
Abstract
Background:
Public safety workers (PSWs), including correctional officers (COs), law enforcement, firefighters, emergency medical service, and military personnel, are at risk of organizational stress and burnout. Exposure to traumatic events, job hazards, injuries, fatalities, and work-related stressors such as work overload, irregular shift assignments, and lack of administrative support can negatively impact PSWs’ mental health. Peer support programs (PSPs) have been cited as an intervention to address the mental health of PSWs.
Purpose:
The purpose of this review is to explore the use, including facilitators and barriers, of PSPs to reduce organizational stress and trauma for PSWs. Implications for COs will be discussed.
Method:
A scoping review was conducted using the Arksey and O’Malley methodology. A search was conducted for articles published between 1996 and 2021 using six databases. Selected articles described, implemented, or evaluated peer support as an intervention to reduce PSW organizational stress and trauma.
Findings:
Thirteen articles met eligibility criteria. Organizational support, including policies, practices, and peer leadership training, contributed to the sustainability of PSPs. Confidentiality, trust, and shared lived experience were also essential to PSP. Stigma was identified as the primary barrier to participation. Public safety workers found PSP helpful in normalizing experiences, increasing hope, and decreasing stigma. Peer support programs also serve to bridge the gap in mental health services use.
Conclusions:
Peer support programs are a potential mental health intervention to reduce organizational stress and trauma for COs. Awareness of the facilitators and barriers to PSPs is the first step in developing such programs.
Keywords
Background
Correctional officers, firefighters, police officers, and emergency medical personnel are employed in some of the most dangerous occupations in the United States (National Occupational Research Agenda [NORA], 2019). These workers, collectively referred to as public safety workers (PSWs), represent approximately 2.86 million workers in the United States (NORA, 2022). Public safety workers come from a variety of educational and experiential backgrounds, and between 10% and 25% of PSWs have served in the military. Former military personnel often transition into PSW roles because they are familiar with the unpredictability of work, organizational structure, and work culture (Turner & Moran, 2021). Military personnel were included with PSWs in this scoping review due to frequent exposure to stress and trauma, and transition to PSW positions after active duty, including the U.S. criminal justice system (Turner & Moran, 2021; Weichselbaum et al., 2017).
Public safety workers routinely place their lives and well-being at risk as an intrinsic component of their work (LaTourrette et al., 2008). Unlike other workers in the United States, PSWs are exposed to job hazards, injuries, and fatalities that are as much as 3 times higher than those faced by workers in nonsafety occupations (LaTourrette et al., 2008; NORA, 2019). A recent report by the Department of Justice on workplace violence noted that correctional officers had the highest rate of nonfatal workplace violence injuries compared with other occupations (Bureau of Justice Statistics [BJS], 2022). Public safety workers are expected to engage in response efforts, often during and after traumatic events. These traumatic events may be direct, witnessed by the individual, or indirect, experienced by hearing, reading, or viewing reports about the event. Organizational stressors refer to the psychosocial aspects of the work relative to the agency itself and act as barriers to the use of PSPs. These stressors may include inadequate training, politics, shift assignments, heavy workload, coworker conflict, disciplinary action, lack of administrative support, unclear policymaking, negative interactions with the judicial system and negative public image, and stigma (Brower, 2013; Spinaris, 2020).
Although the work may be rewarding, it can also affect their physical and mental well-being. Repeated exposure to these occupational risks results in physical, mental, and emotional disorders, often at incidences greater than the general population (Substance Abuse and Mental Health Services Administration [SAMHSA], 2018). It is estimated that 30% of PSWs experience behavioral health issues compared with 20% in the general population (Abbot et al., 2015). Public safety workers are at a greater risk of cardiovascular disease, cancer, infectious disease, musculoskeletal disorders, motor vehicle accidents, and workplace violence (LaTourrette et al., 2008). They are also at risk of mental health issues, including stress, depression, burnout, posttraumatic stress disorder (PTSD), and suicide (Heyman et al., 2018; Jaegers et al., 2019; Konda et al., 2012; Violanti et al., 2017). While the prevalence of mental health issues among PSWs has been studied, interventions and strategies to improve mental health outcomes, such as peer support programs (PSPs), have received less attention and appear to be understudied among PSWs.
Worksite PSPs have shown effectiveness in addressing health behaviors such as improved nutrition, weight loss, participation in programs for cancer screenings, and smoking cessation (Allen et al., 2001; Bondy & Bercovitz, 2013; Hersey et al., 2008; Sorensen et al., 1998). Peer support programs also contribute to a positive workplace culture in which workers care for each other and feel supported (Linnan et al., 2015). As workplaces seek to address the increasing mental health concerns of workers, PSPs are receiving attention as a possible strategy to assist workers (World Health Organization, 2022). The role of PSPs in mental healthcare varies depending upon the needs of the organization. Peer support programs are designed for crisis intervention and provide mental health relief to workers exposed to daily stress and trauma in their everyday work. Because PSPs can be flexible in their aim, they are well suited for supporting staff in high-risk organizations where employees not only respond to traumatic events but also experience chronic daily stress (Levenson & Dwyer, 2003).
