
Abstract
Background: Migrant and seasonal farmworkers (MSFW) experience disproportionate infection, severe disease and death from COVID-19. This report describes an innovative process to address the safety of MSFW that utilized cohorting that eventually allowed for safe release to work in the fields on a large family farm in Iowa. Methods: Upon worker departure from Mexico, the employer arranged for bus seat assignments, mask use, and hand hygiene practice during the 3-day trip to Iowa. Upon arrival at the farm, surveillance testing and low-density housing cohorting based upon travel seat assignments allowed for early identification of infected workers and appropriate quarantine as per CDC guidelines. Upon completion of isolation or quarantine as appropriate, workers were released to congregate housing and work in the fields. Findings: Compared to a migrant farmworker COVID-19 outbreak without travel pre-planning, the cohorting process produced a 3.5% positivity rate compared to an earlier season July farmworker group on the same farm with a 12.7% positivity rate. Conclusions/Application to Practice: The success of this model points to the power of collaboration between farm employer, health care providers and workers to minimize worker infection and enable safe work in the fields. Increased state and federal support for MSFW protections could support infrastructure to proactively plan for prevention mechanisms to prevent the spread of known communicable disease. With support in place from the top down, employers, workers, and health care providers will be able to prioritize the management of infectious diseases and the needs of essential workers.
Keywords
Background
Over the past year, the United States has yielded the highest number of COVID-19 infections (9,649 per 100,000) and one of the highest number of death rates (173 per 100,000) (Dong et al., 2020). As of May 7, 2021, the US has experienced over 32 million cases, including over 576 thousand deaths (COVID Data Tracker, 2021). During the early days and months of the pandemic there was a steady stream of lay media reports that focused on the disproportionate effect the pandemic was having on ethnic communities, including Latinx and Black communities in the US (Lai & Lin, 2020; Oppell et al., 2020a, 2020b). The migrant and seasonal farmworker (MSFW) community experienced high COVID-19 risk complicated by existing challenges related to structural and social determinants of health (Fan & Pena, 2021; Handal et al 2020; Lauzardo et al. 2021; Lewnard et al., 2021; Quandt et al., 2021; Ramos, 2018; Sattler, 2019). To date, over 480 thousand agricultural workers have been infected by COVID-19 across the country (Purdue University, n.d.); however, only 14 states have implemented farmworker protections during the pandemic (Berkowitz, 2020). As scientific data collection affirming the association between social determinants of health and COVID-19 risk accumulates, one could reasonably expect such an association based upon what we already understand regarding socio-economic risk factors and infectious disease, such as crowded, structurally deficient housing (Quandt et al., 2015) and underlying medical conditions (Butler-Jones & Wong, 2016). The MSFW experience during the pandemic is a stark example of this unfortunate paradigm (Culp & Umbarger, 2004). Often, workers live in poverty (Pulgar et al., 2016; Sandhaus, 1998), experience language barriers (Arcury et al., 2010), reside in inadequate housing (Levesque et al., 2012; Mora et al., 2016; Quandt et al., 2015), have poor access to health care (Frank et al., 2013), and now appear to be at heightened risk of COVID related mortality (Fielding-Miller et al., 2020).
The Iowa farm economy depends on the labor of seven to twelve thousand MSFW for soy, seed corn, vegetable, and livestock production every year. Many of these workers come to the state through the H-2A visa program. Workers under the H-2A visa program are uninsured and uninsurable and rely heavily on community health centers (CHCs) and federally qualified health centers (FQHCs) to address health needs. As in many other states, non-governmental and nonprofit organizations provide support for the migrant and seasonal farmworker population in Iowa. Corwin et. al (2021) reported on an early COVID-19 outbreak among farmworkers during the first summer of the pandemic, that was mitigated with support by Proteus, Inc., a federally qualified health center In Iowa (Proteus, Inc., nd). Later that summer, Proteus, Inc., developed an innovative practice adaptation to help mitigate COVID-19 transmission risk for a cohort of migrant farmworkers traveling from Mexico to Iowa for work. As workers boarded buses for travel to US work sites, seats were assigned on buses to the US, tracking close contacts and requiring masks at all times. This process was implemented during the late summer and fall and informed by the early season experience with migrant farmworker infection transmission on the same farm.
