
Abstract
Background:
During the COVID-19 pandemic in the United States, healthcare workers were devastated by the insufficient preparedness to respond to their patients’ and personal health needs. A gap exists in resources to prevent or reduce acute and long-term healthcare worker mental illnesses resulting from COVID-19 frontline response.
Methods:
We performed an exploratory, mixed methods, longitudinal study of healthcare workers at a regional rural-urban hospital system in the Midwest United States during the COVID-19 response (4 timepoints, 2020). Using the Total Worker Health® (TWH) participatory needs assessment approach, self-identified frontline COVID-19 workers participated in a survey including Health-Related Quality of Life, Impact of Event Scale, and a modified version of the American Nursing Association COVID-19 survey; and a hospital timeline tracked system-level activities.
Findings:
Response rate at Timepoint (T)1 was 21.7% (N = 39) and of those, 14 (36%) completed all four surveys. From T1 to T4, the rate of COVID-19 patients steadily increased, staff exceeded the threshold for post-traumatic stress disorder at T1 and T4; staff reported not enough rest or sleep 50% of the month, T1-T4. Helpfulness of family support increased but community support decreased, T1-T4. Concerns with performing new tasks increased; the challenges related to lack of protective equipment and negative media decreased. Workers wanted to be involved in decision-making, desired timely communication, and needed adequate physical, environmental, and psychological supports.
Conclusions/Applications for Practice:
Utilization of a TWH® strategy for describing health needs, hospital response, and multi-level staff suggestions to workplace health solutions during the COVID-19 pandemic identified evidence-based health promotion interventions in a hospital system.
Background
An effective coronavirus 19 (COVID-19) response depends on a workforce that is capable of caring for patients and protecting public safety while maintaining personal health and well-being. Healthcare workers (HCWs) exposed to COVID-19 experienced post-traumatic stress, depression, anxiety, burnout, insomnia, and acute stress (Aymerich et al., 2022). At the end of 2020, a large survey of nurses found that over half of the respondents were exhausted, overwhelmed, anxious, and irritable, and fewer than one-third reported positive sentiments about their work such as “determined” and “optimistic about the future” (American Nurses Foundation, 2020). Additional studies revealed that HCWs were inadequately prepared, experienced emotional challenges, and received insufficient information (Koontalay et al., 2021). These findings suggest guidelines are needed to inform multilevel workplace health-promoting interventions to maintain workforce health.
The Total Worker Health® (TWH) approach offers strategies for assessing workplace stressors, conditions, policies, and practices to address holistic safety and health hazards (Punnett et al., 2020; Schill, 2017; Sorensen & Barbeau, 2012; Sorensen et al., 2016). A work organization’s employee safety, health, and well-being are affected by multiple variables including both physical and psychological working conditions, home and community life and environment, and personal health behaviors. These conditions contribute to workplace health and should be integrated during assessment activities (Punnett et al., 2020). Multilevel informants provide their lived experience and suggestions for solutions in this approach.
The overarching goal of this project was to use a TWH® strategy to perform a mixed-methods assessment of frontline HCW’s health needs during the first 9 months of COVID-19 in the United States to inform health promotion resources for the future. We replicated our previous longitudinal study procedures with public safety workers (Jaegers et al., 2020; Jaegers et al., 2021). Specifically, we aimed to: (1) map the real-time hospital response to COVID-19 preparations; (2) assess HCWs symptoms related to post-traumatic stress disorder (PTSD) as well as health-related quality of life; and (3) describe supportive, concerning, and challenging aspects of frontline work during COVID-19 and gather staff perceptions of personal and workplace preparedness.
Methods
This study took place at a hospital organization serving a large region of metropolitan urban and non-metropolitan rural counties (Economic Research Service, 2013). Using the TWH® strategy, two hospital wellness committee staff served as key informants during this study’s design, implementation, and reporting. The team identified existing survey measures and items of interest to targeted frontline work departments. We recruited our sample through recruitment flyers posted in staff areas to attract participants who self-identified as frontline COVID-19 workers. We estimated a sampling pool of 180 staff in direct and non-direct care, services, or supervisory positions. Participants were entered into a drawing for 1 of 13 US$25 gift cards at each time point for study participation. Ethical approval was attained from the Institutional Review Board at Saint Louis University.
