
Abstract
Objectives:
The Coronavirus-2019 (COVID-19) pandemic presents a unique burden specifically for workers in service industries. However, limited research on service worker’s experience during the onset of COVID-19 exists. We aimed to describe the experiences and concerns of service industry workers during the pandemic’s onset.
Methods:
This is a mixed-method study. Participants were recruited through social media and completed either a survey or a phone interview during May and June 2020. The survey and transcribed interview data were analyzed using the SPSS software and content analysis, respectively.
Results:
Twenty-seven individuals completed audio-recorded phone interviews and 28 completed the survey. Participants were mostly women between 19 and 65 years old. Participants worked in food retail (n = 23), restaurant (n = 25), and hospitality (n = 7) industries. There was discordance in perceived threat level of COVID-19. Most participants reported that their workplace complied with their state’s mandates for protection measures, while others reported lacking basic supplies such as soap, hand sanitizer, and masks. Job insecurity, change of job tasks, and work hours were the most common ways that COVID-19 affected the workers. Worker’s assertiveness to self-protect while at work was influenced by their perceived severity of the pandemic.
Conclusion/Application to Practice:
This study highlights the vulnerability of service workers relating to job security and job tasks during the pandemic. Organizational processes are needed to promote safe work environments and facilitate access to resources for these workers. In addition, occupational health practitioners need to be aware of and address the emerging health risks and worker needs.
Background
Service industry jobs such as hospitality, food services, and food retail are characterized by poor job security, low-wages, and minimal access to benefits (Baum et al., 2020; Grimshaw, 2011). Workers in these subsectors were disproportionately affected during the early phases of Coronavirus-2019 (COVID-19) pandemic (Cubrich, 2020). At the onset of the pandemic, businesses within those industries either experienced a significant loss of staff or even closed due to a combination of low customer demands and lockdown orders. Nearly a quarter of independent restaurants did not survive the initial 2 months of the pandemic (Brizek et al., 2021). Of those that survived, Brizek et al. (2021) found that 65% of independent restaurant operators projected they would have to close if COVID-19 restrictions persisted through the end of 2020.
Unemployment at the start of COVID-19 (i.e., March and early April 2020) was significant for the hospitality industry (8.3 million, or about 50%) and the food service industry (6 million, or about 50%; Bureau of Labor Statistics [BLS], 2021b, 2021d). Food retail did not experience significant unemployment because demand for groceries remained high during this period (BLS, 2021a). December 2020, 45 states and the District of Columbia had increased rates of joblessness compared with December 2019 (BLS, 2021c). The resulting job insecurity in the hospitality industry made existing vulnerabilities and disparities in health and worker protections far worse (Sönmez et al., 2020). Lund and colleagues (2020) stated, “The workers bearing the brunt of the initial shock [of the pandemic] are the very people least equipped to weather it (p. 6).” Lund et al. found that a vast majority (86%) of jobs—many of which were in the service sector—affected by the initial impact of COVID-19 paid under US$40,000 annually (Lund et al., 2020). In fact, 98% of employees who were affected through furloughs, layoffs, and reductions in income held jobs that fell short of the U.S. living wage for a family of four (US$68,808). Forty-two percent of these vulnerable jobs are from just two industries: (a) accommodation and food services and (b) retail, which disproportionately affects minorities including immigrants (Lund et al., 2020; Sönmez et al., 2020).
Workers in hospitality (particularly those who work in hotels), food service, and retail are at greater risk for COVID-19 exposure not only due to their essential, in-person work environment but also due to factors collectively known as “social determinants of health” such as language barriers, education level, health literacy, multi-family and multi-generational cohabitation, social customs, shared transportation, and trust of their employer (Kalia et al., 2020).
