
Abstract
Background:
Health care workers (HCWs) are at high risk of COVID-19 infection; therefore, screening is recommended for early detection and management to break the chain of transmission. Globally, multiple strategies have been utilized for the screening of HCWs. This article reports and evaluates an active surveillance and screening strategy for severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) among HCWs following work or nonwork exposures in Brunei Darussalam to prevent health care–associated COVID-19 transmission.
Methods:
In March 2020, the Ministry of Health through the Occupational Health Division adopted an active screening strategy for symptomatic and asymptomatic HCWs, which involved symptom screening, risk assessment, SARS-COV-2 testing, and management following work/nonwork exposure and recent overseas travel, and those with influenza-like illness (ILI) symptoms. Screening frequency was based on the HCWs’ symptoms and exposure, with the intent to evaluate all possible sources of exposure.
Findings:
As of December 31, 2020, 821 HCWs were screened, of which 632 (77%) had ILI symptoms and 14 (1.7%) had high-risk occupational exposure. Reverse transcription polymerase chain reaction (RT-PCR) swab testing was carried out on 577 (70.3%) HCWs, with the highest proportion of swabs done on doctors (85.1%; p < .01) due to their workplace exposure (34.3%) and overseas travel (38.7%).
Conclusion:
By July 2021, Brunei Darussalam had recorded zero cases of COVID-19 among HCWs from occupational exposure. Our strategy of active screening for SARS-COV-2 RT-PCR testing since early in the outbreak has proven to be successful, in combination with infection control practices and public health measures, in the prevention of occupational transmission, thereby facilitating early return to work for HCWs with low-risk exposure and without symptoms.
Background
Health care workers (HCWs) are at high risk of severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) infection (COVID-19) as initially reported in a case series of 138 patients in Wuhan in January 2020 where 29% of affected patients were HCWs (Wang et al., 2020). By April 2020, more than 22,000 cases of HCWs from 52 countries were diagnosed with COVID-19 and reported to the World Health Organization (WHO, 2020a). A systematic review estimated that there were more than 150,000 infections and 1,413 deaths globally among HCWs from the outset of the pandemic in January 2020 through May 2020 (Bandyopadhyay et al., 2020). These figures had increased to 570,000 infections and 2,500 deaths by September 2020 (Pan American Health Organization/WHO, 2020). It was observed that infections were higher among female HCWs and nurses; however, there were more deaths among males and doctors (Bandyopadhyay et al., 2020).
HCWs have a higher risk of acquiring COVID-19 infection from their workplace as a result of exposure to infected patients or infected health care colleagues, as opposed to acquiring the disease from the community (Rivett et al., 2020). In a study from the United States, 55% of 1,423 HCWs infected with COVID-19 reported a positive contact at the workplace, 27% in the household, and 13% in the community (Burrer et al., 2020). In view of this, active screening, risk assessment, and clinical management of HCWs are important measures to take for early detection of the disease and to break the chain of transmission to co-workers and patients (WHO, 2020b). In early 2020, WHO (2020c) and the U.S. Centers for Disease Control and Prevention (CDC, 2020a) published guidelines on screening HCWs with suspected or confirmed contact with COVID-19 cases. These strategies include both passive and active surveillance whereby HCWs self-assess their symptoms and remotely report to their respective facility or authority by phone (passive) or are actively screened in-person for fever and/or other related symptoms (CDC, 2020a).
Brunei Darussalam is a country in South East Asia with a total population of 459,000 (Department of Economic Planning and Statistics, Ministry of Finance and Economy [DEPS, MOFE], Brunei Darussalam., 2019). Health care services in Brunei Darussalam are provided by four government hospitals, two private hospitals, several government health centers, and private clinics (Ministry of Health [MOH], Brunei Darussalam, 2019). In 2019, the Ministry of Health (MOH) recorded a total of 4,146 HCWs that included doctors, dentists, nurses, midwives, pharmacists, and other allied health professionals (AHPs). Eighty percent of these HCWs were employed in the government health sector (MOH, 2019)
Brunei Darussalam reported its first community transmission case on March 9, 2020, resulting in a total of 141 local and imported cases by May 6, 2020. Thereafter, confirmed cases of COVID-19 were from travelers diagnosed via reverse transcription polymerase chain reaction (RT-PCR) swab test on arrival during their mandatory 14-day quarantine period at government-designated quarantine facilities, including hotels. By June 15, 2021, there were 109 imported cases, resulting in a total of 250 cases (MOH, 2020a).
