
Abstract
Background:
Occupational health professionals (OHPs) are in a unique position to impact the health and well-being of employees at work and outside of work. One way of achieving this holistic health goal is to integrate the concept of Total Worker Health® (TWH) into the organization’s culture. It is critical for OHPs to develop the ability to incorporate TWH into their practices, yet there are gaps in our understanding of OHP’s attitudes toward change and toward TWH, their level of TWH knowledge, and the number of OHPs who have adopted TWH.
Methods:
An electronic survey was administered to a national sample of 4,777. This cross-sectional study used Qualtrics to record survey responses measuring knowledge of TWH, attitude toward change, resistance to change, transformational leadership ability, perception of organizational readiness, and leadership commitment.
Findings:
The total sample size was 253 (5.3%). Most respondents were bachelors prepared nurses (75.1%) with greater than 10 years’ experience (71.5%) and employed in manufacturing (42.6%). Approximately 74% (n = 125) of respondents knew about TWH, but did not have a program in place or were unsure of the existence of one. A high percentage (74.0%) were open to implementing TWH, had favorable attitudes toward change (M = 3.9 on a 5-point Likert-type scale), but needed education on how to move forward (56.0%).
Conclusions/Application to Practice:
Findings suggest that most OHPs know about TWH, but generally have not adopted the TWH concept at their worksites. However, they are open to implementing TWH programs and have favorable attitudes toward change.
Background
Total Worker Health® (TWH) is a holistic approach to improving worker well-being developed by the National Institute for Occupational Safety and Health (NIOSH) (Centers for Disease Control and Prevention [CDC], 2018e). The concept of TWH integrates workplace safety and health, with health promotion to reduce injury, illness, and advance overall well-being. NIOSH’s mission is to produce and transfer knowledge to promote occupational safety and well-being for workers. One way that NIOSH is achieving its mission is by collaborating with professional organizations to extend research opportunities regarding TWH and to disseminate efforts to put TWH into practice. NIOSH has established an affiliate program whose main goal is to “increase the visibility, uptake and impact of total worker health to advance the safety, health, and well-being of workers” (NIOSH, 2014, p. 4). The American Association of Occupational Health Nurses (AAOHN) has been an Affiliate of the NIOSH TWH program since 2016. AAOHN is committed to advancing their members knowledge regarding TWH and to increasing the rate of implementing TWH programming within the workplace (CDC, 2020b).
The evidence base for the positive impact of TWH Health® programs is growing. For example, Anger et al. (2015) reviewed 17 TWH intervention studies to evaluate impact on risk factors for employees’ health. Approximately 94% of the interventions improved risk factors related to injuries and chronic illnesses. Examples of interventions included physical exercise and stress management programs, weight loss and safe driving competitions, and training/coaching in health eating and exercise. In a 2016 systematic review, Feltner et al. (2016) found that TWH interventions may improve overall health behaviors, such as decreased tobacco use or improve healthy eating, but the impact of these intervention on quality of life and reduction in injuries is unknown.
Based on these findings, a group of panelists and experts were convened to explore research gaps and develop future research focus areas that would contribute to the advancement of total health of workers (Bradley et al., 2016). Eight recommendations were identified including setting priorities, developing a consensus conceptual framework, listing a set of core measures and outcomes, using a transdisciplinary process, including a range of worker population and settings, using rigorous methodologies, disseminating findings to a wide audience, and using research to develop TWH research laboratories (Bradley et al., 2016). In addition to prioritizing a unified approach to TWH research, Newman et al. (2020) proposed a set of TWH competencies to standardize education and training, further supporting the knowledge needs of OHPs.
The Bureau of Labor Statistics (2020) reported approximately 900,000 nonfatal injuries/illnesses occurred in the work setting in 2018, and approximately 1,200 workers died from work-related illness in 2018. Fortunately, however, prioritizing the health and safety of employees is becoming a trend (Chaudet, 2019) and some organizations have begun to place more attention on their employee’s overall health and wellness beyond the time they spend within the work environment (Hersman, 2018). This shift in attention is critical, for chronic co-morbidities are rising within the United States. The CDC (2017) recognized that employers have a unique opportunity to advance the level of care offered to employees at work and outside the work setting. Chronic conditions such as diabetes (CDC, 2020a), arthritis (Barbour et al., 2017), obesity (American Society for Metabolic and Bariatric Surgery, 2018), heart disease, and cancer are among the top causes of death and disabilities (CDC, 2018b). Schill (2017) stated that TWH is a new paradigm that advocates for a “foundation of safety and health through which work can contribute to a higher level of well-being” (p. 158).
The Department of Health and Human Services (2016) in conjunction with NIOSH determined that TWH can be achieved in workplaces through 5 key elements: (a) demonstrating leadership commitment to worker safety and health at all levels of the organization, (b) designing work to eliminate or reduce safety and health hazards and promote worker well-being, (c) promoting and supporting worker engagement throughout program design and implementation, (d) ensuring confidentiality and privacy of workers, and (f) integrating relevant systems to advance worker well-being.
Occupational health professionals (OHP’s) require resources and education to advance the concept of TWH within their organizations. OHP’s can prepare for the future by following industry trends to guide the integrated approach of TWH. The American Society of Safety Professionals (ASSP, 2020) identified significant trends that are driving the future of safety such as the demographics of the world population, technology advances, emerging businesses, work relationships, and the speed of change. By following these trends, OHP’s can bridge gaps between safety and health promotion within the organization’s occupational health programs and policies.
