
Abstract
Background:
Effective management of health emergencies is an important strategy to improve health worldwide. One way to manage health emergencies is to build and sustain national capacities. The Ebola epidemic of 2014 to 2015 resulted in greater infection prevention and control (IPC) capacity in Liberia, but few studies have investigated if and how that capacity was sustained. The purpose of this study was to examine the maintenance of IPC capacity in Liberia after Ebola.
Methods:
For this case study, data were collected via direct observation of nurse practice, semistructured interviews, and document collection. Data were collected in two counties in Liberia. Data were analyzed using directed content and general thematic analysis using codes generated from the safety capital theoretical framework, which describes an organization’s intangible occupational health resources.
Findings:
Thirty-seven nurses from 12 facilities participated. Ebola was a seminal event in the development of safety capital in Liberia, particularly regarding nurse knowledge of IPC and facilities’ investments in safety. The safety capital developed during Ebola is still being applied at the individual and organizational levels. Tangible resources, including personal protective equipment, however, have been depleted.
Conclusions/Application to Practice:
IPC capacity in Liberia had been sustained since Ebola but was threatened by under-investments in physical resources. Donor countries should prioritize sustained support, both financial and technical, in partnership with Liberian leaders. Occupational health nurses participating in disaster response should advocate for long-term investment by donor countries in personal protective equipment, access to water, and clinician training.
Keywords
Background
Better management of health emergencies is an important strategy to improving health globally (World Health Organization [WHO], 2018), including that of healthcare workers, as the current COVID-19 pandemic has shown. A major goal of the WHO’s Thirteenth General Program of Work is to build and sustain the national capacities that protect populations from health emergencies, such as epidemics, natural disasters, and conflicts, with the aim of protecting at least one billion people worldwide (WHO, 2018).
The Ebola epidemic of 2014 to 2015, which primarily affected Liberia, Guinea, and Sierra Leone, is an exemplar case of a health emergency that prompted global investments in national epidemic response capacity, particularly in infection prevention and control (IPC) (Cooper et al., 2016; WHO, 2015). IPC programming sought to protect healthcare workers who were highly vulnerable to Ebola transmission; early analyses indicated nursing workers were about 32 times more likely to be infected with Ebola than the general population (WHO, 2015). Programming included developing two-tier personal protective equipment (PPE) guidelines, rapidly training IPC specialists, writing workflows for identifying and triaging Ebola patients, and working with logisticians to ensure the appropriate distribution of PPE (Cooper et al., 2016).
The Ebola epidemic largely ended in 2015; approximately 4,800 Liberians had died (Centers for Disease Control and Prevention [CDC], 2020), including about 8% of the Liberian healthcare workforce (CDC, 2020). A few studies assessed IPC capacity in countries affected by Ebola shortly after the epidemic (Keïta et al., 2018; Tremblay et al., 2017); however, 5 years later, little research has been conducted on how, or whether, the IPC programming has been sustained. The purpose of this study was to examine the sustainability of IPC programs implemented during the Ebola epidemic in Liberia.
Methods
We conducted a case study pertaining to the sustainability of IPC and clinical practice among Liberian nurses and its impact on their occupational health. A case study design was selected due to its ability to address the political, cultural, and health systems contexts of the implementation of centralized plans for human resources for health (Egger et al., 2000).
Safety capital was chosen as the theoretical framework for this study for its potential to capture many facets of an organization’s occupational health capacity. The framework, developed by Nuñez and Villanueva (2011), adapted the concept of intellectual capital to occupational safety and health activities. Like intellectual capital, safety capital is both a process and a product. It is both a way of generating knowledge about occupational health and safety and the knowledge itself, which can be managed as an organizational asset (Nuñez & Villanueva, 2011).
Safety capital has three components: human, structural, and relational (Nuñez & Villanueva, 2011). Human safety capital is the knowledge and skills of employees, which can be used only while they are workers at the facility. Structural safety capital is the facility’s procedures, protocols, and routines. This knowledge belongs within the facility regardless of who is employed there. Relational safety capital is the knowledge embedded in and mobilized through relationships; these relationships can be either internal, and involve only people who work at the facility, or external, and involve actors outside the facility. Both types of relationships are germane to occupational health (Nuñez & Villanueva, 2011). This study’s results are presented by component; within each component, they are organized by IPC activity.