Methods
In March 2020, the MOH Brunei Darussalam through the Occupational Health Division (OHD) began active screening and surveillance of HCWs, including doctors, nurses, AHPs (radiographers, physiotherapists, laboratory staff, etc.), and support and administrative staff (receptionists, clerks, cleaners, security personnel, etc.). Screening was conducted using a questionnaire, developed by OHD, which collected demographic information on gender, occupation (doctor, nurse, AHP, cleaner, security personnel, administrative/support staff), workplace, symptoms of influenza-like illness (ILI; rhinorrhea, sore throat, cough, fever, shortness of breath), contact with a confirmed or suspected case, travel history (recent overseas travel, and if yes, when and where), and personal protective equipment (PPE) details. The PPE details included questions on the use of surgical/medical mask, N95 respirator or similar, gloves, face shield, goggles, head cover, shoe cover, fluid-resistant gown, and jupiter suit (a full PPE kit, including, head-to-toe body suit, shoe covers, face mask, and face shield). A risk assessment was conducted on each HCW based on the standard operating procedure (SOP) developed by MOH (2020b) following guidelines published by WHO (2020d) and CDC (2020b), USA; this assessment included job-specific PPE practices. By the first half of 2020, 74% of clinical HCWs had undergone respirator fit testing as a part of COVID-19 pandemic preparedness (Trivedi et al., 2021). Duration of contact exposure, estimated distance between the HCW and contact, work tasks involving aerosol-generating procedures (AGPs), and use of PPE were parameters considered for risk assessment. High-risk exposure was defined as those performing AGPs without wearing any PPE or wearing inadequate PPE, or those providing direct care to a confirmed or suspected COVID-19 case without wearing any PPE (MOH, 2020b). The SOP was disseminated to all health care facilities, both in the government and in private sectors.
A walk-in swab clinic was opened up to HCWs at the Occupational Health Clinic under the MOH, for their ease of accessibility and to avoid overcrowding at other designated swab centers that were open to the general public. This clinic also provided preemployment and periodic health screening to registered HCWs in the country. The clinic is located in the central area of the capital city, Bandar Seri Begawan, and is within 10 to 15 km distance from all primary and tertiary health care facilities of the Brunei-Muara district where almost 70% of the nation’s population reside (DEPS, MOFE, Brunei Darussalam, 2019). Health care workers with workplace or nonworkplace exposure to a confirmed or suspected COVID-19 case, those with recent overseas travel history, and those with symptoms of ILI were screened and swabbed as part of active surveillance for high-risk exposure. Nasopharyngeal (NP) swab for RT-PCR was the test method used for the diagnosis of SARS-COV-2. Health care workers’ participation was ensured by dissemination of the risk assessment SOP to all health facilities for awareness through departmental heads and supervisors.
Data were analyzed using Epi Info version 7.2.0.1 and presented using descriptive statistics, including percentages and proportions. For statistical significance, chi-square test was used to compare for symptom status, risk level, and RT-PCR test performed among different categories of HCWs and unpaired t test was used to compare screening pattern during outbreak and nonoutbreak phase of the pandemic.
Findings
From March 10 through until December 31, 2020, 821 HCWs were screened in the Occupational Health Clinic for SARS-COV-2, of which 341 (41.5%) were nurses and midwives, followed by 181 doctors (22%), 98 AHPs (11.9%), 83 administrative staff (10.1%), and 83 support staff (10.1%). Of the 821 HCWs, 495 (60.3%) were screened following their presentation with ILI symptoms, followed by 238 (29%) for close contact with either a confirmed or suspected COVID-19 case (224 from workplace contact, and 14 from nonworkplace contact), and 88 (10.7%) following recent overseas travel. Overseas travel and workplace exposure were the most common reasons for screening for doctors and dentists, whereas other occupational groups (ranging from 62.5% to 85.5%) were mainly screened following ILI symptoms (Table 1).
