
Abstract
Background:
At the time of our study, occupational health evidence specific for long-term care employees was mostly lacking. The purpose of this study was to determine the proportion of positive cases in employees after the first COVID-19 wave in May 2020. We also determined the prevalence of asymptomatic cases.
Method:
The study population included all health care workers (HCW) employed at one mid-size long-term hospital in Spain (May 2020). A cross-sectional study design included an interviewer-administered self-reported questionnaire (including sociodemographic questions, risk factors for COVID-19 complications such as hypertension or diabetes, and previous polymerase chain reaction [PCR] results) and antibody determination (Biozek rapid test). Data were analyzed using Student’s t, Fisher, and chi-square tests. Two multivariate logistic models were created to evaluate exposure factors and symptoms separately on the outcome of having had COVID-19.
Findings:
Of the 97% of workers who participated (580/596), 300 (51.7%) suffered symptoms of COVID-19, 161 (27.8%) of the rapid antibody tests were positive for IgM and/or IgG, 160 (27.6%) workers had at least one risk factor, and 32 (19.0%) of the 168 SARS-CoV-2-positive cases were asymptomatic. The proportion of negative or unavailable PCRs, with positive antibody, was 11.7% (56/477). Casual contact without protection (odds ratio [OR]: 1.9, 95% confidence interval [CI]: 1.1–3.4), doctor occupation (OR 3.3, 95% CI: 1.1–10.2), and nursing assistant occupation (OR 2.5, 95% CI: 1.2–5.8) were independently associated with SARS-CoV-2 infection.
Conclusion:
Physicians and nursing assistants in a long-term care setting were at a higher risk of SARS-COV-2 infection over other occupations in the first wave of the pandemic, especially when in contact with patients without protection. Almost one-fifth of the workers with a positive PCR test for SARS-COV-2 were asymptomatic and seroprevalence (27.8%) was well below the approximated herd immunity cutoff (60–70%). Essential workers in long-term care must be monitored frequently by Employee Health Service and should be required to wear personal protective equipment including a fit-tested N-95 while in close contact with patients and coworkers.
Background
Seroprevalence is the proportion of individuals with antibodies against SARS-COV-2. The presence of specific antibodies seems to confer protection against coronaviruses in general (Huang et al., 2020), and sera from convalescent patients can have in vitro neutralizing properties against SARS-COV-2 (Lee et al., 2021), but the in vivo long-term duration and factors of immunity are not precisely known.
Since the start of the worldwide spread of SARS-COV-2, estimating the proportion of immune individuals has been of paramount importance as many of them might have had an asymptomatic course. In the early phases of the COVID-19 pandemic, the prospect of reaching herd immunity was seen as key to achieving epidemic control. That is, when a large percentage of the population (60–70%) was immune, no large outbreaks would occur, and the pace of transmission would slow down (Fontanet & Cauchemez, 2020). In Spain, a seroprevalence study was performed in April to May 2020, with 61,075 participants in the general population; 5.0% (95% confidence interval [CI]: [4.7, 5.4]) of these were positive for antibodies as detected with the point-of-care tests (Pollán et al., 2020). This suggests a large percentage of the population was still susceptible to SARS-COV-2 infection.
Prevalence in Health Care Workers
Health care workers (HCW) in tertiary-care hospitals had a high COVID-19 disease burden in the first wave of the pandemic (March-April 2020): In the first COVID-19 wave in Spain, until May 11, 2020, a total of 40,961 COVID-19 cases had been reported in health care workers (Spain’s National Epidemiology Center, Centro Nacional de Epidemiología, Instituto de Salud Carlos III, 2020b, #2). The evidence regarding long-term care institutions is more limited; however, in six London care homes that had experienced an outbreak at the peak of the pandemic, 156 (75.0%, 95% CI: [68.7, 80.4]) members of 208 HCW were seropositive, and 95 (66.4%) of 143 asymptomatic HCW with a previously negative were seropositive against SARS-CoV-2 (Ladhani et al., 2020). Estimating the prevalence of asymptomatic HCW’s in long-term care provides evidence that employees in these facilities must be tested regularly to provide early care and isolation to protect the employees and the residents. Herein we describe a SARS-COV-2 seroprevalence study in HCWs after the first wave in a mid-size community long-term care hospital and analyze the clinical presentations.
Method
Study Setting
This cross-sectional study was carried out from April to May 2020 at the Virgen de la Poveda Hospital (Madrid), a rural, mid-sized community hospital with 200 beds in Spain, formally a middle-term care hospital. See Supplementary Material (S1) for additional remarks on this institution’s characteristics. There were 3 types of wards at the time of the study:
(1) General medical care (patients needing medical/nursing care),
(2) Inpatient Rehabilitation, and
(3) Palliative care.
