
Abstract
Background:
Cattle production in the United States is heavily supported by Latino/a workers. Beyond injury rates, our understanding of the health status of cattle feedyard workers is limited. The purpose of this study was to describe the health status and health care access among Latino immigrant cattle feedyard workers in the Midwest.
Methods:
A cross-sectional design using face-to-face structured interviews with Latino immigrant cattle feedyard workers in Kansas and Nebraska was conducted between May 2017 and February 2020.
Findings:
A total of 243 workers completed interviews; 91% were men. Over half (58%) had health insurance but few (36%) had a regular health care provider. Few chronic health conditions were reported despite most being overweight (53%) or obese (37%). The sample mean of sleep hours/24 hours was 7.1 ± 1.1. Problem drinking was moderate (42%), cigarette smoking was low (14%), and drug use was extremely low (<1%). Receiving health information from work was associated with less problem drinking, less obesity, lower blood pressure, and better sleep.
Conclusions:
Although few workers reported having a chronic health condition, most workers had chronic disease risk (i.e., elevated body mass index, problem drinking) and few had a regular health care provider. Receiving health information at work may have protective health effects.
Applications to Practice:
Occupational health professionals can partner with feedyard employers to expand current health and safety training programs beyond injury prevention to focus on health more broadly and to connect workers with local health care resources.
Background
In the United States, beef cattle production is the largest sector of the agricultural industry generating approximately US$73 billion in cash receipts in 2021 (United States Department of Agriculture, 2021). According to the U.S. Department of Agriculture (USDA ERS—Sector at a Glance, 2022), beef production is divided into two general stages. Cow–calf operations, the first stage of production, are where cows are bred to produce calves. Once the calves are weaned, they may be moved to graze on pasture, or they may be sent directly to a feedyard. Feedyards are the final stage of production where cattle will typically spend 3 to 6 months while being fed a ration of nutrients to maximize growth efficiency until they reach market weight for processing. Given the size and scale of many feedyards, labor is a constant concern.
Nearly two thirds (64%) of all hired farmworkers and half of all livestock workers in the United States are Latino/a (USDA ERS—Farm Labor, n.d.). However, our understanding of the health status of farmworkers, particularly those engaged in livestock production, is limited. Large data sources such as the Farm Labor Survey and the Census of Agriculture do not collect worker health data. Likewise, the National Agricultural Workers Survey, a large ongoing survey collecting demographic and health data on workers since 1989, includes only crop farmworkers, not livestock workers. According to the U.S. Bureau of Labor Statistics, the rate of illness with days away from work and rate of non-fatal injuries among animal production workers is twice that of crop production workers (Injuries, Illnesses, and Deaths in Agriculture, 2015–19, n.d.). In the central states region (i.e., Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, and South Dakota) where an estimated half of all cattle feedyard workers are employed, the fatal and non-fatal injury rates are 1.1 and 1.4 times greater, respectively, than the national average for the agricultural sector (Ramos et al., 2022).
Although agricultural occupational injuries and illness has been a concern for many decades, less attention has been paid to the physical, mental, and social well-being of farmworkers. Public health surveillance data have shown that the prevalence of preventable chronic cardiovascular conditions (i.e., diabetes, hypertension, obesity, dyslipidemia) continues to rise and disproportionately affect ethnic minority groups living in the United States (Boersma, 2020). Type II diabetes affects 17% of Hispanics compared with 8% of non-Hispanic Whites (Centers for Disease Control and Prevention [CDC], 2022). Among U.S. migrant and seasonal agricultural workers, the most common non-communicable diagnosed health conditions in descending order of prevalence are obesity, hypertension, and diabetes (National Center for Farmworker Health, Inc., 2020). A better understanding of farmworker health status and access to health care is needed to support the well-being of this vulnerable worker population. The purpose of this study was to describe the health status and health care access among Latino immigrant cattle feedyard workers in the Midwest.
