
Abstract
Little is known about long-term care workers’ cardiovascular disease (CVD) risk. Thus, the authors used baseline objective and subjective data from 98 long-term care staff participating in a worksite health promotion study to provide a comprehensive CVD assessment. The median age of the sample was 32 years (SD = 13.38). Nine (12.2%) participants smoked and 27 (37.0%) participants reported exposure to secondhand smoke. The average nightly hours of sleep was 6.5 (SD = 1.18), with 24 (32%) participants reporting sleeping at least fairly bad. Sixty-eight participants (73.1%) were overweight or obese. The median aerobic activity was 0 (SD = 18.56). Participants ate on average 27 (SD = 17.34) servings of high fatty and/or salty foods per week. Although blood pressure and cholesterol levels were within normal limits, this population demonstrated poor behavioral CVD risk factors. Given this finding and the young age of the sample, these workers may be ideal candidates for health promotion efforts before health risk factors are present.
A number of risk factors have been identified as contributing to the burden of cardiovascular disease (CVD): smoking or exposure to secondhand smoke, body mass index (BMI) of 25 or greater, hypertension, hyperglycemia, hypercholesterolemia, limited physical activity (PA), little compliance with heart healthy eating recommendations, excess alcohol, and illicit drugs (Lim et al., 2013). Given the risk factors and current behaviors of Americans, it is not surprising that the prevalence of CVD is expected to rise from 37% to 41% by 2030. The increase in CVD is expected to result in total health care costs for CVD increasing from US$237 billion to US$818 billion by 2030. Indirect costs related to CVD will increase by 61%, rising to US$276 billion by 2030 (Heidenreich et al., 2011).
Health Promotion Programs for Health Care Workers
Health care workers are ideal candidates for health promotion programs because of their high risk for CVD and their availability at work. Research has shown health care workers have higher or similar rates of overweight or obesity, PA, and hypertension as the general population of the United States (N. Blake, Blayney, Loera, Rowlett, & Schmidt, 2012; H. Blake, Malik, Mo, & Pisano, 2011; Flannery, Resnick, Akpadiaha, & McMullen, 2014; Frank, Tong, Lobelo, Carrera, & Duperly, 2008; Schult, Awosika, Hodgson, & Dyrenforth, 2011; Zapka, Lemon, Magner, & Hale, 2009). In addition, the health behaviors of these individuals extend beyond personal benefit to potentially affect patient behaviors as these caregivers can be role models in regard to diet and PA. In addition, health care workers who adhere to heart healthy behaviors report more confidence in their ability to counsel patients on reducing risk factors for CVD and patients view these workers as credible health advocates (Alleyne, Hancock, & Hughes, 2011; H. Blake et al., 2011; Crawford et al., 2004; Lobelo, Duperly, & Frank, 2009). Last, facilitating healthy behaviors and optimizing the health of all employees in health care facilities can reduce missed workdays and maintain a consistent and productive workforce (Chapman, 2012; Goetzel et al., 2014; Goetzel et al., 2013; van Dongen et al., 2013).
Specific subsets of health care workers have demographic profiles that suggest they are at high risk for CVD due to nonmodifiable risk factors (e.g., gender, race, and socioeconomic status). Specifically, direct care workers are the largest employee group in long-term care, predominantly female (89%), a member of a racial minority (53%), and eligible to receive government assistance (49%; for example, Medicaid or food stamps; Paraprofessional Healthcare Institute, 2011). Despite known correlations between demographic characteristics and CVD risk, few studies have focused on the evaluation and management of CVD risk factors among workers in long-term care facilities. Therefore, the purpose of this study was to assess the prevalence of CVD risk factors among all employees in selected long-term care facilities. The findings from this study will guide the development of appropriate wellness programs for a priority population.
Method
This descriptive study used baseline data from a randomized trial testing the impact of a worksite health promotion (WHP) program in four assisted living settings. The four settings were located on the east coast of the United States in a metropolitan area. All four facilities were owned by the same company; therefore, the work contracts and positions within all settings were the same.