At the first surge of the pandemic, despite the many uncertainties, the U.S. federal government proposed some measures not only for the general public but also for employers to adapt to protect workers. To slow the spread of COVID-19, the Centers for Disease Control and Prevention (CDC) recommended all individuals keep 6-feet apart, wear a mask, and frequently wash hands with soap and water (CDC, 2020a, 2020b, 2020c). Industries were provided additional recommendations, which included cleaning and disinfecting frequently touched surfaces and staying home when sick. The three service industries of interest—hospitality, food service, and food retail—were given specific recommendations by the CDC to protect both employees and customers from COVID-19 (CDC, 2020a, 2020b, 2020c).
In hospitality, for example, the room cleaners were advised to wash their hands before and after cleaning guest rooms, wear disposable gloves when handling dirty laundry or trash, throw away single-use items, not shake dirty laundry, and wash all hotel linen in the warmest water setting. In addition, if a guest was isolating in their room with the virus, all but essential housekeeping services were required to be discontinued. Once the guest left, it was recommended that 24 hours passed prior to any cleaners entering the room. In addition, it was recommended that a vacuum with High Efficiency Particulate Air (HEPA)-filters were recommended to be used (CDC, 2020c).
For the food service industry, the CDC advised employers to collaborate with state and local officials; clearly communicate their safety protocols with vendors, staff, and customers; and rotate or stagger shifts. Employers were also recommended to reduce shared items, avoid self-serve options, provide touchless payment options, limit seating to increase social distancing, install physical barriers, and increase ventilation (CDC, 2020a; Parks et al., 2020).
The CDC recommended employers in the food retail industry to provide their employees with access to handwashing, hand sanitizer, disinfectant wipes, as well as flexible sick leave. They were also advised to install physical barriers, encourage touchless payment options, use every-other check-out lane, stock shelves during off-peak or after hours, and use verbal announcements and signage to remind employees and customers to keep 6-feet apart (CDC, 2020a). This exploratory study aimed to describe the impact of COVID-19 on the work experience of hotel, food service, and food retail employees during the early stage of the pandemic. We also aimed to assess the workers’ perceptions of the effectiveness of the safety measures provided by their employers.
At the initial surge of the pandemic, we knew that service industries, particularly hospitality (i.e., hotel workers), food service, and food retail, were severely affected by the pandemic. We also knew that federal guidelines were beginning to be put in place as noted above. However, we lacked information on the workers’ perceptions of the impact of COVID-19 on their work experiences. We also lacked information about the workers’ perception on the safety measures in their workplace. This study aimed to address these gaps.
Methods
This was a mixed-method study with a congruent triangulation design. This study received exemption from the University of Michigan’s Institutional Review Board (HUM00180845). We sought to understand the experiences of individuals who worked in hotels, food service, and food retail, between May and June 2020 (once the CDC recommendations had been issued). We posted flyers describing the study with contact information on social media platforms (i.e., Facebook and Instagram). Nearly 70% of U.S. adults have used Facebook and about 40% have used Instagram in 2020, with a range of demographic groups represented (Pew Research Center, 2022). We also recruited via chain referrals, where participants were encouraged to tell their coworkers about the study. Once individuals indicated interests, they were provided the link to a Qualtrics web-based survey platform to determine their eligibility. Participants were eligible if they were 18 years or older; English-speaking; employed in the food retail, food service, or hospitality industries; and resided in pre-selected U.S. states based on their range of COVID-19 cases as of April 2020 (i.e., Arkansas, Florida, Iowa, Louisiana, Michigan, Nebraska, Nevada, New York, and Washington). These states were categorized into low, medium, and high using the following COVID-19 case count thresholds: low for states with less than 150 cases, medium for those between 150 and 300 cases, and high for states with greater than 300 cases per 100,000 residents.
Eligible individuals were offered the choice to complete a survey or complete phone interviews. Those who opted for surveys were directed to the consent page. Those who indicated interest in being interviewed were prompted to provide their phone number and preferred day and time of contact. For the phone interviews, verbal consent was obtained for both agreeing to participate in the study and to be audio-recorded. Research team members trained in qualitative interviewing techniques completed the interviews. Interviews lasted up to 20 minutes. Participants received a US$5 electronic gift card after completing the phone interviews. There was no incentive offered for completing the online survey.