The Center for Health, Work & Environment at the Colorado School of Public Health is one of six Centers of Excellence for TWH and is a funded resource for OHPs to obtain additional knowledge on TWH. The mission of this center is to conduct research and educate future safety and health leaders to advance worker health, safety, and well-being. Housed within the Mountain and Plains Education and Research Center (ERC), this TWH center supports the research and training of future occupational health and safety leaders through online continuing education, TWH leadership programs, and Certification in TWH (The Regents of the University of Colorado, 2020).
The purpose of this study was to explore OHP’s current level of knowledge regarding TWH, determine the number of OHP’s that have adopted the TWH concept, and describe the factors related to challenges and needs perceived by the OHP’s to integrate TWH within the organization’s culture. The information obtained from the study will provide organizations who support OHPs, such as the AAOHN, with key data to drive educational programs, assist OHP’s to embrace and lead change within their organization to support the successful integration of TWH, and more importantly, to support the well-being of employees while at work or home.
Methods
This cross-sectional study surveyed OHP’s in the US to examine whether attitudes toward change and knowledge of TWH predicted readiness to implement TWH programs. The 82-question electronic survey was distributed via email to 4,777 OHPs who were active members of the AAOHN in 2019. Participation was elicited by clicking on an URL embedded within an email from the AAOHN Executive Director. The survey was available for a 3-week window, and two survey completion reminders were sent by AAOHN during this timeframe. Professional characteristics were measured by multiple choice questions including role in occupational setting (licensed practical nurse, registered nurse, advance practice nurse, or other such as a paramedic), work setting (hospital/clinic, corporate setting, academic, consultant and other), multi-site/facility (Yes/No), number of employees (<100 to > 500), respondent education (from EMT Certification to Doctor of Nursing Practice), and years practicing (from <1 to >15). Knowledge regarding TWH was measured using a single dichotomous item asking “are you familiar with the concept of Total Workers Health” (yes/no) and by five multiple choice questions such as “TWH is defined as” (each having one correct response). The existence of a current TWH program was assessed with a single item asking if the facility has a TWH program (Yes/No/Unsure). For those without an existing TWH program, respondents were asked if they were interested in creating a program (Yes/No) and what challenges are anticipated in creating a program (multiple choice mark all that apply).