Sample
Participants were invited to learn about the study via printed information, conversations at staff meetings, and several “meet and greet” sessions where research staff were available to answer questions about the project. Long-term care staff were eligible to participate if they were 18 years or older, could read and write English, worked day and/or evening shifts, and were an employee of the facility. Participants were ineligible if they self-reported they were pregnant or could not provide informed consent. The Evaluation to Sign Consent test (Resnick, Rogers, Galik, & Gruber-Baldini, 2007), which includes five questions to assess participants’ understanding of study activities and risks, was completed prior to signing the consent form. The study was approved by a University’s Institutional Review Board, and all participants provided consent.
Across all the sites, 146 staff (43% of all staff) attended meet and greet sessions. Of these, six employees were not eligible: due to pregnancy (n = 2), working night shift (n = 2), not employed by the facility (n = 1), and below 18 years of age (n = 1). Among the 140 eligible staff members, 98 participants (70%) consented to participate in the study.
As shown in Table 1, the majority of workers were nurse aides (n = 19, 24.1%) and nurses (n = 18, 22.8%). Other participant job titles included housekeeper (n = 14, 17.7%), dietary service worker (n = 8, 10.1%), concierge staff (n = 7, 8.9%), activities staff (n = 4, 5%), kitchen staff (n = 2, 3%), maintenance (n = 1, 1%), and one individual who described the position as rotating (n = 1, 1%). The median tenure of participants working in the facility was 18 months (SD = 38.18), and the median age of the participants was 32 years (SD = 13.38). Most participants were educated beyond high school (n = 58, 65.2%) and non-Latino (n = 78, 95.1%). Approximately half of the sample was African American/Black (n = 47, 49.5%).
Select Demographic Characteristics (N = 98)
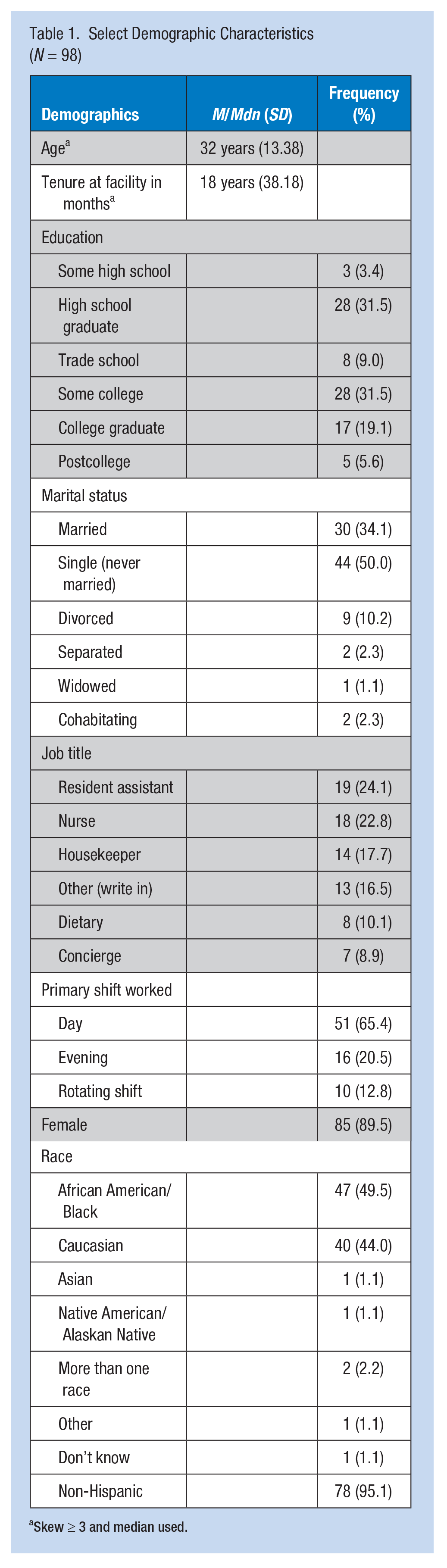
Skew ≥ 3 and median used.
