
Abstract
This case study draws attention to the psychosocial difficulties that emerged in the context of the coronavirus disease 2019 (COVID-19) outbreak in relation to the remote management of subjects with psychiatric vulnerabilities following exposure to prolonged quarantine. The case involves a 56-year-old hospital nurse, followed by the Occupational Health Department of a major university hospital in central Italy for mood instability in the context of a cyclothymic temperament. She was quarantined for occupationally acquired COVID-19 and remained positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) via swab test for more than 2 months between March and May 2020. In this case study, we discuss the challenges presented by the risk of a prolonged quarantine in a psychologically vulnerable employee, the need for occupational medicine to provide adequate health surveillance of all health care workers during the COVID-19 pandemic, the effectiveness of telepsychiatry, and the difficulties in formulating a proper treatment strategy.
Keywords
Introduction
Italy was one of the first countries impacted by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; coronavirus disease 2019 [COVID-19]) global pandemic and, as of the date of this article, the pandemic continues to grow with almost 3 million cases recorded in Italy and more than 90,000 deaths (World Health Organization [WHO], 2021). Italy was the first European country to impose a nationwide lockdown on March 13, 2020, setting forth a prohibition on leaving one’s home except for proven needs such as work, health or emergencies, as well as an absolute prohibition on leaving one’s home for people in quarantine who tested positive to the virus (Cagnin et al., 2020; Montanari Vergallo et al., 2020).
Quarantine and the resulting isolation in times of epidemics have been known to have negative impacts on the psychosocial well-being. The general themes reported in the literature are feelings of helplessness, fear of falling sick or dying, and increased levels of self-blame and low mood which can be wide-ranging, substantial, and long-lasting (Brooks et al., 2020; Reagu et al., 2021). Research exploring this issue, during the current COVID-19 pandemic across the world, reported higher levels of depression, anxiety, and post-traumatic stress symptoms in home-quarantined populations (Brooks et al., 2020; Reagu et al., 2021). Women, the young, and people over the age of 60 have been reported to be more vulnerable to the psychological effects of quarantine with low mood and irritability as the most prevalent psychopathological symptoms (Brooks et al., 2020; Pandey et al., 2020; Reagu et al., 2021). It appears that the emotional responses brought on by the pandemic and its management might be more substantial among vulnerable groups, such as people with preexisting psychiatric conditions or specific categories of subjects, like health care workers (HCWs; Buselli, Baldanzi, et al., 2020; Buselli, Carmassi, 2020; Buselli et al., 2019; Cagnin et al., 2020; Pan et al., 2021). Female HCWs who work on the front lines are at high risk of exposure to COVID-19 during the pandemic and may also have a higher risk of psychiatric symptoms during the COVID-19 pandemic (Vindegaard & Benros, 2020). The strict quarantine might exacerbate preexisting conditions such as depression and anxiety. Lockdown and boredom may unmask susceptibility to unhealthy behaviors, especially in the context of a mood disorder (Kontoangelos et al., 2020; Vinkers et al., 2020). Some studies describe an acute deterioration with improvement of symptoms in patients with mild psychiatric symptoms (de Kloet et al., 2005; Rohde et al., 2020). A more severe reaction to quarantine can be suffered by bipolar patients who may be intolerant to any form of limitation with a tendency to serious reaction both on the affective and behavioral level. In particular, a cyclothymic disposition, a temperament characterized by mood swings, was most frequently associated with anxiety-sleep disturbances, sensitivity to separation, eating disturbances in women, and antisocial-aggressive behavior in men (Perugi & Akiskal, 2002). These unnatural circumstances have been hypothesized to also lead to extreme risk-taking behaviors—including suicidal tendencies. Social isolation and loneliness are recognized risk factors for suicidal attempts (Brown & Schuman, 2021; Pandey et al., 2020). It is clear that the criterion of evaluation of the degree of distress associated to forced isolation depends on the clinical severity of the disorder in the present stage of its progress (Hernández-Gómez et al., 2021; Montanari Vergallo et al., 2020).
