
Abstract
Background:
Emergency responders are the most frequent overdose responders, however, little is known about the impact of supervised injection facility (SIF) location on first responders. The purpose of this study was to determine whether firefighter/paramedic attitudes about being stationed near an SIF were related to burnout, secondary traumatic stress, and compassion satisfaction.
Methods:
Firefighter/paramedics from Vancouver Fire and Rescue Services (n = 54) completed an online survey. General linear models were used to assess differences in burnout, secondary traumatic stress, and compassion satisfaction based on attitudes regarding being stationed near an SIF while controlling for occupational stress.
Findings:
Firefighters with negative attitudes regarding station placement near an SIF experienced more burnout compared with those with neutral/mixed attitudes and less compassion satisfaction compared with those with positive attitudes. There were no differences between those with positive and neutral/mixed attitudes.
Conclusions:
These findings have implications for education and training of emergency responders stationed near SIFs. They also highlight the need for more research into the effects of and possible clinical opportunities needed to support first responders’ work near an SIF.
Application to Practice:
While these findings represent early exploratory evidence, increased burnout and reduced compassion satisfaction may be common reactions among first responders who experience negative attitudes toward SIFs. Prevention efforts could incorporate programs to enhance health and well-being of first responders and education regarding substance use and harm reduction, while workforce surveillance for signs of distress or burnout could be implemented to trigger additional mental health services and interventions. while policymakers should remain aware of SIF-related impacts on all stakeholders, including first responders.
Since the 1990s, the opioid epidemic has ravaged communities across North America (Myer & Belisle, 2018). Over 600,000 individuals in the United States and Canada have died from an opioid overdose since 1999, and, at this rate, 1.2 million more are expected to die of opioid overdose by 2029 (Humphreys et al., 2022). To mitigate harm caused by elevated opioid use, some communities have opened supervised injection facilities (SIFs). In 2003, Vancouver, British Columbia opened the first SIF in North America, which has had over 3.6 million visits since its inception (Vancouver Coastal Health [VCH], 2019). More recently, the United States opened its first SIF in New York City in 2021, with other U.S. cities, such as Philadelphia, San Francisco, and Seattle initiating steps to open sites as well (Mays & Newman, 2021).
Supervised injection facilities are locations that provide medical supervision to people who inject drugs (PWIDs; European Monitoring Centre for Drugs and Drug Addiction, 2018). These facilities follow a harm reduction model of care and address public health concerns surrounding injection drug use by reducing the negative consequences of drug use without requiring abstinence (International Harm Reduction Association, 2010). Evidence has shown that SIFs decrease overdose morbidity and mortality, prevent transmission of infectious disease, improve injection behaviors, encourage PWID to access health services, and reduce public drug use (Levengood et al., 2021; Marshall et al., 2011; Strike et al., 2014; Watson et al., 2012; Wood et al., 2005).
While the public health benefits of SIFs have been clearly demonstrated (Kennedy et al., 2019; Levengood et al., 2021; Marshall et al., 2011), debate over the legal and moral implications of these sites continues (Levengood et al., 2021). In addition, though emergency responders are the most frequent overdose responders (Cash et al., 2018), little is known about the impact of SIF implementation on first responders who respond to medical emergencies at these sites. In the event of an overdose, the SIF nurse and team are available to intervene, but a study of overdose events at Vancouver’s SIF from 2004 to 2008 found that 911 was called for 42% of overdose events (Milloy et al., 2008). Understanding first-responder well-being in SIF-serving communities is critical as they are important stakeholders and play a central role in addressing the opioid epidemic (Cash et al., 2018).
Limited research has found that police officers and emergency personnel who respond to a greater number of overdose calls tend to have more pessimistic attitudes toward drug treatment and naloxone (Murphy & Russell, 2020), and reports of burnout are high among those who frequently respond to overdose calls or regularly encounter PWID (Garner et al., 2007; Oser et al., 2013; Oyefeso et al., 2008; Pike et al., 2019). First responders commonly report experiencing trauma and grief in response to overdose calls (Shearer et al., 2019). In fact, previous qualitative research with first responders reveals they report increased stress, sleep problems, negative effects on family functioning, and increased drug stigmatization while working near SIFs (Pennington et al., 2021). Emergency service personnel also report safety concerns when considering SIF implementation due to previous experience with calls involving substance use (Perlmutter et al., 2023). Conversely, our previous qualitative analyses revealed that some first responders feel that working near an SIF can increase camaraderie among crew members and make them feel like they are making a positive difference (Pennington et al., 2021).