Attitude toward change (Kwahk & Ahn, 2010), resistance to change (Oreg, 2003), organizational readiness for change (Claiborne et al., 2013), leadership commitment toward safety changes (Faris & Parry, 2011), and transformational leadership (Clark, 2011) were measured using standardized instruments that were modified slightly to make wording applicable to the study participants; for example, changing “staff” and “students” to “employees.” The responses used a five-point Likert-type scale (strongly disagree = 1 to strongly agree = 5), with each group asking the respondent to reflect upon their own attitudes. The AAOHN leadership reviewed the survey questions for face validity confirming the items were appropriate, clear, and inclusive.
Data Analysis
Descriptive statistics were compiled for each question. In addition, five sets of inferential statistics were computed by dividing the responses into two groups based on their responses to several of the background questions and running two-tailed t-tests to detect statistically significant differences between groups. Specifically, groups were created based upon their response to the “Familiar with TWH” question (as well as their response to whether or not their organization has a TWH program). Groups were also created based upon responses to three demographic questions: years of experience (≤5 years, ≥6 years), education level (Bachelor’s and below Master’s and above), and age (≤45 years, ≥46 years). This study was reviewed and approved by the Chatham University Institutional Review Board.
Findings
Two hundred fifty-three (5.3% response rate) respondents returned the survey and 198 completed all questions. When performing the inferential statistical analysis using the groups listed above, we found that 76.3% of respondents were familiar with TWH, though only 26.1% were certain that a TWH program was implemented by their organization. In addition, the majority of the respondents fell into the groups with 6 or more years of experience (82.6%), an education level of bachelor’s degree and below (71.9%) and aged 45 or younger (52.4%).
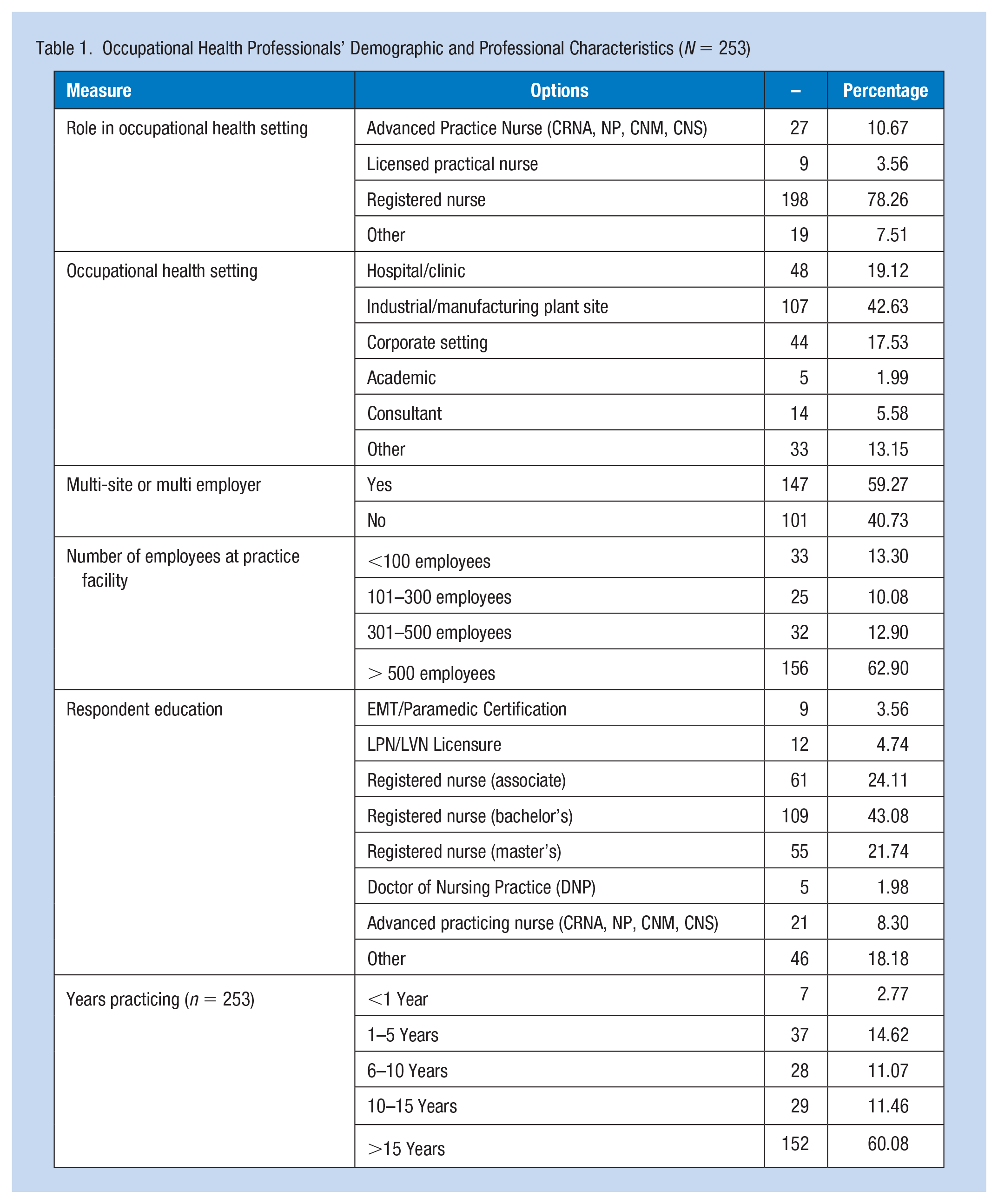
Table 1 describes the personal and professional characteristics of the sample. The majority of survey respondents reported being registered nurses (78.3%) followed by advance practice nurses (10.7%), licensed practical nurses (5.6%), and others (7.5%), which included a variety of roles including Safety and Wellness Organizational Consultants and Directors of Health, Safety, and Wellness. The facilities where these OHP’s practiced included industrial or manufacturing plant sites (42.6%), hospitals and clinics (19.1%), and corporate settings (17.5%), among others. These organizations often covered multiple facilities (59.3%), and the majority of facilities had more than 500 employees (62.9%). Most respondents (75.1%) also achieved a bachelor’s degree or higher educational level, though others reported EMT/Paramedic certifications (3.6%) and LPN/LVN Licensure (4.7%), among other qualifications. Most respondents (71.5%) also reported more than 10 years of experience practicing occupational health.
Occupational Health Professionals’ Demographic and Professional Characteristics (N = 253)