Health care workers who present both a preexisting psychiatric condition and that were quarantined for COVID-19 should be kept under close surveillance by occupational teams (Buselli, Baldanzi, et al., 2020; Buselli, Carmassi, et al., 2020; Buselli, Corsi, Baldanzi, et al., 2020; Buselli, Corsi, Necciari, et al., 2020; Holmes et al., 2020). A recent review published in the Lancet found that HCWs who had been quarantined had more severe symptoms of post-traumatic stress than members of the general public who had been quarantined, scoring significantly higher on all dimensions. Health care workers also felt greater stigmatization than the general public, exhibited more avoidance behaviors after quarantine, and were consistently more affected psychologically: They reported substantially more anger, annoyance, fear, frustration, guilt, helplessness, isolation, loneliness, nervousness, sadness, worry, and were less happy (Brooks et al., 2020).
In this regard, the scientific community has pointed out the need for tailored mental health interventions for HCWs (WHO, 2020). For several years, the WHO urged action on this issue and from the very beginning of the pandemic has emphasized the extremely high burden on HCWs. They have called for action to address the occupational health needs of HCWs who are needed to save lives but must also be protected from the serious impact on their physical and mental health (WHO, 2020). Therefore, supporting mental health of HCWs is a crucial part of the public health response to the COVID-19 pandemic (Buselli, Baldanzi, et al., 2020; Buselli, Carmassi, et al., 2020; Buselli, Corsi, Baldanzi, et al., 2020).
Many health organizations have already committed resources to the well-being of HCWs. The majority opted for helpline services, usually applicable and effective for urgent social and psychological problems (Buselli et al., 2021). Specifically, within hospitals, psychological services were offered to medical staff and patients in the form of psychological education and telepsychological and telepsychiatry interventions (Chen et al., 2020; Zaka et al., 2020). Evidence supports telepsychiatry, demonstrating good acceptance and similar outcomes across ages, conditions, cultures, and languages (Hilty et al., 2015). Remote consultation via telemedicine to accommodate the rules of social distancing during the peak of the COVID-19 pandemic was rapidly embraced in several countries (Kesner & Horáček, 2020). In particular, some countries adopted specific psychological support intervention programs, such as the program at University Hospital of Pisa in Italy. Azienda Ospedaliera Universitaria Pisana (AOUP), since the very beginning of the pandemic, organized an active medical surveillance program for health professionals with psychological disability. In addition to the monitoring of physical symptoms, and laboratory and microbiological tests, the Occupational Medicine Unit, through its multidisciplinary team, organized and conducted a psychological and psychiatric intervention specifically designed for HCWs using telemedicine (Buselli, Corsi, Baldanzi, et al., 2020). The team adopted the Istituto Superiore di Sanità (ISS, 2020) guidelines for stress management in HCWs during the SARS-CoV-2 emergency. It is an evidence-based approach to diseases and crisis management (Di Tecco et al., 2020; Jun et al., 2020; WHO, 2020). The aim of this case report is to draw attention on the psychosocial difficulties that emerged in the context of COVID-19 outbreak analyzing the remote management of a nurse with cyclothymic temperament and mood instability. She was followed by the multidisciplinary team of the Occupational Medicine Unit of AOUP since before the COVID-19 outbreak and quarantined for positivity to SARS-CoV-2 in March 2020.
This case study is noteworthy because it contains all the major psychosocial risk factors related to the pandemic and became the basis for a holistic and personalized approach to occupational health surveillance for HCWs, which has proven to be effective in this pandemic era (see Figure 1).