Previous research indicates that a marked difference in attitudes toward patients may result in mental health-related effects among first responders (Christodoulou-Fella et al., 2017; Koutra et al., 2022). For example, negative attitudes toward patients, including feelings of indifference, appear to be associated with secondary traumatic stress symptoms in nurses (Christodoulou-Fella et al., 2017). In addition, unfavorable attitudes toward mental illness are associated with higher scores on measures of emotional exhaustion, depersonalization, compassion fatigue, and burnout among mental health professionals (Koutra et al., 2022). Accordingly, further investigation is warranted into key outcomes, such as burnout and secondary traumatic stress, which appear to precede a host of psychopathology (Harr, 2013; Jo et al., 2018; Lourel et al., 2008).
For first responders, many stressors experienced in the line of duty are related to burnout and secondary traumatic stress (Cocker & Joss, 2016). Burnout results from chronic stress and typically includes symptoms, such as depression, exhaustion, and anger (Pike et al., 2019). More specifically, burnout resulting from occupational stress has been shown to be a predictor of post-traumatic stress disorder (PTSD) symptomatology (Jo et al., 2018; Lourel et al., 2008). Secondary traumatic stress refers to stress symptoms resulting from exposure to others’ trauma and includes symptoms, such as fear, intrusive thoughts, and avoidant behaviors (Stamm, 2010). Increases in work-related stress can impact individuals in a variety of ways, including increasingly negative cognitions, sleep disturbances, difficulty concentrating, decreased self-esteem, and thoughts of self-harm or harming others (Harr, 2013). In contrast, first responders may also experience compassion satisfaction, or the fulfillment one receives from providing care for others while on the job (Stamm, 2010). A component of compassion satisfaction is a sense of calling and fulfillment derived from participating in a meaningful job, which has been associated with lower levels of burnout (Hagmaier et al., 2013).
As the United States begins to establish more SIFs, our team sought to examine the down-stream impacts of this public health service on firefighters and paramedics serving these communities. Thus, the aim of the present study was to identify firefighter/paramedic attitudes about working near an SIF and determine whether these attitudes were related to occupational burnout, secondary traumatic stress, and compassion satisfaction, while controlling for overall occupational stress. We hypothesized that firefighter/paramedics with negative attitudes toward working near an SIF would experience greater burnout and secondary traumatic stress and less compassion satisfaction compared with those with positive attitudes.
Methods
Procedures
Approximately, 900 firefighters and paramedics were recruited from Vancouver Fire and Rescue Services via an email and follow-up reminder from their local fire service Union to complete an anonymous online questionnaire through Qualtrics, a secure web-based platform. Total study participation time averaged 25 minutes. Survey data were collected from 101 firefighters/paramedics (response rate: ~11.2%), of which 57 completed the free-response question. Three respondents had never worked a rotation at the station closest to the SIF (typically 1 year in duration, although some respondents indicated they completed multiple rotations), and thus were excluded, resulting in a sample size of 54 firefighter/paramedics. All study procedures were approved by Baylor Scott & White Research Institute’s Institutional Review Board (IRB). Participants provided consent electronically before completing the online survey by selecting “I agree” when asked if they agreed to take part in this research.
Measures
Demographics were collected, including age, sex, race, Aboriginal descent, years of education, relationship status, and military veteran status. Race was dichotomized to “white” and “non-white” due to low counts of non-White individuals. Relationship status was dichotomized to “single” and “married, engaged, or cohabitating.” Career-related information was collected, including rank, years in fire service, current station, and years since being stationed at Firehall 2 (the station closest to the Vancouver’s SIF) for those who were not currently stationed there but had been in the past.
