
Abstract
Medical interpreters play a vital role in fostering understanding and ensuring safety and transparency in healthcare for patients with non-English language preference. Limited research describes work-related experiences of medical interpreters. The purpose of this research was to explore perceptions of occupational health and safety among medical interpreters. A structured, online survey was administered to all certified medical interpreters in Hawaii, New York, New Jersey, California, and Texas. Participants described occupational experiences as an interpreter via an open-ended question. Responses were coded using qualitative thematic analysis. Response text was reviewed, a codebook of descriptive themes developed, and data thematically coded and summarized. Of 981 potential participants, 199 responded (20.3% response rate). Four main themes were identified: Professionalism and Role, Work-Related Challenges, Approaches to Mitigate Vicarious Trauma, and The Rewarding Nature of the Job. Respondents described compassion fatigue, vicarious trauma, intentional emotional distancing from clients, and loneliness. Respondents identified needs for workplace support to ensure professionalism and safeguard interpreter safety. Medical interpreters appreciate their work, yet face challenges, including compassion fatigue and vicarious trauma. Employers and healthcare institutions should support the occupational and emotional needs of medical interpreters as a vital member of the healthcare team.
Background
Spoken language medical interpreters play a vital role in healthcare for thousands of patients with non-English language preference (NELP) or those who prefer a non-English language with respect to a particular type of service, benefit, or encounter (Ortega et al., 2022). In the United States, 66 million people, or 21.5% of the population aged 5 years and older, speak a language other than English at home, of whom 38.3% identify as speaking English less than “very well” (United States Census Bureau, 2020). Medical interpreters service use is associated with increased patient satisfaction and comprehension as well as improved clinical outcomes (Diamond et al., 2019; Karliner et al., 2007; Lindholm et al., 2012; Lor & Martinez, 2020). Interpreter services are linked to improved ability to provide and understand informed consent (Lee et al., 2017). Without interpreter services, patients with NELP receiving end-of-life care experience more pain, anxiety, and have a lower understanding of their prognosis than patients who have an interpreter (Silva et al., 2016). Available data, albeit sparse, suggest that professional medical interpreter services present benefits for improved patient care that outweigh the relatively low costs of providing the service (Brandl et al., 2020).
Professional medical interpreters in the United States may obtain credentials through the Certification Commission for Healthcare Interpreters (CCHI) or the National Board of Certified Medical Interpreters (NBCMI), which require 40 hours of formal training, dual language proficiency, and demonstrated knowledge of medical concepts and terminology, ethics, and standards of practice. Some states, like Washington, have interpreter testing and credentialing programs (Washington State Coalition for Language Access & Tools for Health, 2015), as do many health systems for staff or contract interpreters. Medical interpreter training programs are offered through many higher education institutions (typically as community education offerings), by some language professional associations, and other organizations. However, medical interpreters in the United States are not required to obtain formal certification or even specific training. As a result, some receive very little formal training prior to working as a medical interpreter.
The right to language access in healthcare has long been established, originating with Title VI of the Civil Rights Act of 1964, which included a ban on national origin discrimination, of which language can be an identifier (United States Department of Justice, 2020). The first guidance specifically concerning language access responsibilities for entities that receive federal funds from any source was established via Executive Order 13166 in 2000 (Presidential Executive Order 13166, 2000). Section 1557 of the Patient Protection and Affordable Care Act and the Final Rule of 2020 delineate specific competencies required of medical interpreters for patients with NELP (U.S. Department of Health and Human Services, 2016; U.S. Department of Health and Human Services & Centers for Medicare and Medicaid Services, 2020). These rules and regulations serve to improve access to quality of services and drive demand for and utilization of interpreter services. While demand for medical interpretation has increased over time, interpreter workforce shortages, especially during the COVID-19 pandemic, initiated delays in services and low-quality care (Aitken, 2019; Knodel, 2018).