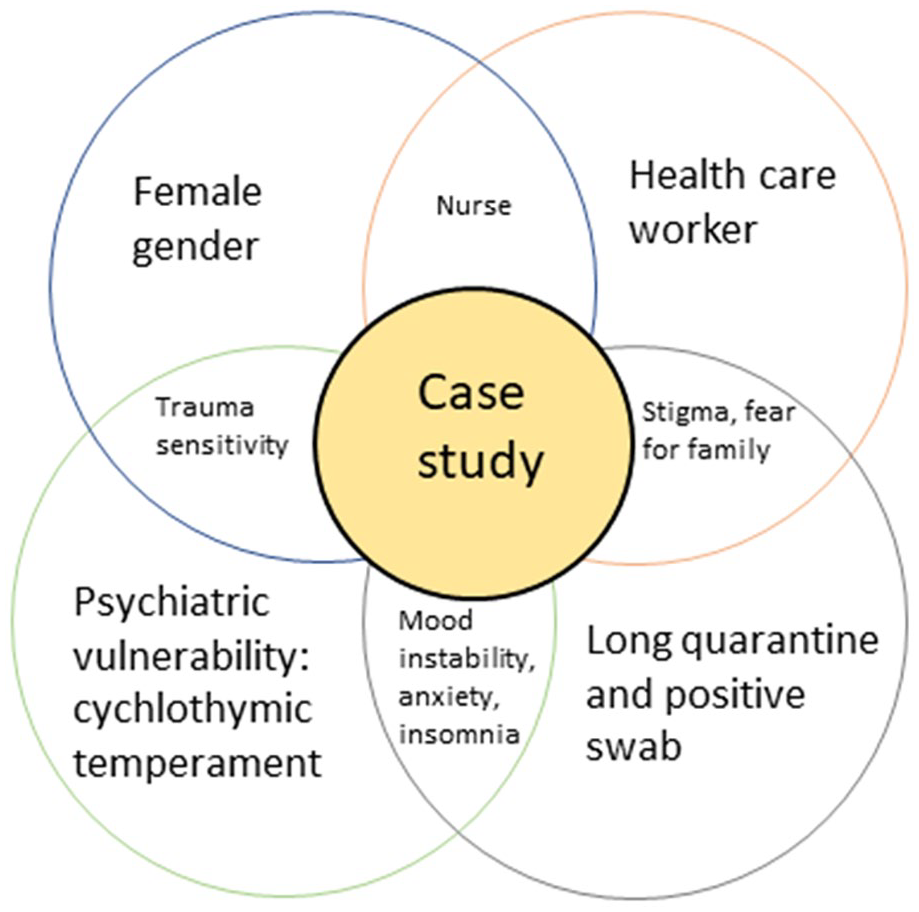
Case study: COVID-19 psychosocial risk factors.
Patient Information
Sociodemographic and Clinical Details
The patient was a 57-year-old female hospital nurse who lives with her two daughters and works as a shift nurse in a surgical department. The patient had no personal history for physical diseases except for fibromyalgia that was not on medication. The patient was not yet in menopause. She presented no family history for psychiatric disorder, but she was currently affected by a psychiatric disorder belonging to the mood spectrum and had been under pharmacological treatment for about 2 years.
Psychiatric History
Her premorbid temperamental and personological features included a cyclothymic temperament with hypersensitivity to stressful life events, and interpersonal sensitivity and impulsivity. She reported negative family history for psychiatric disorders. At the age of 54, the patient showed a worsening of emotional dysregulation with mood instability, affective lability, overt anger, anxiety fluctuation with minor panic symptoms, musculoskeletal somatizations, and subsequent diagnosis of fibromyalgia. As a result, the patient turned to the psychiatrist of the multidisciplinary group of the Occupational Medicine Unit directed by an occupational physician responsible for the physical and mental health surveillance of HCWs.