The Professional Quality of Life Scale: Compassion Satisfaction and Fatigue Version 5 (ProQOL; Stamm, 2010) is a validated 30-item self-report measure that includes three 10-item subscales: compassion satisfaction, burnout, and secondary traumatic stress. Each item assesses how frequently respondents have experienced symptoms in the last 30 days in their current work situation. Items are rated on a 5-point Likert-type scale (1 = never to 5 = very often). Raw scores for each of the three subscales were converted to t-scores with a mean of 50 (SD = 10). In the present study, alpha coefficients for internal consistency for each subscale were 0.86 (compassion satisfaction), 0.80 (burnout), and 0.89 (secondary traumatic stress). These are similar to alpha coefficients reported by Stamm (2010): 0.88 (compassion satisfaction), 0.75 (burnout), and 0.81 (secondary traumatic stress).
The Sources of Occupational Stress (SOOS-14; Kimbrel et al., 2011) scale is a 14-item self-report measure adapted from Beaton and Murphy’s (1993) SOOS scale designed to assess occupational stressors in firefighters and paramedics. The SOOS-14 is an abbreviated version of the original 57-item measure. Participants indicate how bothered they have been by various sources of on-the-job stress (e.g., thoughts about past runs, conflicts with co-workers, disruption of sleep, discrimination) experienced during the last 10 shifts they worked. Items are rated on a 5-point Likert-type scale (1 = not at all bothered to 5 = extremely bothered). Item scores were summed for a total score ranging from 14 to 70 with higher scores indicating higher levels of occupational stress. The SOOS-14 has been shown to have good internal consistency (α = .82) and moderate test–retest reliability (r = .51, p < .001) (Kimbrel et al., 2011, 2015). In the present study, the alpha coefficient for internal consistency was .86.
A free-response question queried participants’ feelings about being assigned to the station near the SIF. This question asked, “How do you feel about being mandated to be stationed at Firehall 2 in Downtown Eastside at [Street Address]?” This question was developed with input from firefighter collaborators from both Vancouver Fire & Rescue Services and other departments. Two of the authors coded all responses for overall attitude (“positive,” “negative,” or “neutral/mixed”) independently in Microsoft Excel. Inter-rater reliability was calculated, and raters had a high level of agreement (κ = 0.91).
Statistical Analysis
Data were analyzed using SAS v9.4 (English). Descriptive statistics were used to describe the sample’s demographic and occupational characteristics. Fischer’s exact tests were used to compare demographic and occupational characteristics by attitude group for categorical variables, and one-way analysis of variance (ANOVA) tests were used to compare demographic and occupational characteristics by attitude (positive, negative, or neutral/mixed) for continuous variables. General linear models (GLMs) were used to assess differences in burnout, secondary traumatic stress, and compassion satisfaction based on attitude (positive, negative, or neutral/mixed). Occupational stress was then entered as a covariate in subsequent analyses. Post hoc comparisons were made using Scheffe’s test. Independent t-tests were conducted to identify any differences on burnout, secondary traumatic stress, and compassion satisfaction scores between first responders who were currently or previously stationed at Firehall 2.
Results
The demographics of respondents were consistent with those of fire service, with the majority being White (92.5%) males (98.1%). On average, respondents were 42.9 (SD = 8.3) years old and had completed 14.5 (SD = 2.3) years of education. A majority of respondents were ranked as firefighter/paramedic (57.4%), and the average respondent had served 16.1 (SD = 7.9) years in fire service. Respondents were predominantly married, engaged, or cohabitating (88.9%), and 9.3% were military veterans. Ten participants were currently stationed at Firehall 2, 43 were previously stationed at Firehall 2, and one participant did not provide information on current station (M = 3.7 years ago, SD = 2.9, range: 0.5–12.0). This is consistent with staffing policies that require firefighters to be assigned to Firehall 2 for 1 to 3 years before rotating to a different assignment. Approximately, 26% of respondents fell into the negative attitude group; the remaining majority of participants fell into the neutral/mixed (48%) and positive attitude groups (26%) (Table 1).