Medical interpreters often work on-demand in fast-paced healthcare settings. Within similar professions like social work and nursing, burnout, compassion fatigue, and secondary trauma can be common (Alhawamdeh & Zhang, 2021; Ondrejková & Halamová, 2022). Interpreters in non-medical settings also experience traumatic work situations, with burnout and compassion fatigue commonly observed (Kindermann et al., 2017; Mehus & Becher, 2016). A 2016 online survey of 119 spoken language interpreters (employed across all sectors) indicated high levels of compassion satisfaction and secondary traumatic stress but average levels of burnout (Mehus & Becher, 2016). Still, further research suggests that translators experience high levels of stress stemming from perceived unfair treatment from agencies, low pay, and uncertainty about the future (Courtney & Phelan, 2019). Despite these challenges, however, translators reported high levels of job satisfaction (Courtney & Phelan, 2019).
Within the healthcare setting, interpreters face tense, high-pressure situations that may contribute to elevated rates of stress, burnout, or compassion fatigue. Indeed, a qualitative, interview study of seven mental health sign language interpreters in England reported themes consistent with compassion fatigue (Zafirah et al., 2020), as did a small study of 15 hospital-based medical interpreters conducted in 2011–2012 (White, 2012). To our knowledge, beyond these small studies, none have explored the work-related experiences of medical interpreters specifically. The purpose of the current study is to explore factors contributing to perceptions of occupational health and safety among medical interpreters.
Methods
Study Design
This study utilized open-ended survey response data and qualitative thematic analysis to explore perceptions of occupational health and safety among medical interpreters in the United States. This research was deemed exempt from human subjects review by an Institutional Review Board.
Participants
The sample consisted of all certified medical interpreters in the online registry for NBCMI from the five states with the highest percentage of individuals who reported speaking English “less than very well” in the U.S. Census: California, Hawaii, New Jersey, New York, and Texas (United States Census Bureau, 2015). Interpreter names, email addresses, state, and language for which each participant provided interpreting services (Spanish, Cantonese, Mandarin, Russian, Korean, and Vietnamese) were obtained from the online registry for the NBCMI, one of the two interpreter certification boards in the United States. (Contact information was not available for interpreters certified through the CCHI.)
Survey Content and Administration
The present study is part of a larger study focused on interpreter’s professional quality of life. As part of the larger study, an anonymous, online survey was administered, and it included a professional quality of life battery and an open-ended question asking respondents to describe their work as an interpreter. Participants were asked, “Is there any additional information you wish to share about your work as a spoken language medical interpreter? (Please respond in the text box below. Write as little or as much as you’d like.)” Responses to the open-ended question, which were extensive, are the sole focus of the present study. Participants were encouraged to include any comments they deemed important (without word limits).
The survey was administered via email using Qualtrics, an online survey software, from November 2019 to January 2020. An initial invitation to participate was distributed to all potential participants and contained information about and a link to the survey. Non-respondents received up to three reminder messages. The survey and all correspondence were in English and were anonymous.
Analysis
Qualitative responses to the open-ended question on professional experiences were analyzed using the codebook approach for the thematic analysis described by Braun and Clarke, which allows for flexibility, rigor, and transparency (Braun & Clarke, 2022). Text responses were reviewed by two authors (JG and NR), and ideas for general codes were developed inductively, which was appropriate given the open-ended nature of the prompt. Both authors assigned codes to the text, which were then grouped by themes. A codebook of descriptive themes and subthemes was developed, utilized, and, when needed, modified iteratively. To increase rigor and reliability, all text was double-coded by both researchers. Coding discrepancies were resolved through mutual discussion and consensus.
Results
Of the 981 potential participants, 199 responded (20.3% response rate) to the survey, of whom 55 respondents completed the open-ended question. Table 1 summarizes respondent demographics. Most survey respondents were female (69.6%), from California (59.3%), and provided Spanish interpreting services (77.5%). Approximately half of the respondents were 41 to 65 years old and had been a medical interpreter for 6 to 15 years. One respondent now lived in Colorado (see footer, Table 1).