Methods
The “Health and Safety of Latino Immigrant Cattle Feedyard Workers in the Central States Region” study used a cross-sectional design to evaluate the health, safety, and well-being of adult Latino immigrant cattle feedyard workers in Kansas (age of majority was ≥18 years) and Nebraska (age of majority was ≥19 years) between May 2017 and February 2020. Structured face-to-face interviews were conducted within participants’ homes, community locations (i.e., library or restaurant), or at the feedyard during working hours. Bilingual field research team members conducted the 60- to 75-minute interviews using a questionnaire that included items on work context, work safety, physical health, mental health and stress, social well-being, and demographics. Study findings on occupational injuries, fatigue, and work-related stress and adjustment are reported separately (Ramos, Adhikari, et al., 2021; Ramos, McGinley, et al., 2021a, 2021b). This study was approved by the University of Nebraska Medical Center Institutional Review Board, and all participants provided informed consent prior to completing the interview. Personal identifying information was not collected.
Measures
Questions related to health status and health care access were part of a 216-item structured interview guide prepared in English and Spanish. Participants had the option to complete the interview in their preferred language; however, only one participant completed an interview in English.
Health Status
General health status was evaluated using two standard items from the Behavioral Risk Factor Surveillance System (CDC, 2016); one item asks participants to rate their general health with five response options ranging from “poor” to “excellent” and one item asking for the number of days “in the past 30 days was your physical health not good” (CDC, 2016). History of chronic health problems was evaluated by asking participants if they had ever been told by a health professional that they had any of the 13 most common health conditions (e.g., cancer, diabetes, hypertension, etc.). Participants also had the option to select “other” and report any other condition that was not listed. Body mass index (BMI) was calculated from self-reported height and weight. Tobacco use was evaluated with two standard questions regarding ever smoked and current smoking (CDC, 2016). If a participant reported current smoking, then the six-item Fagerstrom Test for Nicotine Dependence was administered to evaluate nicotine dependence (Heatherton et al., 1991). Alcohol use was evaluated with the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) that includes three items on frequency of use in the past year and hazardous drinking (Saunders et al., 1993). Non-prescription drug use was evaluated with the Drug Abuse Screening Test, which includes 10 yes/no questions on drug use over the past year (Skinner, 1982). Physical health was evaluated by asking participants to self-report their height, weight, and average number of hours of sleep in 24-hour period.
Health care Access
Health care access was evaluated with three standard questions used in public health surveillance including: (a) health insurance coverage, (b) having a regular health care provider, and (c) inability to see a doctor in the past 12 months due to cost (CDC, 2016). An additional item asked participants how long it had been since their last visit to a doctor for a routine check-up.
Health and Safety Information Sources
Participants were asked to report what sources they used to learn about health and safety by selecting from a list of typical sources (e.g., work, family, friends, TV, radio, social media) and by reporting any additional sources. Participants were also asked which language (English, Spanish, or either) they preferred for health and safety information related to their work.
Data Analysis
Analysis was conducted using SPSS version 29. Continuous variables were evaluated using means, standard deviations, and ranges. Categorical variables were evaluated using counts and frequencies. Spearman’s rank correlation coefficients were used to evaluate associations between categorical variables. A series of logistic regressions were specified with the health care access variables predicting health status variables. Sex (male, female) and age (in years) were specified as demographic predictors in the logistic regression models. The health care access variables of having a health care provider (no or yes), health insurance (no or I don’t know/yes), time since last check-up (<36 months or ≥36 months), information through work (no or yes), social media (no or yes), friends (no or yes), and preferred language to receive health information (English or either language/Spanish) were specified as predictors in the logistic regression models. The health status variables of problem drinking (based on positive AUDIT-C), current smoking (not at all or some days/every day), sleep (≥6 hours or 0-5.5 hours), overweight (normal or BMI 25-29.9), obese (normal or BMI >30), diabetes (no or yes), high cholesterol (no or yes), and high blood pressure (no or yes) were specified as the logistic regression outcomes. Specifically, univariate logistic regressions (i.e., one predictor at a time) were estimated for current smoking, diabetes mellitus, high blood pressure, and high cholesterol due to the relatively low prevalence of these health status outcomes; multivariate logistic regressions (i.e., all health care access and demographic predictors together) were estimated for the health status outcomes of problem drinking, inadequate sleep, overweight BMI, and obese BMI, respectively.