Demographic and Occupational Characteristics of Firefighter/Paramedics (n = 54)
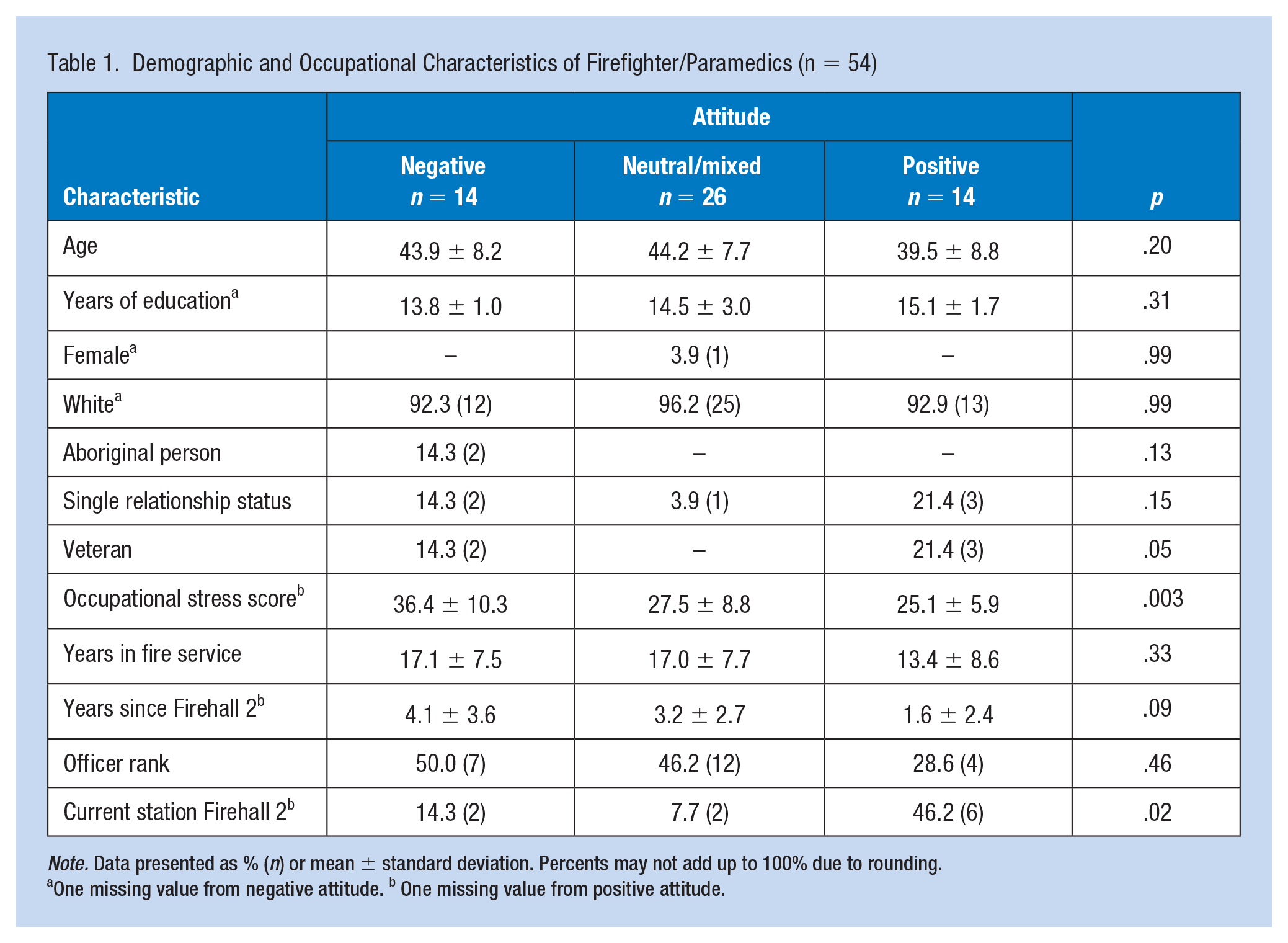
Note. Data presented as % (n) or mean ± standard deviation. Percents may not add up to 100% due to rounding.
One missing value from negative attitude. b One missing value from positive attitude.