Hospital System COVID-19 Response
A Hospital Timeline Diary was completed with hospital census data (all patients, COVID-19–positive patients), visitor restrictions dates, all staff communication response (email alert, well-being task force formed, and staff town hall meetings), and staffing changes related to layoffs and furloughs.
Staff Health-Rated Outcome Measures
Demographic data collected included age, gender, race/ethnicity, assigned work shift, direct or non-direct care, highest level of education completed, and work department. The Impact of Event Scale-6 (IES-6) was used to gauge symptom severity in PTSD-related categories of intrusion, avoidance, and hyperarousal (Hosey et al., 2019). Centers for Disease Control and Prevention (2000) assessment of health-related quality of life (CDC HRQOL-14) was used to measure constructs related to quality of life and well-being such as anxiety and energy levels.
Staff Reported COVID-19 Supports, Concerns, and Challenges
A modified version of the American Nurses Association (ANA, 2020) survey was used to gather knowledge, preparedness, and perceptions of workplace support during COVID-19, personal causes for concern with COVID-19, and challenges to protecting self and prevent the spread of COVID-19. Participants rated each item on a three-point rating scale: 0-not at all, 1-a little, and 2-definitely a lot. In addition, there were two open-text options for asking COVID-19 questions and suggestions for additional resources. Workforce data collection began in April/May 2020 with repeated surveys in June, July/August, and December. For the first three timepoints, online surveys were open an average of 10 days with the baseline (T1, 4/30/20), T2 and T3 repeated at 6 weeks between surveys. Participants completed the last survey 4 months after the T3 survey.
Data Analysis
Data were analyzed using version 3.5.1 of the R Foundation for Statistical Computing environment (R. Core Team). Means and standard deviations (SD) were computed for IES-6 and HRQOL-14. For the ANA survey, linear mixed-effects modeling was used to examine the variables across all four time points. We accounted for missing data by excluding missing values from the analyses because our value of missingness was less than the recommended cutoff where missingness could be ignored (<5%; Bennett, 2001). A basic two-level model with growth curves was used to examine trends among outcome variables for healthcare workers. Time was entered into each model as the Level 1 variable, with Person entered as Level 2. The significant variables included were two supports (family support, community support), one concern (performing new tasks), and two challenges (lack of PPE, negative media about one’s workplace). The remaining support, concern, and challenge variables did not show a significant change in participants over the four time points. We used maximum-likelihood estimation to compare the fit of the conditional growth