Type of Exposure and Screening Among HCWs by Occupational Group (N = 821)
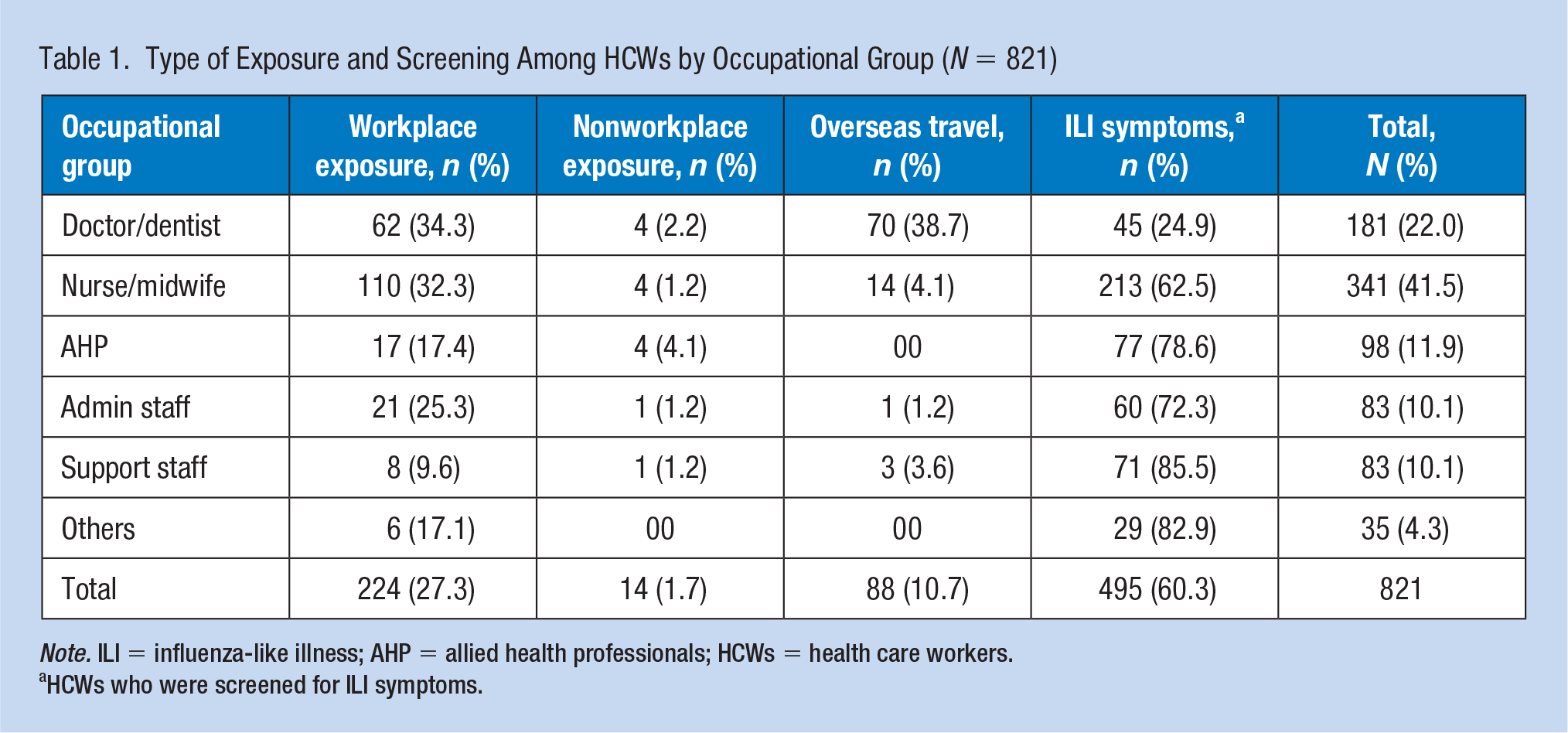
Note. ILI = influenza-like illness; AHP = allied health professionals; HCWs = health care workers.