General linear models revealed significant differences in burnout, secondary traumatic stress, and compassion satisfaction scores by attitude group (positive, negative, or neutral/mixed). There was a statistically significant difference in burnout, F(2,51) = 10.80, p < .001, η2 = .30, secondary traumatic stress, F(2,51) = 8.11, p < .001, η2 = .24, and compassion satisfaction, F(2,51) = 8.42, p < .001, η2 = .25, scores between attitude groups (Table 2). Post hoc comparisons indicated that burnout scores were significantly higher among those with negative attitudes (M = 59.82, SD = 11.25) compared with those with positive (M = 46.27, SD = 6.46, p < .001) or neutral/mixed attitudes (M = 47.91, SD = 8.22, p < .001). Secondary traumatic stress scores were also significantly higher among those with negative attitudes (M = 58.91, SD = 11.66) compared with those with positive (M = 45.21, SD = 6.53, p = .001) or neutral/mixed attitudes (M = 49.38, SD = 9.19, p = .013). Conversely, compassion satisfaction scores were significantly lower among those with negative attitudes (M = 40.76, SD = 8.67) compared with those with positive (M = 54.87, SD = 8.11, p < .001) or neutral/mixed attitudes (M = 48.77, SD = 9.86, p = .038). Burnout, secondary traumatic stress, and compassion satisfaction scores did not differ significantly between those with positive attitudes and those with neutral/mixed attitudes. In addition, there were no significant differences on scores between those currently stationed at Firehall 2 and those stationed there in the past.
Firefighter Attitudes and Burnout, Secondary Traumatic Stress, and Compassion Satisfaction
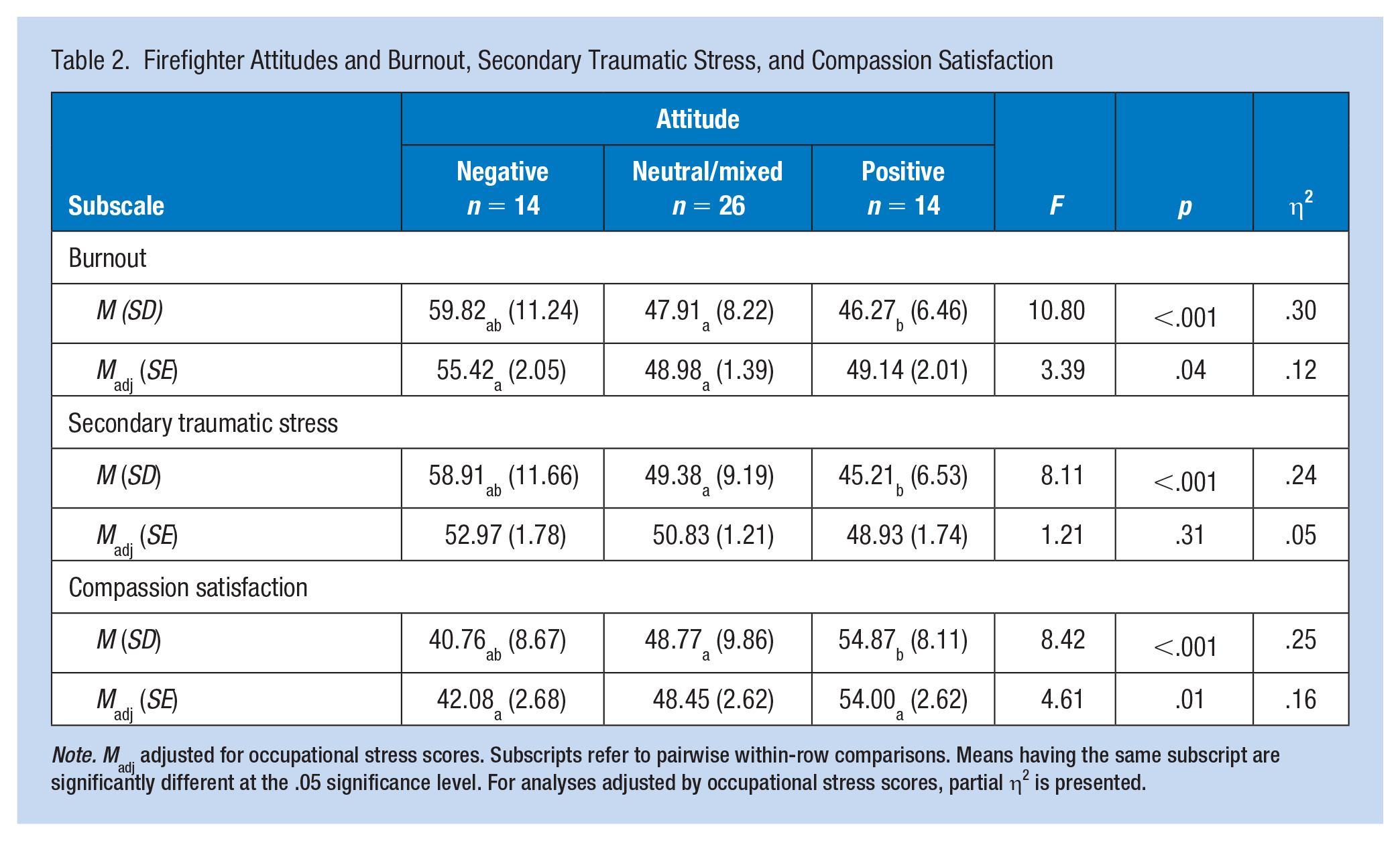
Note. Madj adjusted for occupational stress scores. Subscripts refer to pairwise within-row comparisons. Means having the same subscript are significantly different at the .05 significance level. For analyses adjusted by occupational stress scores, partial η2 is presented.