The majority of respondents reported familiarity with the concept of TWH (76.3%), though most did not have a TWH program in their organization (56.6%) or were not sure if such a program existed (17.3%) (Table 2). However, of the respondents who reported they did not have a TWH program in their organization or were unsure, the majority (74.4%) expressed interest in implementing such a program. The primary hurdles reported for implementing a TWH program are, in decreasing order from most to least impactful: personnel to implement a program (62.4%), budget (59.5%), management commitment (56.7%), time constraints (50.3%), and employee interest (39.9%).
Occupational Health Professionals’ Familiarity With and Adoption of Total Worker Health Program
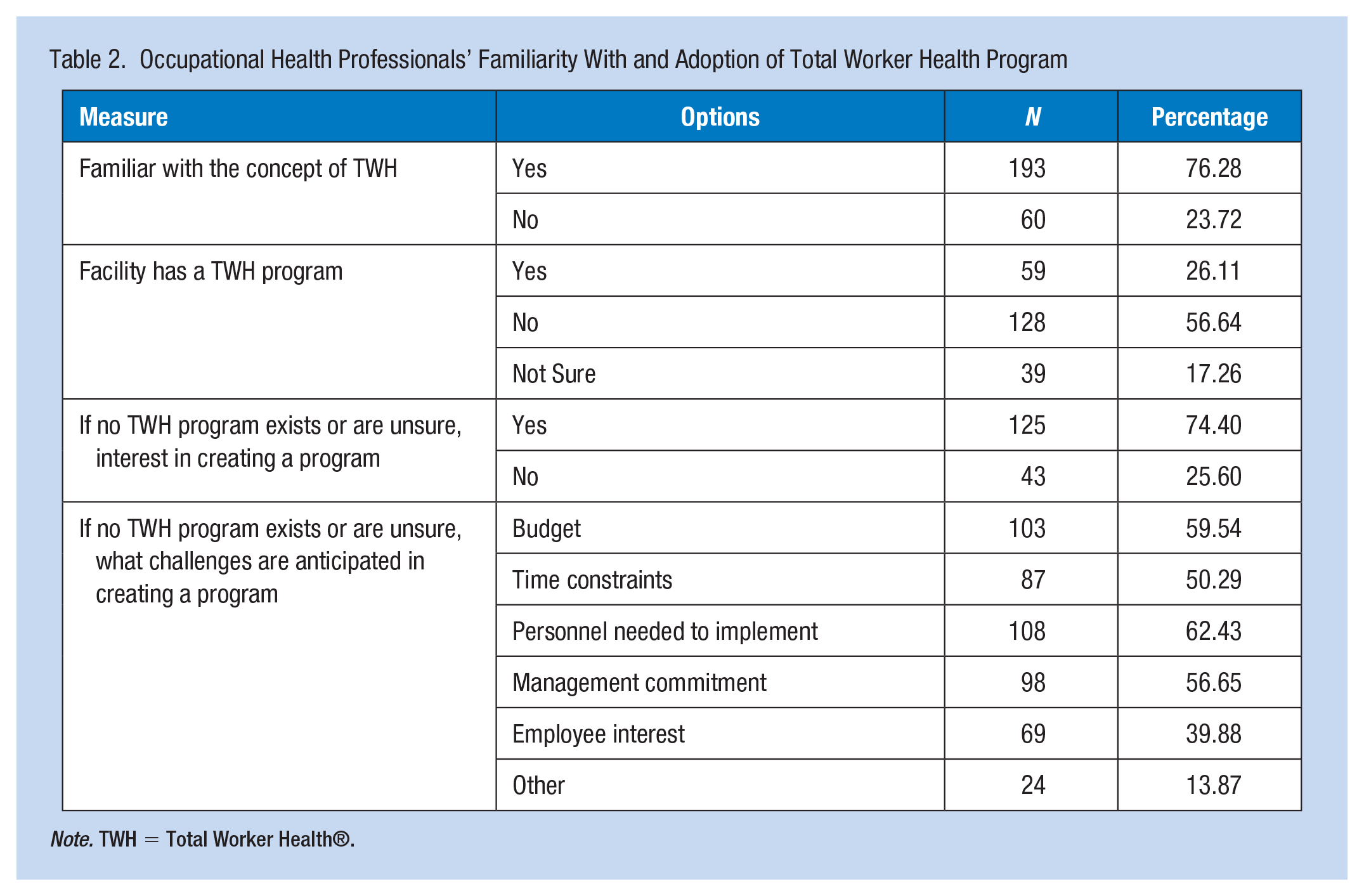
Note. TWH = Total Worker Health®.
Many of the respondents reported they had positive attitudes toward change. The highest mean scores on the 5-point Likert-type scale were given for statements such as “I am inclined to try new ideas” (M = 4.2, SD = 0.7), “I usually support new ideas” (M = 4.1, SD = 0.6), and “I often suggest new approaches to things” (M = 4.0, SD = 0.7). Similarly, some of the lowest self-reported mean scores were given for statements that demonstrated resistance to change, such as “I generally consider changes to be a negative thing” (M = 2.0, SD = 0.7) and “I like to do the same old things rather than try new and different ones” (M = 2.0, SD = 0.7). However, this was not universally true, as some statements such as “If I were to be informed that there’s going to be a significant change regarding the way things are done at work, I would probably feel stressed” (M = 3.1, SD = 1.0) and “My views are very consistent over time” (M = 3.3, SD = 0.9) had higher mean response scores.
Responses were more mixed when participants responded to statements regarding their organization and leadership rather than themselves. For example, respondents generally agreed that “Some employees resist any type of change” (M = 4.2; SD = 0.7) and that “Employees ask questions and express concerns about changes” (M = 3.9, SD = 0.8). However, they also generally agreed that “The leadership is genuinely interested in safety” (M = 4.0, SD = 0.9) and “Leaders in my organization are personally involved in activities that promote safety” (M = 3.9, SD = 1.0). When considering their own impact on leadership, respondents reported high mean scores for statements such as “I get things done” (M = 4.4, SD = 0.8) and “I help others with new ways of looking at new and complex ideas or concepts” (M = 4.0, SD = 0.8).
Employees who were familiar with TWH report more favorable feelings toward change and self-reported qualities that imply transformational leadership (Table 3). For example, respondents who were familiar with TWH reported being more inclined to try new ideas and to suggest new approaches. They also reported less of an impact on their emotional state when things do not go according to plans or when unexpected changes are announced. They also reported more flexibility regarding the employees that they supervise and that they go out of their way to make employees feel comfortable around them. None of the statements related to the organization or leadership was statistically significant. Similarly, respondents who worked for an organization with a TWH program report that their places of employment are more favorable toward change and that employees are adaptable when they need to accommodate change.