Peer support is founded on the premise that people who have similar experiences may better relate to one another and offer more authentic empathy and validation (Mead & McNeil, 2006). Peer support programs offer several benefits. They are often readily available once established in the organization. They provide an opportunity to develop resilience by learning to effectively negotiate, adapt to, or manage significant sources of stress or trauma with a group of peers (Agarwal et al., 2019). Peer support programs can further improve mental health and well-being by focusing on strengths and recovery through emotional and social support, encouragement, and hope (Cyr et al., 2016; Repper & Carter, 2011). Finally, there is evidence that boosting social support, in the form of PSPs, can increase an individual’s capacity to deal with potentially traumatic events (Norris & Stevens, 2007).
Peer support programs for PSWs, however, represent a cultural shift in mental health well-being by workers who typically are hesitant to talk about their feelings, particularly their distress (SAMHSA, 2018). Public safety workers’ reluctance to seek treatment has been due to the concern of personal failure, fear of appearing weak, career repercussions, and perceived stigma (Heffren & Hausdorf, 2016; Wills et al., 2021). As a result, PSWs may not seek needed professional assistance. Stuart (2008) found that greater than 50% of surveyed police officers would not seek professional help if they were symptomatic with a mental illness. This is consistent with data that more than half of U.S. adults with a mental illness did not receive care in 2020 (Mental Health America, 2022).
There is evidence to suggest that PSWs may prefer informal sources of help over formal or professional mental health interventions (Carleton et al., 2020; Jeannette & Scoboria, 2008; Tamrakar et al., 2020). Informal sources of mental health help include family, friends, and peers collectively referred to as social support. These sources of help have been less studied than formalized mental healthcare (Lauzier-Jobin & Houle, 2022). There is growing interest in exploring and using informal sources of support to address mental healthcare in the workplace, because peers understand the unique challenges of the job, which can promote the expression of genuine empathy by the intervening peers, and peers provide a sense of camaraderie and support not available from family and friends (Billings et al., 2021). Peers offer an informal day-to-day understanding of the work culture that is preferred over support from other sources of help (Jeannette & Scoboria, 2008). Finally, PSWs tend to trust their peers more than mental health professionals (Horan et al., 2021).
Studies exploring PSPs and other mental health interventions for PSWs have primarily focused on a subset of workers: law enforcement and firefighters. A recent systematic review and meta-analysis of mental health interventions and their uses in public safety organizations found that workplace mental health interventions were primarily focused on police officers and firefighters, with few studies targeting other PSWs (Edgelow et al., 2021). More than half of the studies were regarding police officers (n = 64), and less than a third included firefighters (n = 23) and paramedics (n = 9; Edgelow et al., 2021). Only four studies identified in the meta-analysis included corrections officers, and one of the studies combined police officers, firefighters, and paramedics (Edgelow et al., 2021).
In the United States, there are approximately 390,000 correctional officers working in facilities housing just under 1.7 million individuals incarcerated in the United States (Bureau of Labor Statistics [BLS], 2022; Carson & Kluckow, 2023). Correctional officers (COs) are among the least studied group of PSWs (Brower, 2013; El Ghaziri et al., 2020; Evers et al., 2020; Ferdik & Smith, 2017). A scoping review covering the past 26 years explored intervention studies to address stress and trauma for COs. Only 25 studies addressed this group of PSWs (El Ghaziri et al., 2020). White papers on the mental health of COs have cited PSPs as a promising intervention to decrease stress and improve mental health (Brower, 2013; Denhof et al., 2014; Ferdik & Smith, 2017; Finn, 2000). The National Corrections Collaborative (NCC), a consortium of researchers and practitioners in corrections, has also identified peer support as an intervention modality needing further exploration to address mental health of COs (El Ghaziri et al., 2020). Peer support programs have also been identified by key stakeholders in corrections as a program that may benefit mental health of COs; however, such programs have not been fully explored or evaluated (NCC-Project Taskforce Meeting, 2021).
Therefore, the purpose of this study was to perform a scoping review to capture what is known about PSPs as an intervention to address the mental health of PSWs. The findings will be discussed using the lens of the social ecological model (SEM). This model posits that the individual is influenced by multiple interactions, including interpersonal, organizational, and societal (McLeroy et al., 1988). For this review, PSP will be explored with attention to these interactions, including interpersonal (peer-to peer), organizational (workplace setting), and societal factors (stigma and policy). Furthermore, the findings will be discussed with implications for COs as an understudied workforce compared with other PSWs.
Methods
The methodology for this scoping review was guided by the framework proposed by Arksey and O’Malley (2005). This method is used to map the extent, range, and nature of research activity in a topic area to determine the value of undertaking a full systematic review, to summarize and disseminate research findings, and to identify gaps in the existing literature (Arksey & O’Malley, 2005). This approach is preferred when research is emerging. Scoping studies allow a researcher to incorporate a range of study designs, including published and gray literature, to address questions beyond those related to intervention effectiveness (Levac et al., 2010). This review followed the six phases described by Arksey and O’Malley: identifying the research question; identifying relevant studies; study selection; charting the data; collating, summarizing, and reporting the results; and consultation with subject matter experts.
Identifying the Research Question
This review was guided by the following question: What is known about PSPs as an intervention for PSWs aimed at reducing organizational stress and trauma?
