
Abstract
Posttraumatic stress disorder (PTSD) is a serious mental health concern for returning U.S. military personnel who have a higher prevalence rate of PTSD than the general population. Among the military population, reserve service members are at increased risk of developing PTSD compared with full-time active duty service members mainly due to difficulty reintegrating into civilian life. Understanding the social risk factors along with the protective effects social support has on PTSD in veterans will provide occupational health professionals the opportunity to support reserve veterans with adjustment into post-deployment life. This literature review examines PTSD in reserve veterans, with a focus on occupational factors, social factors, guideline recommendations, available resources, as well as provides suggestions for occupational health nurses caring for reserve veterans returning to the workplace.
Following the First Gulf War (1990-1991), the size of the active duty military force was reduced by nearly 40% in an effort to decrease federal military spending (Department of Defense [DOD], 1995, 1999). However, multiple wars have not reduced the need for large numbers of military personnel that have been essential in meeting the U.S. military mission in many regions of the world. The recent wars in Afghanistan and Iraq (2001-present) have resulted in large-scale mobilizations of U.S. military personnel composed of full-time active duty as well as reserve service members. Unlike the active duty service member who may reside on base and work as a full-time military employee, a reserve service member, or reserve, lives and works in a non-military capacity until the need arises for more military personnel at which time they are called to active duty.
Prior to the First Gulf War (1990-1991), reserves experienced fewer deployments of shorter duration than those deployments over the last two and a half decades of U.S. military conflict. Activated reserves accounted for approximately 49% of all military personnel deployed during the conflicts in Afghanistan and Iraq (2001-present) surpassing the number deployed during the First Gulf War (1990-1991) by as much as 50% (Griffith, 2011). Reserve personnel now experience multiple and longer deployments of 1 or more years, and it is not uncommon for reserve service members to indicate they have had three or more deployments during their reserve career.
When military reserves transition to active duty, they leave behind family and full-time civilian jobs, and are deployed to an environment where their jobs as soldiers are first priority and any other skilled job becomes secondary. A higher rate of posttraumatic stress disorder (PTSD) has been shown in reserves over active military personnel due to reintegration difficulties associated with the abrupt interruption in and out of civilian life. Reintegration difficulty is one of the most significant psychosocial factors contributing to the increased risk for PTSD among reserves (Griffith, 2011; Hoge, Auchterlonie, & Milliken, 2006). PTSD in reserve service members has been associated with lower social and emotional support as well as impairments in post-deployment social, familial, and work functioning (Kehle et al., 2011).
Occupational health nurses should possess special knowledge of PTSD in reserve veteran employees and recognize its impact on mental health in and out of the workplace. Assessment, screening, coordinating care with mental health providers, workplace education, and maintaining a supportive work environment provide a collaborative support system to aid in the reintegration of reserve veterans into the workplace as well as the community.
Background and Epidemiology
PTSD
PTSD is a chronic mental health disorder that follows an exposure to a traumatic event. Symptoms include continually re-living the experience (flashbacks, nightmares), trauma stimuli avoidance, numbing, intrusive thoughts, hyperarousal, hypervigilance, poor concentration, having negative thoughts and feelings, as well as feeling socially distant and isolated (Cardenas et al., 2011; Cohen et al., 2013; U.S. Department of Veteran Affairs/Department of Defense [VA/DoD], 2010). PTSD is diagnosed when symptoms persist beyond 1 month and cause an impairment in daily functioning (American Psychiatric Association, 2000; Godfrey, Lindamer, Mostoufi, & Afari, 2013).
Prior to 1980, terms used for PTSD symptoms throughout past wars included shell shock, combat fatigue, and soldier’s heart (U.S. Department of Veteran Affairs, n.d.). Traumatic stress symptoms have evolved into what is now recognized in the American Psychiatric Associations’ Diagnostic and Statistical Manual (DSM) as PTSD (Davidson et al., 2004).
Prevalence
PTSD has a lifetime prevalence rate of as high as 31% in military service members compared with 6% to 8% among the general population (Godfrey et al., 2013). Prevalence rates among veterans are 30% in Vietnam Era veterans, 10% among First Gulf War (1990-1991) veterans, and 22% among Afghanistan and Iraq War (2001-present) veterans.
Since 9/11, approximately 2.2 million living veterans have served in Afghanistan and Iraq and most have experienced some type of war-related trauma (VA, n.d.). Between 2002 and 2008, PTSD prevalence rates in 289,328 military veterans ranged between 17% and 22%. Of this number, 36.9% were newly diagnosed with a mental health disorder, 21.8% with PTSD, and 17.4% with depression (Seal et al., 2009).
Milliken, Auchterlonie, and Hoge (2007) reported that of the 88,000 soldiers who returned from Iraq, 42% of reserve soldiers needed mental health treatment for PTSD, major depressive disorder, and/or other mental health disorders compared with 20.3% of full-time active duty soldiers.