Measures
All participants were asked about their age (in years), gender, relationship status (single, married, divorced, widowed), country of birth, industry type (hospitality, food service, food retail, other), current job title, duration in their current position (in years), full-time or part-time working status, number of hours currently working per week, hourly wage (before taxes), and to describe any work-provided benefits. Participants were asked to state whether changes to their work had been made because of COVID-19 (less or more hours worked, paid less or more, job title changed, work tasks changed). Both the interview guide and the online survey included the open-ended questions regarding measures the workplaces have enacted since the pandemic began and how employees are protecting themselves at work. These open-ended questions included, “What measures (if any) has your work organization put in place during the COVID-19 pandemic?” “Please tell us how it has been for you during the COVID-19 pandemic”; “What is your most urgent need right now?” and “Please tell us anything else you would like for us to know about your experience working during COVID-19.” Participants were also asked to describe how worried (not at all–extremely worried) they are about the following because of COVID-19: job security, physical health, mental health, personal finances, and paying bills. Additional items were included in the phone interview, including “How would you say your work differs right now during the pandemic compared with before?” and “What would you say is your most dire need right now (inside and outside of work)?”
Analysis
Descriptive statistics (e.g., frequencies) were used to determine the worker and work characteristics using SPSS v27. Those who participated in the phone interview and online survey were asked the same demographic questions. Data are reported for both sets of participants; however, quotes are pulled solely from the phone interviews. For the phone interview data, qualitative content analysis of the interview transcripts was performed, following the approach described by Graneheim and Lundman (2004). A research team member transcribed each interview verbatim omitting any identifiable information (e.g., participant’s name and specific names of location for place of work). Using this method, two coders (independently) read the de-identified transcripts and re-read to highlight key passages. Each coder imported these key passages into an analysis table, detailing the interpretive and meaning units. A third research team member reviewed any discrepancies to finalize the study’s themes and related quotes. Integration for this mixed-method approach began after analysis for joint interpretation. Divergence or convergence between the survey and interview data were explored.