With regard to treatment choices, a standard treatment for mood spectrum disorders, based on gabapentin, an anticonvulsant with anxiolytic and analgesic properties, was combined with an integrated treatment for agitated depression, anxiety, and sleep disturbances based on a combination of perphenazine, a typical antipsychotic drug and a tricyclic antidepressant, amitriptyline. This treatment strategy led to a remarkable improvement in her clinical situation, including substantial mood stabilization, a reduction in anxiety, and improvements in global personal functioning. Thereafter the patient presented a period of euthymia (a stable mental state) of about 2 years.
COVID-19 Details and Psychiatric Clinical Findings
The patient tested positive for SARS-CoV-2 on March 13, 2020, and was started on home isolation. The Occupational Health Department, supported by hospital’s management, organized and conducted psychological and psychiatric interventions while the general practitioner managed her COVID-19 symptoms. During her absence, the worker was not replaced and she was on paid sick leave without losing her job.
She contracted the infection in the first 2 weeks of Italian pandemic when the workload suddenly increased, but at the same time, there were still inadequate protection systems. As she was undergoing home quarantine, she started taking anti-inflammatory medications, analgesics, and antibiotic (azithromycin) therapy under the supervision of her general practitioner. She presented the following symptoms of COVID-19: fever, dry cough, myalgia, and asthenia for almost 2 weeks. Her partner also tested positive in the same period and had been hospitalized for a few weeks. The patient remained positive for more than 2 months, finally testing negative on June 4. For the last 2 weeks of quarantine, the patient moved to a hotel for COVID patients because her home lacked the appropriate conditions to apply strict isolation and consequent protection of the cohabitants. Nevertheless, during the quarantined period, she presented with a relapse of psychiatric symptoms with a rapid escalation of emotional dysregulation with extreme mood instability and reactivity. In the first month, she experienced only symptoms of frustration and physical concern for herself and her family. She reported that drug therapy probably helped her manage her mood and anxiety more than she expected. During the first month, she was able to sleep, organize time at home, and be productive. Her pharmacological therapy was not changed. After 1 month, however, and in the absence of clinical signs of COVID-19, the patient quickly began to worsen showing bipolar mixed features with agitation. She experienced frequent anxiety episodes with cardiorespiratory symptoms that often interfered with her sleep; she reported having suffered from initial and middle insomnia. She explained that her head was always full of thoughts and that she was unable to focus and engage in home activities. She started displaying marked affective lability, characterized by an unpredictable succession. For example, within a single day, she reported violent fits of crying, irritability, internal tension, and even episodes of verbal aggression against family members or against the doctors of the Hygiene and Public Health Unit.
Therapeutic Interventions, Follow-Up, and Outcomes
Telemedicine visits intensified, both in frequency and duration. Psychiatric visits increased from one evaluation carried out in the first month to five in the second month of quarantine.
At that point, a therapeutic modification was necessary. The authors opted for the addition of a mood stabilizer, valproic acid, and the involvement of the psychologist of the occupational team to start a psychological treatment. The referred psychologist adopted a cognitive-behavioral therapy (CBT) designed for crisis management based on week sessions (Lloyd et al., 2013). In particular, third-generation CBT such as Mindfulness and Acceptance and Commitment Therapy (ACT; Bond et al., 2006) have been integrated into the AOUP protocol to help the worker to embrace her thoughts and feelings, rather than fighting or feeling guilty for them. The therapeutic options proved to be effective and the patient experienced complete remission of acute mood symptoms.