model (full model) to the unconditional growth model (including time as a fixed then random slope) to examine the predictive power of time on the outcome variables. Model significance was reviewed at each step as well as the ICC calculation to examine within-person variability. Model significance was reviewed at each step for each of the above variables. Open-ended responses from the ANA survey were included from any timepoint. Two researchers independently content coded the open-ended responses into TWH® topic areas. They came to consensus on the thematic categories and summarized the qualitative results.
Results
Details from the Timeline Diary are provided in Table 1 and show the growing surge of the COVID-19 census during 2020. The cumulative hospital census and regional case rate was low at T1 coinciding with staff furloughs and layoffs but demonstrated an upward trend throughout.
COVID—19 Hospital Response Activities March—December 2020
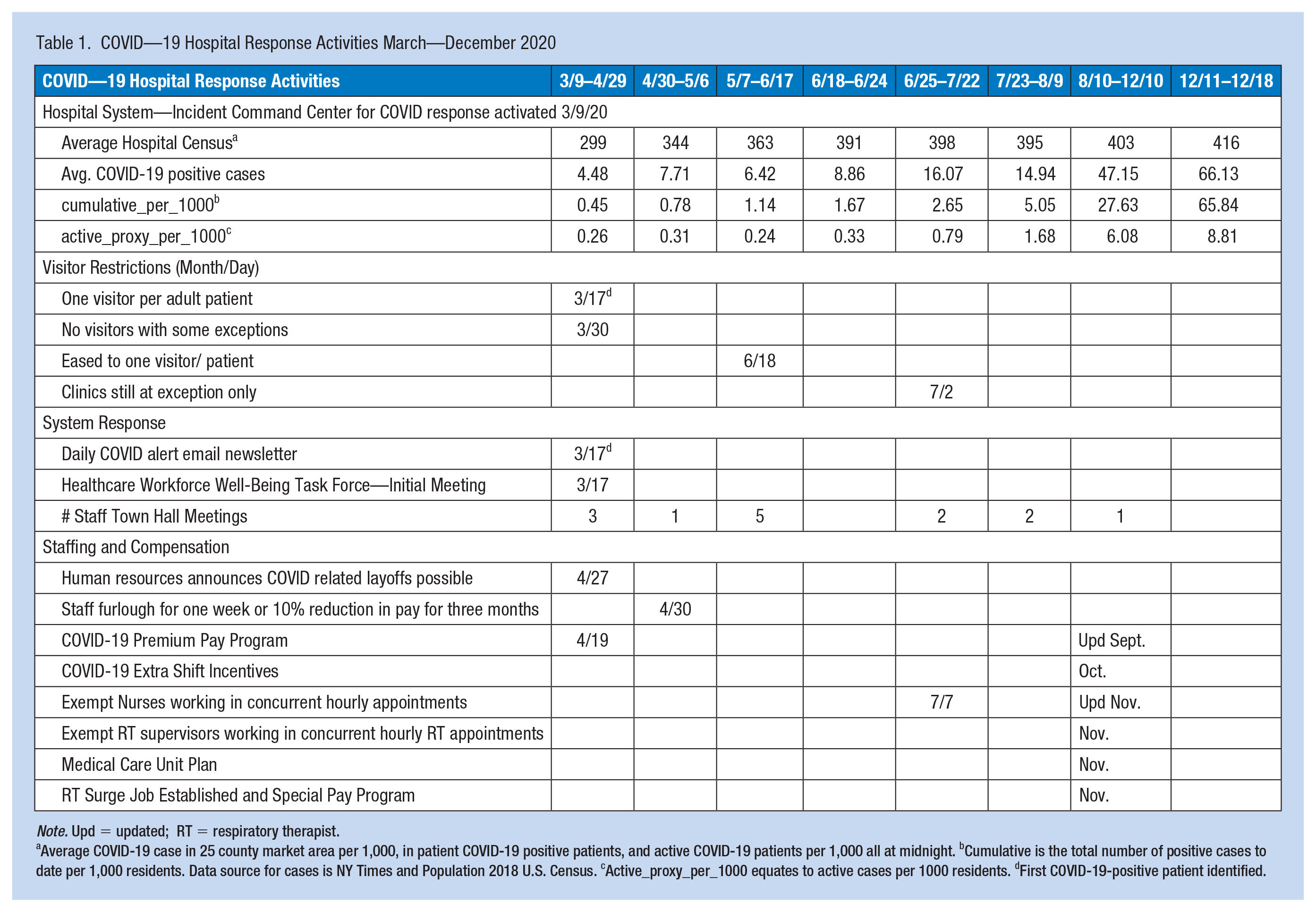
Note. Upd = updated; RT = respiratory therapist.
Average COVID-19 case in 25 county market area per 1,000, in patient COVID-19 positive patients, and active COVID-19 patients per 1,000 all at midnight. bCumulative is the total number of positive cases to date per 1,000 residents. Data source for cases is NY Times and Population 2018 U.S. Census. cActive_proxy_per_1000 equates to active cases per 1000 residents. dFirst COVID-19-positive patient identified.
The response rate at T1 was 21.7% (N=39) and of those, 14 (36%) completed surveys at all four time points, for a total of 56 observations. The sample at T1 (N=39) had a mean age of 39.5 years (SD 12.7), was primarily female (84.6%), white (92.3%), working full-time (92.3%), providing direct person care or services (69.2%), completed a bachelor’s, master’s or professional degree (66.7%); and worked in a department other than emergency or specified care services (61.5%). On average during T1 through T4, most worked during first shift 57.1% or a 12-hour shift 21.4%, all were currently employed, and all received health insurance benefits. At T1-T3 employees working within six feet of positive/presumed positive COVID-19 patient(s) ranged between 21.4% and 35.7%. At T4, there was a substantial increase to 76%.
Cohort mean scores exceed the symptom severity cutoff score (1.75) for post-traumatic stress (Hosey et al., 2019) at T1 (1.79, standard deviation [SD] 1.03) and T4 (1.79, SD 0.94). In health-related quality of life, participants rated not enough rest or sleep at the highest frequency at all four time points, for at least half of the month each time. Participants rated the number of days they felt very healthy and full of energy lower (mean range 6.29, SD 5.88 to 8.71, SD 9.11) than the days they felt sad, blue or depressed, (mean range 10.23, SD 13.43 to 13.57, SD 12.88). They rated the days they felt mentally unhealthy higher than the days they felt physically unhealthy at each time point.