HCWs who were screened for ILI symptoms.
During the screening process, 632 (77%) of HCWs had ILI symptoms and 189 (23%) were asymptomatic. A total of 495 of symptomatic HCWs were screened for their ILI symptoms; the other 137 were screened following contact exposure or overseas travel but also had ILI symptoms. The proportion of asymptomatic HCWs screened was significantly higher among doctors (50.8%) compared with other categories of HCWs (p < .01). Based on risk assessment, 14 (1.7%) HCWs were assessed to have high-risk exposure; however, there was no significant difference observed between different occupational groups of HCWs. The RT-PCR swab test was carried out on 577 (70.3%) of screened HCWs, with the proportion of swab testing observed to be significantly high among doctors (85.1%; p < .01) compared with other HCWs. This was due to a higher proportion of doctors returning from overseas compared with other HCWs as well as following workplace exposure. The PCR swab results were available within 24 hours and HCWs were advised to self-isolate or return to work with self-monitoring based on risk assessment according to the SOP (MOH, 2020b) (Table 2).
Risk Assessment, Symptom Status, and RT-PCR NP Swab Done Among HCWs by Occupational Group (N = 821)
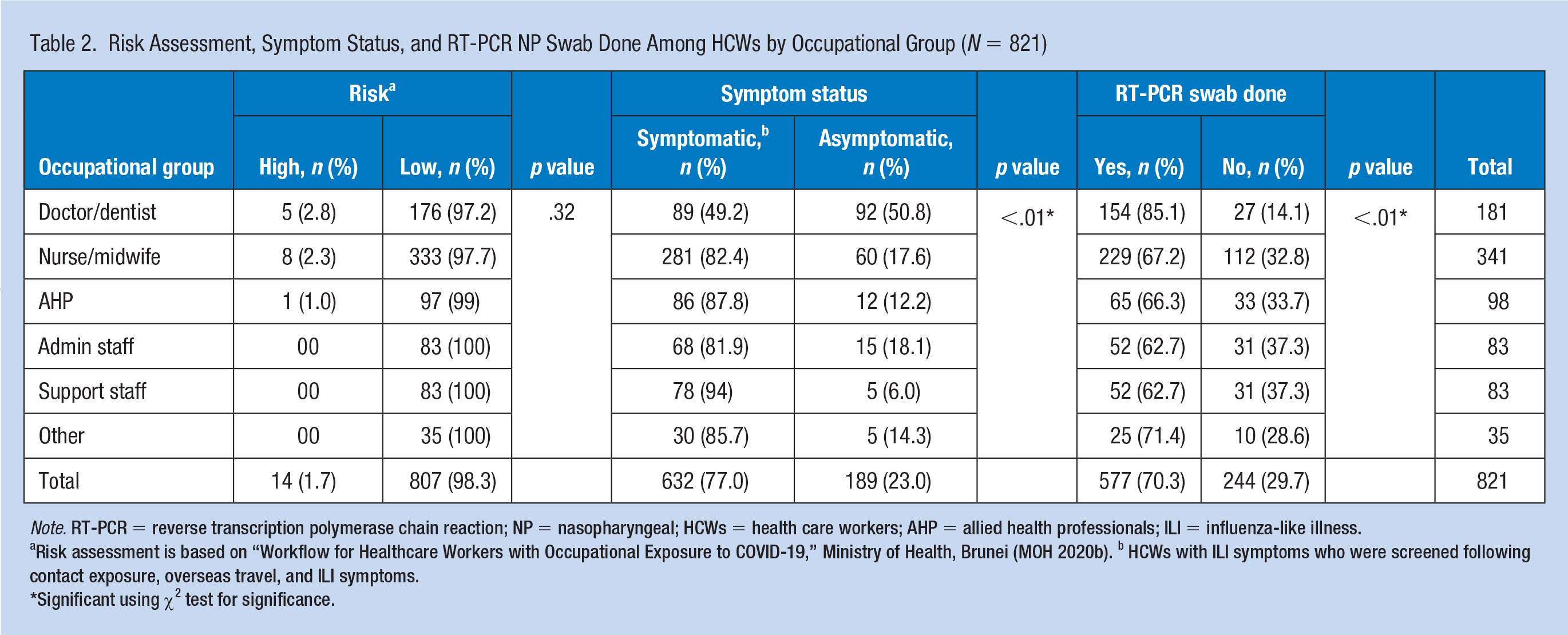
Note. RT-PCR = reverse transcription polymerase chain reaction; NP = nasopharyngeal; HCWs = health care workers; AHP = allied health professionals; ILI = influenza-like illness.