Risk Factors
Common traumatic combat experiences that typically result in PTSD include improvised explosive device (IED) blasts, killing enemy combatants, being fired upon, witnessing death or serious injury, fearing loss of life, and being unable to prevent or stop tragic situations (Ashley, Honzel, Larsen, Justus, & Swick, 2013). Although many veterans have faced combat, experiences do not have to be combat related to induce PTSD. Physical stressors during deployment include harsh living conditions, fatigue, sleep deprivation, hunger, harsh climates, high impact noise, and hazardous environmental exposures. Psychosocial stressors during deployment such as separation from family, interruption in career, feelings of inadequate experience or training, and daily life concerns act as sources of stress that could result in an increased risk for PTSD as well (Shea, Reddy, Tyrka, & Sevin, 2013; Spelman, Hunt, Seal, & Burgo-Black, 2012; VA/DoD, 2010).
In addition to physical and psychosocial stressors experienced during deployment, social stressors and low levels of social support upon returning home have emerged as independent risk factors for PTSD in veterans (Shea et al., 2013). PTSD is also commonly associated with coexistent mental health conditions that include depression, alcohol abuse, substance abuse, sleep disturbances, and anxiety disorders (VA/DoD, 2010). It has also been correlated with unhealthy behaviors and overall poor health in military veterans (Cohen et al., 2013; Godfrey et al., 2013).
Review of Relevant Literature on Veteran Social and Occupational Reintegration
Occupational Functioning
The high prevalence of PTSD and reintegration difficulty among post-deployment service members has been associated with impairments in occupational functioning among veterans reentering the workplace. Lower levels of functioning within work environments have been shown in veteran service members with PTSD, depression, and/or alcoholism. Veterans with a PTSD diagnosis showed higher rates of work role deterioration over any other mental health diagnoses in returning service members following Iraq War deployment (Erbes, Kaler, Schult, Polusny, & Arbisi, 2011).
Several studies have suggested that effective social support networks have been shown to be a significant protective factor for PTSD symptoms. Price et al. (2013) suggested that emotional support improved PTSD symptoms in returning Afghanistan and Iraq War veterans. Perceptions of safety elicited better compliance and reinforcement of PTSD treatment, which led to improved coping mechanisms in veterans.
Pietrzak et al. (2010) found that social and unit support formed a protective effect on psychosocial functioning and protected against PTSD symptom severity in Afghanistan and Iraq War veterans. Hinojosa and Hinojosa (2011) suggested that military friendships acted as an important resource during post-deployment reintegration. Veterans felt close bonds with their military comrades and the friendships provided protective social support during times of stress. The study suggested that reserve service members experienced less social and emotional support than active duty personnel in terms of military friendships due to difficulty retaining connections once outside of the unit assembly and recommended further investigation into this finding.
Cognitive Factors
Cohen et al.’s (2013) Mind Your Heart Study examined the association between PTSD and cognitive function while evaluating health behaviors. The study suggested that the differences in cognitive function among participants with PTSD were accounted for by modifiable health behaviors and should be further examined as potential targets for preventing the negative cognitive impacts of PTSD.
Ashley et al. (2013) examined the effects of combat-related words (e.g., insurgent, gunmen, IED) on cognition in Afghanistan and Iraq War veterans with PTSD. The study findings showed a significant cognitive interference from combat-related words. Findings also supported other theories of hyperarousal symptoms of PTSD from trauma-related stimuli and difficulty with disengaging attention from the unpleasant stimuli.
Physiological Factors
Veterans with PTSD have shown impairments in mental health functioning that have emerged in the wake of deployment (McAndrew et al., 2013). Pitman et al. (2012) found that the most significant structural abnormality in magnetic resonance imaging (MRI) studies of patients with PTSD was decreased volume of the hippocampus. The hippocampus and amygdala control the recognition of both safety and danger, functions regulating memory, and functions eliciting fear and stress responses.
The hypothalamic–pituitary–adrenal (HPA) axis is a major component of the brain’s stress response. The HPA activates the sympathetic nervous system (SNS) during the stress response resulting in increased production of cortisol. Over-activity of the SNS from repeated stressful stimuli results in over-exposure to glucocorticoids, which can lead to increased cerebral inflammation, atherosclerosis, cerebral ischemia, and neurodegeneration (Cardenas et al., 2011; Cohen et al., 2013).
Neuroimaging studies have also shown decreased gray matter volume in prefrontal brain regions in individuals with severe PTSD symptoms (Pitman et al., 2012). PTSD-associated neurodegeneration and structural changes in parts of the limbic system and frontal lobes have been shown to have a significant effect on cognitive functions such as memory and learning (Cardenas et al., 2011; Cohen et al., 2013).