Family support significantly increased over time and community support significantly decreased over time (Table 2). The null model for family support indicated 54% within-person variability and its relationship with time showed significant variance in the intercepts across participants (p < .01). There was a trend indicating an increase in family support from T1 to T4 with changes and responses consistent across participants. Community support over time showed significant variance in intercepts across participants, (p < .001). A trend indicated that community support decreased over time, with no significant differences in participants’ responses regarding community support for each timepoint.
Significant Frontline Staff COVID-19 Supports, Concerns, and Challenges Over Time (N = 14)
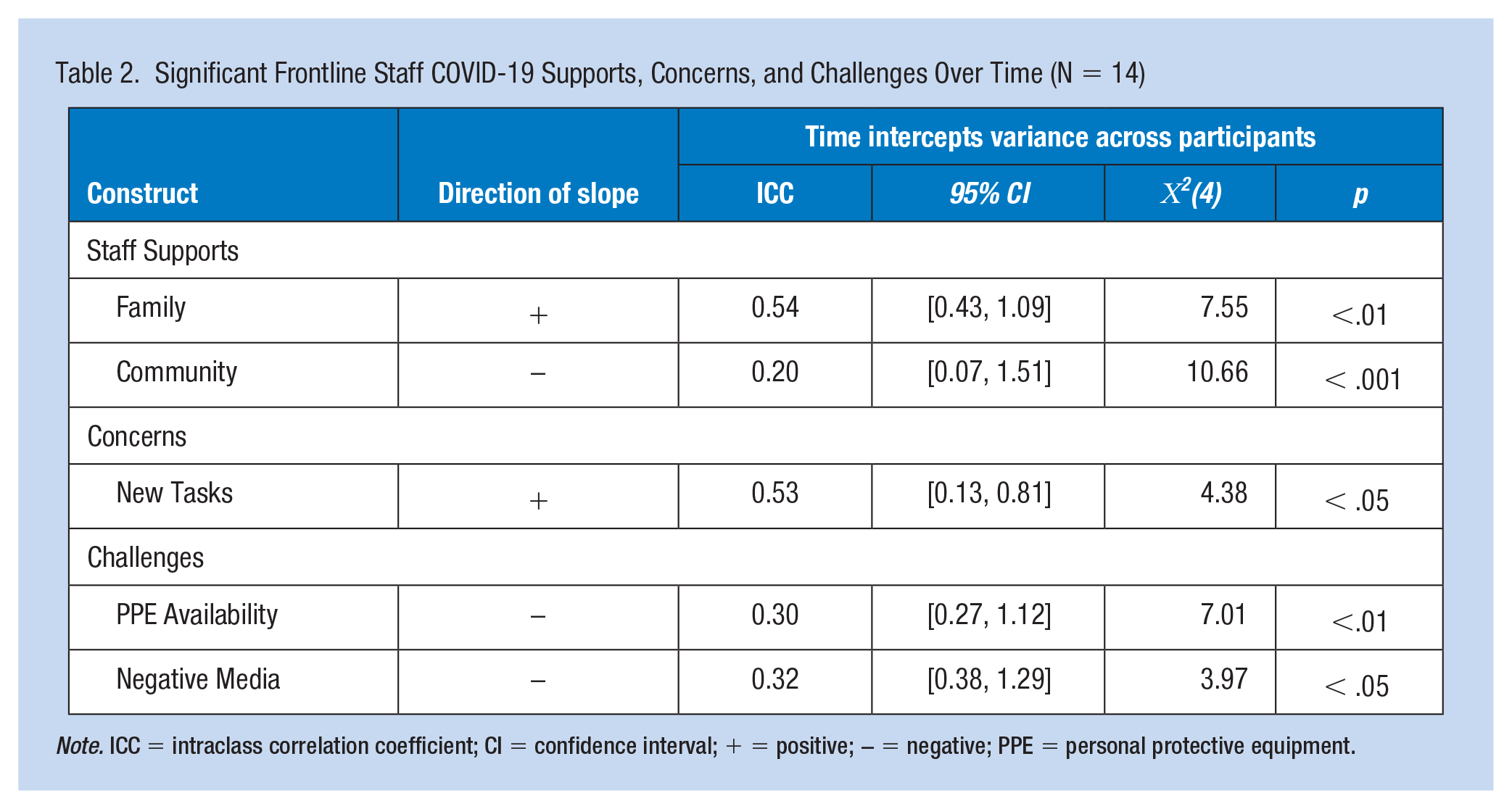
Note. ICC = intraclass correlation coefficient; CI = confidence interval; + = positive; − = negative; PPE = personal protective equipment.