Measures
Data collection was via a paper-and-pencil survey completed by the participants during the workday. As shown in Table 2, to assess CVD risk, the authors collected an evaluation of PA (via pedometer and the International Physical Activity Questionnaire), salt and fat intake (via the Modified Block Brief Food Questionnaire), physical measurements (i.e., weight, height, blood pressure, lipid panel, body fat, muscle mass, waist circumference), and psychosocial measurements (i.e., short version of the Depression Anxiety Stress Scale). Other demographic and CVD risk factors, personal information (e.g., age, race, past health history, prescribed medications), work characteristics (e.g., shift worked, job tenure), and personal habits (e.g., sleep hygiene, smoke exposure, alcohol intake), were assessed with nonstandardized scales.
Description of Study Measures
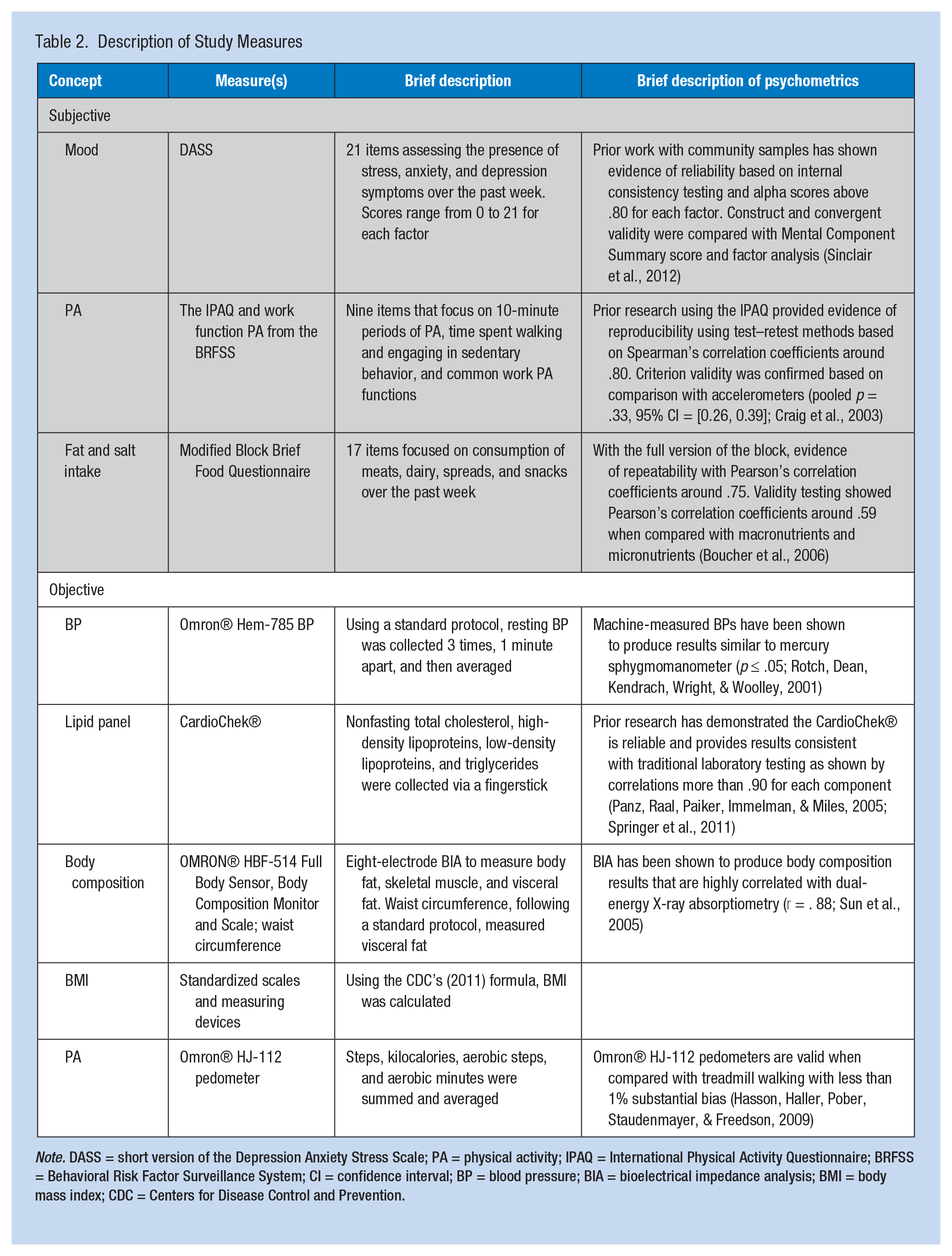
Note. DASS = short version of the Depression Anxiety Stress Scale; PA = physical activity; IPAQ = International Physical Activity Questionnaire; BRFSS = Behavioral Risk Factor Surveillance System; CI = confidence interval; BP = blood pressure; BIA = bioelectrical impedance analysis; BMI = body mass index; CDC = Centers for Disease Control and Prevention.