Guidelines, Practices, and Policy
Following the Vietnam and Gulf Wars, veterans have re-entered civilian life with very few resources available to aid in their reintegration. Over the last 15 years, a significant increase in the demand for mental health treatment services for returning Afghanistan and Iraq War (2001-present) veterans experiencing signs of PTSD has been noted. According to the Veteran Health Administration Office of Public Health (2014), approximately 326,000 veterans of the Afghanistan and Iraq Wars have been evaluated for PTSD since active duty deployment. The VA is now able to identify and track access to care for veterans with mental health needs via the implementation of the Iraq and Afghanistan veteran registry and the Primary Care–Mental Health Integration (PCMHI) system (Brawer et al., 2011; Elnitsky et al., 2013). In an effort to meet the mental health needs of veterans with PTSD, nearly 200 specialized treatment programs have been designated throughout the United States and all VA Medical Centers offer PTSD treatment by PTSD specialists regardless of whether they have a specific PTSD program. All regions have specialized inpatient and outpatient programs within the Veterans Integrated Service Network (VISN) to treat individuals with PTSD (United States Department of Veteran Affairs, Veteran Health Administration, n.d.).
The VA/DoD (2010) has developed clinical practice guidelines for the management of PTSD for health professionals providing care to veterans. The guidelines include recommendations for initial and routine screening, assessment and diagnosis, and evidence-based management through collaborative care. An initial screening followed by annual screenings using a validated PTSD screening tool can improve early detection of PTSD as well as later detection of delayed symptoms. Many veterans may not show any symptoms of PTSD for several months after active duty release, which could lead to the disorder going undetected by health service providers (Milliken et al., 2007). Symptoms can have a delayed onset of at least 6 months after trauma exposure, and have even been documented to last as long as 45 years after combat experience (Spiro, Schnurr, & Aldwin, 1994; VA/DoD, 2010).
Screening tools that can be used in primary care and occupational settings include the Primary Care PTSD Screen, the PTSD Brief Screen, the Short Screening Scale for DSM-IV Defined PTSD (Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; APA, 1994), and the PTSD Checklist (VA/DoD, 2010).
Relevance to Occupational Health Nursing
Reserve veterans may return to work following deployment with an existing VA diagnosis of PTSD or may not show any obvious signs or symptoms of the disorder. Occupational health nurses can identify employees’ current military status through a thorough health and occupational history as well as physical examination. Military status can determine whether risk factors for PTSD or other mental health conditions may be present and an optimal worker plan of care can be initiated. A VA/DoD-recommended screening tool should be used in the occupational setting, and if the screening renders positive results, a referral to a specialized PTSD treatment facility or mental health professional can be facilitated; the worker’s plan of care should be modified to meet specialized mental health needs within the workplace.
Unfortunately, a stigma exists in society surrounding military active duty service, combat, and PTSD, which could affect an occupational setting that lacks military culture awareness. A lack of social support for veterans can exacerbate feelings of isolation and lead to social distance as well as the overall avoidance of a veteran seeking social support from coworkers and peers (Blais, Renshaw, & Jakupcak, 2014). It is important for employees and employers to be educated on the possible psychological effects associated with military deployment and the significance of a supportive social network provided to veterans in the workplace. Workplace education on PTSD awareness as well as suggestions for showing supportive behavior toward veterans could include the following:
Avoidance of using combat-related words around veterans, which could elicit negative cognitive effects (Ashley et al., 2013).
Recognition of PTSD symptoms that could cause alarm or offense in coworkers, which include but are not limited to agitation, irritability, anxiety, hypervigilance, change in alertness, memory problems, poor concentration, suspiciousness, and an inappropriate emotional response (VA/DoD, 2010).
A no-tolerance policy for stigmatizing military service and PTSD in the workplace.
Awareness of the positive effects that social and emotional supports have on PTSD in veterans.
The occupational health nurse may identify veteran employees experiencing overwhelming PTSD symptoms in the workplace or encountering unsupportive coworkers. Both sources of stress could lead to impairments in employees’ ability to perform their job duties. The Work Loss Data Institute (2013) has made recommendations for stress management in the workplace that could be used for veterans with PTSD, which include the use of the following:
Relaxation techniques (such as meditation)
Exercise that has shown to positively influence mood
Behavioral training (time management, anger management, conflict resolution training)
Modified work
Organizational interventions
The Work Loss Data Institute (2013) also suggests that although
time off work may be helpful, the ultimate goal should be to preserve the worker’s ability to function both occupationally and socially. Time off should not be so excessive that employees lose their sense of function and appreciation at work and at home.