Identifying Relevant Studies
A literature search was conducted to identify articles published from 1996 to 2022. The following databases were searched: PubMed, CINAHL, Scopus, Criminal Justice Abstracts, PsycINFO, and Google Scholar. Also, journals of professional associations and government documents were hand-searched for additional articles that met the search criteria. Key terms that guided this review included peer support, peer counseling, peer mentor, peer mentoring, peer support groups, support group, peer support programs AND correctional officers or prison employees or prison guard or corrections officer, police officers or law enforcement or cops, police, firefighters, first responders, EMT, paramedic, emergency medical technician, emergency medical service or EMS, veterans or military or soldiers, military personnel or serviceman or servicewoman.
Study Selection
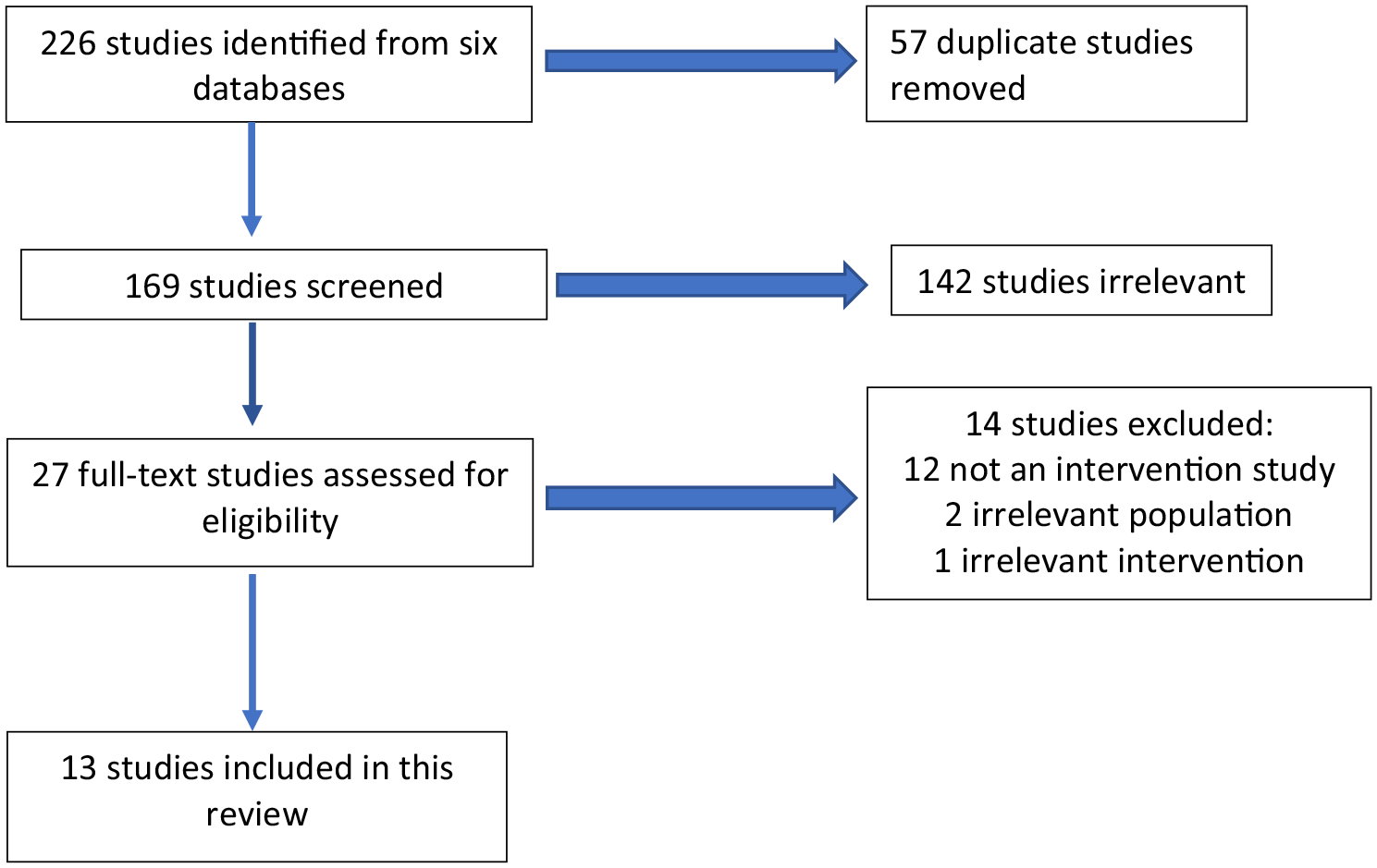
Titles and abstracts were reviewed using Covidence, a software platform used to organize and streamline the review process: The inclusion criteria were the following: articles must be written in English; a PSP intervention was described, implemented, or evaluated; and the goal of the peer support intervention was to reduce workplace stress or trauma. The following types of studies were excluded: studies that mentioned peer support as an intervention but did not fully describe either implementation or evaluation; studies not aimed at reducing workplace stress or trauma; and studies that did not explore the impact on PSWs. Crisis intervention groups were not included in this review because they are often designed to address a single traumatic event. The goal of this review was to explore peer support as a health promotion intervention rather than tertiary prevention program. A PRISMA-ScR flowchart (Figure 1) depicts the study selection process.