We present this practice adaptation as an example of effective collaboration between a farm employer of a migrant workforce and Proteus, a trusted health care provider of migrant workers. The purpose of this model was to reduce the number of infections of migrant farmworkers in communal living settings on a family-owned farm operation in Iowa as workers returned for harvest compared to positivity rates on this farm earlier in the season. Our hope is that the dissemination of this experience will encourage other farm employers and health care providers to develop similarly innovative solutions to minimize migrant and seasonal farmworker COVID-19 infection and disease during this pandemic as well during other potential public health emergencies.
Methods
At the beginning of the COVID-19 pandemic, there was little coordinated consensus on how to prevent or mitigate infection among essential workers who were unable to work from home or physically distance at work. There are significant challenges to developing infection prevention plans for MSFWs who travel, work, and live in congregate settings which prevent them from following many of the protective strategies recommended for others. In July of 2020, a family-owned farm operation in Iowa supported by H-2A visa workers experienced a 12.7% positivity rate during July 2020, with subsequent disease spread through the migrant camp. Following usual schedules, workers planned to return to Mexico for three weeks between detasseling and harvest periods. To better protect workers and reduce disease transmission in those returning for harvest in August and September, Proteus cohorted workers during travel back to Iowa as well as upon arrival while awaiting COVID-19 test results. Positive workers were isolated and close contacts were quarantined as necessary and received education and medical follow-up as appropriate. We describe the intervention of the cohorting process, population, health care provider, and data collection and analysis in detail below.
The Population
The workers involved in this practice adaptation are H-2A visa holders who travel to Iowa to perform farmwork. Like other H-2A visa holders working in Iowa, they remain in the state from three weeks to eight months to complete their contract. They travel to Iowa in vans or buses and live in communal settings on work sites. As part of the H-2A visa agreement, the agricultural employer provides housing and transportation to and from Mexico and while workers are in Iowa.
The Healthcare Provider
As a federally qualified health center (FQHC) and 501c3 non-profit organization, Proteus provides primary care and health education for migrant and seasonal farmworkers. Proteus has provided services to farmworkers in Iowa since 1979 and the Agricultural Health Program has provided health care to migrant and seasonal farmworkers in Iowa since 1991. Proteus operates mobile field clinics, providing bilingual and culturally responsive primary care to approximately 1500 migrant and seasonal farm workers annually. In Iowa, Nebraska, and Indiana, Proteus delivers health and safety training, job training, education support, and food or financial assistance. Proteus employs a clinical practice and educational model that acknowledges the influence of low wages, distance from family members, lack of access to health care, and literacy and language proficiencies of this worker population.
Typical Primary Care Practice and Practice Adaptation in Response to COVID-19 Pandemic
In a typical year in Iowa, upon arrival at the work site, Proteus staff offer primary health care for farmworkers and deliver training on heat stress and pesticide safety. Subsequently, they operate mobile clinics that provide regular weekly visits to registered patients while they remain in Iowa. Throughout the agricultural season, Proteus regularly reaches out to employers, recognizing the need for cooperation and collaboration with employers to keep workers safe and healthy.
In early 2020, Proteus proactively communicated with farm owners and managers about COVID-19 infection prevention and mitigation, providing education and guidance to prepare for the influx of H-2A visa workers. Proteus staff identified knowledge gaps among employers and collaborated with county and state public health and state agencies, to help lead pandemic response for both employers and MSFW as they arrived in the state. Response efforts included the organization of mass testing events, over 1800 COVID tests performed, provision of over 15,000 masks, delivery of sustenance support (food, water, hygiene products), and provision of temporary housing when needed.
As workers arrived in Iowa, Proteus held bilingual virtual “town halls” reaching across Iowa to discuss testing and infection prevention and handed out face masks as needed. As trusted sources of information and health care, Proteus team members provided education on COVID-19, mitigation and prevention strategies, and modeled testing in front of workers to encourage workers to get tested. In order to comply with social distancing guidelines, they conducted mobile clinics outdoors and developed telemedicine options including telephone visits for clinical encounters. When needed, providers offered in-person care the following day and medication delivery. Staff and patients used personal protective equipment (PPE) as appropriate and reinforced the need to follow CDC recommendations at all times.