Discussion
We have presented the case of a female nurse with a mood spectrum disorder who was already being followed by the multidisciplinary team of the Occupational Department of a Major University Hospital in central Italy with specific experience in work-related stress and emergency management. Upon the arrival of the pandemic, the patient presented high psychosocial COVID-19 risk factors related to both her professional role and her temperamental predisposition to mood disorders. In other words, her work exposures plus her mood disorder may have increased the risk of infection. A cohort study published in the Lancet in July 2020 found an increased risk for SARS-CoV-2 infection among HCWs compared with the general community. The review also reported that infections are mainly in women, especially nurses (Nguyen et al., 2020). Consistently, she tested positive in the first days of March, during the peak of the first wave when there was still a lack of information and inadequacy of personal equipment protection for health personnel. Another Lancet position paper published in November found that having a psychiatric history seems to be another independent risk factor for infection (Taquet et al., 2021). Possible explanations for the association include behavioral factors as well as lifestyle factors that are not sufficiently captured by the available data in any of the studies. Another possible explanation to the vulnerability to COVID-19 is the increased pro-inflammatory state postulated to occur in some forms of psychiatric disorder (Orsini et al., 2020; Smith et al., 2020; Taquet et al., 2021). Another important personal risk factor for psychological distress was the patient’s temperament. Some studies evidenced how cyclothymic/depressive individuals may be more likely to perceive the COVID-19 outbreak and related containment measures as distressful and to experience increased amitriptyline negative affect in response to social isolation (Moccia et al., 2020; Preti et al., 2020).
A further notable feature of this case study lies in the duration of the illness. After the infection, in fact, the nurse remained positive for more than 2 months and this led to a long quarantine. Some studies suggest that HCWs that are quarantined deserve special attention as they can be concerned about causing their workplaces to be understaffed resulting in extra work for their colleagues (Brooks et al., 2020). Other studies highlighted how HCWs quarantined versus those not quarantined were significantly more likely to report stigmatization and rejection from people in their local neighborhoods or led their families to consider their jobs to be too risky, creating intra-household tension (Desclaux et al., 2017; Ramaci et al., 2020). Evidence from the literature also showed that longer durations of quarantine were associated with poorer mental health, in particular, post-traumatic stress symptoms, avoidance behaviors, and anger. Although the duration of the quarantine was not always clear, one study from the SARS outbreak showed that those quarantined for more than 10 days presented significantly higher post-traumatic stress symptoms than those quarantined for less than 10 days (Desclaux et al., 2017). In this regard, we can hypothesize that the patient’s psychopathological worsening could be due both to her psychiatric predisposition for mood episodes and to the onset of post-traumatic symptoms during quarantine. Post-traumatic stress symptoms and mood spectrum symptoms could, in fact, be related to sequential causality, in which a mood disorder would occur secondarily to prolonged post-traumatic stress symptoms. Comorbidity of post-traumatic stress symptoms and depression has been documented in trauma-affected populations, with the extent of diagnostic overlap varying from 21% to 45% (Bryant, 2019; Carmassi et al., 2013; Flory & Yehuda, 2015; Hawryluck et al., 2004). Concurrently, the National Comorbidity Survey (NCS) data evidenced how almost 80% of traumatized individuals reported the onset of a mood disorder following post-traumatic symptoms (Carmassi et al., 2019; Kessler et al., 2005).
A final consideration is the question of which drug to use, having the least possible interactions with antivirals, antibiotics, and/or anti-inflammatories. The best choice seems to be drugs that do not act, or act very little, on cytochrome P450, and this is the reason why we opted for valproate as adjunct therapy (Orsini et al., 2020). In light of all these considerations, personalized monitoring of vulnerable HCWs during quarantine is a useful intervention measure to prevent adverse effects (Carmassi et al., 2021; Figueroa & Aguilera, 2020; Gómez-Durán et al., 2020). In this particular case, clear and rapid communication, through the use of visits in telepsychiatry with specialist intervention, allowed the team to manage the psychopathological worsening of the nurse.
Conclusion
This clinical experience has led us to consider the importance of multidisciplinary personalized occupational surveillance of vulnerable HCWs during quarantine, as quarantine can be an important mental distress trigger.
Footnotes
Acknowledgements
The authors thank Anand Saha for assistance with the English language review of this article.