Results
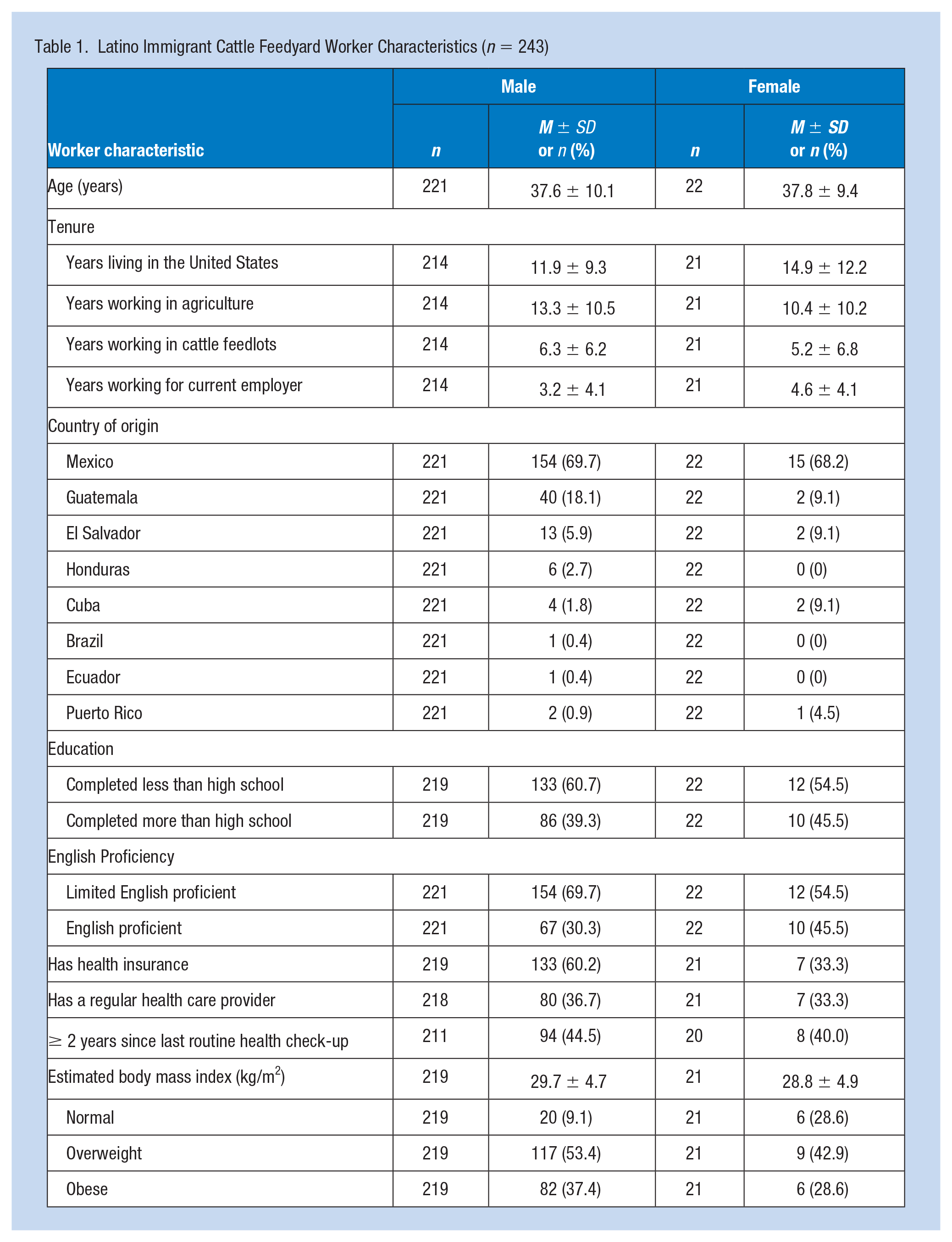
A total of 243 cattle workers completed structured interviews; 91% were men. Men and women participants were similar in age, ethnicity, education level, and English proficiency (Table 1).