After adjusting for levels of occupational stress, a GLM revealed significant differences in burnout, F(2,49) = 3.39, p = .04, partial η2 = .12, and compassion satisfaction, F(2,49) = 4.61, p = .01, partial η2 = .16, by attitude group. See Table 2. In addition, there was a statistically significant relationship between occupational stress and burnout scores (p < .001), in which occupational stress explained 37% of variance in burnout (partial η2 = .37). After adjusting for occupational stress, there was no significant difference between the three attitude groups on secondary traumatic stress; however, there was a statistically significant relationship between occupational stress and secondary traumatic stress scores (p < .001), in which occupational stress explained 59% of variance in secondary traumatic stress (partial η2 = .59). After adjusting for occupational stress, post hoc comparisons indicated that burnout scores were significantly higher among those with negative attitudes (M = 55.42, SE = 2.05) compared with those with neutral/mixed attitudes (M = 48.98, SE = 1.39, p = .05). Conversely, compassion satisfaction scores were significantly lower among those with negative attitudes (M = 42.08, SE = 2.68) compared with those with positive attitudes (M = 54.00, SE = 2.62, p = .01).
Discussion
Our hypothesis that firefighters with negative attitudes toward working near an SIF would report higher levels of burnout and secondary traumatic stress and lower levels of compassion satisfaction relative to those with positive attitudes while controlling for general occupational stress was partially supported. Before adjusting for occupational stress, those with positive and neutral/mixed attitudes reported lower levels of burnout, secondary traumatic stress, and higher levels of compassion satisfaction compared with those with negative attitudes, while those with positive and neutral/mixed attitudes reported similar levels of all outcome variables. However, after controlling for general occupational stress, those with neutral/mixed attitudes reported lower levels of burnout, and those with positive attitudes reported higher levels of compassion satisfaction compared with those with negative attitudes. While there was not a statistically significant difference on burnout scores between those with positive attitudes and negative attitudes, the adjusted mean burnout score for those with positive attitudes is quite similar to the adjusted mean burnout score for those with neutral/mixed attitudes. All other pairwise comparisons became nonsignificant. Because of the cross-sectional nature of this study, we cannot determine the direction of the relationship between attitudes and the outcomes.
As more U.S. cities seek to establish SIFs, these results have important implications for enhancing mental health and well-being of first responders stationed near SIFs. First, while these findings represent early exploratory evidence, policymakers should remain aware of SIF-related impacts on all stakeholders, including first responders, when considering implementation of new SIFs to guarantee a healthy and adequately prepared first-responder workforce. Future research should employ a more rigorous study design to further understand potential policy implications. Second, mental health programming specific to overdose response-related stressors and traumatic exposures should be explored. This is important because focus group research among substance abuse counselors has indicated that burnout leads to poorer quality clinical care; thus, high levels of burnout among first responders would likely affect the quality of their work as well (Oser et al., 2013). Substance abuse counselors in Oser et al.’s (2013) study indicated that co-worker support and self-care were important strategies for preventing burnout. Thus, peer support and self-care may be important components to be considered for programming. Furthermore, in our previous qualitative report on firefighter/paramedic perspectives of working near an SIF, first responders emphasized the importance of limiting the duration of their assignment at Firehall 2 to mitigate negative effects on physical and mental health (Pennington et al., 2021). Finally, in a previous study emergency service personnel reported safety concerns when considering SIF implementation due to previous experience with calls involving substance use (Perlmutter et al., 2023). Protection from harm at work is a key component of the U.S. Surgeon General’s Framework for Workplace Mental Health & Well-Being (U.S. Office of the Surgeon General, 2022). Supervised injection facility-related safety concerns should be minimized as workplace violence, operationalized as verbal or physical threats or assault in this study, has been shown to be associated with PTSD, depression, and anxiety among first responders (Setlack et al., 2021).