Demographic and Employment Characteristics of Medical Interpreter Participants From California, New Jersey, New York, Texas, and Hawaii, 2019 (N = 55)
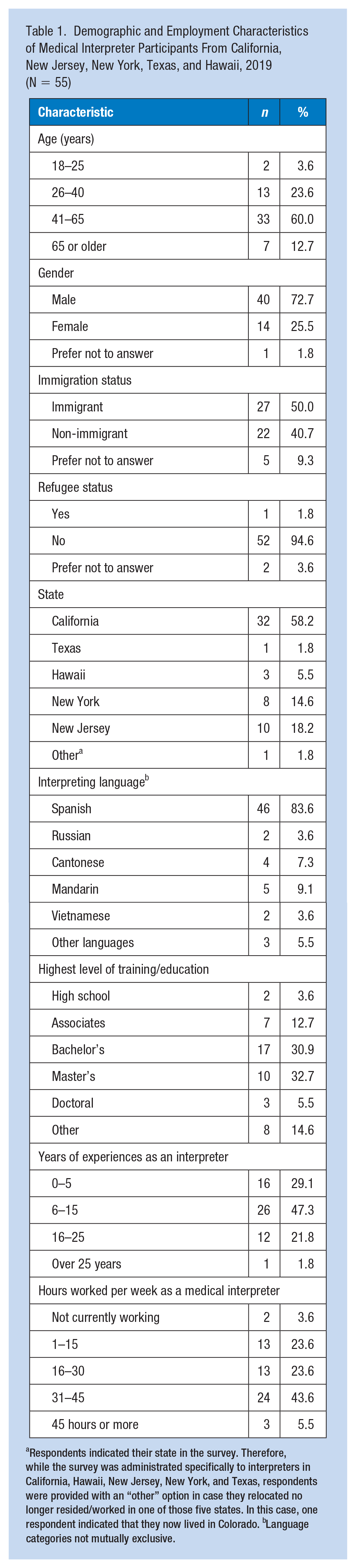
Respondents indicated their state in the survey. Therefore, while the survey was administrated specifically to interpreters in California, Hawaii, New Jersey, New York, and Texas, respondents were provided with an “other” option in case they relocated no longer resided/worked in one of those five states. In this case, one respondent indicated that they now lived in Colorado. bLanguage categories not mutually exclusive.
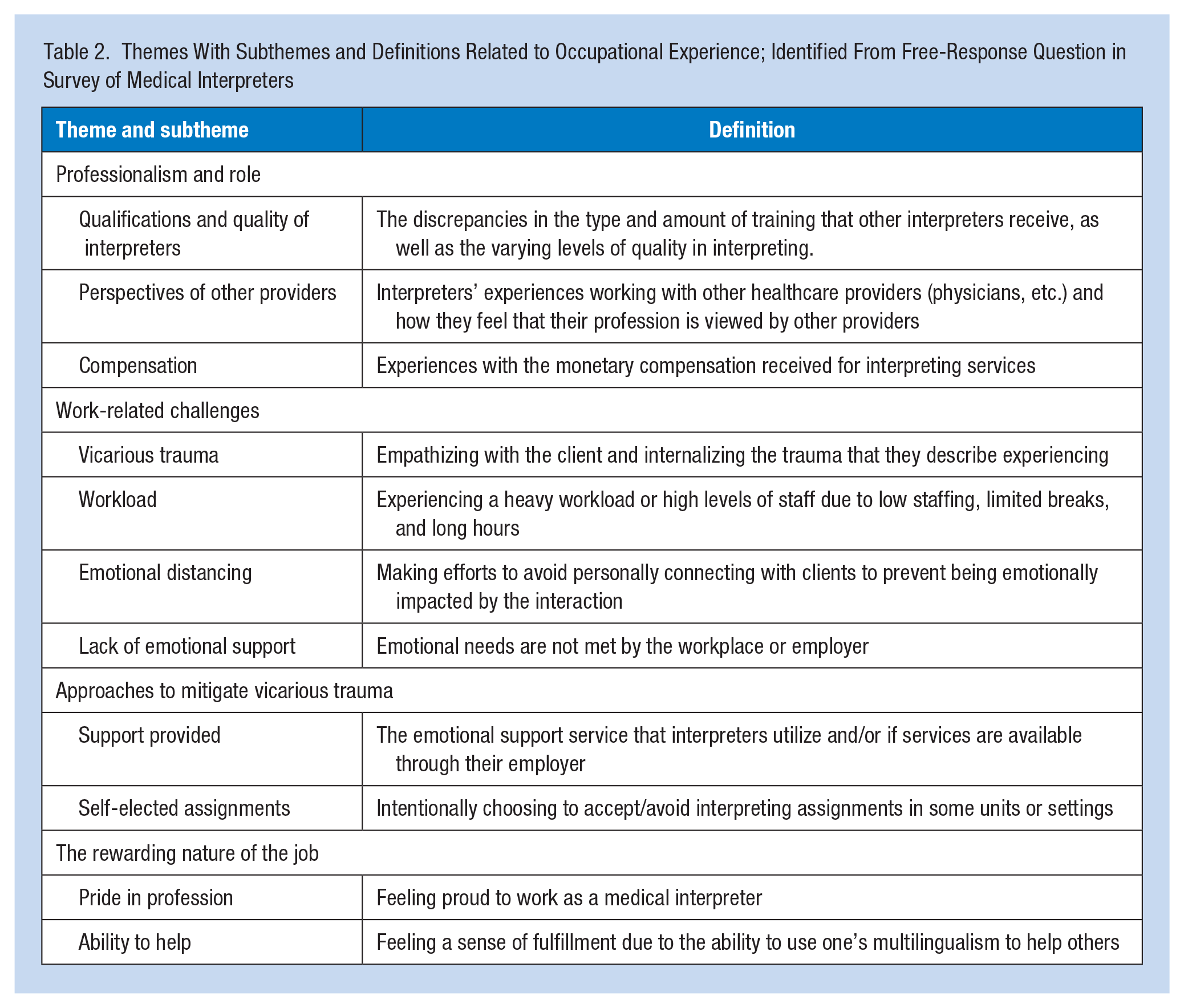
Four primary themes emerged in the text responses: Professionalism and Role, Work-Related Challenges, Approaches to Mitigate Vicarious Trauma, and The Rewarding Nature of the Job. Each theme and relevant subthemes within each domain are described below and summarized in Table 2.
Themes With Subthemes and Definitions Related to Occupational Experience; Identified From Free-Response Question in Survey of Medical Interpreters
Professionalism and Role
Professionalism and Role included ways in which interpreters felt that their profession is perceived by others, regard for their work, and skills and abilities of other interpreters. This theme was comprised of three subthemes: Compensation, Qualifications and Quality of Interpreters, and Perspectives of Other Providers.
Compensation
Respondents discussed challenges in receiving sufficient and fair pay for their interpreting services. Some felt that their compensation was not enough to meet their financial needs. One respondent shared that “where I live it’s very difficult to make a living doing nothing but medical interpreting.” Respondents also emphasized that the level and quality of services that they provide as interpreters is not reflected in their pay; one respondent stated that the “pay does not match the professional certified interpreter.” Respondents conveyed that fair and sufficient compensation is a concern and challenge among medical interpreters.
Perspectives of Other Providers