Latino Immigrant Cattle Feedyard Worker Characteristics (n = 243)
Health Status
Most participants (88%) reported their general health as “good” to “excellent.” Few participants had been diagnosed with a chronic health condition commonly found in the U.S. adult population. Participants reported being diagnosed with high cholesterol (n = 41), high blood pressure (n = 24), diabetes (n = 18), asthma (n = 8), arthritis (n = 8), bronchitis (n = 3). Self-reported physical indicators of health included BMI (calculated from reported height and weight) and average hours of sleep in a 24-hour period. Few participants had a normal BMI (18.5-24.9), most were either overweight (53%) or obese (37%). The mean hours of sleep reported per 24-hour period was 7.1 hours ± 1.1. In general, substance use (i.e., alcohol, tobacco, or other drug use) as indicator of health status, was mixed. Drug use was low, tobacco use was relatively low, and problematic alcohol use was moderate (42%) (Table 2).
Latino Immigrant Cattle Feedyard Worker Substance Use Behaviors (n = 243)
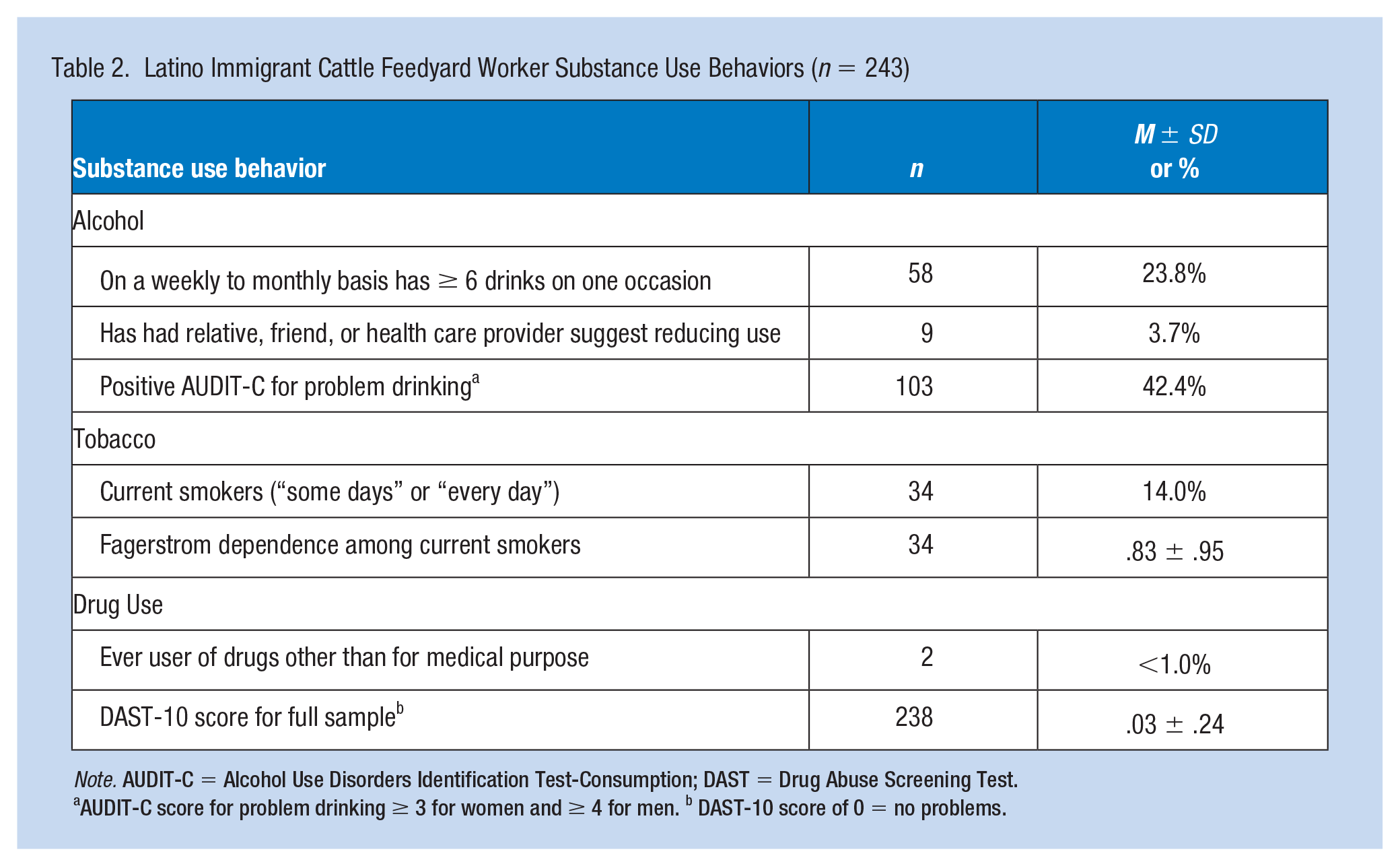
Note. AUDIT-C = Alcohol Use Disorders Identification Test-Consumption; DAST = Drug Abuse Screening Test.