Results
Worker Characteristics
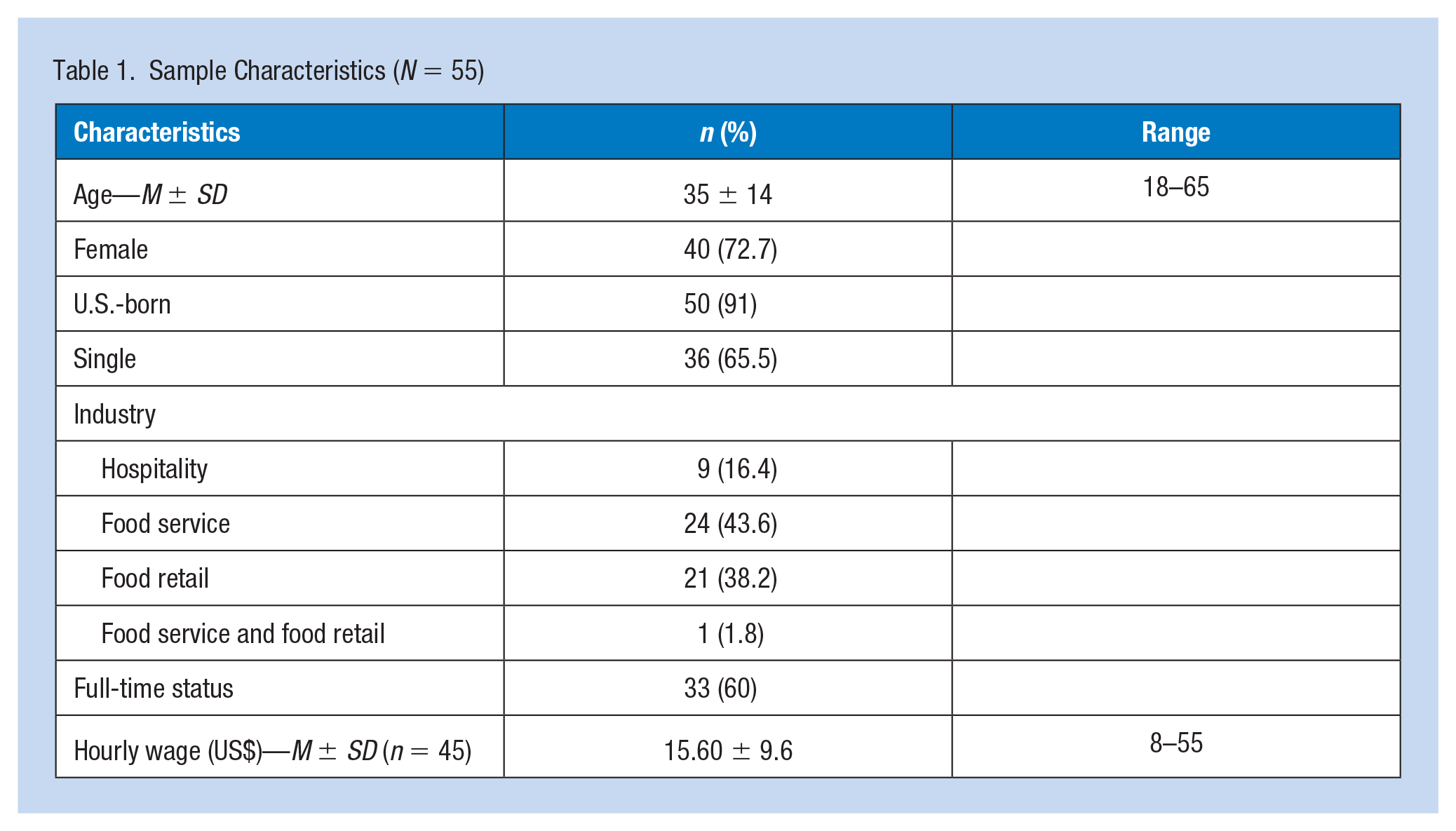
A total of 55 individuals participated in the study (phone interview n = 27, online survey n = 28) representing the following industries: hospitality (16%), food service (44%), food retail (38%), and one participant working in both Food Service and Food Retail in separate positions (1.8%). Sample characteristics are presented in Table 1. Two of the interviewees did not want to be audio-recorded so the research team member took detailed notes. The majority of participants were female (72.7%), U.S. born (91%), and currently single (66%). Participants ranged between 18 and 65 years old. Job titles included Cashier/clerk (31%), Food Server (21%), Manager (10%), Other (35%) with an average of 4.8 years working at their current job (range = 0–25 years). A majority were employed in full-time positions (60%) with an average hourly wage of US$15.6 (range = US$8–US$55). Majority of participants resided in Michigan (49%), followed by Florida (20%), New York (15%), Arkansas (5%), Nevada (4%), and a single participant from Iowa, Louisiana, Nebraska, and Washington. Accordingly, most of the participants (49%) resided in states with medium COVID-19 case counts (per 100,000 residents), followed by low (35%) and high (16%). When asked about their most dire needs, participants reported the need for things to go back to normal. We found no difference in participants’ accounts of their experiences across each of the regions.
Sample Characteristics (N = 55)
Worker Perception of the Impact of COVID-19 on Their Job Experiences
Participants’ experience during the onset of COVID-19 centered mainly on job insecurity and change in work hours and job tasks.
Job insecurity
Nearly half of the participants reported being somewhat to extremely worried about their job security due to the pandemic (27 out of 55). A high proportion of hospitality workers (6 out of 9) reported job insecurity, followed by food retail workers (14 out of 24) and food service workers (7 out of 21).
I received an email saying “due to social distancing” they’re asking me not to come in, and I was kind of in limbo for some odd number of weeks.