It is important for veteran employees to remain working in functional capacities with the best possible social support network available in the workplace. The workplace may be the only source of social support for reserve veterans with low levels of support from family and peers. Occupational health nurses should be familiar with community resources for veterans and encourage the joining of support groups such as veteran peer support groups, as well as other local support groups such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) if needed (see Table 1 for online resources).
PTSD Online Resources for Providers
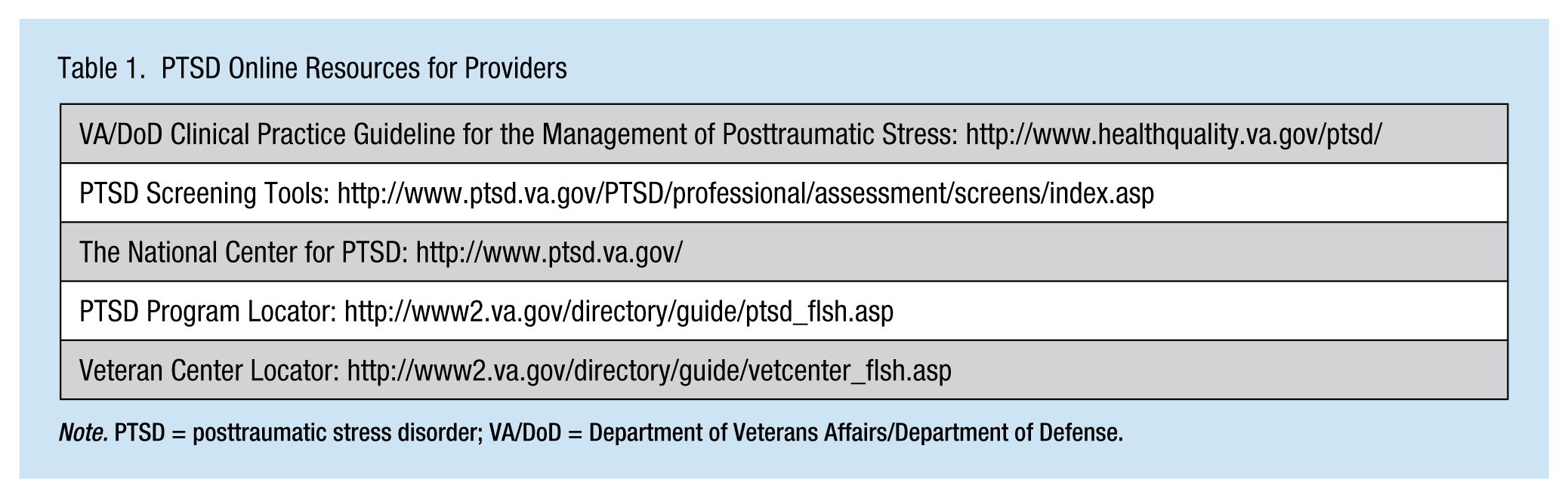
Note. PTSD = posttraumatic stress disorder; VA/DoD = Department of Veterans Affairs/Department of Defense.
Summary
Literature suggests that a social support network for veterans reentering the workforce not only leads to higher levels of work functioning but also provides significant protective factors for PTSD symptoms (Erbes, Kaler, Schult, Polusny, & Arbisi, 2011; Pietrzak et al., 2010). In addition to the assessment and screening for PTSD symptoms, facilitation of appropriate specialist referrals, and providing mental health support to employee veterans, education and a workplace policy that promotes veteran support are fundamental in meeting the social support needs of reserve veteran employees. A work culture with the awareness of what service members may have endured during active duty as well as what they endure coping with post-deployment life may garner a new appreciation for military service or reinforce the appreciation that may already exist within the workplace.
In Summary
PTSD rates in U.S. military service members and veterans are two to three times higher than in the general population. PTSD rates among reserve veterans are significantly higher than in full time military personnel as a result of problems associated with reintegrating back into civilian life.
Reserve veterans transitioning back into the workplace may experience PTSD symptoms which can impair occupational functioning. Effective social support can improve PTSD symptoms in veterans and decrease work role deterioration.
Occupational health nurses can effectively support veterans with PTSD in the workplace by performing PTSD screening, facilitating specialist referrals, providing collaborative mental health support, and educating employees. Workplace education should include awareness of the psychological effects of war on veterans, the significant positive effects of social support, recognition of PTSD symptoms, as well as a zero tolerance for unsupportive behaviors.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Ms. Henderson is an Occupational/Adult Nurse Practitioner graduate student, University of South Florida Sunshine Education and Research Center, Tampa; and a Registered Nurse, South Lake Hospital, Clermont, FL.
Dr. Burns is Colonel (U.S. Army Reserve, Retired), Professor and Director, Dual Degree Program ANP/Occupational Health Nursing, and Deputy Director, USF Sunshine Education and Research Center (SERC), University of South Florida, Tampa, FL.