PRISMA-ScR Flow Diagram
Charting the Data
The pertinent findings, including author, date of publication, type of PSWs, aim of the study, study design, and outcome measures, were transposed into a table format. As recommended by Arksey and O’Malley (2005), the study methodologies were not formally appraised as the purpose of this review is to describe what is known about peer support in PSWs, rather than as a formal review of method.
Collating, Summarizing, and Reporting the Results
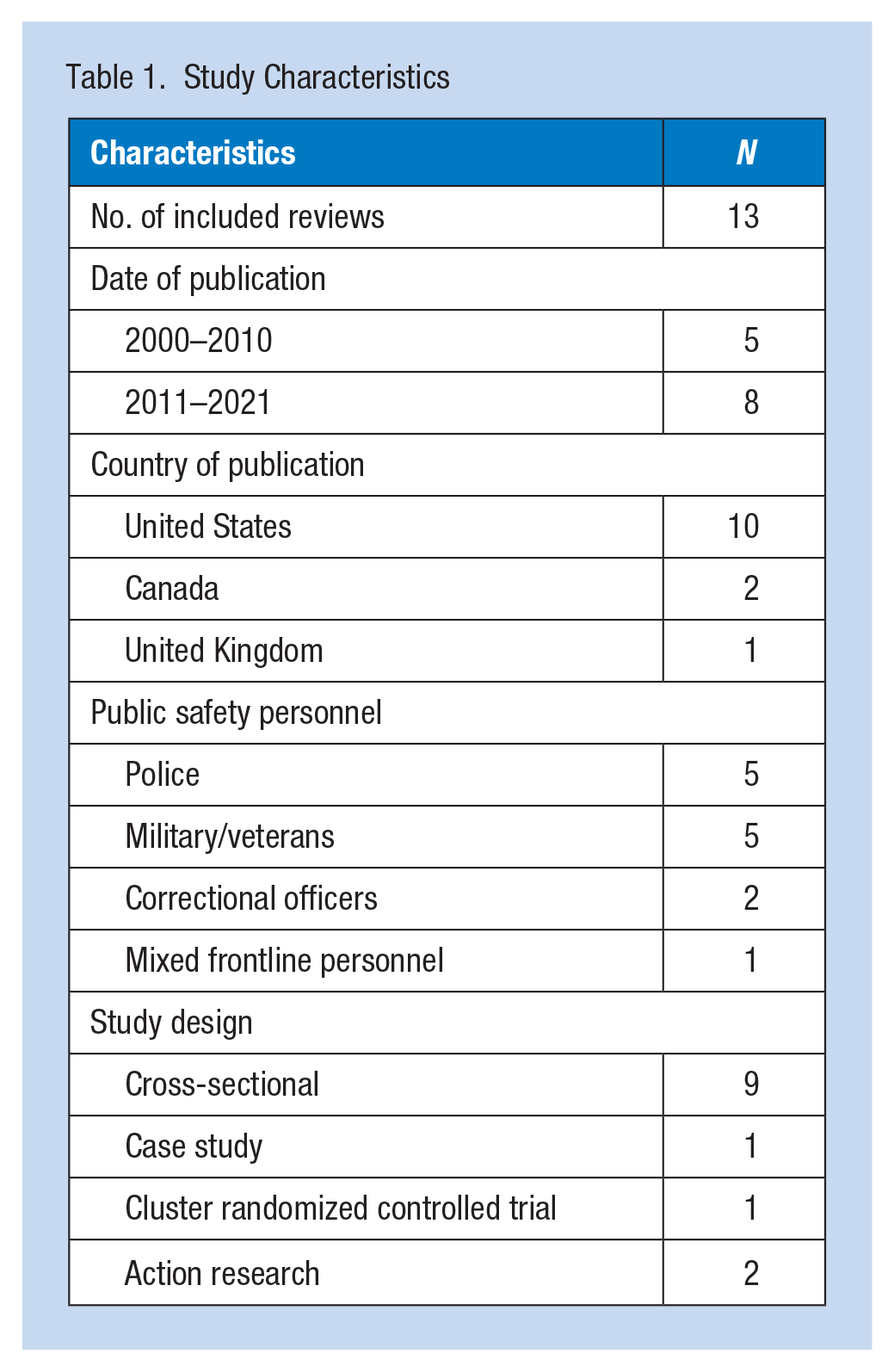
Characteristics of each study, including date of publication, country of origin, population identification, and study design, are summarized in Table 1. Detailed findings from the review are summarized in Table 2. Finally, a narrative of the findings is described in the “Results” section.