For objective data collection, equipment was purchased new for this project and used within 1 year. The Omron series 10 BP monitor auto-calibrates every time the machine is turned on, and control testing was instituted when the strips used for lipid testing had new lot numbers.
Data Analyses
Data analyses used SPSS Versions 16 and 17. Frequency data with percentages as well as means and medians with standard deviations were calculated to describe the prevalence of CVD risk factors among long-term care workers. All continuous CVD risk factors were assessed for skewness (defined as skewness/standard error of skewness ≥3). Twelve variables were noted to be skewed (i.e., age, job tenure, average alcohol drinks consumed per week, triglycerides, average daily steps, summed weekly aerobic minutes, average calories burned each week, self-reported minutes spent sitting each week, self-reported minutes engaged in exercise each week, total weekly servings of high fat and/or salty foods, combined weekly diet score, and cheese consumption), so median values were reported for these variables.
Participants were asked to wear pedometers for 7 consecutive days. If participants returned pedometers with missing data, they were given a second opportunity to provide complete PA data for 7 days. Using the data returned, an average daily steps value was created and used in the analysis. If participants returned no pedometer data, it was coded as missing (Flannery, Resnick, Galik, et al., 2012). If participants were taking antihypertensive or lipid-lowering medications, they were so coded and reviewed separately to determine if their blood pressures or lipid levels were within recommended guidelines.
Results
CVD Health Risk Factors
The average systolic BP was 114.38 (SD = 14.12) and diastolic BP was 77.49 (SD = 9.73). Eleven (11.3%) participants were hypertensive, and four (4.1%) participants reported taking antihypertensive medicine. Of the participants taking antihypertensive medications, one was hypertensive (i.e., ≥140 and/or ≥90) and three had elevated blood pressure (i.e., ≥120 and/or ≥80; Go et al., 2013). The average total cholesterol to high-density lipoprotein (HDL) ratio was 3.98 (SD = 3.94), with 22 (24.2%), 29 (33.7%), and 59 (64.8%) participants with elevated total cholesterol, elevated low-density lipoprotein (LDL) levels, and low HDL levels, respectively. Four (4.1%) participants reported taking a cholesterol-lowering medication or supplement; of these four, two had normal lipid panels. The sample’s average BMI was 30.55 (SD = 7.33); 68 participants (73.1%) were overweight or obese. The average waist circumference was 39.14 (SD = 6.62).