Data Collection
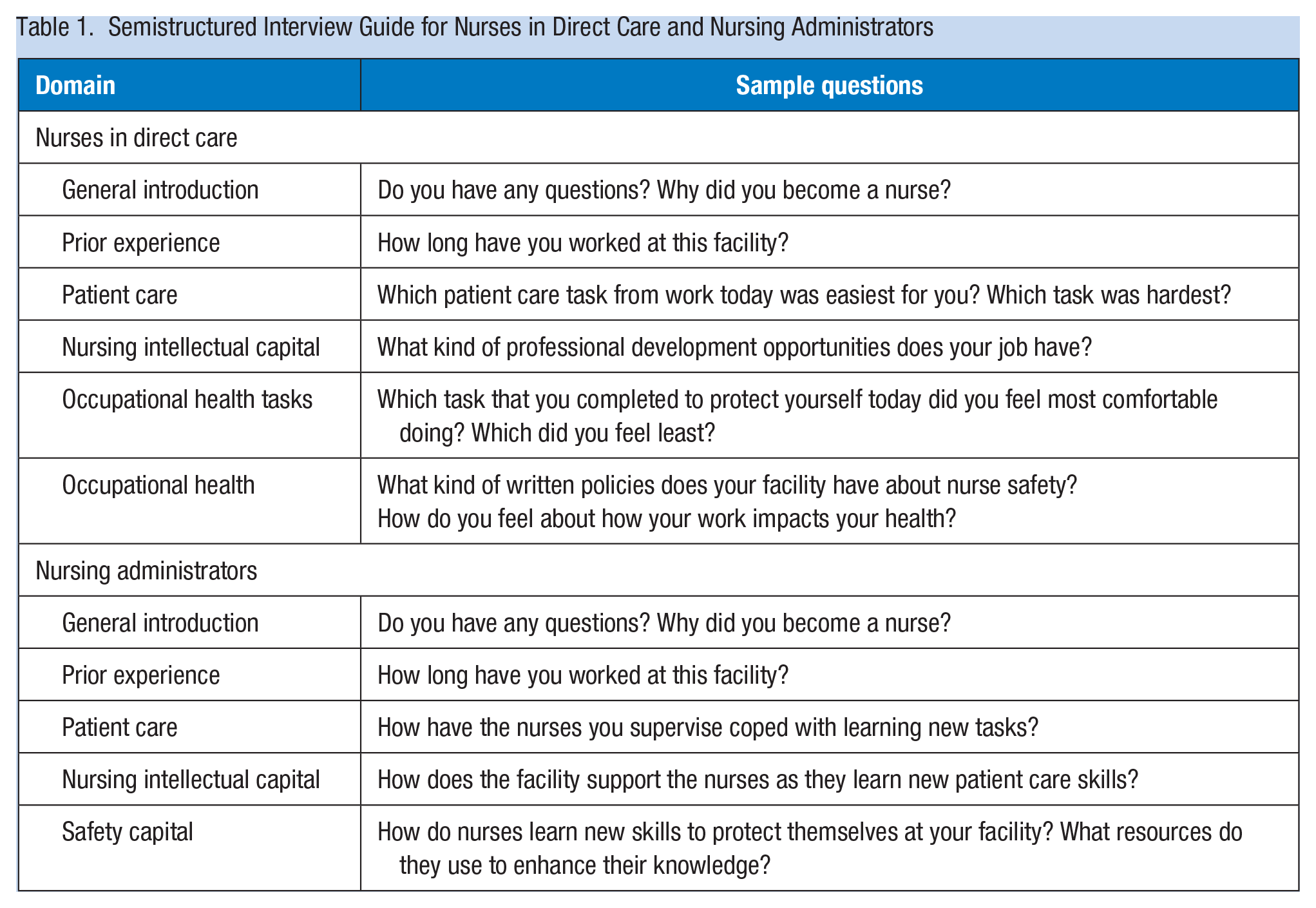
Data were collected from practicing nurses in two counties in Liberia, including Montserrado and Nimba, from February through June 2019. These counties were selected for their size; about one third of Liberians live in one or the other (Liberia Institute of Statistics and Geo-information Services et al., 2014). Data collection methods for all aims included: (a) direct observation of nurse practice in the clinical setting, (b) semistructured interviews following direct observation, as well as review of documents at the clinical site pertinent to nurse practice. Direct observation took place over a shift, or portion of a shift. See Table 1 for the semistructured interview guide. Documents that were relevant to nurse practice were photographed with the participants’ permission during direct observation at the clinical facility. Some of these pertained to clinical practice (e.g., disease management protocols), others to occupational health (e.g., IPC procedures). All data collection was conducted by one researcher, also a nurse, who had extensive experience working with nurses in Liberia. Data collection ended when the researcher’s reflexive journaling, conducted throughout data collection, indicated saturation had been reached.
Semistructured Interview Guide for Nurses in Direct Care and Nursing Administrators
Recorded interviews were transcribed verbatim by either an experienced freelance transcriber in Liberia or a transcription agency in the United States. LJR checked transcripts for accuracy by selecting interviews at random and comparing the audio file to the transcript.
Study Population
Nurses working in either direct nursing care or as nursing administrators were included in the study as long as they had been employed at their current facility for 6 months or more. Purposive and snowball sampling were used to obtain a representative target sample of 30 to 50 nurses working in a variety of facility types in two counties, including public, private for-profit, and private faith-based facilities at each level of the Liberian health care system (primary, secondary, tertiary). Nursing administrators were approached in person about participating and for their written permission to collect data at their facility. Once that permission was obtained, nurses at the facility were notified about the study opportunity in the manner suggested by the nursing administrator; this was usually a brief presentation given by the researcher at the nurses’ station. Nurses previously known to the researcher were excluded. Informed consent was obtained prior to beginning direct observation; participants had the opportunity to decline to sign the informed consent form and give verbal consent only if they chose. The University of Liberia’s Institutional Review Board approved this study, protocol #17-10-071, and New York University’s Institutional Review Board’s University Committee on Activities Involving Human Subjects approved this study, protocol #FY2018-1723, in the United States.
Data Analysis
Interview transcripts, field notes, and photographs of documents were analyzed beginning with directed content analysis using codes generated by the study team prior to data collection from the safety capital framework. Coding continued with general thematic analysis as described by Hsieh and Shannon (2005). Coding was conducted on Atlas.ti version 8.3.1 by the study researcher. Early in the coding process, a second researcher, APS, reviewed coded data for coding accuracy. After coding was completed, reports were generated by code to assess for convergence of evidence across data types to ensure rigor (Yin, 2018).
Results
Thirty-seven nurses participated in the study. Thirty-three were both interviewed and directly observed. Three were interviewed only because it was not feasible to directly observe their practice (i.e., they were off-duty or did not have any cases on the day they were available), and one who had been directly observed ended participation in the study prior to being interviewed for personal reasons.