Occupational Health Professionals’ Response to Survey Questions Regarding Openness to New Ideas and Change by Whether or Not They Are Familiar With Total Worker Health (N = 253)
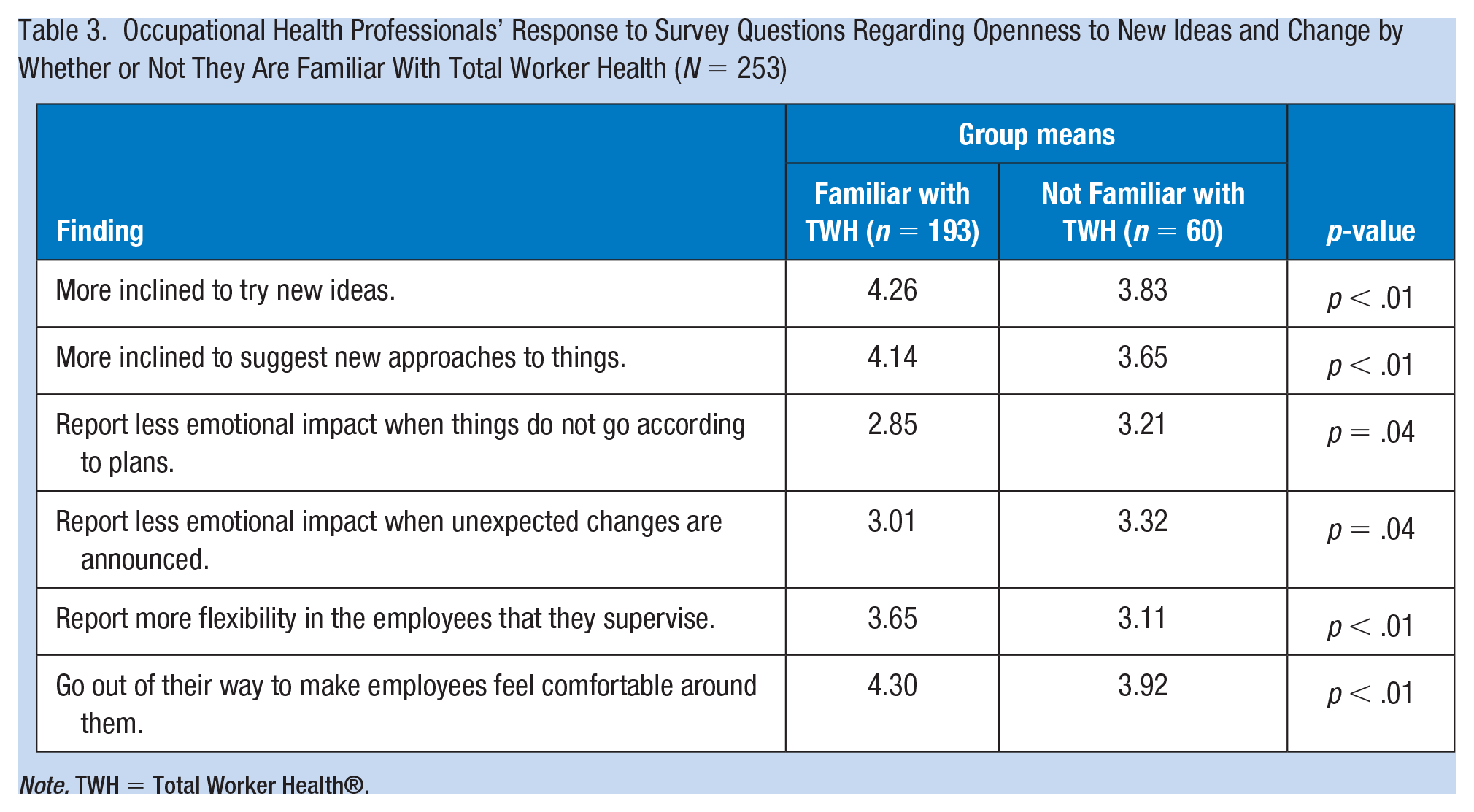
Note. TWH = Total Worker Health®.
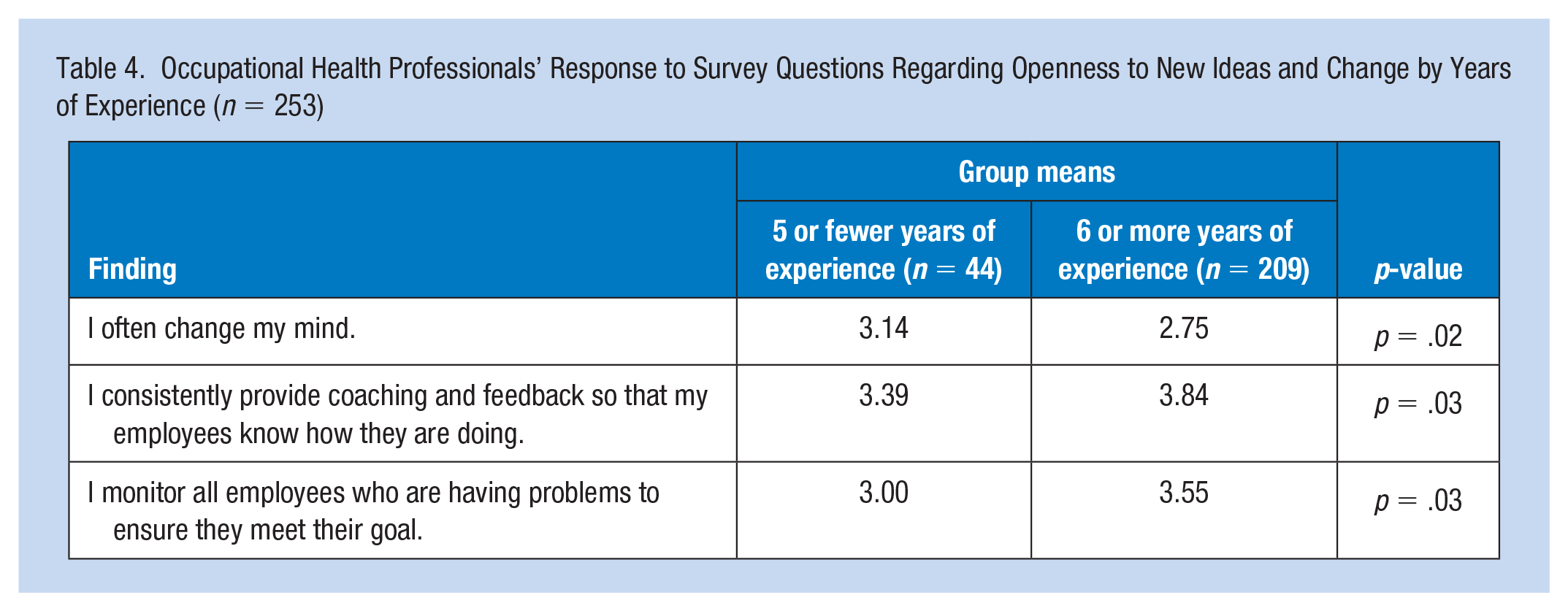
Table 4 summarizes the impact of experience on readiness for change. More experienced respondents tended to be more resistant to change; respondents with five or fewer years of experience were more likely to agree with statements like “I often change my mind.” However, these more experienced respondents also reported being more supportive of their employees, being more likely to agree with statements such as “I consistently provide coaching and feedback so that my employees know how they are doing” and that they “monitor all employees who are having problems to ensure they meet their goal.”