Staff concerns regarding performing new job tasks showed significant change over time. There was 53% within-person variability, and there was an increase in performing new job tasks at each time point for all participants. The relationship between time and performing new job tasks showed significant variance in intercepts across participants(p < .05); however, there were no significant differences in participants’ responses regarding performing new job tasks across the timepoints.
Staff challenges showing a significant change over time included a lack of PPE and negative media coverage. There was 30% (ICC) within-person variability in the outcome and challenges related to lack of PPE over time decreased from T1 and T4 with significant variance in intercepts across participants (p < .01). Thus, as the COVID-19 pandemic progressed, the lack of PPE decreased for all participants, with no significant differences in participants responses about lack of PPE at any time point. The challenge of negative media about one’s workplace decreased over time for all participants (p < .05) and showed 32% (ICC) within-person variability in the outcome.
Table 3 describes open-text responses grouped under three categories from the TWH® strategy: Home, Community, and Environment; Physical Working Conditions/Environment; and Psychosocial Working Conditions. At T1, suggestions focused on engaging staff in problem-solving, gaining their perspectives, and caring about their contributions to decision-making. At T2, additional comments focused on staff mental health, technology needs, staffing support, and continued shared decision-making. At T2 and T3, community-specific themes emerged among participants including using the community to improve patient experiences and concerns about community safety, specifically related to college students returning to the community. Comments about pay and staffing needs persisted, and participants reinforced the need for workplace wellness supports. Finally, at T4, feedback expanded to vaccine and testing-related concerns, and criticisms of personal vaccine beliefs. Throughout the study, participants expressed concerns regarding patient isolation and mental health needs.
Hospital Staff Responses for Identifying Additional Information and Resources
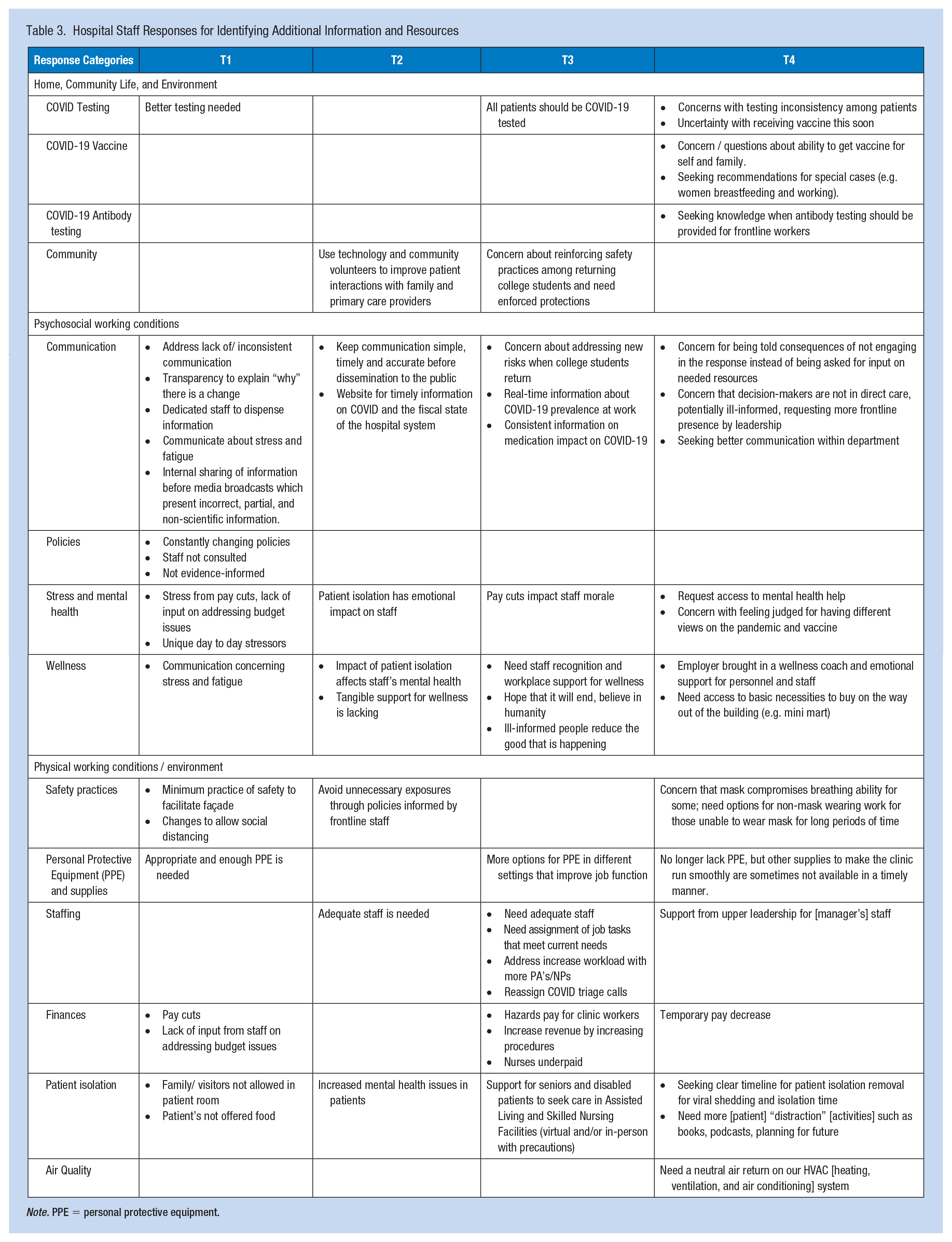
Note. PPE = personal protective equipment.
Discussion
We rapidly responded to assessing the needs of HCWs, health-related symptoms they experienced, and the hospital response to COVID-19, to inform future preparedness using the TWH® strategy. TWH® research acknowledges that innovative, specific work improvements are best informed by multiple sources (Dennerlein et al., 2020), which we employed through the hospital Timeline Diary and input from frontline health workers at four time points over a 9-month period.