Participant characteristics are presented in Table 2. Twenty-one participants were from Montserrado county and 16 were from Nimba county. Participants practiced in public facilities, private faith-based facilities, and private for-profit facilities. Four were Directors of Nursing at tertiary care facilities. Three participants in this sample had worked in Ebola Treatment Units during the Ebola crisis.
Participant Employment Settings and Experience (n = 37)
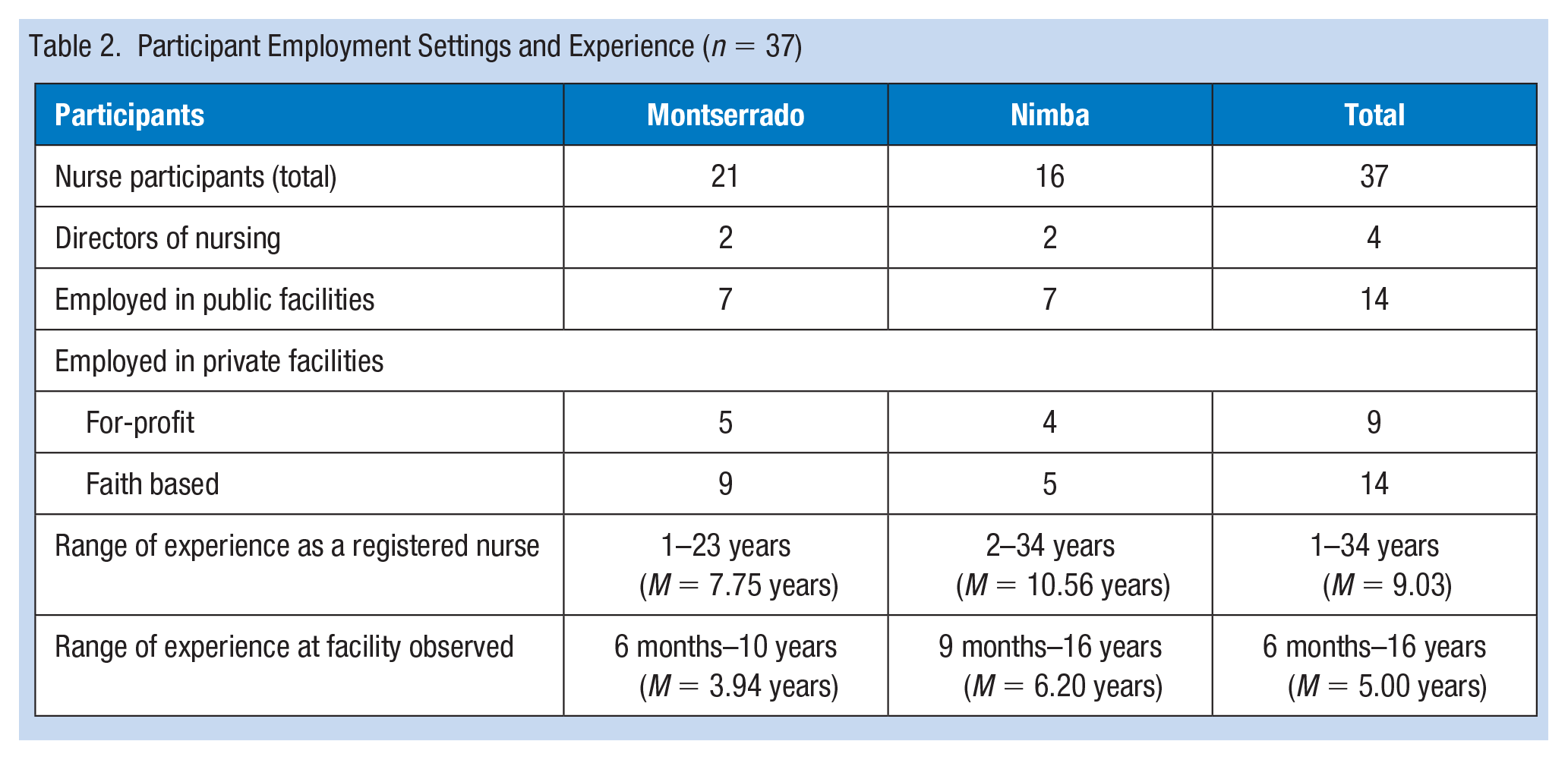
Twelve facilities were included in the study, seven in Montserrado and five in Nimba. Five were public facilities run by the Government of Liberia: two of these were in Montserrado, three were in Nimba. Four were private facilities operated by a faith-based organization: three of these were in Montserrado and one in Nimba. The remaining three were private, for-profit facilities, two of which were in Montserrado, and one in Nimba. Five of the 12 facilities provided mainly ambulatory care, but also staffed midwives who managed deliveries, and had a few beds available for patients to stay overnight if indicated (e.g., for complicated malaria). One facility provided mainly primary care and managed deliveries only. Six facilities provided extensive (>15 beds) inpatient care in addition to ambulatory care.