All employees (n = 596) working during the study period were included.
Testing and Data Collection
All HCWs received at least one SARS-CoV-2 polymerase chain reaction (PCR) appointment between March and May 2020, for at least one of the following indications: symptomatic worker evaluation, close contact testing, and the lower priority asymptomatic whole-institution screening. We followed this approach as reported in other studies and institutions (Lumley et al., 2021). In addition, participants completed a questionnaire and a rapid SARS-COV-2 antibody test between April 30, 2020, and May 19, 2020. This study was carried out in accordance with ethical regulation for human subjects by the ethics committee of the Fundación Alcorcón University Hospital.
The questionnaire was designed by consensus and peer consultation among the researchers who included experienced preventive medicine professionals. It included sociodemographic variables (age and sex), possible protective factors (smoking and flu vaccination the previous year), complicated COVID-19 risk factors of the worker (hypertension, diabetes, malignancies, chronic heart/lung/liver diseases, immunosuppression, malignancies in the last 5 years, or pregnancy), risk factors of the cohabitants of the worker, workplace variables (position and professional category, unit where they were working during the study period and before), workplace exposure in the first wave (including casual close contact with patients without PPE, routine close contact with patients with PPE, and no exposure), previous work in COVID-19 wards, recent close contact with a COVID-19 case (patients or otherwise), COVID-19 symptoms and their start and end date (fever, headache, cough, asthenia, myalgia, rhinorrhea, sore throat, dyspnea, anosmia, ageusia, abdominal pain, and diarrhea), COVID-19 history (including hospital admission), and previous test results (PCRs and their result). In this questionnaire, all questions were self-reported and interviewer assisted (with the participation of the research team). To minimize recall bias in this study, the questionnaire was administered the same day as the rapid test, so the study subjects did not know its result when answering the questions. Emphasis was placed on asking all the included people about all the symptoms and risk factors listed in the questionnaire.
COVID-19-positive cases were defined as those who were positive by PCR for SARS-Cov2 and/or had the presence of IgG antibody against the SARS-CoV2 virus (this definition is used in all statistical analysis unless noted otherwise). Those who tested positive for IgM antibody alone were subject to a confirmation PCR. The chromatographic immunoassay test used to detect the presence of antibodies against coronavirus was the Biozek COVID-19 IgM / IgG Rapid Test.
The sample size estimated for a population proportion of 6%, with a precision (as margin of error of the estimate) of 2%, a confidence level of the estimate of 95% (the confidence that the estimate ± the margin of error will contain the true proportion), and a sample population of 100,000 people (for a population with an unknown size) was 539 people. A Microsoft® Access® database was designed for data collection, with validation rules to prevent errors. All personal data were protected, and in particular, hospital management was barred from any access to the clinical data of HCW.
Statistical Analysis
The only continuous variable (age) was described with mean and standard deviation, as it followed the normal distribution. Categorical variables (other variables) were described with their counts and percentages. Student’s T was used to compare quantitative normally distributed variables (age). In the case of categorical variables, they were compared using the Fisher test for 2 × 2 tables and chi-square test otherwise, and odds ratios (OR) were calculated. Two multivariate logistic regression models were created: one with occupation-related variables (intended for risk assessments) and one with symptoms and contact data (intended for evaluating COVID-19 probability). The dependent variable was being COVID-19 positive.
A figure was created with the proportion of positives by professional category and type of tests, with CIs calculated via the Clopper-Pearson method (Clopper & Pearson, 1934). The possible association between underdiagnosis, defined here as the seroprevalence (IgG+) in cases with no previous positive PCR for COVID-19, and professional category was evaluated via the Fisher’s test. Finally, a descriptive table of both tests results was elaborated, without further statistical analysis (since this study was not designed as a method comparison study). STATA 15 and R 4.0.3 were used to perform the statistical analysis. The resulting seroprevalence can be compared with the results of the first round (April-May 2020) of the ENECOVID study (National Center of Epidemiology, 2020a). (The ENECOVID is a seroepidemiological SARS-CoV-2 infection study performed in Spain in several phases, targeting general population of all the regions, which included antibody testing and questionnaire assessment and whose results included the COVID-19 seroprevalence).
Results
A total of 580 HCWs participated in the study, and 16 declined participation, for a response rate of 97%. The mean age was 46; there were 115 (19.8%) men and 465 (80.2%) women. Table 1 displays the professional categories, occupational exposure, medical risk factors, symptoms, and COVID-19 status of the participants. According to the definition used, 168 cases were COVID-19-positive. The percentage of COVID-19-positive HCWs by professional category is shown in Figure 1.