CVD Behavioral Risk Factors
As shown in Table 3, nine (12.2%) participants smoked and 27 (37.0%) participants reported exposure to secondhand smoke. Forty-four (57.9%) participants reported currently drinking alcohol regularly and on average consumed two (SD = 4.35) drinks per week. The average hours of sleep reported each night was 6.5 (SD = 1.18), and 24 (32%) participants reported sleeping fairly bad or very bad. Participants believed they spent most of their work time walking (n = 35, 46.1%). The sample’s median self-reported sitting time each week was 240 (SD = 217.73) minutes. Objectively, the median daily step average was 5,902.71 (SD = 4,184.43), and using established PA criteria (Tudor-Locke, Hatano, Pangrazi, & Kang, 2008), this finding placed 63 participants (73.2%) in the sedentary or low activity category. The sample’s median objective minutes in aerobic activity was 0 (SD = 18.561), and the median calories burned was 191.01 (SD = 116.64) kcals per day. When participants were asked about their intake of 17 common foods high in fat and/or salt, they reported they ate a median of 27 (SD = 17.34) servings a week of these types of foods. Overall, this finding resulted in a median of 1,367.95 mg (SD = 819.54) of sodium and an average of 34.14 g (SD = 28.31) of fat consumed each day. The most common foods consumed were butter (M = 3.29, SD = 2.59) and cheese (Mdn = 3.00, SD = 2.77). Some participants reported multiple negative mood symptoms (e.g., depression and anxiety), but 24 (30.4%), 16 (20.3%), and 8 (10.1%) participants reported experiencing at least mild symptoms of anxiety, stress, and depression, respectively, within the previous week. Twelve (12.2%) participants reported they were prescribed mental health medication(s).
Cardiovascular Disease Risk Factors of Long-Term Care Staff (N = 98)
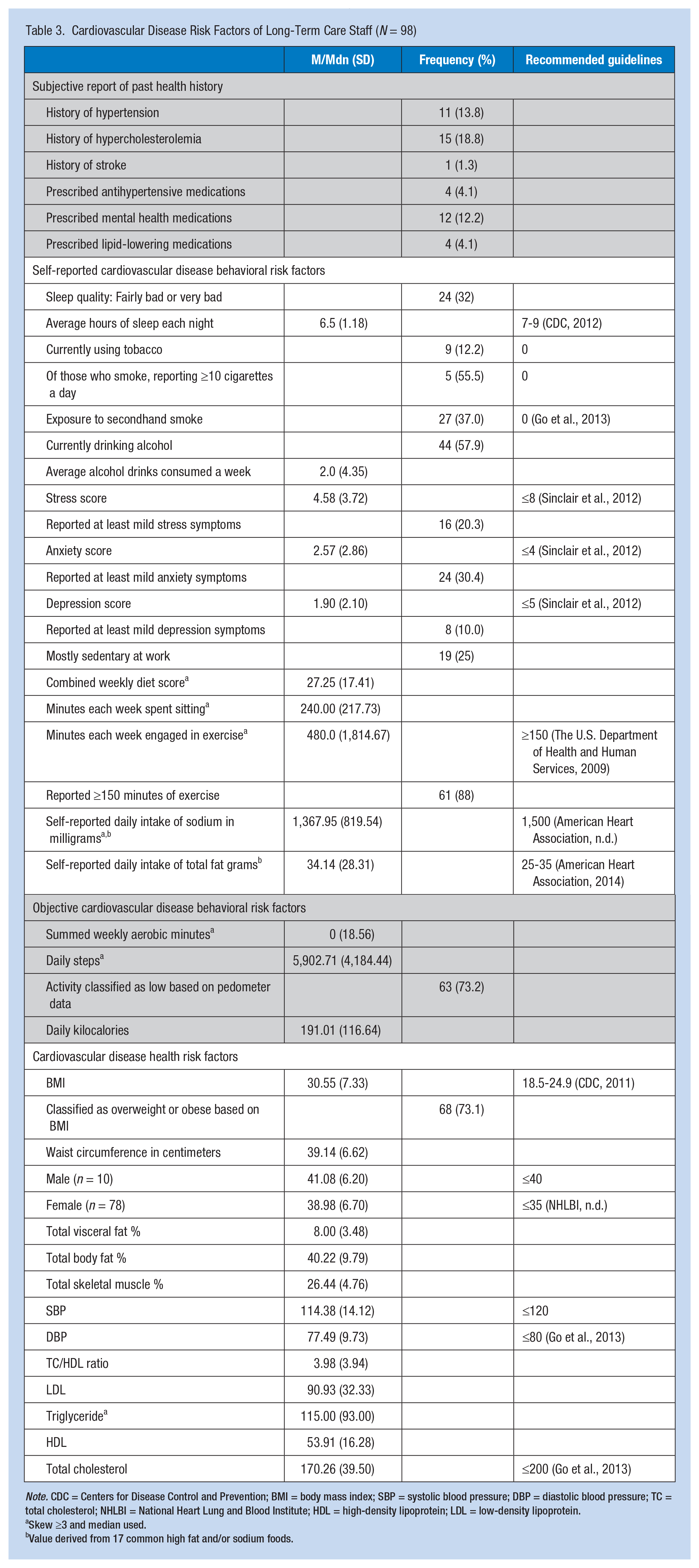
Note. CDC = Centers for Disease Control and Prevention; BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; NHLBI = National Heart Lung and Blood Institute; HDL = high-density lipoprotein; LDL = low-density lipoprotein.