Programs to destigmatize substance use and promote education regarding substance use and the harm reduction model could also minimize negative outcomes among first responders and increase compassion satisfaction. Recently, Strike et al. (2014) reported that the majority of police in their study were skeptical of the SIF-model and the harm reduction approach. However, a qualitative study among first responders regarding stigmatization related to opioid use and harm reduction proposed that educating first responders on the benefits of a harm reduction approach and providing trauma-informed training may increase compassion satisfaction (Knaak et al., 2019).
This study has several strengths: (a) it is the first study to examine first-responder attitudes, burnout, secondary traumatic stress, and compassion satisfaction related to working near an SIF and (b) it further examines the relation between the opioid crisis and first responder well-being. Limitations must be noted as well. One limitation of this study is the small sample size. These data are derived from a small sample, and attitude was determined from a single, self-reported, free-response question. This in addition to the low response rate (~11.2%), limits our ability to draw statistical conclusions based on length of assignment at Firehall 2. There is a potential for recall bias as respondents were stationed at Firehall 2 up to 12 years ago. However, participant anonymity and consistency in response themes in our previous report (Pennington et al., 2021) increases our confidence that these findings accurately capture first-responder attitudes toward working near the SIF in Vancouver. In addition, our sample lacked demographic diversity. Although this reflects the demographics of fire service, it is possible that varying demographic populations may have differing views. Finally, the cross-sectional nature of the study restricted our ability to assess for temporal relationships between station assignment and burnout, secondary traumatic stress, and compassion satisfaction. Future research should employ a more rigorous design with a larger sample size to further examine these effects.
Implications for Occupational Health Practice
This is the first exploratory study to examine how attitudes regarding working near an SIF relate to burnout, secondary traumatic stress, and compassion satisfaction among first responders who serve these communities. Although more research is needed, this study suggests that burnout and reduced compassion satisfaction may be experiences that are more common for first responders who experience negative attitudes toward SIFs. However, it also suggests that those with positive or even potentially neutral/mixed attitudes can experience greater compassion satisfaction while being stationed near an SIF.
As such, this study represents an important step toward targeted assessments of experiences and anticipation/amelioration of novel challenges in this occupation. These results also have important implications for developing programs to enhance mental health and well-being of first responders stationed near SIFs as these harm reduction facilities become more common in the United States. Results of this study indicate that programs to destigmatize substance use and promote education regarding the harm reduction model could minimize negative outcomes among first responders and increase compassion satisfaction from the job. Prevention and intervention efforts could include mental health programming specific to overdose response-related stressors. Finally, this study adds valuable perspective to ongoing discussions regarding clinical utility and implications of SIFs. An accurate understanding of the risks and benefits of SIFs for all stakeholders, including first responders, is vital to productive policy discussions and decision-making, especially in the United States.
Applying Research to Occupational Health Practice
First responders in this study who endorsed negative attitudes toward working near a supervised injection facility (SIF) also endorsed higher levels of burnout and lower levels of compassion satisfaction compared with those who endorsed positive or neutral/mixed attitudes. Previous research in other substance use-related settings suggests that burnout leads to worse quality clinical care (Oser et al., 2013), so it is important to mitigate these impacts. SIF-related policy should account for the possibility of these occupational hazards; one policy-level change suggested by several respondents in a previous report from this sample (Pennington et al., 2021) was to limit length of assignment near an SIF. In addition, this research indicates that mental health programming specific to overdose response-related stressors and programs to destigmatize substance use and educate on harm reduction could minimize negative outcomes among first responders and increase compassion satisfaction derived from the job.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
All study procedures were approved by Baylor Scott & White Research Institute’s IRB on July 10, 2018 (IRB# 018-546).