Cohorting Intervention
During the summer of 2020, an outbreak within the migrant farmer population at a family-owned farm in Iowa revealed weaknesses in recommendations to address disease spread within H-2A visa workers living in communal living settings. Prior to starting work in the fields, the Iowa Department of Public Health COVID-19 tested 339 arriving H-2A visa workers and Proteus tested 251 H-2A visa workers at this farm. The workers lived in communal settings while they awaited test results (3 days, on average). The living space for the 590 workers consisted of a large, two story building with rows of bunk beds spaced six feet apart. Workers shared locker room style bathrooms and showers, ate meals in a large cafeteria, and rode buses to and from work sites. Masks were recommended when workers were unable to socially distance from others; however, they were not mandated. Once test results were available, workers were notified of their results by their employer and positive workers were moved to isolation in non-air-conditioned housing. Workers were provided with jugs of drinking water that passed water quality testing, but even then, many workers experienced diarrhea which contributed to dehydration. No clinical care was provided to positive workers unless Proteus has performed the test or the patient notified Proteus of their test results and illness. Infection transmission and illness burdened local rural EMS services as well as alarmed local hospitals and regional emergency management professionals, as the outbreak progressed. Over the course of July 2020, four workers were transported to a hospital emergency room. One worker was admitted while three workers were treated with IV hydration and nebulizer therapy and discharged from the emergency room.
In August of 2020, in anticipation of workers returning from Mexico, Proteus proposed a plan to state officials and state public health staff in order to reduce infection transmission during travel, upon arrival to the farm, and while awaiting initial on-arrival test results. Proteus used Coronavirus Aid, Relief, and Economic Security (CARES) funding to support and collaborate with the employer to execute the plan.
This innovative program tracked workers’ close contacts from their point of departure in Monterrey, Nuevo Leon, Mexico, to their arrival at the Iowa farm, supported workers who had tested positive as well as their close contacts during quarantine and isolation, and followed workers’ health after testing, with all workers eventually successfully released to work. The workers included in this pilot included two groups of H-2A visa workers returning to Iowa for fall harvest. The first group included 90 workers and the second group of 80 workers followed nine days later. Each group boarded two buses, and at the time of departure each worker was assigned a number. They were asked to remain in the same seat for the duration of the trip and masks were mandatory while on the bus. At the time of departure the plan for cohorting during travel and instructions regarding use of masks and hand sanitizer was communicated by the bus driver. The bus drivers were experienced farmworkers who had worked for the employer in the past and who had trusted relationships with the employer and the workers. Upon arrival at the farm 30 hours later, workers were cohorted into groups of two to five, based on proximity during travel. Cohorts were assigned to a local hotel room or to employer housing that consisted of isolated rooms or socially distanced pods within a large communal living building. Within 24 hours of arrival, Proteus conducted expedited polymerase chain reaction (PCR) testing through collaboration with the Iowa State Hygienic Laboratory. Once results were received, negative workers were released to work and housing in the communal facility on site. Positive workers were moved to employer-provided isolation housing for ten days, following CDC guidelines. Notification of positive result and medical evaluation was conducted by a provider during telehealth visits. Medication was prescribed, dispensed, and delivered by Proteus. Follow up telehealth visits occurred on day three and day seven of isolation. Close contacts of positives were quarantined in groups based on the described numbering system, assessed for symptoms at notification of exposure and three days after notification, and re-tested seven days after last known exposure. Those who tested negative on day seven were released from quarantine to communal living and work in the fields. Subsequent testing was performed based upon symptom development or exposure.
Close communication with the farm owner, while time consuming for health care providers, was essential to the success of this program. The process was presented to the employer during a video conference to discuss preparations for harvest. Proteus agreed to perform testing, cover the cost of hotel rooms to separate workers while awaiting test results, and provide follow-up and medications for workers. The employer agreed to provide food, water, and worker transportation to and from the hotel.