Occupational Health Professionals’ Response to Survey Questions Regarding Openness to New Ideas and Change by Years of Experience (n = 253)
Furthermore, respondents with higher levels of education were found be more favorable toward change, and they overwhelmingly reported being supportive of their employees (Table 5). Respondents (Total n = 263 [BSN n = 169; MSN n =6 6; Other n = 18]) with a master’s degree or higher education were more likely to agree with statements such as “Employees understand that specific changes may improve outcomes for them and their families” and “Most employees are willing to try new ideas.” In half of the 18 questions regarding transformational leadership, respondents with a Master’s degree or higher were more likely to express their leadership qualities, agreeing with statements such as “I let employees work toward their degree plan in the manner that they want” (p < .01) and “I help employees with their self-development” (p < .02) more highly than respondents with a bachelor’s degree or lower education level.
Occupational Health Professionals’ Response to Survey Questions Regarding Openness to New Ideas and Change by Level of Education (N = 253)
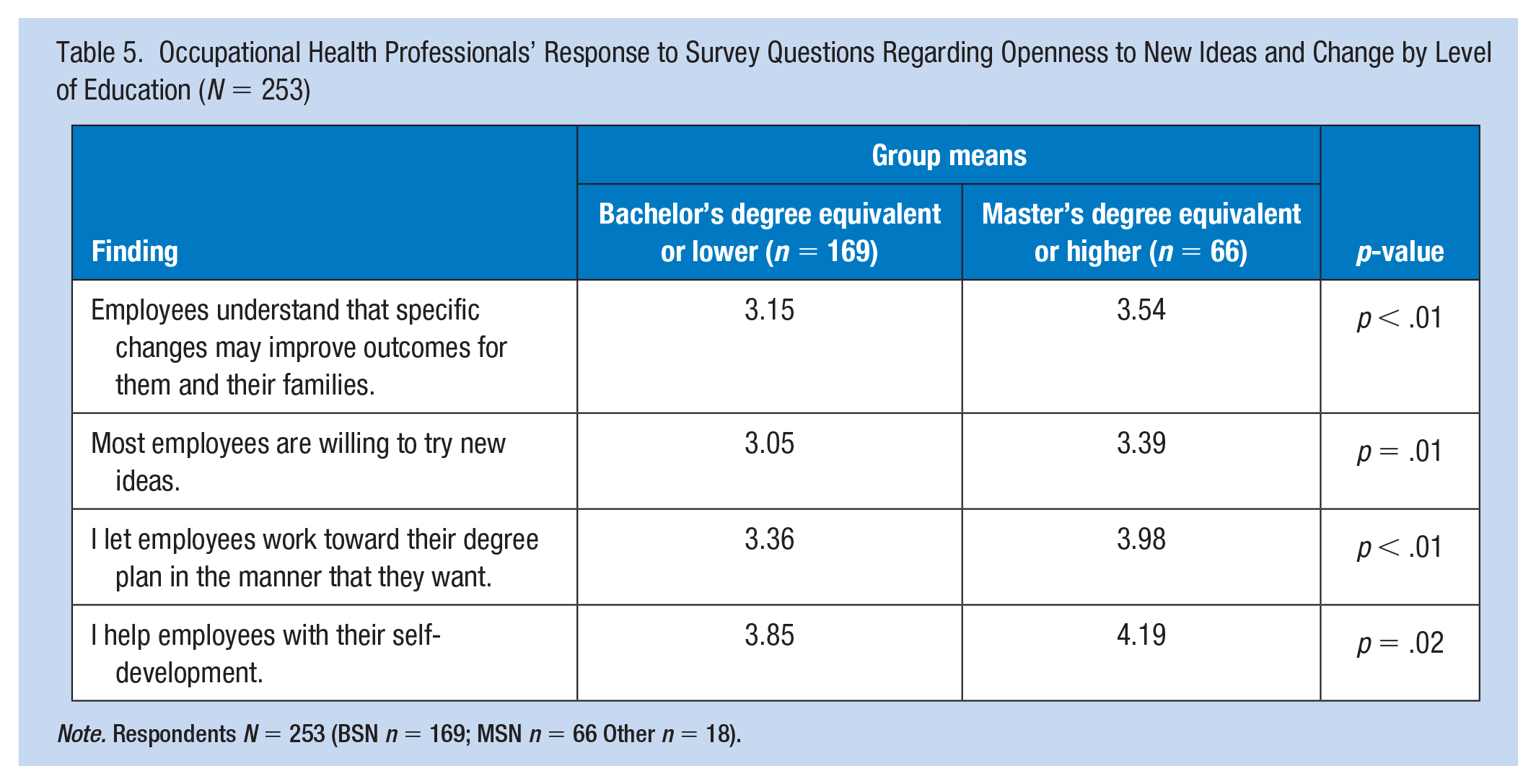
Note. Respondents N = 253 (BSN n = 169; MSN n = 66 Other n = 18).
Few statistically significant differences were noted when dividing respondents into groups of age 45 and below and age 46 and above. However, older respondents responded being more resistant to change, agreeing with statements such as “When I am informed of a change of plans, I tense up a bit” (M = 3.1, p < .01) and “When things don’t go according to plans, it stresses me out” (M = 3.1, p = .03).