Respondents elaborated on their experiences of working alongside healthcare providers and how they felt that their profession is regarded by other healthcare professionals. They also perceived providers’ frustration and impatience due to patients taking time to answer questions or lack of understanding. Respondents explained that some patients with NELP have little education and that their responses to providers’ questions were influenced by cultural differences. This may result in patients giving long responses or the interpreter having to take the time to translate the provider’s query or explanation at a level that the patient can understand. Respondents expressed that as interpreters, they are often overlooked and their role is sometimes misunderstood by other healthcare team members. As one respondent shared, “One of the most frustrating issues for a Medical Interpreter is not to be considered as part of the team and are sometimes taken for granted and made to feel disrespected.” Some also emphasized specific challenges related to interactions with providers. One respondent stated, Providers: some of them to do not know their roles in the session. They do not know how to manage or control the three-people conversations, especially when patient’s relatives are involved in the conversation. It makes interpreters feel bad and tired.
Qualifications and Quality of Interpreters
Respondents discussed a lack of mandated, universal qualifications and training requirements to work as a medical interpreter, and how this results in discrepancies in the quality of interpreting services. The respondents emphasized that while they are Certified Medical interpreters, there are some individuals working as interpreters who do not undergo any formal training or credentialing. The quality of interpreting thus greatly varies between professional and credentialed interpreters and those with less training and experience. One respondent shared, The level and quality of interpreters in this field are different. It required not only the language skill and accuracy, but also the caring, patience, intelligence, and time management. But nowadays medical interpreters are under paid because most of the jobs don’t required certified, instead, they have plenty of bilingual staffs. So the quality is not in control.