Data Collection and Analysis
Proteus collected numbers of positive and negative test results and identified close contacts of workers who received positive results using the assigned seating list. Proteus tracked telehealth and in-person visits with infected workers, COVID-19 specific education provided during visits, as well as visits by workers to emergency departments or other health care access. Positivity rate was calculated through use of the State Hygienic Lab reporting portal, Open Enterprise Laboratory Information System (ELIS), and hospital transfers were determined through internal chart review.
Results
At this farm, implementation of worker cohorts reduced the impact of COVID-19 on migrant farmworkers living and working in communal settings. In July of 2020, prior to implementation of the cohorting process, Proteus tested 251 workers at the farm. In those workers, thirty-two individuals tested positive (12.7% positivity rate). Four uninsured and uninsurable individuals eventually required hospital transfers. After implementation of the cohorting process, the positivity rate was 3.5%. Six of 170 workers tested positive. None required hospital transfers or admissions, reducing the impact on local hospitals and emergency medical services. In August, Proteus spent $8935 to support hotel housing for the intervention group. Assuming consistent positivity rates between two groups without intervention, the cohorting process prevented isolation of an estimated 21 workers that would have resulted in 1700 hours of lost work. Implementation of this process increased productivity and had a positive impact on the employer’s operation.
Discussion
Proteus’ experience on this large family farm in Iowa demonstrated the potential devastating impact that widespread infectious disease outbreaks could have on farmworkers and the Iowa economy. Without structured testing, quarantine, and isolation, a greater number of workers would have become infected, felt sick, and missed work. The process for cohorting workers during travel through release to work decreased the number of workers in isolation or quarantine. This translated as increased productivity with a positive impact on worker health, employer operations, and potentially the Iowa agricultural economy.
This innovative intervention of cohorting workers from the time of departure from Mexico through release to work in the fields was very resource intensive. The process required significant resources from the employer (buses, drivers, housing, hotels) and from Proteus (financial support for hotels and workers, clinical and staff support). Thus, while the model worked well for infection reduction on this farm, the entire process might not be easily used for other farms or larger migrant worker groups.
Nonetheless, this model (Figure 1) served as a valuable pilot process and presented multiple individual points at which the risk of infection for traveling workers could be mitigated. Certain steps may well be adaptable by many farms across Iowa and the country. For workers who travel to a single destination in groups, whether in a smaller sedan or via bus, requiring masking and handwashing would be fundamental measures. For those traveling several days via bus, numbering seats and cohorting workers during travel could enable contact tracing when a worker subsequently becomes symptomatic or receives a positive test result. Routine testing of workers upon arrival was not necessarily standard practice; however, this was an opportunity to identify infected workers very early during employment. This procedure could be enhanced by separating workers and housing them in low density living quarters until the receipt of test results were available. This would reduce the likelihood of disease spread in communal settings when workers needed to remove their masks during activities such as eating or showering. Once results were available, arrangements for isolation of positive workers could be implemented. Contact tracing could then be conducted to determine those workers who may need to quarantine. Initial separation of workers upon arrival may minimize the number of workers quarantined.
