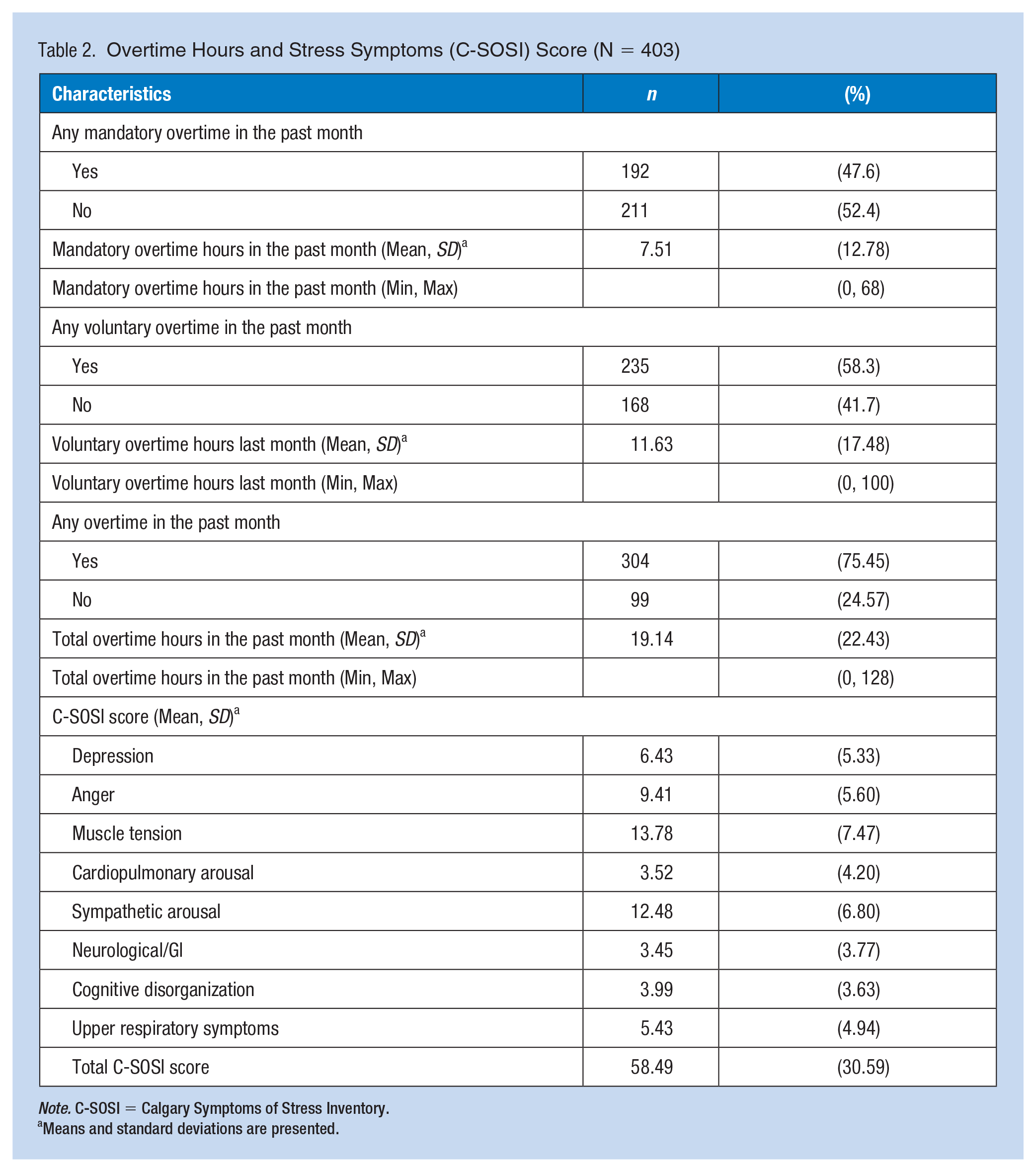
Note. C-SOSI = Calgary Symptoms of Stress Inventory.
Means and standard deviations are presented.