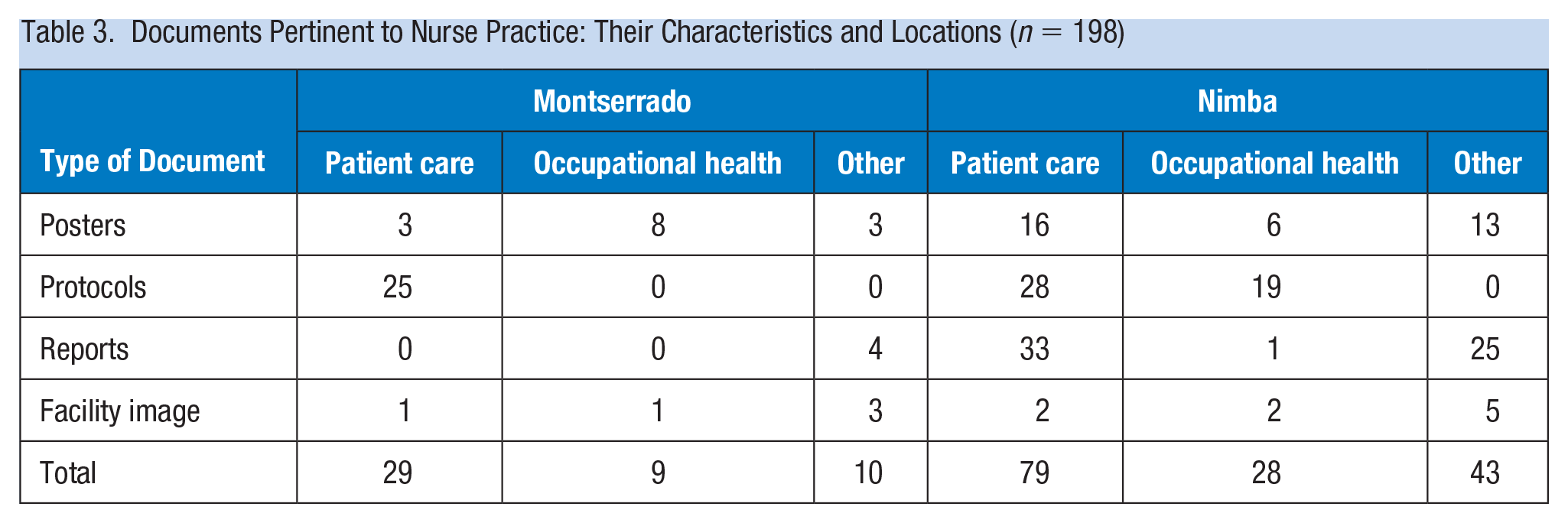
See Table 3 for a list of documents that were reviewed and their characteristics. Documents pertinent to IPC programming were counted under occupational health. Facilities in Nimba county had more protocols and reports related to occupational health than Montserrado county; this was driven by two tertiary care facilities (one public, faith-based private) that had extensive IPC progamming.
Documents Pertinent to Nurse Practice: Their Characteristics and Locations (n = 198)
Human Safety Capital
Nuñez and Villanueva (2011) define human safety capital as the occupational health-oriented knowledge and skills of employees the firm can use during their employment. Participants repeatedly identified Ebola as a seminal event in the development of human safety capital in Liberia. Human safety capital development was accomplished primarily via in-person trainings and included the IPC topics of hand hygiene and injection safety. New IPC roles also emerged as a result of investments made during Ebola.
Further Training
The training of licensed nurses that occurred as a direct result of the Ebola epidemic (usually referred to as the “Ebola crisis” by Liberians) reached almost every participant. A participant who practiced at a private faith-based facility in Montserrado described the training: “During the Ebola, let’s say just after the Ebola, we had trainings about handwashing, handling of . . . infectious material, and disposal.” Participants reported trainings during Ebola were on a variety of IPC topics: handwashing, handling sharps, PPE, and the use and disposal of infectious materials. One participant denied learning about the use of PPE during her prelicensure training, although she reported learning about handwashing. A fourth participant said she received some IPC training in school, but “it was not in detail like the training [during Ebola].”
The trainings were offered throughout Liberia; one participant reported attending one in the relatively rural county of Grand Cape Mount. Some of these trainings were offered by the Government of Liberia, others were offered by international nongovernmental organizations or by the WHO. As a result of Ebola, there appeared to be a high level of safety awareness, most of it around IPC issues. One participant’s comment was representative: “To help other people you have to help yourself.” Similarly, another participant recited the slogan, also the title of a major IPC program during Ebola, “Keep safe, keep serving.”
All but three facilities reported ongoing IPC training at the time of data collection. Of the three that did not offer ongoing training, two were public, primary-care facilities, and one was a private for-profit facility that offered both inpatient and outpatient care. Trainings were typically ad hoc and took place as part of standing monthly or bimonthly meetings not earmarked for IPC purposes; thus, IPC trainings took place even less frequently. One Director of Nursing at a public tertiary care facility said that after the Ebola crisis the Government of Liberia began to hold refresher courses on occupational health topics “once in a while.” Participants from two facilities reported IPC coaching took place in the clinical care settings, such as at the bedside on an inpatient ward; both of these facilities were private. IPC trainings were the only occupational health trainings mentioned by participants; trainings pertaining to other occupational health issues faced by nurses, such as musculoskeletal injury or mental health issues, were not offered.
Awareness and Enforcement of Hand Hygiene
Across facilities, awareness of proper hand hygiene was high. Direct observation indicated participants consistently washed their hands after direct patient contact, although there were exceptions such as a participant touching intact skin on the face of one patient and then not washing their hands prior to the next patient. Participants at two different facilities reported conducting regular audits on hand hygiene compliance. Both of these facilities were private, faith-based tertiary-care facilities.
Several participants reported purchasing the hand hygiene supplies they were using at work (i.e, hand sanitizer and cloth towels in particular). This could be costly; “Even to get hand sanitizer, they are very expensive now. During the Ebola crisis, it was free, but now they are very expensive.” The salary for nurses working in the public sector was $269 United States Dollar (USD) per month at the time of data collection; a small bottle of hand sanitizer was about $2 USD. Nurses working full-time would need to purchase more than one small bottle monthly, so this is a significant expense.