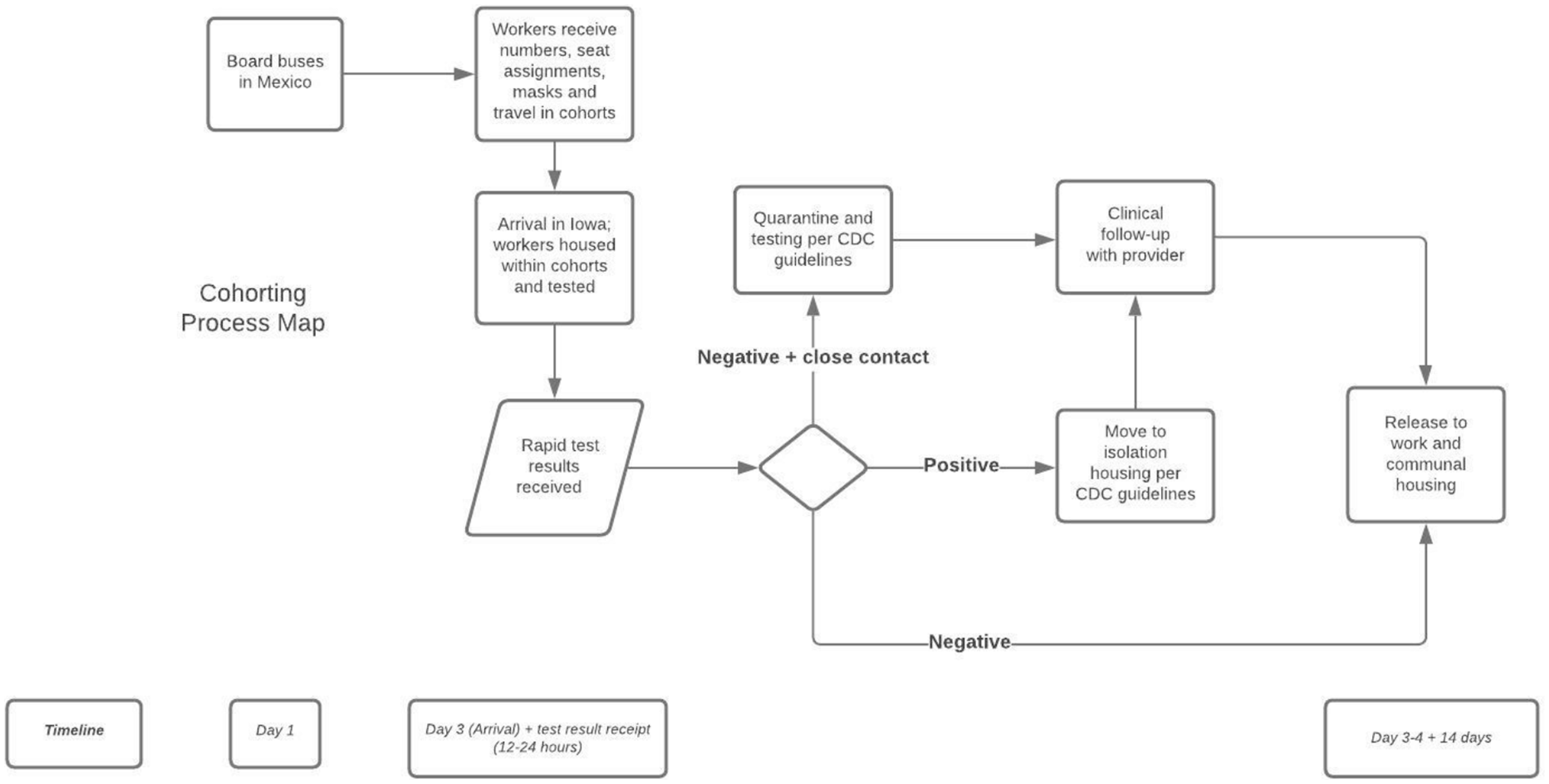
Cohorting process map—Timeline from boarding buses in Mexico to release to work.
The described model implemented initial cohorting of workers during travel who had unknown infectious status, as testing was only performed after travel and upon arrival at the destination. Point of departure testing would offer another opportunity to mitigate spread of infection. Rapid testing technology is evolving and may offer additional opportunities to reduce infection among mobile workers. Point of departure testing and point of departure health-related decision-making could be enabled by increased collaboration and coordination at the US-Mexico border for workers traveling from Mexico, as well as between state and local public health departments within the US. Creative partnerships could effectively tailor existing public health COVID-19 messaging to an audience of agricultural workers (Liebman et al., 2020). Further collaborations between public health and community health care providers such as migrant health clinics and FQHCs or other non-profits and stakeholders in agricultural health as well as with farm employers, could help pool and coordinate resources. This could promote a more comprehensive, feasible approach to mitigating infection risks for migrant workers who travel through distinct and often predictable migrant streams across the US. Finally, intra-state communication and information sharing between migrant health care providers and state entities, such as departments of public health, is critical. For example, barriers to sharing COVID-19 test results by public health officials with health care providers impeded expedient and often urgent clinical care for the individual and mitigation for co-workers on this farm. Beyond the unique circumstances of a pandemic, rapid point-of-departure testing, travel cohorting, and maximal organizational communication could help protect migrant workers during conditions of endemic disease transmission or epidemic infectious disease outbreaks.