Risk assessment is based on “Workflow for Healthcare Workers with Occupational Exposure to COVID-19,” Ministry of Health, Brunei (MOH 2020b). b HCWs with ILI symptoms who were screened following contact exposure, overseas travel, and ILI symptoms.
Significant using χ2 test for significance.
Figures 1 and 2 indicate that during the 3 months following the first reported COVID-19-positive case in Brunei Darussalam, workplace exposure to a suspected or confirmed case accounted for the main reason for HCWs attending the Occupational Health walk-in clinic (p < .05). After Brunei Darussalam recorded its last community transmission case on May 6, 2020, attendance to the clinic was primarily HCWs presenting with ILI symptoms. A high proportion of HCWs returning from overseas travel were screened in March 2020 as soon as Brunei Darussalam implemented strict border control measures as well as outbound and inbound travel restrictions. As per Figure 2, when comparing between the outbreak period (March–May 2020) and nonoutbreak period (June–December 2020), HCWs screened in the clinic for the workplace (221 vs. 3) and nonworkplace (14 vs. 0) contact exposures were significantly higher during the phase of active community transmission. The overall number of HCWs screened in the clinic also showed a declining pattern in Q3 and Q4 of 2020 and this is attributed to a reduced number of COVID-19-positive cases in the country.
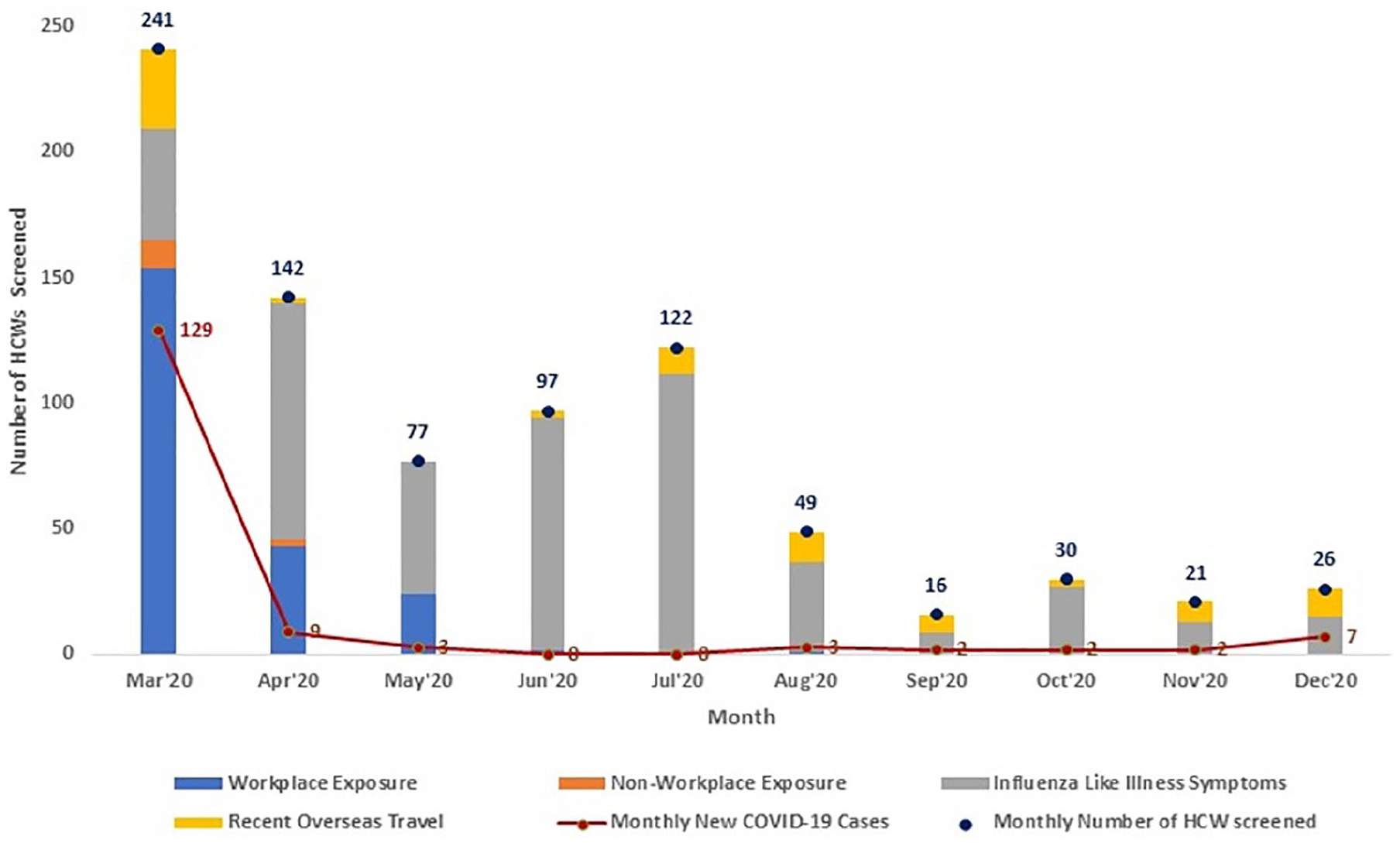
Type of screening on HCWs in relation to the number of new COVID-19 cases.
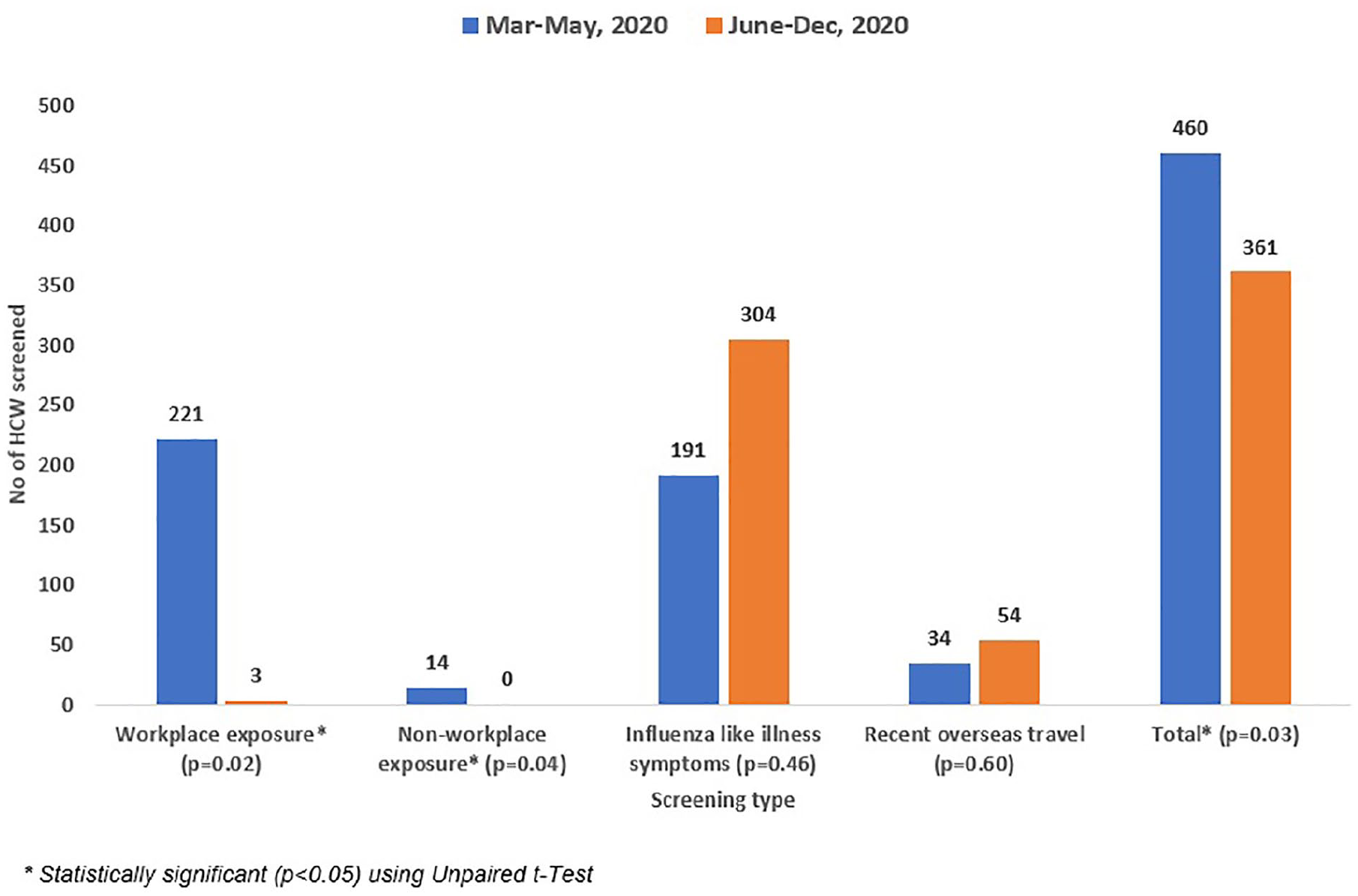