Study Characteristics
Scoping Review Findings
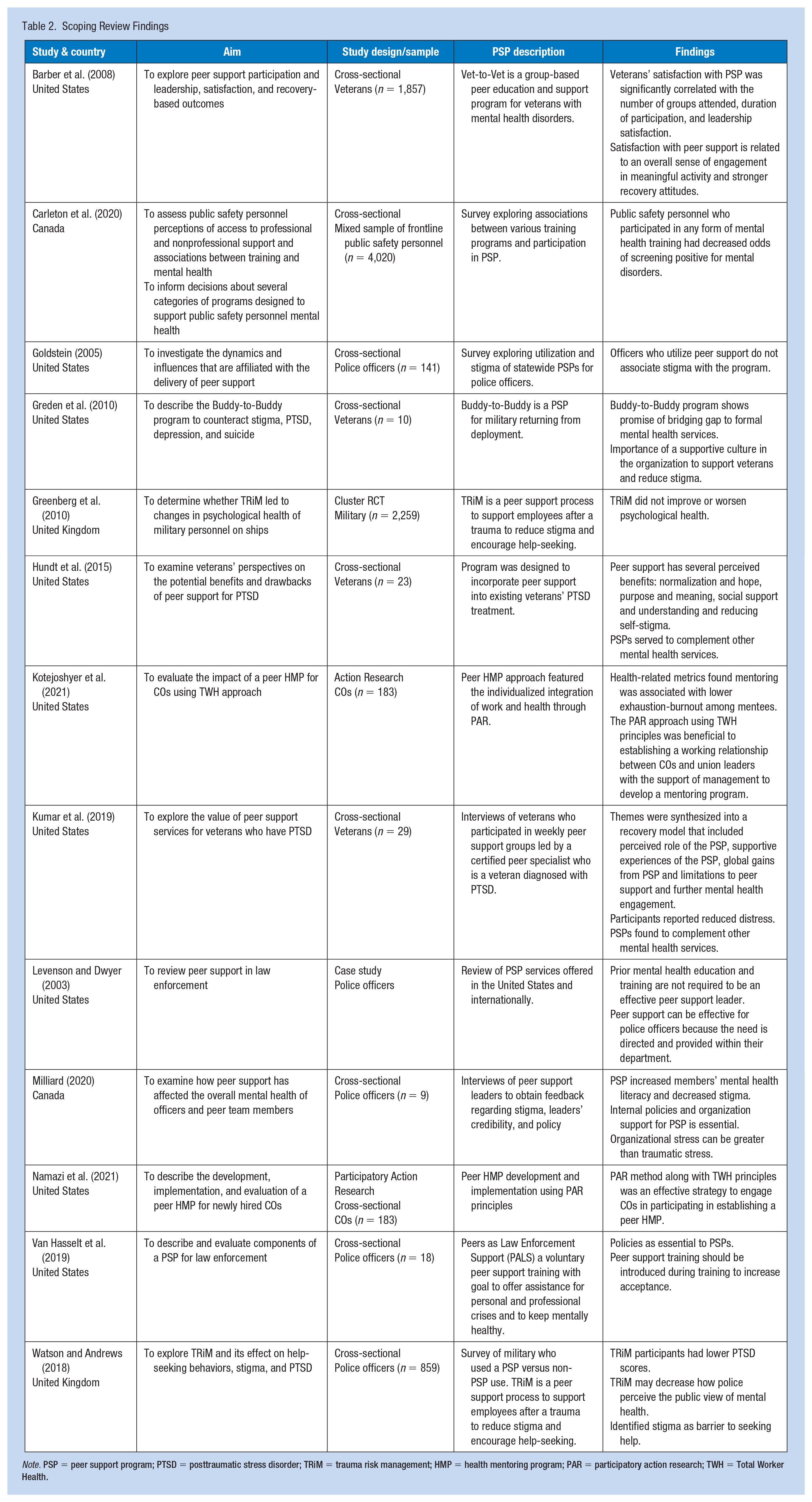
Note. PSP = peer support program; PTSD = posttraumatic stress disorder; TRiM = trauma risk management; HMP = health mentoring program; PAR = participatory action research; TWH = Total Worker Health.
Consultation
While this is an optional phase in Arksey and O’Malley’s (2005) framework, it adds methodological rigor to the review (Levac et al., 2010). Consultation with experts and stakeholders can provide additional sources of information, perspectives, and meaning to the scoping review. For this review, the initial findings were shared with researchers in correctional health who helped the authors expand the scope of this study to include other PSWs. Consultation was also undertaken to ensure that the implications for research, policy, and practice were pertinent to COs.
Results
Literature Search
The initial search yielded 225 articles for review. Of these, 57 articles were duplicates and were removed, leaving 168 articles screened by title and abstract. Twenty-six articles underwent a full-text review for eligibility. For this review, 15 articles were excluded for one of the following reasons: irrelevant intervention, no intervention, or irrelevant population. Thirteen articles met the criteria for full-text extraction and were included in this scoping review.
Study Characteristics
Thirteen studies were found for this review. The characteristics of the articles selected for this scoping review are shown in Table 1. Ten studies were conducted in the United States, two in Canada, and one in the United Kingdom. All PSPs described were led by peer leaders, considered as informal sources of support. There were no studies addressing PSPs for PSWs prior to the year 2000. Five articles were found between the years 2000 and 2010, and eight articles between the years 2011 and 2021. Studies that explored PSPs specifically aimed to reduce stress and trauma among PSWs have increased in the past 5 years, with six of the studies published since 2017.
Studies aimed at PSPs for police officers and military accounted for 10 of the 13 studies reviewed for this article. There were five studies aimed at police officers (Goldstein, 2005; Levenson & Dwyer, 2003; Milliard, 2020; Van Hasselt et al., 2019; Watson & Andrews, 2018), and five studies describing military experiences (Barber et al., 2008; Greden et al., 2010; Greenberg et al., 2010; Hundt et al., 2015; Kumar et al., 2019). Two studies explored correctional officers (Kotejoshyer et al., 2021; Namazi et al., 2021), and one study included a mixed sample of PSWs (Carleton et al., 2020). There were no identified studies that explored PSPs for frontline safety personnel such as firefighters or emergency medical technicians using the inclusion criteria cited.