More than one third (36%) of participants reported looking for other employment as a contingent plan if they lost their job. Some participants reported their job as a service worker was their secondary form of employment in response to losing their primary job due to the pandemic. That said, many participants felt helpless as those who attempted to seek other employment experienced barriers, including lack of job openings/availability as well as concerns related to travel, housing, having to care for family members, and access to child care.
Hospitality is really suffering I would say. So, yes, it’s not that easy to find a job and if you find something it isn’t that easy to get it.
Workers also reported being concerned about loss of financial livelihood. About 16% reported getting paid less than before the pandemic began (9 out of 54), with the highest proportion occurring among hospitality workers (3 out 8), followed by food retail (5 out of 24), and only one in food service (out of 21). This subsequent decrease resulted in workers concerned with their ability to make ends meet such as paying bills.
I’m just stressed out because I’m not making what I am used to making.
Work hours and job tasks
Participants reported changes in work hours and job tasks. About 40% reported working less hours (22 out of 55), with majority of hospitality workers (6 out of 9), half of food retail workers (12 out 24), and a smaller proportion of food service workers (4 out of 21) reporting this change. About 55% reported a change in job tasks (30 out of 53), with the more than half of participants in both food retail (13 out of 21) and food service (13 out of 23), and just under half in hospitality (3 out of 8) reporting this change.
Uhm, except we’re shorthanded. So, we’re helping each other . . . It just depends, we’re moving everywhere. You just never know. You gotta go where you’re needed. The restaurant hours are cut back. Like we’re not open as many hours as we normally would so then my hours are cut back. Plenty of people’s hours at this store also reduced. My sister works at a restaurant so she’s been like- ah she’s still working but she lost her-her hours have been cut back so like-almost like maybe like 4 hours a week or something, it’s really low.
Workers’ Perception on the Workplace Safety Measures
Workplace safety measures put in place during onset of COVID-19
Participants’ reports of enacted workplace safety measures at the surge of the pandemic were broadly similar across the industries. The most common measures reported by 39 participants included face mask requirements for employees and customers (n = 23, 59%), social distancing (e.g., signs, floor markers, occupancy limits; n = 12, 30.8%), more frequent cleaning (n = 12, 30.8%), providing gloves (n = 12, 30.8%), and hand sanitizer (n = 7, 17.9%). In addition, putting up physical barriers between employees and customers (e.g., plexiglas at checkout stations; n = 5, 12.8%), and COVID-19 symptom screening (e.g., daily questionnaires, temperature checks; n = 5, 12.8%) were reported by participants working in food retail.
Participants reported confusion about mandates and pandemic severity, communications, and management support.
Confusion about mandates and pandemic severity
Participants reported inconsistencies in safety measures at the onset of the pandemic. They reported feeling relieved when the federal guidelines were finally put into place which made their work experiences more pleasant.
Before they weren’t provided any masks because they didn’t think it was necessary and they were thinking-like they didn’t-we didn’t need them but then the CDC said that they had to so now we’re allowed to wear masks. When it started, masks weren’t mandatory but then they became mandatory. So, uhm, I feel a bit better now.
Another participant, who was a restaurant server, expressed his increased sense of confidence to enforce workplace measures once the guidelines were put in place.
Our restaurant [has] really strict policy, like if people don’t have a face covering, they are not allowed to enter. And then you reinforce it and usually we don’t have any problem [with] customers.
Yet, some conflict arose from confusion over the mandates, along with difficulty adjusting to new procedures, and questions over the necessity of each change given the uncertainties surrounding this novel virus. For example, one participant doubted the severity of the pandemic.
I tend to think a lot of it’s blown out of proportion . . . I’m skeptical about this disease and if it’s legitimate.
In addition, another worker stated,
I’m not for making everyone wear a mask because I don’t really know how much they actually really protect, but I do think for the food service workers it’s relieving for the customers that the people who are handling your food are being careful.