Author Contributions
M.C. (Martina Corsi), R.B., A.V., S.B., and F.C. conceptualized, drafted, and critically reviewed the manuscript for important intellectual content; A.C., R.F., and G.G. coordinated the study, supervised data collection, and reviewed and revised the manuscript; E.D.L., M.C. (Martina Chiumiento), R.M., F.C., S.P., and G.N. collected data and critically reviewed the manuscript for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Approval
The collection of clinical data and the psychiatric and psychological intervention are part of a health surveillance program for hospital employees. The whole project is supported by the hospital management. The worker fulfilled a written informed consent regarding the case presentation and signed a publication consent.
Author Biographies
R. Buselli, MD, in Occupational Medicine at the Preventive Occupational Medicine Unit of Pisa University Hospital. Founder and coordinator of a group of specialists dealing with consultancy, assistance, and research in the field of psychosocial risks in occupational medicine at the University Hospital of Pisa. Main areas of interest in research are the diagnosis, pathophysiology, and prevention of psychic illnesses due to work-related stress and the management of workers with mental disabilities. Author of publications in national and international journals of Occupational Medicine and Psychiatry
M. Corsi, MD, psychiatrist at the Preventive Occupational Medicine Unit of Pisa University Hospital. Member of the Italian Society of Psychiatry. Expert in the field of neuroscience, neurobiology and clinical management of stress-related psychiatric disorders. Invited peer-reviewer for scientific journals and member of the Cochrane Review Group. Author of several publications in national and international journals.
A.Veltri, MD, PhD, psychiatrist at the Preventive Occupational Medicine Unit of Pisa University Hospital. Expert in the field of neuroscience, neurobiology and clinical management of stress-related psychiatric disorders. Author of several publications in national and international journals.
S.Baldanzi, M.Sc.,PhD, Psychologist at the Preventive Occupational Medicine Unit of Pisa University Hospital. Expert in the field of work-related stress and of mental disorders related to work organization dysfunctions. Author of publications in national and international journals.
M.Chiumiento, M.Sc., Psychologist at the Preventive Occupational Medicine Unit of Pisa University Hospital. Expert in the field of work-related stress and of mental disorders related to work organization dysfunctions. Author of publications in national and international journals.
E.Del Lupo, M.Sc., Psychologist. Author of publications in national and international journals.
R.Marino, MD, Research fellow at the Preventive Occupational Medicine Unit of Pisa University Hospital. Expert in the field of work-related injuries and illnesses with a particular focus on work-related stress. Member of the Italian Society of Occupational Medicine. Author of publications in national and international journals.
G.Necciari, MD, Resident at the Preventive Occupational Medicine Unit of Pisa University Hospital. Member of the Italian Society of Occupational Medicine. Author of publications in national and international journals.
F.Caldi, MD, in Occupational Medicine at the Preventive Occupational Medicine Unit of Pisa University Hospital. Member of the Training and Guidelines Commission of the Italian Society of Occupational Medicine. Author of several publications in national and international journals.
S.Perretta, MD, in Occupational Medicine at the Occupational Medicine Unit of Pisa University Hospital. Health surveillance activities for workers of Pisa University. Expert in the field of work-related injuries and illnesses. Member of the Italian Society of Occupational Medicine. Author of publications in national and international journals.
Rudy Foddis, MD, PhD, Associate Professor in Occupational Medicine at Pisa University Hospital. Professor of occupational medicine and industrial toxicology. Head of the health surveillance program ofPisa University. Member of the National Executive Council of the Italian Society of Occupational Medicine and Industrial Hygiene. Author of over 100 scientific articles mostly published in international scientific journals.
G.Guglielmi, MD, in Occupational Medicine. Acting Director of Division of Occupational & Preventive Medicine of Pisa University Hospital. Author of about 120 publications in national and international journals.
A.Cristaudo, MD, in Occupational Medicine. Former Full Professor of Occupational Medicine, University of Pisa. Coordinator of the Training and Guidelines Commission of the Italian Society of Occupational Medicine. Author of about 300 publications in national and international journals.