Discussion
OHPs are in a unique position to impact both the health and well-being of employees (at work and outside of work), but also worker families. Historically, OHPs focused on the worker and how the worker can remain safe while on the job. The TWH concept extends beyond the workplace and into the worker’s home and community environment. When adopting the TWH model, OHPs are holistically integrating workplace hazard reduction and health promotion by targeting risk factors in the workplace that can also contribute to health problems previously considered unrelated to work (CDC, 2018c).
The findings suggest a variety of positive attitudes about the adoption of TWH into organizations, as well as some potential warning signs regarding future adoption by some OHP groups. For example, some respondents reported caution toward change, suggesting some OHP’s may not view the adoption of a TWH program as a positive development at their workplace.
We also found that when stratified by experience OHP’s are more likely to take on additional leadership and support roles, indicating that senior employees may be relied upon to assist in the adoption of a TWH program. Such a positive mind-set can assist with overcoming hurdles that appear during TWH adoption. However, when considering the role of age, we found that some senior employees are more resistant to changes, noting feelings of stress, and tension when change occurs and when things do not go according to plans. This indicates that younger employees may be the more flexible ones when a TWH program is introduced, even if they are less likely to lead in its adoption.
The authors note several limitations to the results presented in this study. First, all measures were self-reported by the survey participants, which may lead to internalized bias being reflected in their responses. Second, the number of responses to the study implies margins of error in the reported means on the order of 5% to 7%, depending on the selected confidence level used in the computation. While this degree of uncertainty is encapsulated in the p-value results from our t-tests in the results, we opted to present mean values rather than intervals for clarity when summarizing the attitudes of groups. Furthermore, the number of responses received dwindled as participants approached the end of the survey, increasing those error margins in later responses. Finally, our analysis approach of obtaining trends and accumulating evidence from individual question responses rather than aggregating results (as was performed in several of the source studies for our measures) could lead to a different interpretation of the results than other methods of analysis.
OHPs can be transformational change leaders by embracing the concept of TWH and integrating TWH programs within their organizations. The CDC (2018d) has identified several assessment tools to begin the planning and assessment stage within their organizations. For example, the Center for Work, Health, and Environment created a Health Risk Calculator. This tool assists with identifying the costs associated with employee health and worker’s compensation expenses to further identify cost savings by implementing employee health programs. Another tool is the CDC Worksite Health Scorecard, which assists employers in identifying gaps in health, well-being, and safety programs, and to prioritize high-impact, evidence-based strategies for worksite programs in several different health related areas (CDC, 2018c).
The CDC (2018c) has also outlined a series of steps to assist organizations and OHPs by first eliminating workplace conditions that cause or contribute to worker illness and injury, or otherwise negatively impact well-being (see Figure 1). This includes factors related to supervision throughout the management chain. For safety, health, and well-being, redesigning the work environment where needed and removing impediments to enhance employer-sponsored benefits, as well as providing flexible work schedules is crucial. Through TWH, OHPs can encourage personal changes for improvements to health, safety, and well-being, while offering support for healthier choice-making, and provide safety and health education to enhance individual knowledge.
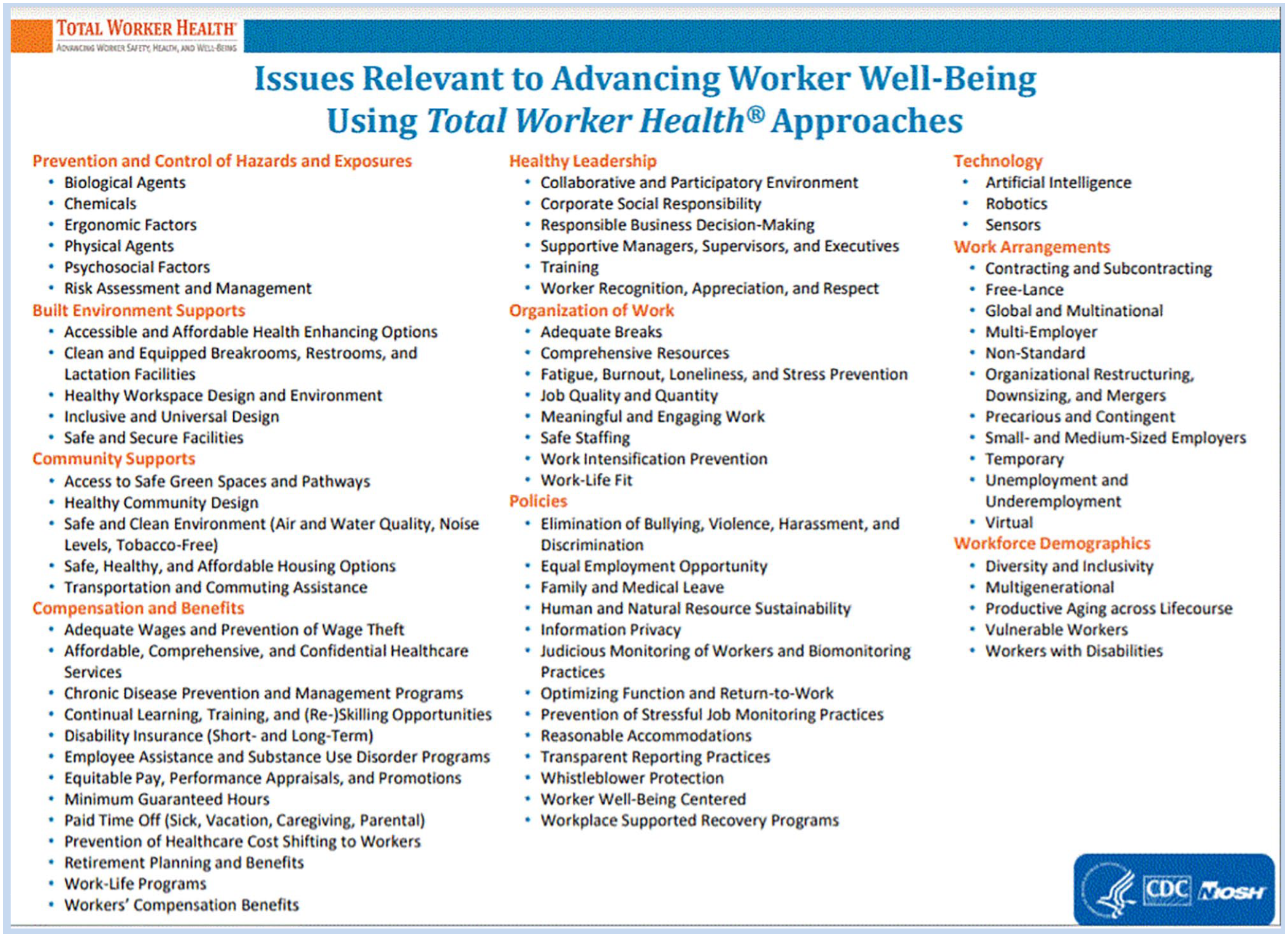
CDC (2020): Issues relevant to advancing worker well-being through total worker health.