The study designs represented in this review are varied. This is common when a scoping review is conducted to capture a broad perspective of an emerging topic. The designs include nine cross-sectional studies (Barber et al., 2008; Carleton et al., 2020; Goldstein, 2005; Greden et al., 2010; Hundt et al., 2015; Kumar et al., 2019; Milliard, 2020; Van Hasselt et al., 2019; Watson & Andrews, 2018), one case study (Levenson & Dwyer, 2003), one cluster random controlled trial (Greenberg et al., 2010), and two participatory action research studies (Kotejoshyer et al., 2021; Namazi et al., 2021).
Key Findings
The findings from this review are described in respect to three key themes: health outcomes, process evaluation, and benefits and barriers to PSPs for PSWs. These themes emerged through an iterative process of reading each study, careful notetaking, and combining like ideas until themes developed.
Health Outcomes
Three qualitative studies and one cross-sectional survey designed study indicated efficacy in PSPs to improve mental health literacy and decrease stigma about participating in help-seeking behaviors among participants (Goldstein, 2005; Hundt et al., 2015; Milliard, 2020). Participants in a PSP program were reported to have reduced distress (Kumar et al., 2019). Hundt et al. (2015) found that PSPs might normalize PTSD and reduce self-stigma. Goldstein (2005) found that police officers who participated in PSPs also had reduced feelings of stigma related to attending PSPs, t(128) = −2.717, p = .008. In another study, themes of normalization, hope, social support, and understanding and recovery emerged from a focus group of veterans who participated in a PSP (Hundt et al., 2015). Another benefit cited was that PSPs that are readily accessible serve as a bridge or complement to other mental health services (Greden et al., 2010; Hundt et al., 2015; Kumar et al., 2019).
Process Evaluation Findings
Organizational Support
Organizational support from administration and managers, along with training, funding, and policies were identified as key factors to develop and sustain PSPs (Milliard, 2020; Van Hasselt et al., 2019). This need demonstrates the influence of factors at the organization level of the SEM that affect the use of PSP. Participants in one study shared that PSPs should be “driven by the top down and should have a formal policy” (Milliard, 2020, p. 5). Another participant in the Milliard (2020) study commented that an internal policy “gives it credence . . . shows that it is important, supporting our people.” (Milliard, 2020, p. 5). Van Hasselt et al. (2019) described policies as well as mandatory trainings as essential parts of the Peers as Law Enforcement Support (PALS) program. This study also recommended that peer support be introduced during law enforcement trainings to increase its acceptability among officers.
Organizational support by key stakeholders coupled with CO involvement has also shown to be an effective approach to support mental health interventions in corrections. Namazi et al. (2021) found that engaging COs using a participatory action research (PAR) approach, guided by National Institute for Occupational Safety and Health (NIOSH) Total Worker Health (TWH) principles, resulted in the participation of almost 300 COs in a peer health mentoring program. Total Worker Health includes the policies, programs, and practices that integrate protection from work-related safety and health hazards with promoting injury and illness prevention efforts to advance worker well-being (NIOSH, 2021). It incorporates all aspects of work using a collective approach to engage workers to address safety, health, and well-being. The PAR approach engages key stakeholders in multiple stages of planning, development, implementation, and project evaluation (Cherniack & Punnett, 2019). High participation rates were noted among workers who often are reluctant to engage in programs that require sharing of personal health issues with peers (Namazi et al., 2021).
Peer Support Leadership
Several of the studies in this review described the characteristics of an effective PSP (Goldstein, 2005; Hundt et al., 2015; Levenson & Dwyer, 2003; Milliard, 2020). These findings are consistent with the interpersonal level of influence in the SEM in that peer relationships affect the use of PSPs. The quality of the peer support leader was addressed most often. A participant in one study commented that the peer leader should “lead and not dictate . . . (be) kind of easy going but (able to) still stay on track” (Hundt et al., 2015, p. 855). Participants in the Milliard (2020) study suggested prescreening peer leaders to determine whether they have the aptitude to help others. Van Hasselt (2019) described further criteria to be included in the role of a team member of the PALS program. Team members must have a good rapport with peers, proficient listening skills, and demonstrate the ability to empathize and provide support for fellow police officers experiencing distress (Van Hasselt et al., 2019, p. 2). Levenson and Dwyer (2003) write that professional mental health education and training are not required to be an effective peer support leader. They suggested training can be provided for those who express an interest in this role. Other criteria of an effective peer leader include being a peer of equivalent rank, being willing to share their lived experience, and providing reassurance and access to resources, including professional mental health resources (Carleton et al., 2020; Hundt et al., 2015; Kumar et al., 2019).