Respondents also stressed that the less experienced and undertrained interpreters reflect poorly on the professional medical interpreter community’s work. A participant shared, “What I don’t like is the lack of transparency and responsibility of the some of the agencies I have worked with due to dishonest pay and hiring incompetent interpreters who undermine my professional standard of work.” Another respondent shared a similar sentiment: “They allow people to interpret for patients with only 40 hours of class and they are called ‘qualified’. It is a disgrace to our profession. We should make it a NATIONAL LAW to use ONLY certified medical interpreters” (Respondent’s emphasis).
Work-Related Challenges
Another prevalent theme in the responses was the work-related challenges that interpreters face. These challenges affect the interpreters emotionally and physically in both their professional and personal lives. This theme encompassed four subthemes: Vicarious Trauma, Emotional Detachment, Lack of Emotional Support, and Lack of Workplace Support.
Vicarious Trauma
Several respondents discussed the vicarious trauma that they experienced through their work as a medical interpreter. Vicarious trauma is the psychological distress that healthcare professionals who work with traumatized patients can experience (Lai et al., 2015). Because interpreters work so closely with patients and translate their words to the provider, often using “I” statements, they are susceptible to vicarious trauma. Respondents reflected on interpreting for patients and families in traumatic situations, such as discussing autopsy results and extubations. Others described how they find themselves internalizing traumatic events that they witness while working as an interpreter, and how it affects their personal life, as one participant shared: It’s been almost 24 years since I became an interpreter and I feel it was the right choice albeit a difficult career path with all of the vicarious trauma I have undoubtedly suffered. The trauma in my personal life has added more stress to my life as a mom.
While some participants actively tried to avoid situations that can induce vicarious trauma, others expressed an acceptance of trauma being embedded in their work. As one respondent described, “Just learning that vicarious trauma is a job hazard and one needs to know this with eyes wide open going into the profession.”
Emotional Distancing
Participants expressed a need to distance themselves from their clients to prevent emotional involvement and stress related to working so closely with clients, such as one interpreter who wrote, “I’ve learned to detach from the encounters.” Detaching and distancing themselves from patients reduces the impact of helping clients in emotional or traumatic encounters. As interpreters, they recognize that their role is solely to translate the conversation between the patient and the provider; multiple respondents wrote of the challenges of wanting to advocate for the client but not being able to do so, as well as trying to remain impartial. One participant shared, As a medical interpreter, it is very difficult to feel compassionate for our clients, as our relationship starts and ends within the time of the on-site visit. We are not there for compassion, but as bridge of communication. Unfortunately, there were some cases, I wished to advocate for the patient, but, as a medical interpreter, we are supposed to be neutral and objective. It’s only our voice, not our heart.
Lack of Emotional Support
Multiple participants voiced that they are not equipped with the emotional support that they need to aid their occupational health and mental health. A common underlying barrier to emotional support is that many interpreters are independent contractors or work through a contracted agency. As a result, they are not included in the programs that the hospitals offer to employees. In addition, it was regarded as a “lonely field” and one participant commented on being expected to work “beyond our mental limits.” Respondents noted that as interpreters, their mental health is often overlooked or even ignored. One participant shared her personal experiences with being denied mental health services as an interpreter, “I have brought to management’s attention issues concerning my mental health and my work as a medical interpreter. All of the times, I have been ignored or no answer.”
Workload
Challenges pertaining to a heavy workload were frequently cited by participants. Multiple respondents discussed having an overwhelming number of patients and cases each day, with little relief or support. “Burnout” was also a prevalent experience. A participant wrote of her experiences balancing the workload of being both a nurse manager and an interpreter because there are not any other interpreters at her hospital. Other challenges related to workload included short-staffing, large amounts of documentation, and long commutes to interpreting assignments, as one participant described: “The difficulty was the endless documentation & lack of support in these institutions. Now as a CMI, the workload is stressful due to the long driving duration’s, unpredictable work schedules, insensitive medical providers.”