Needlestick Safety
Knowledge of sharps safety was generally high and demonstrated in practice. Participants were observed either disposing of needles without recapping or recapping using the scoop technique. Three nurses were observed recapping a clean needle that had been used to draw up medication. Only one was observed recapping a used needle. Sharps were typically disposed of promptly, often in a small cardboard container called a “safety box,” designed for sharps disposal and seen in most facilities. One participant, who worked at a private facility, reported: “the training told us that sharps shouldn’t be moved from one unit to another . . .”
Knowledge around the management of needlestick injuries (NSIs) had clear gaps. Only three participants had ever experienced an NSI, and one reported a history of splash exposure. Two of the nurses with a history of NSI reported taking postexposure prophylaxis; the third did not because the source patient’s follow-up tests were all negative. Many participants, when asked about NSI management, forgot the first step of washing the site, seemed confused about the fact that there are different types of postexposure prophylaxis for different bloodborne illnesses, and often did not remember treatment for NSIs should be obtained as soon as possible after the injury. One participant, who correctly identified washing the wound as the first step for managing an NSI, then stated: “After that, maybe after one week, I would do all my tests.” Another participant reported that her facility would tell staff with NSIs “to wait” for their labs “within six weeks or a few weeks.”
The IPC Officer at a private, faith-based primary-care facility, said postexposure testing and prophylaxis at her facility included HIV, HBV, and HAV, though HAV is not a bloodborne illness. Similarly, another participant stated that if she tested positive for HCV after an NSI, she would “take the vaccine.” A third reported the first step after an NSI was a tetanus injection along with antibiotics, and his facility “always” tests the source patient for diseases including HIV, HBV, typhoid, and malaria, some of which are not transmissible via NSI.
Participants could identify limited resources available for postexposure prophylaxis; for example, participants at two large facilities with numerous inpatient wards reported the facility had postexposure prophylaxis for HIV available, but not for HBV. Two smaller primary-care facilities, one private and one public, were both unable to treat HIV exposure.
New Roles: IPC Officers and Focal People
An important component of human safety capital in Liberia was the training for the IPC Officers. Two of the 12 facilities in this study did not report having a focused IPC Officer or Focal Person. One of these was a government primary-care clinic, another was a primary for-profit clinic. Both clinics were in Montserrado. Three facilities had IPC Teams. Like so many aspects of human safety capital in Liberia, the role of IPC Officer was developed during Ebola. One participant, a member of the IPC Team, stated: “We had a training after Ebola, and from there, we became focus people for IPC.” One participant reported she was selected to be the IPC Officer because of the time she spent working at an Ebola Treatment Unit and stated her IPC training had taken place “only during the Ebola.” A participant who was an IPC Officer in addition to the supervisor of a pediatric ward had been flown to China by the Liberian government, along with two other Liberian nurses, for a 3-week training in IPC. By contrast, another participant became the IPC Officer at her clinic on the basis of a 5-day training that was conducted at a stadium in Montserrado.
Structural Safety Capital
Structural safety capital is defined by Nuñez and Villanueva (2011) as the knowledge, procedures, and practices that buttress employee health at an organization and remain at the organization regardless of who works there. Structural safety capital in Liberia was comprised of the position of IPC Officer, the reinforcement of hand hygiene procedures, policies to support injection safety, and safety routines followed by the nursing staff.
IPC Officer
While the knowledge and skills IPC Officers bring to the role is human safety capital, the existence of the position itself is a form of structural safety capital. Seven of the participants were either IPC Officers themselves or on the IPC team. They characterized their IPC responsibilities similarly: preventing infection transmission between and among staff and patients by ensuring the facility was clean, enforcing proper hand hygiene practices, managing the incinerator at facilities with small numbers of inpatients, managing PPE, meeting with ward supervisors to assess what supplies or training are needed, and offering trainings. In several facilities, these responsibilities included setting up and taking down the facility’s handwashing stations daily. There was one exception, at a private, faith-based, tertiary-care facility where there was one participant, a member of the IPC Team, who also had significant monitoring and evaluation responsibilities as a part of their role on the team. Furthermore, this participant had one unusual clinical responsibility: assessing patients who presented to the facility showing signs or symptoms of diseases of epidemic potential, as defined by the Government of Liberia. Since every other nurse who worked as an IPC Officer or Team member either provided full-time direct care or was a DON, this participant role was an exception.
Reinforcing Hand Hygiene
Hand hygiene procedures were reinforced by both the IPC Officer and simple displayed reminders. One IPC Team member said, “Hand hygiene is one of the tools we encourage, because . . . this is the minimal, minimal one we can afford.” The most common visual reminder was a simple white and orange hand hygiene poster, “The Five Points of Handwashing” (Figure 1), developed by the WHO, and displayed at four of the 12 facilities. A different hand hygiene reminder was posted at a nurses’ station at a public tertiary care facility. Visual reminders on other IPC topics included: a poster on the correct use of PPE, developed by an international nongovernmental organization, at one facility, and a sign clarifying which bin contained infectious waste, at another. One participant also mentioned a hand hygiene audit form, developed by a nongovernmental organization, that her facility used to conduct hand hygiene audits.