The results of the multiple linear regression analyses are shown in Table 3. After adjusting for gender, marital status, having children, and country, we observed a statistically significant association between mandatory overtime hours and the level of stress symptoms among 9-1-1 telecommunicators. An hour of increase in mandatory overtime was associated with an increase in 0.30 scores of the level of stress symptoms (β = 0.30, p = .002). However, there was no significant association between voluntary overtime hours and the level of stress symptoms (β = −0.01, p = .885) and between total overtime hours and the level of stress symptoms (β = 0.09, p = .240). For analyses by mandatory (β = 11.42, p = .003), voluntary overtime (β = 11.60, p = .003), and total overtime (β = 11.62, p = .003), being female was significantly associated with an increased level of stress symptoms.
Mixed-Effect Linear Regression on Stress Symptoms by Mandatory Overtime, Voluntary Overtime, and Total Overtime
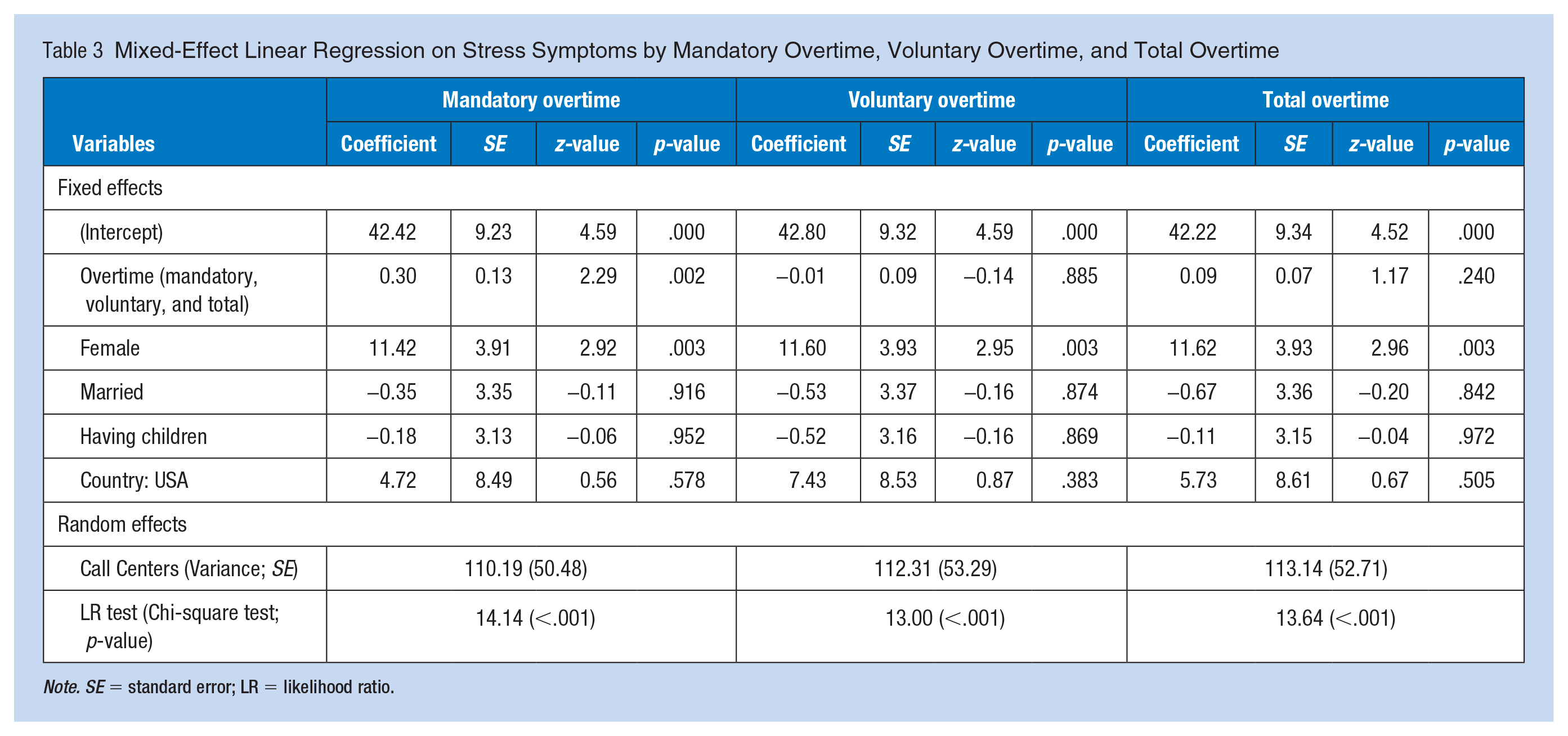
Note. SE = standard error; LR = likelihood ratio.