Demographic and Work Characteristics of Hospital Employees (n = 580)
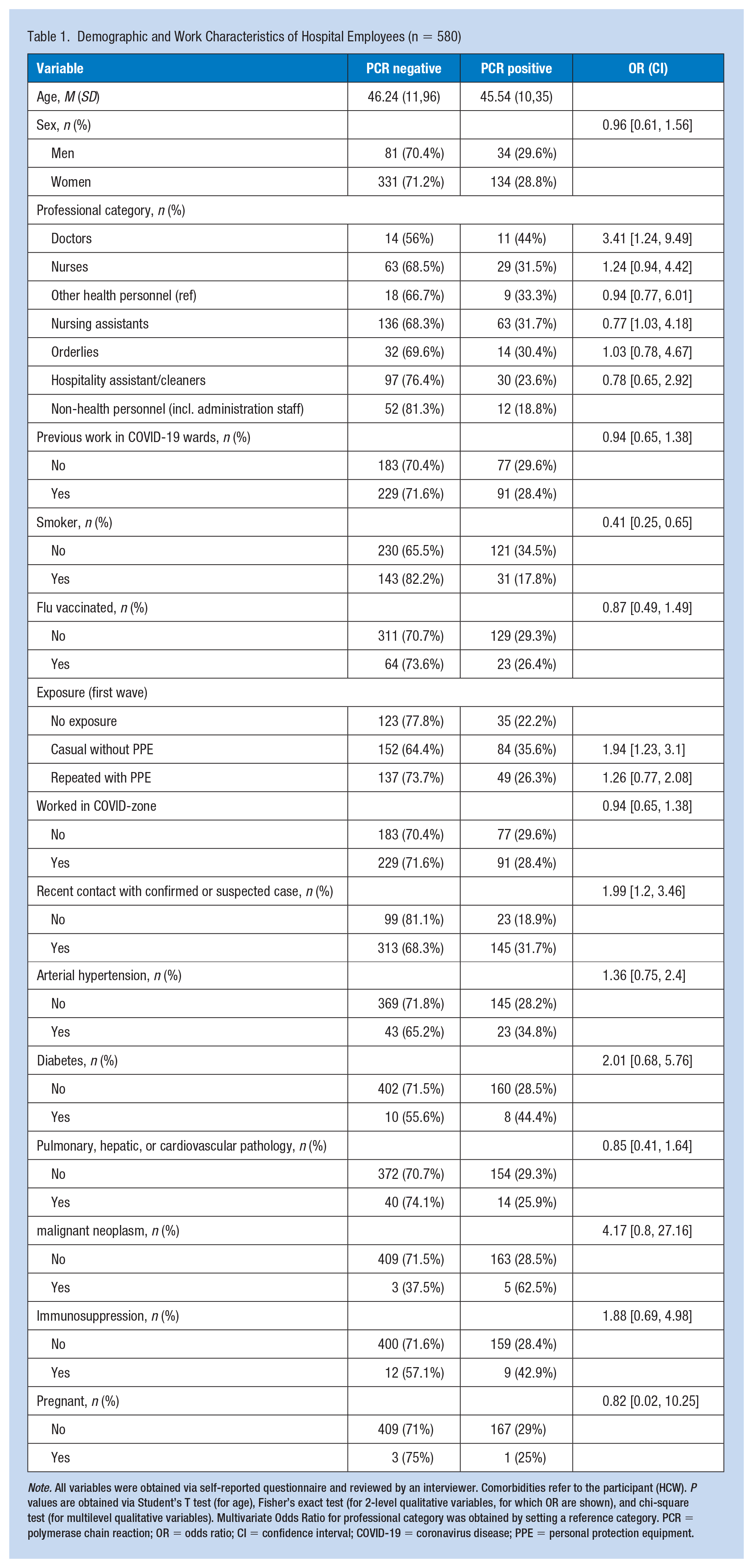
Note. All variables were obtained via self-reported questionnaire and reviewed by an interviewer. Comorbidities refer to the participant (HCW). P values are obtained via Student’s T test (for age), Fisher’s exact test (for 2-level qualitative variables, for which OR are shown), and chi-square test (for multilevel qualitative variables). Multivariate Odds Ratio for professional category was obtained by setting a reference category. PCR = polymerase chain reaction; OR = odds ratio; CI = confidence interval; COVID-19 = coronavirus disease; PPE = personal protection equipment.