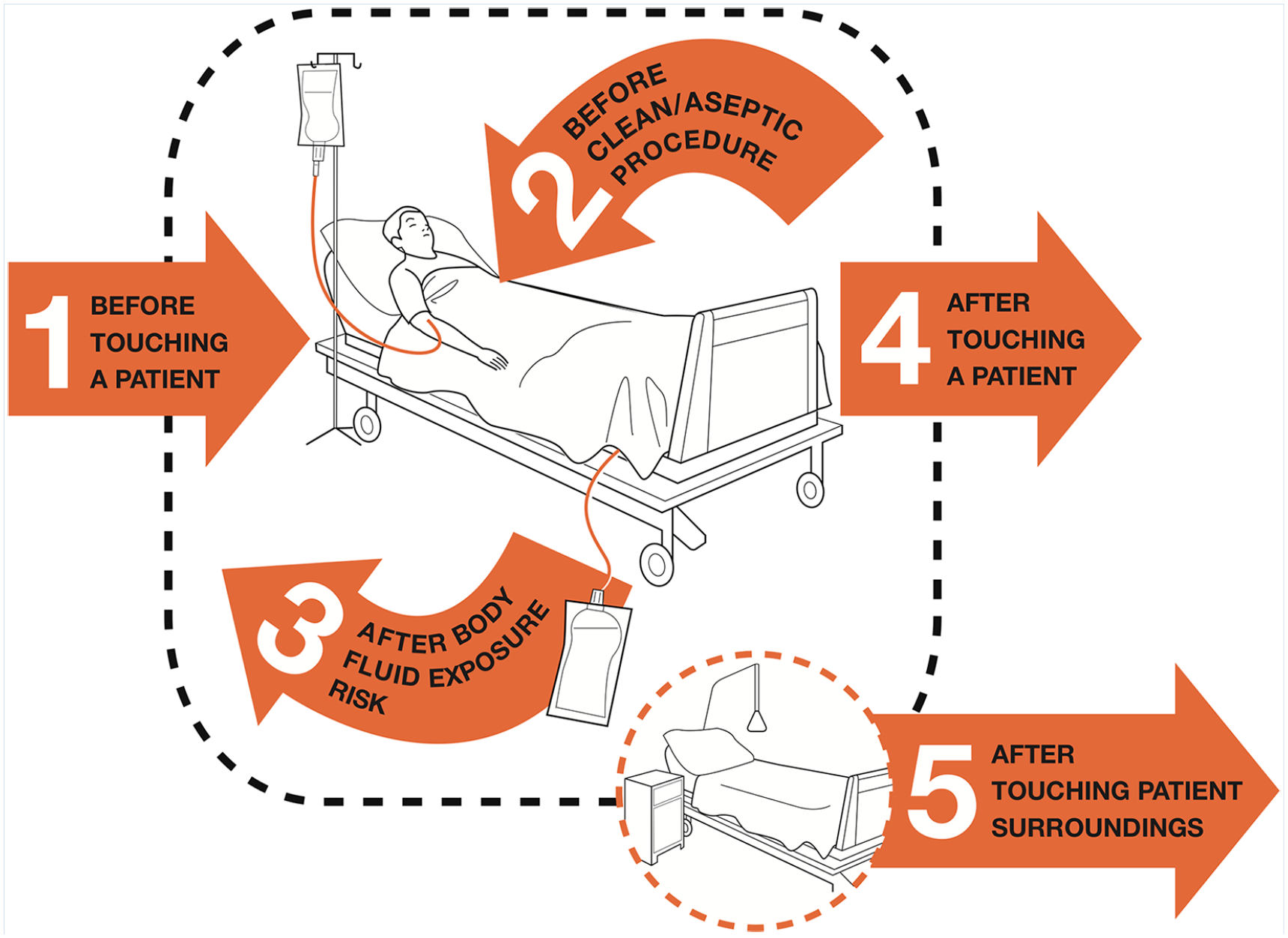
Portion of WHO figure displayed in four facilities.
Injection Safety
Structural capital supporting injection safety was also apparent. Four facilities, all private, had “injection rooms” where injectable medications were administered. “Injection rooms” likely protect nursing staff from NSIs as they allow a single nurse to administer injections away from the distractions of a busy clinic or ward, and to develop expertise in injectable medication administration. Three of these facilities were primarily outpatient, the fourth offered both inpatient and outpatient care.
Facilities’ protocols for NSIs were typically unwritten; however, two facilities had ledgers for recording staff injuries. Participants at two facilities stated time off could be obtained after an NSI (as one participant put it: “you go home and rest”). Another participant reported her facility treated NSIs for free.
Safety Routines
Routines were an important part of IPC programming. In two cases, they were unwritten. One routine described by two participants at the same facility was seen by both as fundamentally protective of healthcare workers: all facility workers take their vitals every morning upon arrival, “to know whether you are well,” and wash their hands before entering the facility. Staffers then go to the clean utility area and get the PPE they need for the day. Another safety routine was observed at a private tertiary-care facility, where a senior nurse, the same nurse who offered the IPC trainings, goes from unit to unit every morning to remind people to use PPE.
One public facility, by contrast, followed written routines from an IPC instruction manual developed by an agency of the U.S. government in partnership with a nongovernmental organization: “Must Do Actions for Daily Opening and Closing of the Health Facility.” The list includes such items as set up handwashing stations, wear appropriate PPE, and set up trash cans.
Relational Safety Capital
Nuñez and Villanueva (2011) argue that relational safety capital is occupational health knowledge embedded within, available through, and used by interpersonal interactions. It can be further divided into two types of relationships: internal and external. In this study, participants generally did not identify relationships as important to IPC programming. Two participants mentioned supervisors as potential resources (per one: “the senior nurse will tell you what to do”), but generally, this topic did not resonate with participants when interviewed. Direct observation affirmed this finding; no nurses were observed seeking assistance with IPC procedures, by contrast, several participants were observed seeking assistance when faced with a clinical care challenge.
One facility demonstrated the potential role of relational safety capital. This private faith-based facility, with extensive inpatient and outpatient care, had a long-standing partnership with a German nongovernmental organization to build the facility’s “Esther Team.” The Esther Team was a group of facility staff members, and included two study participants. This team worked with the German nongovernmental organization via digital platforms to implement projects intended to improve facility performance at “IPC, patient safety, and surgical site infection.” Webinars related to IPC took place every Friday afternoon, and members of the Esther Team were responsible for viewing and disseminating their contents.