We also analyzed whether there were associations between dichotomous overtime (yes or no) and the total C-SOSI score. Results are consistent with the analyses with overtime (hours), showing that mandatory overtime (yes or no) was positively related to the total C-SOSI score (β = 10.12 above, p = .004), and voluntary overtime (yes or no) was negatively related to the total C-SOSI score (β = −8.68, p = .006). There was no significant association between the total overtime (yes or no) and the total C-SOSI score.
The results of multiple linear regression analyses on subscales of C-SOSI are shown in Supplemental Figure 1. We found statistically significant associations between mandatory overtime and depression (β = 0.06, p = .015), anger (β = 0.06, p = .008), and muscle tension (β = 0.07, p = .022). There were no statistically significant associations between voluntary or total overtime and subscales of C-SOSI.
Discussion
This study examined whether mandatory, voluntary, and total overtime was related to the level of stress symptoms among 9-1-1 telecommunicators. In multiple linear regression and dichotomous analysis, we found that mandatory overtime hours were associated with increased stress symptoms after adjusting for demographic characteristics. In contrast, voluntary overtime was not significantly related to stress symptoms in the multiple linear regression and was negatively related to stress symptoms in the dichotomous analysis. We did not find any statistically significant relationship between total overtime and the level of stress symptoms.
The main factors contributing to overtime for 9-1-1 telecommunicators are understaffing and low retention rates (Moore, 2019). Previous studies described the mechanism of understaffing, overtime, and stress (Furihata et al., 2022; Northwest Center for Public Health Practice, n.d.; Stimpfel et al., 2022). More work hours increase stress and burnout and discourage recruits, leading to a staff shortage. This, in turn, creates more overtime, worsening the shortage in a vicious cycle. The trend of retention rates is going down. Between 2005 and 2008, 65% of call centers had decreased employee retention, while only 22% indicated retention had increased (Association of Public-Safety Communications [APCO] International, 2018).
In terms of the relationship between overtime hours and stress symptoms, even including various types of employees in different companies, many previous studies have already verified that levels of stress symptoms were relatively worse among workers with longer overtime than those with shorter hours (Kikuchi et al., 2020; Sato et al., 2020). We could identify possible reasons for higher stress symptoms among workers with long overtime because these workers may not have enough time to rest, relax, sleep, and feel refreshed. Such unbalanced working and recovery from exhaustion may lead to various mental illnesses like stress symptoms (Sato et al., 2020). Moreover, an interesting finding in this study was that the effect of mandatory overtime differed from voluntary overtime on stress symptoms. Beckers et al. (2008) showed that mandatory overtime was associated with relatively high fatigue and low satisfaction, especially with insufficient compensation. Similar results were found in a study on police officers. Mandatory overtime was related to overall burnout, emotional exhaustion, and depersonalization among police officers, while voluntary overtime was not significantly related to overall burnout and emotional exhaustion (Peterson et al., 2019). On the other hand, a previous study reported that one of the reasons for doing overtime for critical care nurses was financial gain for 96% of participants (Lobo et al., 2018). This implies that extra money made from overtime is perceived as a benefit that might reduce adverse effects such as stress from overtime. This may explain our result reporting that voluntary overtime was negatively related to stress symptoms in the dichotomous analysis, indicating that voluntary overtime does not negatively affect stress and may even be a buffer to stress symptoms, as voluntary overtime allows telecommunicators to control when/how much overtime they work, and provides an additional source of income that might reduce worries over finances. Previous findings and our results suggest that mandatory overtime impacted more negatively than voluntary overtime on stress symptoms.