Hospital worker studies from the SARS epidemic revealed a variety of important factors for coping including clear directives, the ability to provide feedback and gain management support; receiving support from supervisors/colleagues and family; talking to someone; and religious convictions (Chan & Huak, 2004). Existing health issues from challenging work combined with the effects of working during the COVID-19 response are likely to compound negative health outcomes among these frontline workers and supporting staff.
Respondents placed higher ratings on family support as time progressed; other studies demonstrate that family support mitigated the psychological toll on frontline workers during the early days of the pandemic (Du et al., 2020; Kannempallil et al., 2020; Teng et al., 2020). Open-ended responses suggest that two-way communication between frontline workers and administrators who set policy is needed throughout a pandemic-like crisis. In their study using TWH® during COVID-19, Dennerlein and colleagues (2020) note that top-down communication needs to be “clear, consistent, transparent, and empathetic” (p. 691) and needs to be followed by action. They note that workplace well-being includes a culture that values and listens to employee participation in the decision-making process.
Our findings of considerable positive symptoms of PTSD and poor health in participants are consistent among many studies and clinical commentary from the first year of COVID-19 (Greenberg et al., 2020; Ho et al., 2020; Lai et al., 2020; Morely et al., 2020). Employee support services could help reduce these symptoms; however, utilization of available services is often low (Kannempalli et al., 2020). Although we did not explore the utilization of employee assistance programs (EAP) or other support services, other research suggests that employees need to be directly connected to supports (Kannempallil et al., 2020). In addition, respondents cited lack of PPE and adequate training, and hospital data showed early furloughs followed by staffing shortages, all factors associated with poorer mental health in workers (Havaei et al., 2021). Outside the hospital, our participants noted a decrease in community support as the pandemic progressed, which may coincide with an increase in hostility toward frontline workers found in other studies (Ghaziri et al., 2021; Spader, 2020). However, the challenges of negative media also decreased over time. Effective crisis communication is needed during COVID-19 and some media coverage was inaccurate or even harmful (Su et al., 2021). Participants may have benefited from improved communication between the hospital system and the media during the early days of the pandemic when they found negative media coverage most challenging.