The partnership’s flagship project was a study in hand hygiene, which evaluated clinical staff members’ hand hygiene habits. The study indicated precare hand hygiene adherence was much lower than postcare. The Esther Team worked to increase the frequency of precare handwashing using immediate, on-the-spot coaching. This mentoring was seen by the Esther Team as a permanent responsibility to the workers; per one participant, “it will never end.” The Esther Team also worked on a project addressing antimicrobial resistance; this was the only example of antimicrobial resistance programming observed.
The Esther Team was a product of both the internal and external social capital, as the facility’s relationship with the German nongovernmental organization was key to the team’s existence, and the team itself built relationships inside the hospital.
Physical Resources for IPC
Nuñez and Villanueva (2011) include tangible occupational health resources in their model of safety capital, acknowledging their role in preventing occupational illnesses and injuries, though they are not a part of safety capital per se. Since the importance of physical resources in IPC programming is widely recognized, and since the IPC programming developed during Ebola included the distribution of PPE, assessing tangible resources is an important part of understanding how programming is being sustained. In this study, physical resources important to sustaining IPC programming included water, for hand hygiene, and PPE.
Water
Handwashing stations were set up at every facility. They were typically comprised of a plastic barrel with a spigot (used to control the flow of water from the barrel), filled with water, placed on a stool, with a soap dish and soap positioned on top, and a plastic bucket on the ground to catch water from the spigot. Only three of these stations had towels, one of which the participant reported bringing in from home, so most often participants had to let their hands air dry. For five facilities, these stations compensated for a lack of piped water. Three facilities had running water in the exam rooms; participants were able to wash their hands in their exam rooms as they saw outpatients. The remaining four facilities had piped water, but it was either very unreliable (at two facilities) or available only in portions of the facility (at two facilities).
PPE
There was a marked contrast between the availability of PPE at public and private facilities. One public facility in Montserrado had some PPE available, but in most public facilities, there was virtually none. Gloves were unavailable at three public facilities, two in Nimba and one in Montserrado. One participant stated simply, “We don’t have PPE.” By contrast, private facilities in both Montserrado and Nimba were fairly well equipped, with one exception, a small private clinic in Montserrado, where one participant said of PPE: “We don’t really have it here.” The other private facilities in both Montserrado and Nimba were observed to have sufficient PPE, with one participant saying: “Anytime we need it we call, they bring it in.”
Much of the PPE in use in Liberia dates to the epidemic. Participants at two different facilities pointed out some of their current PPE supply had been delivered during the Ebola epidemic, and noted their concern that supplies were dwindling. As one said: “But as you can imagine, since 2014, it’s wearing away. We don’t have enough now.”
Discussion
The results of this case study indicate much of the IPC programming introduced in Liberia during Ebola has been sustained for the past 5 years, primarily via human and structural safety capital. Nevertheless, there are some worrying gaps.
The human safety capital generated during Ebola is still highly active; the vast majority of facilities in this study had an active IPC specialist who received their initial training during Ebola, indicating this was one of the more sustainable investments made during the crisis. Furthermore, the presence of an IPC focal person, officer, or team reinforced behaviors that protected the occupational health of nurses. Other research found facilities with IPC-trained personnel were more likely to score above the median on IPC assessments (Keïta et al., 2018). Furthermore, as Keïta et al. (2018) discussed, IPC-trained personnel were very likely to offer IPC-oriented trainings.
However, this study identified opportunities for growth in human safety capital. The main gap in IPC knowledge was little awareness around proper management of an NSI. This was likely due to a variety of factors: other IPC programming was seen as more relevant during Ebola, low reported rates of NSI, and highly limited availability of postexposure prophylaxis for major bloodborne illnesses such as HIV, HBV, and HCV. Nevertheless, this gap was worrying because the estimated prevalence of HBV in Liberia was 17.55% (Schweitzer et al., 2015).
Structural safety capital in Liberia takes the form of the IPC Focal Person role, brief written reminders (often posters), and protective routines, some of which are unwritten. It seemed that, especially with regards to NSIs, documenting the correct protocol would provide a buttress against limited worker knowledge. Furthermore, the extent to which unwritten routines would be sustained in the event of staff turnover was unclear.
Relational safety capital was found to be highly limited. In light of the strong IPC programming being done by the Esther Team, this seems like a missed opportunity. The Esther Team’s facility was the only participating facility that had IPC programming around antimicrobial resistance, yet antimicrobial resistance was a major issue in West Africa (Bernabé et al., 2017). It would be beneficial for institutions that have experience in broader IPC programming, including antimicrobial resistance and NSI management, from both within and outside of Liberia to form relationships with facilities like these and assist with these aspects of IPC programming.
This study also illustrated certain tangible resources, important to IPC programming, were unevenly distributed and managed throughout the healthcare system. PPE was more likely to be available in private facilities than public ones, though private facilities were concerned about dwindling supplies. This finding differs from Tremblay et al.’s (2017) study, which found that public facilities were better equipped than private in 2015. The change is likely due to funding difficulties in a country with many pressing needs. This situation lends an opportunity for donor countries to address the gap.
Access to running water, essential for hand hygiene, was also a challenge. This is of particular concern at this time of the global COVID-19 pandemic, which has affected Liberia, and which Liberia must primarily battle through prevention, since many of the interventions available to fight COVID-19 in high-income countries (oxygenation, ventilation) are effectively unavailable. The absence of these important components of IPC programming constituted a significant drain on healthcare workers’ resources, as they worked to overcome these limitations by, for example, spending time setting up hand hygiene stations, or purchasing their own hand sanitizer. Given nurses’ limited salaries in the country, transferring the costs of IPC to the worker is not a sustainable strategy.