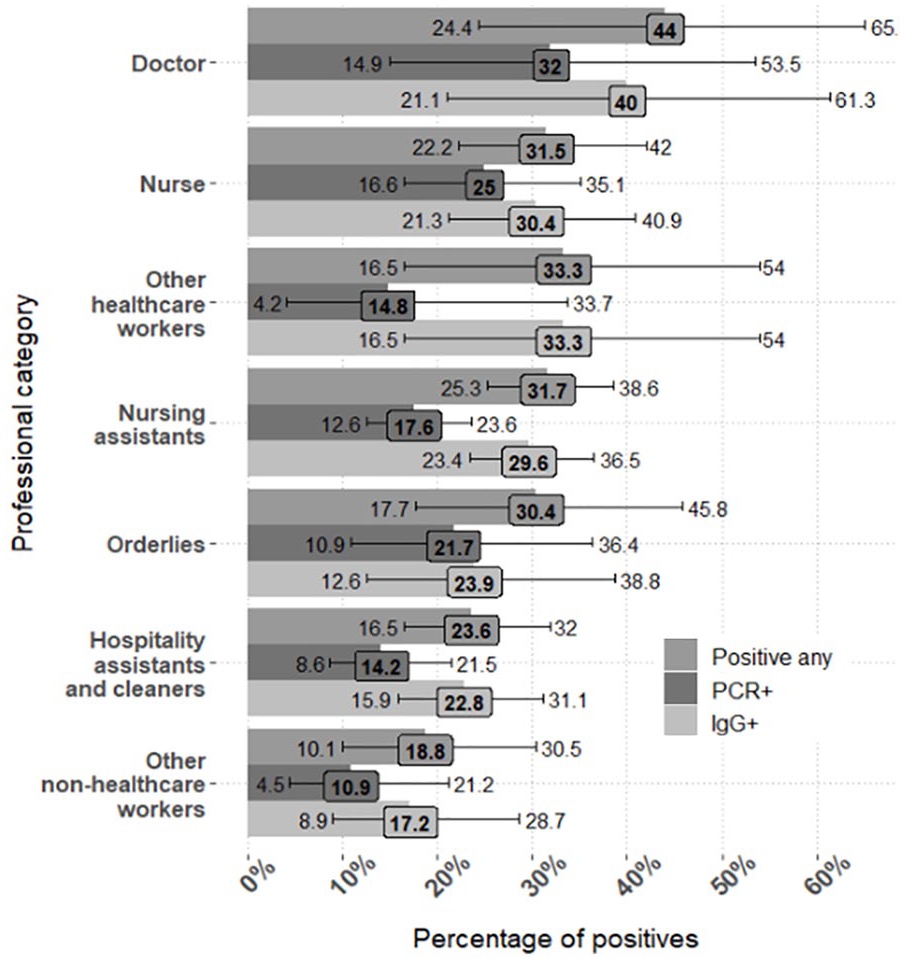
Percentage of Positives by Professional Category and by Type of Test.
In all, 40.7% HCWs (236/580) reported casually being exposed to COVID-19 without personal protection equipment (PPE), and 55.2% (320/580) had worked in COVID isolation units. The multivariate logistic regression with exposure-related factors is summarized in Table 2 (model accuracy: 72%, area under the curve [AUC]: 0.65); predictors associated with COVID-19 included being exposed to COVID-19 cases without PPE and working as doctor or nursing assistant; smoking was also significant but negatively associated.
Logistic Regression Model With Exposure as Predictor (to Determine Associated Factors)
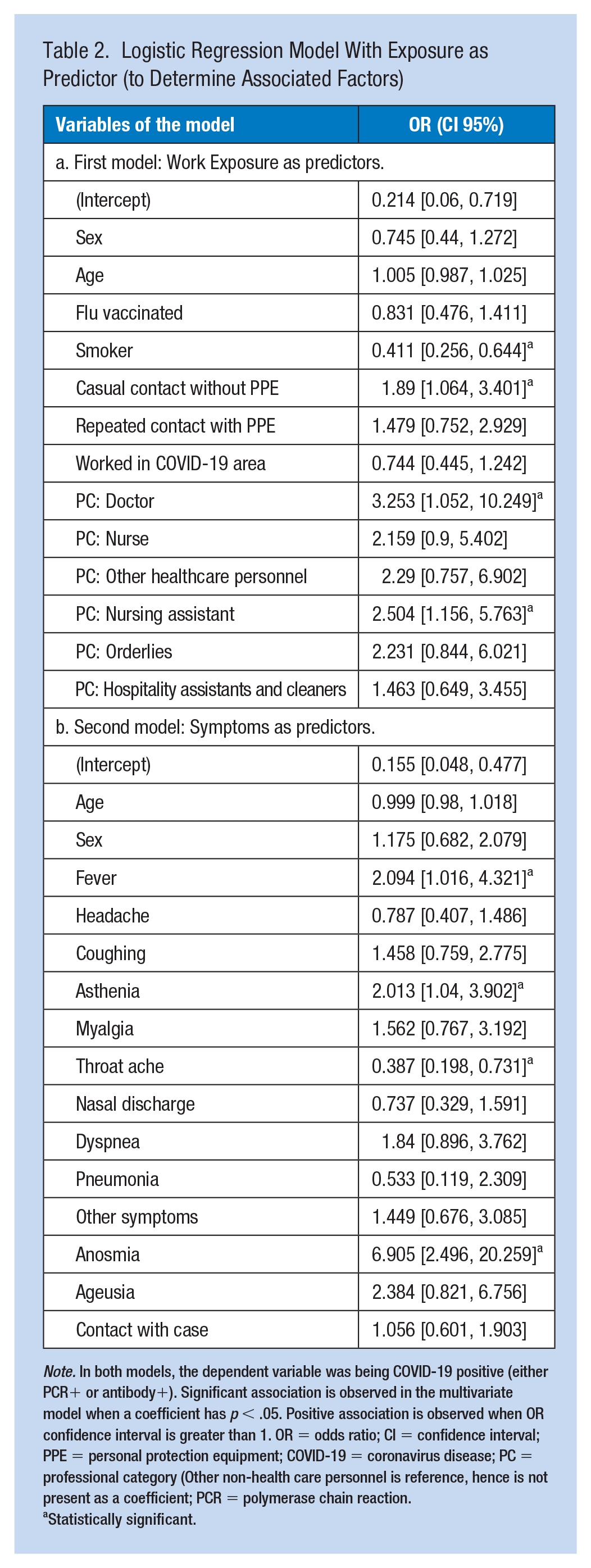
Note. In both models, the dependent variable was being COVID-19 positive (either PCR+ or antibody+). Significant association is observed in the multivariate model when a coefficient has p < .05. Positive association is observed when OR confidence interval is greater than 1. OR = odds ratio; CI = confidence interval; PPE = personal protection equipment; COVID-19 = coronavirus disease; PC = professional category (Other non-health care personnel is reference, hence is not present as a coefficient; PCR = polymerase chain reaction.
Statistically significant.