While this study did not find a significant association between voluntary overtime and any of the eight subscales of C-SOSI, there was a significant association between mandatory overtime hours and C-SOSI subscales of depression, anger, and muscle tension. This is in line with previous literature. A study by Kikuchi et al. (2020) reported that longer overtime work hours among Japanese workers were significantly associated with irritability, fatigue, anxiety, depression, and somatic responses. Another study by Sampaio et al. (2020) found that nurses who experienced overtime working during the COVID-19 pandemic had significantly higher stress levels and depression and anxiety levels. Based on our results and previous evidence, the mental health of 9-1-1 telecommunicators should be paid particular attention when developing tailored interventions for managing stress symptoms for 9-1-1 telecommunicators.
Finally, we found that female 9-1-1 telecommunicators experienced more stress symptoms than males. Women tend to have more child care responsibilities, reducing the time for recovery from work (Caruso et al., 2004). On the other hand, women with children may be more likely to want to work overtime due to the financial need for child care (Bae et al., 2012; Lobo et al., 2018) or prefer flexible shifts (e.g., choosing 8 or 12 hours shifts) to accommodate child care (Association of Public-Safety Communications [APCO] RETAINS Workgroup, 2005). Future studies are needed to verify further relationships between overtime and stress symptoms moderated by gender.
This study contributes to understanding the association of overtime hours, especially mandatory overtime, with stress among 9-1-1 telecommunicators. The secondary dataset, however, did not include several other variables that might be associated with the 9-1-1 telecommunicator’s stress. For example, workload (e.g., the volume of calls received, the intensity of traumatic calls they receive), job satisfaction, or working environment can be important variables affecting stress among 9-1-1 telecommunicators. This study has limitations in that respondents may have been biased in some way in that the data were collected as part of a larger stress reduction intervention study. Even though the sample was a convenience sample, participants were recruited from many call centers across the nation (and Canada), which increases the generalizability of findings. In addition to possible self-selection bias, the main outcome was measured with the C-SOSI, which was originally evaluated with a group of cancer patients rather than a working population. However, the strength of this measure is that it assessed various physical and psychological aspects of stress symptoms, which allows a more comprehensive assessment of the impact of stress on the body and mind. In addition, the data used in this study were collected from 2015 to 2017 and may not reflect the current working conditions of 9-1-1 telecommunicators.
Implications for Occupational Health Practice
The results of this study show that mandatory overtime hours, unlike voluntary overtime, are associated with increased stress levels among 9-1-1 telecommunicators. To reduce the impact of mandatory overtime, organizational interventions such as flexible working arrangements (i.e., greater control over when, how long, and whether they work) can be considered (Joyce et al., 2010; Kröll et al., 2017; World Health Organization, 2022). In addition, developing and implementing stress management programs specifically for 9-1-1 telecommunicators are important steps to stop the vicious cycle (The National Emergency Number Association [NENA] PSAP Operations Committee, 9-1-1 Acute/Traumatic and Chronic Stress Working Group, 2013).
Conclusions
Mandatory overtime hours are associated with increased stress symptoms among 9-1-1 telecommunicators. Further studies on developing organizational and individual interventions to reduce stress and strategies to reduce overtime, especially mandatory overtime. In addition, ongoing efforts should be focused on influencing policymakers to develop successful regulations that limit overtime hours for 9-1-1 telecommunicators.
Applying Research to Occupational Health Practice
9-1-1 Telecommunicators are the first responders in emergencies for the public. In addition to being exposed to traumatic calls, they are frequently required to work overtime due to staff shortages. This study found that working mandatory overtime hours increases symptoms of stress among 9-1-1 telecommunicators. Future protective approaches are needed to reduce overtime, especially mandatory overtime, and manage stress symptoms among 9-1-1 telecommunicators. Call centers need to find innovative strategies to reduce mandatory overtime, which can impact anxiety, depression, and muscle tension. Tailored interventions for reducing and managing stress symptoms are also crucial to reduce the stress of 9-1-1 telecommunicators.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231202794 – Supplemental material for Effect of Mandatory and Voluntary Overtime Hours on Stress Among 9-1-1 Telecommunicators
Supplemental material, sj-docx-1-whs-10.1177_21650799231202794 for Effect of Mandatory and Voluntary Overtime Hours on Stress Among 9-1-1 Telecommunicators by Seungeun Park, Hendrika Meischke and Sungwon Lim in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Institute for Occupational Safety and Health (NIOSH), and the Centers for Disease Control and Prevention (CDC), grant number ROH010536 (PI: Dr. Meischke).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.