Screening pattern during outbreak phase (March–May 2020) and nonoutbreak phase (June–December 2020) in Brunei Darussalam.
Discussion
Since the start of the pandemic, various strategies have been adopted for HCW screening, ranging from surveillance of symptomatic HCWs to mass surveillance of HCWs, including those who were asymptomatic (Black et al., 2020; Chow et al., 2020). A number of studies reported that a high proportion of COVID-19-positive cases were either asymptomatic or presymptomatic at the time of diagnosis, still having transmission potential (He et al., 2020; Wong et al., 2020; Yanes-Lane et al., 2020). Therefore, this unknown transmission potential and the all possible sources of exposure were the main reason for Brunei’s HCW screening inclusion criteria for early detection and prevention of health care–associated COVID-19 transmission (Burrer et al., 2020; Freedman & Wilder-Smith, 2020; Rivett et al., 2020; Treibel et al., 2020). This active surveillance screening also facilitated an early return to work for asymptomatic HCWs with low-risk exposure and returning doctors from overseas travel, to avoid shortages of staff at health care facilities. To date, Brunei Darussalam has been successful in recording zero positive case among HCWs arising from an occupational exposure.
Applications to Professional Practice
Early in the global outbreak of COVID-19, Brunei Darussalam implemented a strategy of active surveillance and screening of symptomatic and asymptomatic health care workers (HCWs) with workplace and nonworkplace exposures, as well as those returning from overseas travel. We developed a standard operating procedure (SOP), an effective management communication strategy and provided a convenient location and clinic for HCWs separate from community clinics. This approach benefited the nation in preventing health care–associated transmission of the virus and in facilitating early return to work for HCWs with low-risk exposure and without symptoms. Such active screening strategy complements infection prevention and control (IPC) as well as public health measures, thus resulting in maintaining zero cases of COVID-19 transmission among HCWs from occupational exposure in Brunei Darussalam.
Footnotes
Author Contributions
A.L. contributed to concept and manuscript finalization; A.T. contributed to data analysis and manuscript draft; and M.F. contributed to data collection and management.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Ashish Trivedi is an occupational health practitioner, with more than 20 years of experience in the academics and workplace health services, currently working at Occupational Health Division, Ministry of Health, Brunei Darussalam.
Maria Fontelera is a public health and occupational health practitioner for more than 20 years, currently with the Occupational Health—Ministry of Health Brunei Darussalam.
Alice Lai is a consultant in occupational medicine and head of Occupational Health Division, Ministry of Health in Brunei Darussalam. She is also an adjunct senior assistant professor and serves as member of several national Committees and Boards. Her research interests and publications revolve around occupational and environmental health.