In all, 51.7% (300/580) of all the participants were “symptomatic,” that is, they said they had suffered COVID-19 symptoms, 136/168, 81.0%, of COVID-19 positive cases, and 164/412, 39.8% of COVID-19 negative cases; p < 2.2e-16, OR = 6.41 (95% CI: [4.1, 10.23]). Among those who reported symptoms, the median number of symptoms was 4 (interquartile range [IQR]: 3–7). Self-reported symptoms and their frequencies can be seen in Supplementary Material (S2). The multivariate logistic regression with symptoms is shown in the Table 2 (model AUC = 0.814, accuracy = 82%). A sensitivity analysis was performed in this model: When predictor “contact with case” was removed, the significant coefficients and their magnitude remained the same.
Rapid IgG/IgM tests were performed on all study subjects. In all, 412 people in the study also underwent a PCR for SARS-Cov2. Table 3 compares the result of both tests. Of all the rapid tests carried out, 27.8% (161/580) were positive, while of all the PCRs performed, 22.0% (105/477) were positive. The test was fully concordant (both positive or both negative) with the PCR in 86% (410/477) of the cases with a PCR available; 11.7% (56/477) of the HCWs were seropositive but previous PCR was negative, and 2.3% (11/477) were seronegative but previous PCR was positive. Four cases had slightly dim positive IgM with negative IgG; in all these a PCR was performed with negative results. In all, 96.6% (461/477) of the subjects underwent PCR prior to the rapid test, and only in 16, it was performed in the same appointment (data not displayed); the PCR was performed on average 22.8 days before the rapid test (95% CI [21.4, 24.3]).