Further research is needed to understand the impact an OHP can have on overall safety and employee well-being when integrating and supporting a TWH environment. NIOSH currently funds 18 Education and Resource Centers (ERC’s) across the United States to assist with training occupational safety and health professions in an interdisciplinary approach to translate research through education, training, and outreach (CDC, 2018a). Programs such as the Pathways to Prevention Program from the National Institute of Health (NIH, 2019) focused on TWH®: What’s Work Got to Do with it? The NIH outlined research gaps needed to address the ability to link data sets to improve occupational health initiatives, develop metrics to highlight return on investment of TWH initiatives, and collaborate with other agencies, such as the United States Census Bureau to better understand characteristics of worker populations. By understanding one’s current knowledge and beliefs regarding TWH, more advanced education and support can be provided to care for employees and their families consistent with geographic and population specific targeted programs.
There are many success stories where companies and organizations have implemented TWH programs. The CDC highlights these success stories, Promising Practices, on the TWH website to showcase industries that integrated successful policies, practices, and programs to protect workers safety and health, and also to advance the worker well-being (CDC, 2019).
Conclusion
The TWH approach is moving from the research to the implementation realm, through the support of the NIOSH. TWH not only focuses on safety and health of an employee, but also the health promotion of every employee to reduce injury and illness and advance overall well-being. Being an affiliate member of NIOSH, AAOHN is advancing TWH resources by offering educational opportunities, such as TWH implementation workshops, for its membership to better understand TWH and how to integrate such a program successfully into practice. The AAOHN website has a practice page dedicated to TWH titled “Make TWH about You and Your Employe,.” Hyperlinks and resources are available on this page to the NIOSH website, as well as many TWH implementation resources (AAOHN, 2020).
OHPs can provide the transformational leadership to guide change successfully and use their leadership position to fully embrace and integrate the concept of TWH to advance the safety, health, and well-being of workers. NIOSH TWH affiliates are working collaboratively to develop tools for assessing workplace needs as well as guides for successful implementation of a TWH program. OHPs can begin the discussions in their workplace, share the information, and establish stakeholders within their organizations to begin change within their organizations.
Applying Research to Occupational Health Practice
OHP’s are in a unique position to affect the health and wellness of workers and their families. The TWH concept integrates workplace hazard reduction with personal health factors that may affect their performance at work. Findings from this study indicated that AAOHN nurses are knowledgeable about TWH, are ready to change but they need more education, and resources to implement a TWH health program within their work facilities. Organizations, such as ASSP and NIOSH, have documented resources for the OHN to explore needs within their organizations, and tools for implementing TWH programs. Below is a list URLS that will provide direct access to these resources:
American Association of Occupational Health Nurses (AAOHN) TWH Practice Page:
http://aaohn.org/page/make-total-worker-health-about-you-and-youremployer
American Society of Safety Professionals (ASSP) Resource:
https://www.assp.org/advocacy/total-worker-health/total-worker-health-resources-and-tools
NIOSH Resources:
https://www.cdc.gov/niosh/docs/2017-112/pdfs/2017_112.pdf https://www.cdc.gov/niosh/twh/tools.html#Planning%20Resources https://www.cdc.gov/niosh/twh/letsgetstarted.html
NIOSH TWH Affiliate members, such as AAOHN and ASSP, are working collaboratively on research and educational endeavors to assist their members in implementing TWH programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kimberly A. Olszewski DNP, CRNP, COHN-S/CM, FAAOHN, FAAN ANCC board certified adult nurse practitioner and is a Certified Occupational Health Nurse Specialist and Case Manager from the American Board of Occupational Health Nurses. In 2007, she received her Fellowship distinction from the American Association of Occupational Health Nurses (AAOHN), and FAAN from the American Academy of Nurses in 2020. Olszewski currently serves on the AAOHN Board of Directors as President.
Debra M. Wolf, PhD, MSN, BSN, RN, FAAOHN Professor of informatics and nursing at Chatham University, and Independent Health care Informatics Consultant. Experienced administrative leader in strategic planning, organizational assessment, integration of innovative technology, performance improvement, quality assessment, and data analysis.
John Wenskovitch MScPhD student and adjunct instructor in the Computer Science Department at Virginia Tech (Virginia Polytechnic Institute and State University). His research focuses on human-centered computation, which incorporates both studies on how humans interact with technology as well as developing software to better support natural human interactions with data visualizations.