Skew ≥3 and median used.
Value derived from 17 common high fat and/or sodium foods.
Discussion
CVD Risk Factors
Generally, this sample of health care workers had no evidence of CVD health risk factors as they were, overall, normotensive, and lipid panels were within normal limits (except for HDL levels) based on guidelines from the American Heart Association (Go et al., 2013). These findings are inconsistent with prior findings that suggest health care workers have a higher prevalence of CVD health risk factors (e.g., hypertension, hypercholesterolemia) compared with the general population (Flannery, Resnick, et al., 2014; Schult et al., 2011). One possible reason for the discrepancy is that this study sample was younger than those surveyed in prior studies (i.e., mean age of 32 vs. a mean age of 41; Flannery, Resnick, Galik, et al., 2012). Other possible explanations for this finding include varying demographic profiles (e.g., race and gender, family histories, or genetic profiles) among study participants.
CVD Behavioral Risk Factors
Study participants did report health behaviors that increase their risk of CVD. Prior literature has likewise noted that young adults may present with ideal cardiovascular health factors (e.g., BP within normal limits) but engage in nonideal behaviors for cardiovascular health (e.g., low/no engagement in PA; Fang, Yang, Hong, & Loustalot, 2012; Folsom et al., 2011; Shay et al., 2012). Specifically, study participants were overweight or obese, ate high fat and/or sodium diets, engaged in little PA, were exposed to tobacco smoke, and reported poor sleep hygiene.
Weight
As noted among other groups of health care workers, almost three quarters of the study sample (n = 68, 73.1%) were overweight or obese; nationally 64.5% of Americans are overweight or obese (Behavioral Risk Factor Surveillance System & CDC, 2015; Flannery, Resnick, et al., 2014; Schult et al., 2011). This higher rate of obesity among health care workers increases their risk of CVD as well as other diseases such as diabetes (Go et al., 2013; King, March, & Anandacoomarasamy, 2013; National Cancer Institute, 2012). Furthermore, obesity and its sequelae indirectly affect not only workers’ health but also their work productivity (Gates, Succop, Brehm, Gillespie, & Sommers, 2008; Goetzel et al., 2010), absenteeism (Neovius, Johansson, Kark, & Neovius, 2009), and early withdrawal from the workforce (American Diabetes Association, 2013; Rosen, Stiehl, Mittal, & Leana, 2011).