Contingency Table of the Test
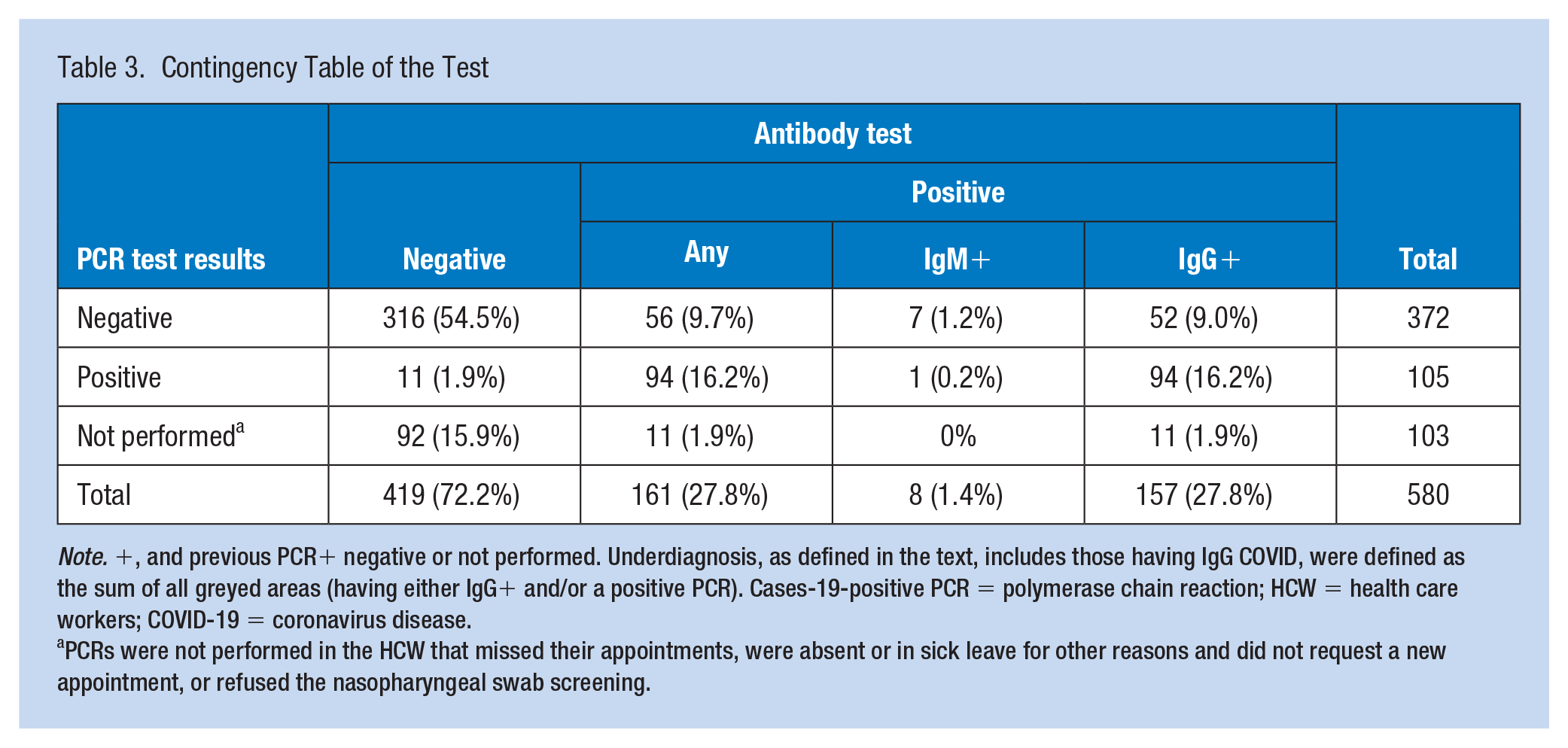
Note. +, and previous PCR+ negative or not performed. Underdiagnosis, as defined in the text, includes those having IgG COVID, were defined as the sum of all greyed areas (having either IgG+ and/or a positive PCR). Cases-19-positive PCR = polymerase chain reaction; HCW = health care workers; COVID-19 = coronavirus disease.
PCRs were not performed in the HCW that missed their appointments, were absent or in sick leave for other reasons and did not request a new appointment, or refused the nasopharyngeal swab screening.
Underdiagnosis percentage was 13.2% (63/475) and was not associated with professional categories (p = .34, data not displayed). Of the 32 asymptomatic cases, 23 did not have a previous positive PCR.
Results of HCW with risk factors of complicated COVID-19, or cohabitating with individuals at risk, are available in the supplementary material (S3). In all, 27% (114/412) of COVID-19-susceptible participants (negative PCR and negative antibody) had at least one risk factor, and among those who answered affirmatively, the median number of risk factors was 2 (IQR 1% to 2). In all, 37% (154/412) of COVID-19-negative (susceptible) participants cohabited with an individual with at least one risk factor.
Discussion
Our study provides evidence specific to a community long-term care center, lacking Emergency Department or Intensive Care Unit. This epidemiological study provided evidence that informed our management of employee health during the COVID-19 pandemic. Risk factors were prevalent in the worker population and their cohabitants, and the low prevalence of positive antibody (related to a moderately low prevalence of asymptomatic COVID-19 cases) suggested a very high proportion of workers were susceptible hence highlighting the levels of immunity and how important preventive measures were. A full-suppression strategy, with the goal of maintaining a zero COVID-19 incidence in patients, HCWs, and visitors, was implemented via quick detection and isolation of positive COVID-19 cases, including asymptomatic ones.
After the first wave of the pandemic, many questions arose: What is the actual proportion of asymptomatic cases in the general population and in this institution? (Pollán et al., 2020) What is the proportion of positive cases untested due to laboratory and health care constraints in the first COVID-19 wave? Many seroepidemiological studies were performed in health care centers (Galán et al., 2022; Kowall et al., 2021; Rodriguez et al., 2021; Varona et al., 2021; Vázquez et al., 2021). These studies generally had a cross-sectional design which included serological testing as well as a questionnaire that included hospital position, symptoms, contact with cases, and risk factors for complicated COVID-19; sometimes a follow-up is present.