This study occurred during the COVID-19 pandemic response, the first of its kind in U.S. modern history. The sharing of this practical information by a medical system leaves them vulnerable to criticism, and they are commended for their willingness to share their experience so that lessons can be learned and solutions identified. Due to the fast-paced and precarious nature of the COVID-19 response, we designed our approach to reduce/prevent extra burden on staff since infection control remained the top priority of the workplace. We were also challenged by the recruitment of additional sites. A small sample size resulted from barriers to recruitment at the first time point and efforts to minimize the recruitment burden on the hospital. The response rate was low, however, not atypical for surveys, and therefore generalizability is low. As with any survey-based study, self-report and selection bias are potential threats to validity. We did not explore potential sources of biases between those who volunteered for study participation as compared with those who did not participate through all study time points. More study is needed among a larger hospital worker population.
Implications for Occupational Health Practice
The TWH® approach provides a holistic framework for workplaces to problem-solve concerns and identify solutions specific to their needs through multiple data sources. Although our project was small, we created evidence-based guidelines for hospitals using the TWH® approach. Implementation of our findings in real-time did prove challenging; hospitals can anticipate future needs based on these results and on lessons learned to prepare for the next crisis or pandemic. Engaging the people whom the policies directly affect may reduce the negative mental health symptoms frontline workers experience. Workplace assistance that directly links workers with community supports that can address burdens due to furloughs, pay reductions, child care needs, or other work–family conflicts. This assistance may be the EAP already in place but with a proactive outreach to employees. Improving sleep quality can be addressed through the intentional scheduling of staff. Reactive furloughs followed by staffing shortages were a lesson learned during the COVID-19 pandemic; ensuring appropriate staffing levels also improves sleep quality and reduces negative mental health symptoms. We recommend having adequate work-duty resources in place throughout a crisis response. This includes not only enough PPE and other equipment but also appropriate training on how to use them. Adequate training is also needed for new job tasks that frontline workers may have to adopt; it should not be assumed that each worker is proficient at all novel job requirements. We also suggest direct communication with the community, including purposeful methods to contact broadcast media to influence the narrative, or through direct communication to consumers, like social media. Misinformation and disinformation may have led to decreased community support in this study and increased hostility in other studies, and planned means to communicate through and by media may mitigate these findings. Finally, we recommend that hospital systems track and document data from multiple resources throughout a crisis response to fine-tune preparation and planning. At present, hospitals continue to record-low staffing, [low] revenue, and lack agility to respond to surges of other infectious diseases.
A TWH® approach based on reflections and current preparedness will support new efforts to address HCW health to reduce or prevent their risks for trauma and mental health issues for emergency response in the future. Applying the TWH® strategy provided a structured means for us to gather multilevel data and information during the early months of the pandemic. This project provides evidence-based findings using TWH® to inform future training and resources for health emergency preparation and response guidelines.
Applying Research to Occupational Health Practice
This study pilot used the Total Worker Health® strategy to investigate the needs of healthcare workers during the COVID-19 pandemic. Hospital response data demonstrated multiple policy and staffing changes. Staff experienced symptoms of post-traumatic stress disorder and did not get enough sleep over half of the month. They rated the days feeling sad, blue, or depressed higher than days feeling healthy. Staff reported an increase in family support but a decrease in community support. Concerns with performing new tasks increased but challenges related to lack of protective equipment and negative media decreased. Staff iterated throughout the need to be involved with policy decisions. Staff wanted clear and timely communication from supervisors. The desired support for physical work environment, such as adequate staffing and COVID-19 testing, as well as psychological needs to address the impact of pay cuts and overall worker morale. These data provide solutions to address future pandemic responses.
Footnotes
Acknowledgements
We commend leadership and staff for their dedication in responding to the COVID-19 pandemic. We thank the participating hospital system for allowing us to conduct this study with their healthcare staff. We appreciate the participation of healthcare staff working during the COVID-19 pandemic who made this study possible. Thank you to Dr. Ian Katz for Qualtrics survey setup support during the development phase of this project and Dr. Dana Stiles for data analysis consultation.
Author Contributions
LJ conceived the study, developed the workplace partnership, and obtained funding. LJ, JB, SS, SP, and MG contributed to survey development. LJ implemented survey data collection and LJ and AC completed data analysis. All authors contributed to the interpretation of the data, writing of the manuscript, and approved the final version.
Authors’ Note
This study was performed at Saint Louis University.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Spark Microgrant from the Saint Louis University Office of the Vice President for Research.
Ethics Approval
Ethical approval was obtained prior to data collection.
Informed Consent
Informed consent was obtained from each participant.
Institutional Approval
This study was approved by the Institutional Review Board (IRB) at Saint Louis University documented at the local IRB.