Team Sharing
The willingness of participants to share their authentic lived experience is essential to a successful program, and this needs to occur within an atmosphere of trust (Milliard, 2020). The following qualities align with the interpersonal level of the SEM and foundation of PSPs. Trustworthiness and credibility of support group members also helped to reduce stigma associated with participation in a PSP. Greden et al. (2010) described PSPs as using culture to change culture. Peer support leaders who are part of the culture are best able to help support those who need help and reduce the stigma of reaching out for assistance. Peer support programs developed within the organization can positively affect how coworkers perceive care and support where they work. Participants commented that they were able to connect with their own peers, stating, “we believe in taking care of our own” and “other veterans can be trusted” (Greden et al., 2010, p. 93). Confidentiality was also cited as a necessary component to PSPs (Greden et al. 2010; Kumar et al., 2019; Levenson & Dwyer, 2003; Van Hasselt et al., 2019).
Barriers to PSP Participation
Stigma was the most frequently mentioned barrier to participation in a PSP. Three types of stigma were identified in this review: public stigma, self-stigma, and stigma by association. Public stigma is the negative attitudes and beliefs that motivate individuals to fear, reject, avoid, and discriminate against people with mental illnesses (Corrigan & Penn, 1999). When public stigma becomes internalized, it is referred to as self-stigma. Self-stigma can have negative consequences for help-seeking behaviors. It is also associated with poorer mental health treatment outcomes (Oexle et al., 2018). Self-stigma was identified as a possible reason that police officers may not seek assistance for mental health issues (Watson & Andrews, 2018). Interestingly, Goldstein (2005) found that police officers reported less self-stigma after participating in a PSP. Watson and Andrews (2018) identified stigma by association as a barrier to PSPs as it may affect relationships with coworkers. Stigma by association is the disapproval of others as a consequence of associating with a stigmatized person (Goffman, 1963). All participants in the Watson and Andrews’s (2018) study expressed fear that participation in peer support may harm their career and coworkers may have less confidence in them.
Discussion
This scoping review aimed to identify studies about PSPs to reduce workplace organizational stress and trauma for PSWs. Among the few studies found, efficacy studies support their use to reduce mental ill-health, and components for effective implementation were identified. The findings from this review highlight the limited number of studies that explored the use and effectiveness of PSPs for this group of workers. It is also noted that this review did not find studies that explored this intervention among firefighters or EMTs. This is consistent with other studies about peer support, suggesting that more evidence-based studies are needed to support its use and effectiveness among workers for mental health support (Creamer et al., 2012). Although limited, the results of this review have identified important findings that might be useful to consider as organizations look to develop and evaluate PSPs, especially for workers in the public safety sector, including COs.
The findings were explored through the lens of the SEM to identify areas that may affect the utilization and use of PSP. The model supports multilevel influences that may affect its use. Peer support programs as an intervention are heavily influenced by the interpersonal relationship between peers; however, it is also evident that organizational-level factors, including policy, practices, and funding, are needed to have such programs available. Finally, societal influences such as public stigma also affect the use of PSP among PSWs.
Health Outcomes
Peer support programs were shown to affect health outcomes, including improved mental health literacy, normalization of PTSD symptoms, and decreased stigma. Mental health literacy has been described as the knowledge about mental health disorders that aid in their recognition, management, and prevention (Jorm et al., 2000). Peer support programs provide an opportunity to share the lived experience, which may increase the awareness and understanding of mental health conditions and available resources. Mental health literacy skills may also help to reduce stigma-related barriers to mental healthcare among PSWs, including veterans (Williston & Vogt, 2022).
Normalization of PTSD symptoms through PSP was also described as a positive health outcome. Participants described how they were able to change how they think about trauma, knowing that some of experiences were common among others (Hundt et al., 2015). Peer support program provided social support to address social isolation that may accompany PTSD. Other PSWs described the process of understanding their symptoms and learning to manage them with support networks and coping strategies (Kumar et al., 2019).
Implementation Needs
Organizational support is necessary for the success and sustainability of PSPs. Peer support programs with leadership support, policies, and practices and PSP mentor training are more likely to become established in the organization. Leadership and administrative support are of particular importance because of the top-down style of management that is common in public safety sector professions. Initiatives supported by administrators may help to validate their use within the organization. It also demonstrates a culture of caring in the workplace. A recent study about PSPs to reduce occupational stress found that workers who had received support from immediate supervisors perceived high support from the entire organization (Agarwal et al., 2019). Participatory action research (PAR) is an approach that was also shown in this review to engage workers and managers in the development of a peer mentoring program. Namazi et al. (2021) found that engaging key stakeholders such as administrators, supervisors, and COs increased peer mentoring participation. This was also described in a study by Kotejoshyer et al. (2021), which supported PAR with TWH principles as an effective method of engaging union members with management and COs to establish and implement a peer mentoring program. This approach should be considered when exploring PSPs as an intervention.
Policies and practices, which fall under the scope of organizational support, help to sustain PSPs. Policies that formalize PSPs by providing written guidelines validate the program as essential to the organization. These policies should also include the ability to attend a PSP without repercussions to their job. Union support in the development of a PSP may also help to lend legitimacy of its use with PSWs while also providing protections for workers who seek PSPs for the management of work-related stressors. Protections such as privacy, confidentiality, and nondisclosure should be considered in policies about PSP participation. Practices within the organization that highlight and support PSPs as an accepted intervention would contribute to its viability. Peer support programs should be discussed during the orientation and training programs with COs that may help normalize these programs as part of the work culture. Creamer et al. (2012) found that peer support should not be limited to critical incidents but be part of routine employee healthcare.