The 27.8% seroprevalence in HCW in our public institution after the first COVID-19 wave can be compared with the results of the literature: 31.6% in HCW in a teaching hospital near our center (N = 2,959, Galán et al., 2022); 16.2% in HCW with no previous history of COVID-19 in hospitals in this region (N = 5,995, Vázquez et al., 2021); 11% in 17 private hospitals in Spain (N = 6,038, Varona et al., 2021); 2.8% in a Hospital in the Balearic Islands in Spain (N = 2,210, Rodriguez et al., 2021). The ENECOVID study, provided similar results in May 2020 (Spain: 10.2 [7.9–13.0], Madrid: 20.6 [12.1–32.8]); for comparison, the seroprevalence in general population was 11.3%. Therefore, the seroprevalence in Madrid (the third most populated and the third most densely-populated Autonomous Community in Spain) was relatively high, and the seroprevalence in HCW was higher than in general population.
In other countries, HCW also showed a high seroprevalence. In Oxford University Hospitals (N = 12,541; Lumley et al., 2021), 1,177 workers were IgG anti-Spike positive at the beginning of the study (9.39%). In a meta-analysis with 97 studies and 230,398 HCWs, 11% (95% CI: [7%, 15%]) had a PCR-confirmed COVID-19 infection (Gómez-Ochoa et al., 2021). Other meta-analysis may provide higher figures (Gholami et al., 2021).
Underdiagnosis was common in the first COVID-19 wave in Spain (Soriano et al., 2021). In a nearby teaching hospital, the seroprevalence in HCW with a previous negative PCR was 29.6% (115/388); in our center, this proportion was smaller, seroprevalence was 13.9% (52/372) in HCW with all previous negative PCR and 10.7% (11/103) in HCW without a previous PCR. Therefore, in the context of COVID-19, screening has been recognized as particularly helpful to diagnose “hidden” asymptomatic cases (Galán et al., 2022). As a particular finding, underdiagnosis was not associated with any professional category.
Many professional categories had a higher seroprevalence than the general population in this region (11%), and we found doctors and nursing assistants were significantly associated with COVID-19 infection in the multivariate model, but working in COVID-19 areas was not. The nurse category was close to statistical significance (multivariate OR 95% CI: [0.9, 5.402]). The increased risk in clinical HCW exposed to non-COVID patients and the increased risk in HCW that have minor or moderate contact with patients have also been noted in other studies in the literature (Galán et al., 2022; Varona et al., 2021). In our study, the group with the highest prevalence was doctors (44%; 95% CI: [24, 65]); the same happened in a nearby teaching hospital (doctors: 39.6%). In other meta-analyses, the most affected category was nurses (48% of positive HCW; 95% CI: [41, 56]; Gómez-Ochoa et al., 2021).
After the first wave, preventive measures were implemented to protect HCWs, patients, and the general population. In the Oxford University Hospitals study in the United Kingdom (Lumley et al., 2021), the estimated daily incidence of COVID-19 ranged between 1/10,000 workers in April to June 2020, ~0.3/10,000 workers in July to September 2020, and 1 to 3/10,000 workers in October/November 2020. In our institution, isolated outbreaks occurred in mid-late 2020 and especially in January 2021, in low numbers, as a “low-probability, potentially high-impact” event, but sufficient availability of staff was ensured, thanks to preventive measures, readily available PPE, and HCW collaboration. In this study, contact with cases without PPE (wearing just a surgical mask or no mask at all, early in the pandemic) was associated with COVID-19, but contact with PPE was not. COVID-19 PPE (including gown, goggles, mask, etc.) is not worn in non-COVID wards unless there is clinical suspicion; in this situation, close contact before patient diagnosis might occur. Surgical masks can provide some variable degree of protection (Howard et al., 2021).
Lack of PPE or improper use or practices have also been observed as an associated factor in other studies (Gómez-Ochoa et al., 2021); and the role of smoking, with a significant negative association with COVID-19, has also been observed and discussed (Kowall et al., 2021; Matos et al., 2021).
In addition, in this study we observed anosmia, asthenia, throat ache, and fever had a significant association with COVID-19, which is coherent with the literature (Elliott et al., 2021; Galán et al., 2022; Gómez-Ochoa et al., 2021; Nomura et al., 2020). In the study with Brazillian HCW (Buonafine et al, 2020), the variables significantly associated with COVID-19 in the multivariate analysis include anosmia, (OR= 4.40, 2.21–8.74), male sex, (OR=2.13, 1.26–3.61), and ocular pain (OR=1.95, 1.14–3.33). Sex is also a significant predictor in other studies (Kowall et al., 2021) but did not reach significance in our study and in the ENECOVID study the prevalence was similar between both sexes.