Finally, the importance of tangible resources to IPC programming highlighted the limitations of the theoretical framework of safety capital when applied to a low-income country. The advances made in occupational health thanks to water access and PPE throughout many high-income countries cannot be taken for granted everywhere.
Limitations
The main limitation of this study was that it was only conducted in two counties in Liberia, both of which were highly accessible compared to other counties; therefore, the results may not be representative of Liberia as a whole. Furthermore, this case study only examined IPC-related national capacities; however, clinical trainings on the management of Ebola in individual patients were also conducted during the Ebola crisis. It was not clear if those capacities had been sustained in the same way. Finally, all data were collected by an American nurse, who, despite her assurances that she was present only to learn, was often treated as an authority figure, with some participants even asking her to tell them what they had done wrong during their shift. This perception likely influenced their behavior during direct observation and answers during interviews.
Implications for Occupational Health Nursing Practice
This study demonstrated the importance of occupational health expertise to healthcare workers, and highlighted the importance of continuing to develop that expertise, particularly in low- and middle-income countries. The results also demonstrated the resource constraints faced by nurses working in occupational health roles in low-income countries; for example, these nurses must keep careful track of resources such that, if and when they treat a healthcare worker who has an NSI, they are able to refer that patient to a facility that can offer them the most comprehensive postexposure services possible. If possible, these nurses should also advocate for HBV vaccination among healthcare workers at their facility.
Occupational health nurses globally who have the time and expertise should consider building relationships with facilities in low-income countries, perhaps via the International Labor Organization’s International Occupational Safety and Health Knowledge Network, to assist with the development of structural safety capital (i.e., policies and procedures) that the facility identifies as useful, such as NSI protocols. Since IPC programming was the primary form of occupational health programming available at these facilities, working with facility administrators to develop programming around mental health challenges, musculoskeletal injuries, and other occupational health needs common to healthcare workers would also potentially be useful. Expertise from nurses who are from other low- and middle-income countries is likely to be particularly useful.
Conclusion
These results indicate the safety capital that is developed during health emergencies, particularly as related to IPC, is likely to be sustained years later, especially in the form of individuals’ knowledge and skills. However, knowledge gaps around areas less pertinent to the emergency can go unaddressed, and sustained relationships oriented toward continuing to build safety capital, such as seen with the Esther Team, are rare. Furthermore, the continued provision of needed resources is often neglected after the emergency is over, to the detriment of the nation’s ability to sustain its new capacities. Donor countries should commit to sustained relationships and provision of physical resources.
Applying Research to Occupational Health Practice
After an emergency, growth in human and structural safety capital pertinent to IPC will likely be sustained, especially if long-term institutional relationships are developed. These relationships can contribute to later capacity building in other areas of IPC. By contrast, investments in physical resources like PPE are unlikely to be sustained. This lack of physical resources may restrict clinicians’ ability to implement IPC knowledge and procedures. Clinicians concerned with occupational health must advocate for emergency response organizations to sustain progress by partnering with local facilities and continuing investments in physical resources as part of disaster response.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Robyn d’Avignon for her contributions to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by grant number, T42OH008422, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services. It was also funded in part by Postdoctoral Fellowship Training Grant (T32 NR016914. Program Director: Titler) Complexity: Innovations in Promoting Health and Safety. This study was also funded by the 2018 AAOHN Medique Research Grant.
Author Biographies
Laura Jean Ridge is postdoctoral fellow at the University of Michigan’s School of Nursing’s T32 in Complexity: Innovations in Promoting Health and Safety (CIPHS) funded by the National Institute of Nursing Research. She completed her doctorate at NYU’s Rory Meyers College of Nursing as a T-42 trainee in occupational and environmental health nursing.
Amy Witkoski Stimpfel is an assistant professor at NYU Rory Meyers College of Nursing and the Deputy Director of the NIOSH-funded T-42 doctoral training program in occupational and environmental health nursing. Her research explores how to optimize nurses’ work environment to improve nurse well-being, such as burnout, and clinical outcomes, like patient safety. Her scholarship draws from theories and methods used in health services research, occupational health and safety, sleep/chronobiology, and nursing.
Robin Toft Klar DNSc, RN, FAAN is a clinical associate professor at NYU Meyers College of Nursing; her clinical, teaching, and research career has focused on health promotion from a community perspective. Her work examining the environment has evolved over the years going beyond air, water, and soil to include the built environment. Current clinical and research work focuses on the social and physical environmental impact on health workforce capacity building in low and middle income countries (LMICs).
Victoria Vaughan Dickson, PhD, RN, FAHA, FHFSA, FAAN is the program director of the NIOSH-funded doctoral training program in occupational and environmental health nursing and an associate professor in the Rory Meyers College of Nursing. She is recognized as an international expert in qualitative research techniques and mixed methods research and has conducted training to interdisciplinary teams locally, nationally, and internationally. She has extensive clinical and research experience in cardiovascular and occupational health nursing, her research program focuses on investigating the bio-behavioral influences on self-care in patients with cardiovascular disease.
Allison Patricia Squires, PhD, RN, FAAN, is an associate professor and director of the Florence S. Downs PhD Program in Nursing Research & Theory Development at NYU Rory Meyers College of Nursing. She was the 2019 -2020 Distinguished Nurse Scholar in Residence for the National Academy of Medicine where she worked on the consensus study for the next Future of Nursing 2020 -2030 report. An internationally recognized health services researcher, Prof. Squires has led or participated in studies covering 38 countries, with current active projects Mexico, Ghana, and the European Union.