AUDIT-C score for problem drinking ≥ 3 for women and ≥ 4 for men. b DAST-10 score of 0 = no problems.
Health care Access
A little over half (58%) of the participants reported having health insurance coverage. More men (61%) than women (33%) reported having health insurance coverage. Few participants (36%) reported having someone they considered as their health care provider. The sample mean time since last routine check-up was >2 years (M months = 27.2 ± 34.1).
Health and Safety Information Sources
Nearly all of the 227 participants were interested in receiving more information on work-related health and safety, and most (85%) preferred it in Spanish. When asked about preferences on how to receive health and safety information, most participants preferred in-person training at the workplace (70%), videos (47%), or a written manual, booklet or brochure (44%) over web-based modules (19%), a smartphone app (18%), or text messages (9%).
Bivariate Correlations
Spearman’s correlations revealed that problem drinking was positively correlated with having a regular health care provider (r = .25, p = .001), health insurance (r = .25, p = .001), and receiving health information from social media (r = .25, p = .001), but negatively correlated with receiving information from work (r = –.16, p = .039) and friends (r = –.26, p = .001). Current smoking (r = .16, p = .013) was positively correlated with receiving health information from social media. Inadequate sleep (0-5.5 hours; r = –.13, p = .045) and obese BMI (r = –.20, p = .033) were both negatively correlated with receiving health information from work. Reporting having diabetes (r = .25, p < .001), high blood pressure (r = .20, p = .002), or high cholesterol (r = .13, p = .05) was positively correlated with having a regular health care provider. Diabetes (r = –.15, p = .027) was negatively correlated with 36 months or more time since last check-up. High blood pressure was negatively correlated with receiving health information from work (r = –.14, p = .026) and friends (r = –.13, p = .04); high cholesterol (r = –.14, p = .032) was negatively correlated with receiving information from social media. There were no further significant correlations between the health care access and health status variables at the bivariate level.
Logistic Regressions
Logistic regression results (Table 3) suggested that receiving health and safety information from social media was related to higher odds of current smoking and problem drinking but lower odds of being overweight and having high cholesterol. Receiving health and safety information from work was associated with lower odds of obesity, high blood pressure, and inadequate sleep (0-5.5 hours/24 hours); receiving health and safety information from friends was associated with lower odds of high blood pressure. Reporting having a health care provider was associated with greater odds of reporting diabetes and high blood pressure. Females had lower odds of being overweight, while being older was related to greater odds of being overweight, obese, having diabetes, high blood pressure, and high cholesterol.