As a particular finding, in the second multivariate regression, recent self-reported “contact with a confirmed case” did not reach statistical significance; so it could be interpreted as less useful than symptoms when evaluating a suspected COVID-19 case. In other predictive models of COVID-19, contact with a confirmed case did reach statistical significance, OR = 2.07 (1.52–2.82), with less strength than taste or smell disorders (OR = 8.79, 6.42–12.0; Kowall et al., 2021).
Study Limitations and Strengths
The study limitations are similar to those found in other similar cross-sectional seroprevalence studies (Galan et al., 2022): Samples were collected over 3 weeks, and in some cases, a previous PCR was not available.
The performance of the Biozek IgG/IgM rapid test has been shown to be worse than enzyme-linked immunosorbent assay (ELISA) or CLIA laboratory methods (Tešija Kuna et al., 2021): It has a good IgG sensitivity (92.3, 95% CI: 82.8–97.1) and specificity (99.0, 95% CI: 96.1–99.96; Tollånes et al., 2021). In the first round of the ENECOVID study, using the immunoassay as reference (N = 51958), the sensitivity of the rapid test was 79.6% (1,793/2,282, 95% CI: [77.1, 81.8]), and the specificity was 98.3% (98.2–98.; Pollán et al., 2020). In some cases serologic tests provided unexpected results: In this study, 10.4% (11/105) HCWs had negative antibody tests with a previous positive PCR; this proportion was 9.1% (31/339) in another study using Diapro ELISA tests (Galán et al., 2022).
The validity of self-reported information by participants could be another source of error; clinical records were not reviewed in order to preserve worker’s privacy. PCR was only available for 82.2% of the workers in the study. This was higher than the percentage in other seroprevalence studies in hospital workers (727, 28.1% in Galán et al., 2022; 1061, 17.6% in Varona et al., 2021) and in the general population (1249, 2.4%, ENECOVID study, first round). PCR was offered to all workers when the incidence of COVID-19 was high (March-April), as a screening due to the risks of COVID outbreaks in this center, and antibody test were performed when the incidence fell (April to May).
A particular limitation of this study is the lack of external validity: These results might not be applicable to other hospitals, especially since community long term care hospitals are not a common denomination; and these findings might not be applicable to other periods in the pandemic. Yet, evidence is mostly lacking for this particular kind of institution.
Finally, as shown by the wide CIs for some estimates, the statistical power of this study was smaller than other COVID-19 studies performed in larger centers.
When it comes to the strengths, we can note the high response rate, the consistency of the methodology, the respect for HCW rights and privacy, and the useful evidence for long-term care centers. Our response rate (97.3%, 580/596) was higher compared with that in other studies: 88.7% (2590/2919, Galán et al., 2022), 94.5% (5995/6344, Vázquez et al., 2021), and 37.9% (855/2253, Rodriguez et al., 2021).
Implications for Occupational Health Practice
In this mid-size community hospital, a COVID-19 diagnostic screening study of the whole workforce of the hospital was carried out to obtain accurate information about the pandemic situation after the first wave; this experience, methodology, and findings could be helpful for other akin centers.
Risk factors for complicated COVID-19 were widespread in the HCWs and in their cohabitants; and HCWs were particularly likely to be infected in the first wave of the pandemic. Underdiagnosis was prevalent (13.2%) but was not associated with any professional category.
Finally, regarding COVID-19 symptoms, there are lists of symptoms but the key symptoms are anosmia, fever, and asthenia.
Applying Research to Occupational Health Practice
This study was an example of integrating epidemiological information into workplace prevention strategies. We have observed that the proportion of infected HCW is markedly high, that working in our hospital increased the COVID-19 risk at least twofold, that some professional categories were associated with COVID-19 positivity, and that the factor most significantly associated was exposure to cases without PPE. In the present and future pandemics, emphasis should be placed on protecting healthcare workers.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221135587 – Supplemental material for Seroprevalence of SARS-CoV2 Infections in Health Care Personnel in a Long-Term Care Institution After the First Wave of the Pandemic: A Cross-Sectional Study
Supplemental material, sj-docx-1-whs-10.1177_21650799221135587 for Seroprevalence of SARS-CoV2 Infections in Health Care Personnel in a Long-Term Care Institution After the First Wave of the Pandemic: A Cross-Sectional Study by Luis Alfredo Bautista Balbás, Rosa Sandino Gómez, Mario Gil Conesa, Olga Velasco Guijarro, Gil Rodríguez Caravaca, Fernando Jou Rivera, María Ángeles Navasquillo Lorda and Enrique Martín Carmena in Workplace Health & Safety
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.