The selection and training of peer leaders require organizational support. Peer support program leaders must be credible, trusted co-workers of equivalent rank. Creamer et al. (2012), in a study aimed to develop guidelines for peer support in high-risk organizations, found that peer support leaders should be a member of the target population with experience in the field of work. It also recommended that these leaders undergo a formal application and selection process. Training should include skills to facilitate groups effectively, share lived experiences, and identify the need for referral to professional mental health resources and services.
Finally, organizational support is needed to address the innate stressors of the work such as staffing issues, scheduling, heavy workload, and lack of administrative support. Without this support, programs designed to reduce stress and trauma, including PSPs, may not be utilized despite efforts to develop and implement them.
Stigma was identified as a barrier to help-seeking for mental health issues. Perceived public stigma is a recognized barrier that affects individuals from engaging in mental healthcare (Parcesepe & Cabassa, 2013). It is often one of the reasons that people who might benefit from mental health services may refrain from using them (Corrigan et al., 2014). Public stigma, which becomes internalized by the individual as self-stigma, has been inversely associated with help-seeking behaviors (Corrigan, 2004). Ricciardelli and colleagues (2018) suggested that COs may describe needing mental health services but may not seek assistance because of a fear of stigmatization. Furthermore, COs’ fear of disclosure makes it difficult for them to support or receive support for mental health needs. While this presents a significant challenge, one study in this review found that once participants engaged in a PSP, the concern of stigma was decreased (Goldstein, 2005). Identifying ways to engage COs in discussions about mental health may help to normalize mental health interventions such as PSPs and improve mental health literacy. A PAR approach to developing a PSP may help engage COs in a nonthreatening manner, which may increase acceptance, normalize mental healthcare, and decrease stigma.
Peer support programs are a promising intervention to consider for addressing the mental health concerns of COs. Peer support programs provide the benefit of normalizing experiences through a shared lived experience. They increase understanding and foster empathy and compassion among participants, which helps build resilience and hope. Resilience may serve as a protective factor against the development of mental disorders (Shrivastava & Desousa, 2016). It may also help the individual by enhancing their ability to cope with unforeseen events, lessening the impact of trauma.
There are currently challenges to accessing formalized mental health services in the United States due to shortages of qualified providers limiting access and availability. Mental health support in the form of PSP might fill a needed gap in services. In some instances, PSPs may be preferable to formal sources of help such as medical providers or mental health counselors. Peer support programs can be a first step in help-seeking that is accessible to the COs. It is possible that participation in a PSP may be adequate to buffer work-related stress and build resilience and hope. However, if additional mental health services are needed, then the peer support leader can assist with referrals. This makes PSPs a comfortable entry point to mental health services.
While PSPs have been described for other PSWs, there is a paucity of studies exploring mental health interventions for COs. This review captured what is known about PSPs for COs and expanded it to include other PSWs to fully explore PSP use, effectiveness, facilitators, and barriers. The scope of the review was broad and may be considered a limitation of this article. However, it was designed to capture a wide range of studies that explored PSPs for PSWs. This review provides a comprehensive overview of the evidence available on this emerging topic. The findings of this study were used to develop a national survey disseminated to COs in the United States from December 2021 to April 2022 to explore awareness, use, and helpfulness of PSPs; stigma related to participation in PSPs; and facilitators and barriers to PSP use. This survey will help discover what is known about current work-related PSP practices to reduce stress and trauma for COs in the United States (Stewart et al., 2022).
Implications for Occupational Health Nursing Practice
Occupational health nurses are in a unique position to address the mental health needs of workers. Mental health concerns have been growing over the past 2 years partly due to the COVID-19 pandemic and the numerous stressors that have been placed on workers (Office of the U.S. Surgeon General, 2022). The NIOSH Centers of Excellence for TWH program has identified supporting mental health in the workplace as a priority area to advance worker well-being (NIOSH, 2021). The National Institute for Occupational Safety and Health recommends developing workplace policies, programs, and practices that support mental health to provide a psychosocially safe workplace. Peer support programs are an approachable mental health intervention that may assist workers to reduce work-related stress and build resilience. More research is needed to determine PSP use and effectiveness, including facilitators and barriers. As worker advocates, occupational health nurses are well suited to lead efforts to explore PSP efforts in their organizations.
Attribution, Nonendorsement
Total Worker Health is a registered trademark of the U.S. Department of Health and Human Services (HHS). Participation by authors does not imply endorsement by HHS, the Centers for Disease Control and Prevention, or the National Institute for Occupational Safety and Health.
In Summary
Peer support programs are potential resources to address mental health concerns of COs in the workplace.
Organizational support, thoughtful selection of peer support leaders along with a commitment of trust and confidentiality among peers are essential to PSP.
Occupational health nurses who serve PSWs are a position to address mental health issues and provide resources to address stress and trauma.
Footnotes
Author Contributions
Pamela Fallon: Conception, design, and analysis, as well as revisions.
Mazen El Ghaziri: Conception, design, and analysis, as well as revision of the manuscript.
Lisa A. Jaegers: Conception, design, and analysis, as well as revision of the manuscript.
Yuan Zhang: Review and revision of manuscript.
Alicia G. Dugan: Review and revision of manuscript.
Martin Cherniack: Review and revision of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.