Communications and management support
Participants, especially those in hospitality and food service, struggled to receive clear information from their employer on how they could maintain their work hours. They were unsure whether they would be able to return to work if they were furloughed and the timeline for them to return to work. For example, Participant 15 who worked in food service described,
Well, I contacted them and, uhm, they still are waiting for, uhm, you know, it seems like it’s gonna be up in the air. It might be a while.
Any amount of support from management was genuinely appreciated by workers in this sample. This was particularly pronounced as a handful of participants described the compassion and accommodation exhibited by their employer. Participants reported appreciating getting help from their managers in handling difficult situations with customers, as stated by Participant 18 who is a stocker for food retail:
Communication with management is open to where we have problems, complaints, or concerns, we addressed it-we address it to them and they know exactly what to do.
Worker-Specific Approaches to Protect Themselves
In addition to the established workplace measures, workers reported being proactive in ensuring their own safety.
We are now doing everything possible to stay safe. So everybody’s wearing gloves and masks and social distancing 6-feet apart, and constantly wiping down tables and chairs and booths and everything.
Some workers were given supplies such as hand sanitizer bottles and noted that they had to be vigilant because customers had been stealing them. Other workers, not initially given Personal Protective Equipment (PPE), bought their own masks and gloves to use in the workplace. One worker reported wearing an extra layer of clothing to be removed and placed into a plastic bag when she got back to her car after work. Others reported focusing on preventing cross-contamination by separating laundry worn outside the house, washing it immediately, and decontaminating themselves via showers before they get near other household members.
Outside of work I pretty much just stay to myself and I stay home. I take a lot of precautions cause I don’t want to bring it home to my family.
However, worker’s self-protective actions varied based on their self-assessment of vulnerability and perceived severity of the pandemic. Workers or their family members who were older or immunocompromised tended to have higher concerns and be more vigilant.
I tend to think a lot of it’s blown out of proportion. Here it hasn’t really made that big of an impression I don’t think.
Discussion
When the country went into lockdown in March 2020, majority of the workers in our study were classified as essential. For those who were not considered essential, job insecurity loomed heavily, with many seeking other employment with great difficulties. Interestingly, jobs in the retail food industry were also second employment for some participants due to a loss of their primary employment. Nonetheless, there was a great deal of financial uncertainty and worries with job insecurity. When the Coronavirus Aid, Relief, and Economic Security (CARES) Act, the largest economic recovery package in history, was passed and went into effect in late March, the unemployment rate had reached the historically highest rate of 14.8% (BLS, 2020). Although the CARES Act provided expansions in unemployment insurances to millions of Americans, it is unclear whether this was accessed by low-wage workers like those in the service industries. For example, Cortes and colleague (2020) noted that the CARES Act excluded many low-wage workers as 30% of individuals (majority of whom are low-wage) who lost their jobs were not eligible for benefits.
That many of the study participants reported change in work hours of job tasks was not surprising given that the pandemic resulted in changes in physical workplace environments, staffing reconfigurations, and work design (Alam, 2020; de Lucas Ancillo et al., 2021; Mediavilla et al., 2021). In addition to job insecurity and financial worries, workers’ primary concern was their safety and health, and that of their families. At the time of the study, some editorials were published about the increased risks essential workers faced for infection among themselves and family members (Yearby & Mohapatra, 2020). Although the Occupational Safety and Health Administration’s (OSHA) General Duty Clause of the OSHA Act (U.S. Department of Labor, OSHA, 1970) obligates employers to provide a safe working environment, the pandemic was unprecedented, and employers were ill-prepared to protect their workers.
There was a great degree of anxiety at the onset of the pandemic from inconsistencies with safety measures; however, the workers felt safer once the federal guideline was in place. It is important to note that the contradictory nature of those federal guidelines and mandates, at the onset of the pandemic, contributed the communication inconsistencies within workplaces (Agnew, 2020; Gostin et al., 2020). However, these guidelines provided a pathway for employers in their efforts to provide a safe workplace environment. For the most part, workers felt that their employers provided adequate safety measures and that they felt they were adequately protected at work. However, workers who did not perceive the pandemic as serious felt that the mask mandates were an over-response from their employers and the government. Recent publications have noted how risk perceptions of the pandemic could influence protective behaviors such as mask wearing (Hopfer et al., 2021; Koebele et al., 2021).