Logistic Regression Results for Health Care Access Predicting Health Status Variables
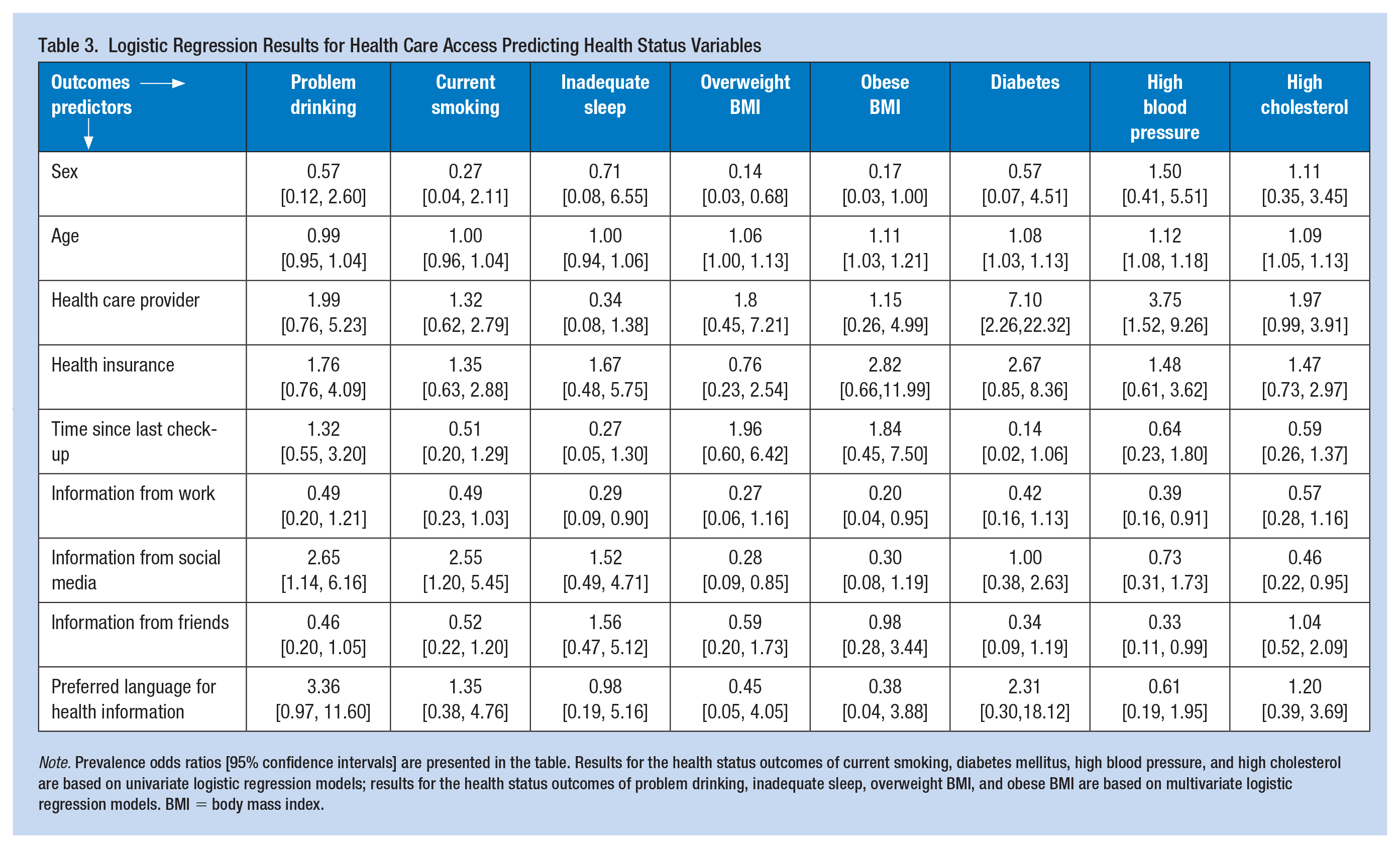
Note. Prevalence odds ratios [95% confidence intervals] are presented in the table. Results for the health status outcomes of current smoking, diabetes mellitus, high blood pressure, and high cholesterol are based on univariate logistic regression models; results for the health status outcomes of problem drinking, inadequate sleep, overweight BMI, and obese BMI are based on multivariate logistic regression models. BMI = body mass index.