Diet
The study sample was noted to have at least a moderate intake of food high in fat and/or salt. The survey to assess diet only included 17 items; using these 17 items alone, the sample reported eating foods just below the sodium and fat intake recommendation levels (American Heart Association, 2014). This finding combined with prior reports suggesting subjective assessments of food intake generally underreport actual fat and sodium intake especially among individuals with high BMI (Johansson, Wikman, Åhrén, Hallmans, & Johansson, 2001); the authors suspect the study sample actually consumed more than the recommended levels of dietary fat and sodium. This suspicion is consistent with the finding that only 1% of Americans meet heart healthy nutrition guidelines (e.g., recommendations for salt; Go et al., 2013). Health care workers in these settings certainly experience similar barriers to heart healthy eating (e.g., lack of time, resources, and knowledge) as other Americans and also face unique work-related challenges (increased levels of job stress, lack of uninterrupted break time, and shift work; Flannery & Resnick, 2014; Puttonen, Härmä, & Hublin, 2010; Zunker et al., 2008).
Physical Activity
Despite the high percentage of participants that reported meeting exercise guidelines (88%), when objectively measured the sample’s median daily steps was low and median minutes engaged in aerobic activity was extremely low, well below the recommended guidelines (The U.S. Department of Health and Human Services, 2009). This discrepancy between objective and subjective reports is typical (Troiano et al., 2008), and perhaps more often seen in populations who do not understand exercise guidelines as well as populations who do not perceive their jobs as sedentary (e.g., health care; Flannery, Burket, & Resnick, 2014). Prior studies have found health care workers record few pedometer steps per day and low weekly aerobic activity (N. Blake et al., 2012; Flannery, Resnick, Galik, et al., 2012). The barriers to engaging in regular PA are likely similar to those for the general population and are particularly similar to barriers experienced by low-income, minority women (e.g., lack of perceived need to engage in heart health behaviors, Harkins et al., 2010; Moore-Greene, 2012; and lack of time or conflicting responsibilities, Flannery & Resnick, 2014; Harley, Odoms-Young, Beard, Katz, & Heaney, 2009; Zunker et al., 2008). In addition, the same reasons that long-term care employees find eating a heart healthy diet challenging are similar to the reasons these employees struggle to engage in PA.
Smoking and secondhand smoke exposure
Only 12.2% of the study sample reported currently smoking, but 37% reported exposure to secondhand smoke. Comparing active tobacco use in this sample with American smokers demonstrated that the study sample smoked less than the national average. However, when comparing secondhand smoke exposure between the study sample and the nation, the study sample was above the national average of 25% (CDC, 2015). Secondhand smoke exposure increases CVD risk by 25% to 30% (Dunbar, Gotsis, & Frishman, 2013). This finding is, therefore, important to consider when developing WHP programs. Educational components of such programs should increase participants’ understanding of the negative impact of secondhand smoke and how to approach individuals who are smoking in their living environments (O’Donnell, 2014).
Sleep hygiene
Increasingly, evidence suggests that individuals who sleep on average less than 6 hours a night have a 15% greater risk of CVD compared with individuals who sleep the recommended hours each night. Furthermore, those who report low sleep quality and less than 6 hours of sleep a night can experience a 63% greater risk of CVD than individuals with better sleep quality and more sleep hours (Grandner, Sands-Lincoln, Pak, & Garland, 2013). Healthy sleep patterns among workers in long-term care can be particularly challenging due to shift work, multiple jobs, and mandatory overtime. The average hours of sleep per night in the study sample were 6.5, and almost one third reported sleeping fairly bad or very bad. These findings are consistent with prior reports suggesting the health care industry has among the highest percentage of employees who report sleeping less than 6 hours a night (CDC, 2012). Future WHP programs should explore sleep interventions with this population not only to reduce CVD risk but to improve patient outcomes and increase return on investment as sleep deprivation among health care workers has been linked to work productivity (Henwood, Tuckett, Bagadi, & Oliffe, 2015; Johnson et al., 2014). Future studies should also consider objectively monitoring sleep using sophisticated devices such as the MotionWatch.