Workers in this study, many of whom were classified as essential workers, described taking precautions to keep themselves and their families safe. Most of these workers could not afford to stop working and several worried about the risk of contracting the virus (contact with the public) and their risk of severe health consequences (middle or older age and pre-existing health conditions). In his perspective piece, Larochelle (2020), argued that the best strategy clinicians can use to protect these workers is “a framework for counseling patients about the risks posed by continuing to work, urgent policy changes to ensure financial protections for people who are kept out of work, and a data-driven plan for safe reentry into the workforce.”
Finally, clear communication from and with the employers was critically important during the time of uncertainty and anxiety. Some workers did not get clear direction or updates from their employers. In general, workers were appreciative of clear communication and compassion from their employers, indicating that the management in the hospitality industry should build on compassion. The findings support Gaitens and colleagues’ (2021) work on the importance of management and organizational support not only for worker’s safety but also for their mental well-being and sense of trust.
Implications
At the individual level, having to provide their own PPE could be burdensome to the individual worker. Consideration for such a burden is warranted in future pandemic or infectious disease outbreak. At the organizational level, following CDC guidelines for best safe practices is ideal for employers. Transparent communication practices across organizational levels are warranted to foster workers’ trust. In addition, better streamlined processes are needed to promote job security, sense of being valued, and facilitate opportunities of professional growth among workers in these service industries.
Limitations
There may be concerns about the small sample size across each industry. In addition, participants represented a range of geographic locations that were experiencing the infection rates differently. Although we found no difference in participants’ accounts of their experiences across each of the regions, we did not explore community attitudes toward the virus nor toward the mandates. Another limitation is that we only included English-speaking workers. Therefore, we did not capture the experiences of other workers (e.g., Spanish speaking) who vastly occupy the jobs in these industries.
Strengths
Despite the limitations, given the unprecedented nature of COVID-19, this work provides a meaningful contribution to our understanding of the workers’ experiences at the pandemic’s onset. Future, more representative studies are needed to capture the nuanced differences across industries and worker characteristics as the pandemic continues.
Conclusion
The COVID-19 pandemic created opportunities for employers, occupational health providers, and policy makers to pay attention to worker groups that were previously ignored. Occupational health and safety concerns of service industry workers, notably those in hospitality, food service, and food retail, are often overlooked. The rapid evolution of safety measure recommendations and governmental regulations combined with variation in management’s implementation led to significant variation in workplace environments. Worker’s personal perspective on whether their workplace was meeting their own safety standards could be a motivation for taking additional action to protect themselves and others, in and out of the workplace, during the ongoing pandemic and in the future.
Applying Research to Occupational Health Practice
This research study can inform occupational health practice. Occupational health safety (OHS) professionals can collaborate with and guide employers to establish and reinform programs to support workers’ needs. OHS can also guide management training in communicative skills such as motivational interviewing to facilitate identification of workers in distress and better support of workers. Also, OHS can guide the establishment of clear organizational guidelines for reporting, without penalization, when workers feel unsafe, as well as streamlined returned to work process if a worker was infected and had to quarantine. Finally, given that the pandemic is still ongoing, OHS must continue to assess and evaluate workplace safety measures to ensure the safety and health of these workers. When employers do not provide on-site occupational health services, this responsibility shifts to the public health authorities who must be aware of and address the emerging health risks and needs (e.g., mental health needs, access to resources) of these workers.
Footnotes
Acknowledgements
The authors wish to thank the workers who shared their experiences. We would also like to thank Stephen Sullivan, MPH, for advising on Facebook recruitment strategies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval Number
HUM00180845
Ethical Committee’s Institutional Affiliation
University of Michigan Institutional Review Board.