Discussion
Although Latino immigrants comprise the majority of the agricultural workforce in the United States, little is known about their health and access to health care. This study is the first to the authors’ knowledge to report on these indicators within the cattle feeding industry. We found that most workers reported good health, and few reported having a chronic condition. Few participants had a regular health care provider; however, having a regular provider was significantly associated with reporting diabetes and high blood pressure. This may in part be due to the fact that such conditions require more consistent monitoring from a health care provider. Most participants had not had a routine check-up within the last 2 years. Given the high association of chronic conditions with obesity (i.e., hypertension, diabetes) in the general U.S. Latino/a population (Aguayo-Mazzucato et al., 2019; Young et al., 2018), the prevalence of related chronic conditions was markedly low in this sample of mostly overweight/obese participants. This may be due in part to limited access and underutilization of health care services. We speculate that health care access may be problematic for these workers and note several contributing factors: lack of health insurance; inability to leave work for health-related appointments; limited access to health care providers or facilities, given the rural and remote geographic location of feedyards, especially those providing culturally, linguistically, and contextually competent care; and limited English proficiency. Furthermore, health care service utilization may be limited by cultural norms related to preventive care and masculinity (Towns, 2013).
Drug use was notably low. However, compared with the general U.S. Latino population, the prevalence of cigarette smoking was slightly higher (11% vs.14%) (Cornelius et al., 2020) and problematic drinking was much higher (9% vs. 42%) (Castañeda et al., 2019). Substance use may be related to health beliefs and social and cultural norms (Arcury et al., 2020). Additional research is needed to assess reasons for the high rates of alcohol use and higher than average prevalence of current smoking among this worker population.
Receiving health and safety information from work resulted in lower odds of reporting inadequate sleep, high cholesterol, and being obese. Extending health promotion efforts in the workplace can be protective to health. Workers, particularly agricultural workers, have long hours and face many logistical challenges to accessing and receiving health information given their demanding schedules. To improve health equity, work must be considered as a social determinant of health (Flynn et al., 2021). As such, workplace health and wellness initiatives including onsite preventive health screenings, health promotion workshops, and regular safety training should be considered.
Limitations of this study include the cross-sectional study design, which limits our ability to determine causality, and the self-reported methodology. It is possible that workers underreported specific behaviors such as substance use due to social desirability or self-presentation bias. Future studies should incorporate objective measures to better evaluate health status in cattle feedyard workers, a population with known health and safety risks, and use longitudinal designs to better understand the temporal nature of relationships between work and health (Ramos, McGinley, et al., 2021a, 2021b).
Implications for Occupational Health Practice
Given the association between receiving health and safety information at the workplace with protective behaviors (e.g., more sleep per 24-hr period) and better health (e.g., normal weight, cholesterol), we view onsite occupational health care and education as key strategies to address the social determinants of health affecting immigrant cattle feedyard workers (Ramos, 2018). Occupational health professionals can partner with feedyard employers to expand current health and safety training programs beyond injury prevention to also focus on health and well-being more broadly, thereby helping to promote and maintain healthy lifestyle behaviors. Onsite clinical visits by an occupational health professional with focus on the occupational context affecting health, health behaviors, and family life outside of work (Ramos et al., 2019) will support the delivery of quality care to a population with access barriers (Ramos & Schenker, 2021).
In Summary
This study found among Latino immigrant feedyard workers . . .
More than half had health insurance, but few had a regular heath care provider
Health risks may stem from an elevated body mass index and/or problem alcohol drinking
Receiving health and safety information at work may have protective health effects and was negatively correlated with problem drinking, inadequate sleep, being obese, and having hypertension
Footnotes
Acknowledgements
The authors acknowledge the valuable contributions of research team members: Marcela Carvajal-Suarez, Axel Fuentes, Rodrigo Gamboa, Sophia Quintero, Natalia Trinidad, and Drs. Casper Bendixsen and Meredith McGinley.
Author Contributions
S.A.R. performed analysis, writing and final approval of version to be published. A.K.R. performed conceptualization, funding acquisition, methodology, investigation, curation, analysis, writing and final approval of the version to be published. S.M. performed analysis, writing, final approval of version to be published. G.C. performed conceptualization, methodology, analysis, writing and final approval of version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Central States Center for Agricultural Safety & Health (CS-CASH) through NIOSH grant U54 OH010162.
Human Subjects review
The University of Nebraska Medical Center Institutional Review Board approved this study, IRB 612-16-EX, as exempt for Educational, Behavioral, and Social Science Research on October 7, 2016.