Approaches to Mitigate Trauma
Interpreters reflected specifically on actions that they take to reduce or prevent the impact of vicarious trauma. This theme encompassed two relevant subthemes: Support Provided and Self-elected Assignments.
Support Provided
The delivery and availability of support for interpreters was important to respondents and was a common theme in their reflections. Participants described a variety of support programs and resources that they utilize to reduce the vicarious trauma that they experience because of their interpreter work. One respondent shared that they speak with a minister to manage their experiences of vicarious trauma. Some interpreters expressed that their workplace or agency does offer emotional support and counseling programs for medical interpreters. One shared, “When it comes to the trauma of interpreting, we have a personal responsibility to seek the help that the hospital provides.” Another respondent noted that their manager intentionally promotes self-care.
Self-Elected Assignments
Several participants explained that they intentionally avoid patient assignments on some units for the purpose of reducing stress and vicarious trauma. Several interpreters discussed experiencing stress and trauma and witnessing threats while interpreting on psychiatric units, and one shared that “mental health facilities are very stressful and I don’t accept assignments there anymore.” Some interpreters also expressed that they modify their work environment to prevent vicarious trauma, such as one interpreter who only interprets for clients over the phone to promote distancing and avoid trauma-inducing situations.
The Rewarding Nature of the Job
The theme, The Rewarding Nature of the Job, pertained to participants describing the gratifying parts of their job. The interpreters described many attributes that make their work as an interpreter worthwhile and fulfilling. Two subthemes were identified within this theme: Pride in Profession and Ability to Help.
Pride in Profession
Respondents emphasized that, challenges of the job aside, they are proud to work as medical interpreters. Several interpreters noted that they like their job, such as one respondent who shared, “I very much enjoy my work as a medical interpreter, and I’m proud of making communication clear between patients and providers.” Some respondents also recognized their talents that make them a good medical interpreter and an important member of the healthcare team. One participant noted that they are in this field not only because of their ability to speak another language but also because they are caring, patient, and intelligent individuals. Interpreters also voiced that as medical interpreters, they have a very important job, and that their work “saves lives.”
Ability to Help
Interpreters also expressed pride in their ability to help patients with NELP by serving as a conduit of communication between the patient and the provider. Respondents reflected on the fulfillment that comes with using their bilingualism to bridge gaps and aid in the healthcare setting, such as one respondent who shared “It is gratifying to me to help others using this gift of being bilingual.” The term “helping” was used by interpreters to describe their role in patient care, such as one participant who wrote, “I love the actual job that I do, which is translation and helping my community.”
Discussion
Results from this study provide valuable insight into the work-life and occupational health of spoken language medical interpreters. Participants provided contextual detail about the rewarding parts of their job as a medical interpreter, such as using their bilingualism to help patients with NELP in their communities and their pride in their profession. The gratification and pride of their work were reflected in participants’ written responses to an open-ended survey question. These findings coincide with previous research of other populations of interpreters, wherein providing language services increased compassion satisfaction among interpreters (Mehus & Becher, 2016; Zafirah et al., 2020).
In terms of work-related challenges, vicarious trauma was commonly reported among the interpreters who participated in this study—many noted that they work closely with their clients who experience traumatic events in the medical setting. These findings complement prior research on the prevalence of vicarious trauma among interpreters and translators (Simms et al., 2021; Villalobos et al., 2021). Participants described strategic approaches to mitigate their risk of vicarious trauma, such as selectively choosing their unit within a hospital. Beyond suggestions offered by respondents, one potential strategy to mitigate the effects of vicarious trauma and secondary traumatic stress is resilience training (Sansbury et al., 2015). Employers may consider offering interprofessional resilience training to simultaneously build collegiality and introduce staff to approaches to address work stressors, like compassion fatigue (Pfaff et al., 2017). Incorporating training in vicarious trauma in interpreter education programs is also critical (Knodel, 2018). In this study, respondents also reflected on how it is a lonely field to be in, and they are often overlooked and not viewed as part of the healthcare team, while they view themselves as highly valuable members of the team. Respondents conveyed that they felt that their profession and role in patient care are misunderstood by healthcare providers, a phenomenon that has also been reported elsewhere in the literature (Courtney & Phelan, 2019; Lai & Costello, 2021). Training for healthcare providers and staff focused on the role of interpreters is warranted, to improve integration into the healthcare team and foster improved interprofessional partnership (Lai & Costello, 2021). Such training may also improve the utilization of language services in the healthcare setting and, ultimately, provide better services for patients (Pechak et al., 2018).