Limitations
This study is a critical first step in assessing the cardiovascular health status of all employees working in long-term care facilities. However, the study is limited by a small convenience sample from four long-term care facilities (N = 98) in the Baltimore metro area. Thus, this sample may not be representative of all staff working in all long-term care facilities. The authors recognize that the compilation of staff could be very different in other parts of the country. Thus, future research should replicate this work in other areas of the United States. Although the authors aimed to provide a comprehensive cardiovascular health status assessment of all workers in long-term care settings, 47% of the sample were nurses and nursing assistants and the remainder of the sample were other workers (e.g., housekeepers). Due to the limited sample and various types of workers, the data can only be used to preliminarily describe the cardiovascular health status of long-term care staff. Although the study assessed many risk factors for CVD, it did not assess all CVD risk factors such as blood glucose and illicit drug use. Furthermore, subjective data can be biased by lack of knowledge and social desirability. Several measures, such as sleep and tobacco exposure, were assessed subjectively and with nonstandardized scales; thus, the results may be biased.
Regarding objective data, the use of pedometers presented challenges. Although participants were reminded to wear their pedometers, situations arose in which participants returned pedometers with missing data so the authors were unable to calculate an average based on 7 days and had to use the data provided. Furthermore, the pedometers used in the study defined aerobic activity as at least 10 minutes of consecutive PA and at least 60 steps per minute. However, prior research suggests the lowest threshold for aerobic activity should be 100 steps per minute; thus, this finding may have overestimated the aerobic activity of the sample (Tudor-Locke et al., 2008). Last, lipid panel assessments were drawn nonfasting. Although prior research has noted (Langsted, Freiberg, & Nordestgaard, 2008) lipid testing is only minimally affected by individuals’ nonfasting status, intake might have introduced biases especially with triglyceride levels. Despite these limitations, these data provide valuable information for future health promotion efforts among a population not commonly studied and with high-risk health behaviors but no identifiable disease.
Implications for the Occupational Health Team
The findings from this study indicate that staff working in long-term care facilities report health behaviors that put them at risk for CVD. The data demonstrate facility-wide programs that focus on CVD risk reduction could be beneficial for long-term care employees. Given these risky behaviors and the age of the sample, these workers are ideal candidates for WHP programs that aim to reduce CVD risk factors before midlife and before CVD is diagnosed. If these workers can reach midlife without CVD health risk factors, their probability for developing CVD may be reduced (Berry et al., 2012).
Research has shown that employers who offer WHP programs receive a significant return on investment in reduced employee health care costs, absenteeism and turnover, and improved work productivity (Baxter et al., 2015; Chapman, 2005; Pronk, 2009; Serxner, Gold, Meraz, & Gray, 2009). Although WHP programs for health care workers implemented during paid work time can be challenging due to the ongoing needs of residents (Flannery, Resnick, & McMullen, 2012; Sorensen et al., 2016), work time opportunities if provided in short duration at convenient times for staff are feasible and effective (Flannery, Resnick, Galik, et al., 2012).
The findings from this study can be used to guide future WHP program activities to optimize outcomes. Currently, the majority of WHP programs do not focus on all areas of CVD risk; they mainly focus on PA and/or healthy eating. Workplace health promotion programs should use a more comprehensive approach and address nontraditional risk factors such as exposure to secondhand smoke, job stress, mental health issues, and sleep. Future programs may consider using national composite measures to assess CVD risk (e.g., American Heart Association’s [AHA] Life’s Simple 7; Sacco, 2011).
Applying Research to Practice
This article provides a comprehensive assessment of behavioral and health risk factors for CVD in a high-risk population. The data suggest this is an ideal population for health promotion intervention due to high-risk behavioral factors in the absence of health risk factors. The article adds to the literature by demonstrating areas of risk that are often not addressed in WHP programs. This information can be used to guide program development for future WHP programs with this population and in this work setting.
Footnotes
Acknowledgements
We would like to thank Zackary Holtzman for his technological support and data entry. We would also like to thank the sites and the participants for allowing us to work with them.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the American Heart Association (Grant 14CRP20480034).
Author Biographies
Kelly Doran is an assistant professor at the University of Maryland, Baltimore, School of Nursing.
Barbara Resnick is a professor at the University of Maryland, Baltimore, School of Nursing.