This study’s findings also highlight important considerations to promote occupational health among medical interpreters. Respondents reported being unfairly or inadequately compensated for their work. Courtney and Phelan reported interpreter concerns about inequitable monetary compensation (Courtney & Phelan, 2019), a growing equity challenge during a shift to machine translation and piecemeal contracting work (Vieira, 2020). They also voiced that there is a need for accessible and appropriate mental health and self-care services for medical interpreters, as their work with patients can have mental health implications, especially when helping patients that are undergoing traumatic experiences. Similar findings have been reported previously for interpreters who work in mental health settings (Knodel, 2018; Zafirah et al., 2020). It is critical that interpreters receive the mental health services they need, however, because many interpreters work on a contract basis, services provided to full-time employees by hospital networks and institutions may not be available to them (Lai & Costello, 2021).
This study has its limitations. First, results from this study reflect the experiences of interpreters from five U.S. states who are certified through the NBCMI, which credentials interpreters who translate in Spanish, Cantonese, Mandarin, Russian, Korean, and Vietnamese. Also, credentialing is voluntary for medical interpreters, and this research only reflects the experiences of those credentialed with one organization in the United States. The findings of this study may therefore not be generalizable to the entire medical interpreter community. Those credentialed in other languages and dialects, through a different organization, who chose not to receive certification may not be captured in this study. Second, some participants identified as freelance and contract interpreters, while others work as permanent staff members at agencies or healthcare institutions. The variation in the type and nature of employment may influence the interpreters’ experiences, such as challenges with compensation, workload, support provided, and management. We did not capture respondents’ nature of employment and were unable to examine this relationship, which is an area for future exploration. Third, participants’ varying levels of education, experience, and training could impact their experiences as medical interpreters. For instance, some respondents noted that their interpreter training or certification included instruction about handling challenges and difficult circumstances.
This study provides insight into challenges associated with medical interpreting from the occupational perspective. Our findings can aid in helping to identify and implement resources that would benefit the medical interpreter community. They also shed light on the complexity and challenges of work as a medical interpreter. Awareness of the experiences and challenges facing this profession can help to promote an inclusive workplace and an informed healthcare team. The work-related challenges and professionalism concerns that participants discussed may be underlying contributors to the nation-wide shortage of professional medical interpreters. Future research could focus on reasons that medical interpreters consider leaving or leave the profession. To date, little to no information exists about attrition in the field of medical interpreting.
Implications for Occupational Health Practice
The results of this study highlight the occupational health challenges facing medical interpreters. To promote healthy, safe workplaces for an interprofessional workforce, it is important to understand and address concerns regarding professionalism, vicarious trauma, and support for medical interpreters. Medical interpreters serve a critical role on the healthcare team for patients and families with NELP, and by ensuring a strong support system for medical interpreters and the healthcare team, we can work toward advancing equitable healthcare for all patients.
Applying Research to Occupational Health Practice
Medical interpreters (n = 199) identified four primary occupational health themes in their response to a survey prompt: Professionalism and Role, Work-Related Challenges, Approaches to Mitigate Vicarious Trauma, and The Rewarding Nature of the Job. Occupational experiences included compassion fatigue, vicarious trauma, intentional emotional distancing from clients, and loneliness. Occupational health services may include trauma and stress exposure assessment coupled with resilience training and mental health care when warranted. Ultimately, these services should be evaluated for their impact on mental health well-being, workplace safety, and optimal patient care within the interprofessional team.
Footnotes
Acknowledgements
The authors would like to acknowledge the thoughtful insights and assistance provided by Joana Ramos, MSW.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects
The Washington State University Office of Research Assurances has found that the project is exempt from the need for Institutional Review Board review and provided a Certificate of Exemption (IRB #17916).