Until very recently, there has been no coordinated federal or state pandemic response on behalf of vulnerable workers across the country. Early in the pandemic, MSFW employers and Proteus looked to state and local public health departments for guidelines in planning, preparation, and implementation of strategies to keep workers safe. Mask mandates only under specific conditions, mitigation strategies that were inconsistent with CDC evidence, and lack of planning for testing and contract tracing of Spanish speaking individuals in the state led to disease spread, hospitalization, lost wages for many, and long-term health complications for some. Although agricultural workers in Iowa are in one of the first tiers to be vaccinated, coordination between employers, FQHCs and local public health departments leading vaccine distribution has been challenging. The Biden administration recently enacted an executive order on protecting worker health and safety, placing a “special emphasis on communities hit hardest by the pandemic” (Biden & Presidential Executive Order, 2021) and shortly thereafter launched the Federally Qualified Health Center (FQHC) Program for COVID-19 Vaccination (White House, 2021). By mid-February, the first 250 FQHCs began directly receiving vaccine supply. In March, Proteus was named in the second cohort of FQHCs to receive direct allocation of vaccine. This strategy acknowledges that FQHCs serve almost 30 million people, most of whom live below the poverty line and are racial and/or ethnic minorities, and that local public health departments are not prepared to address the vaccination gaps in their communities. While these are positive signs for change, it is still uncertain as to what this will mean for the safety of MSFW across the country. Policy that prioritizes the health and safety of workers acknowledging the specific health disparities of the population is needed. Collaboration between employers and FQHCs, as well as local and state health departments, is essential to ensure quality care is being provided to prevent infection and death among this mobile and highly vulnerable population.
Applications to Professional Practice
H-2A visa migrant farmworkers, seasonal farmworkers and other mobile farmworkers who travel through the US to agricultural work sites may be at high risk for COVID-19 infection and transmission, both during travel and during US work periods. Given the urgent and changing nature of the pandemic, little is known about COVID-19 mitigation and infection prevention for these workers. Proteus developed and implemented an innovative program for migrant and seasonal farmworkers. The program assigned specific seating and hotel arrangements for workers traveling from Mexico to a US work site, tested workers for SARS-COV 2 on arrival, and housed positive and negative workers (and close contacts of positive workers) in cohorts to ensure appropriate testing, symptom monitoring, and isolation measures. This practice innovation helped reduce transmission, ensured follow-up for workers who had tested positive, and contributed to the safety of workers before and after arrival.
Footnotes
Acknowledgements
We wish to thank the farm employers for their willingness to collaborate to ensure the safety of workers. We also thank the workers who collaborate in their own health care and safety, and contribute such critical labor within the food system. We also acknowledge the many hours of hard work and crucial commitment on the part of health aides and other Proteus, Inc. staff throughout the year.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Johnson and Mr. Zinnel are paid employees of Proteus, Inc. Drs. Corwin and Sinnwell provide part-time clinical care for Proteus, Inc. Dr. Culp and Dr. Dukes declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Proteus receives federal funding through the United States Department of Health and Human Services, Bureau of Primary Health care including the following grants: H80CS00335—Migrant Health Program, H8DCS36287—Coronavirus Aid, Relief, and Economic Security Act (CARES Act), H8CCS34754—Coronavirus Preparedness and Response Supplemental Appropriations Act, and H8ECS38274—Expanding Capacity for Coronavirus Testing (ECT).
Author Biographies
Caroline Johnson is the Clinical Director and Nurse Practitioner at Proteus, a federally qualified health center serving agricultural workers and their families.
Kimberly Dukes is a medical anthropologist committed to health equity and health service research.
Emily Sinnwell is a dually certified Family Practice/Psychiatric Nurse Practitioner with over ten years providing care to migrant and seasonal farmworkers in Iowa.
Kennith Culp is an epidemiologist and interested in the protection of underserved workers. He has conducted farm related research over the last 20 years.
Daniel Zinnel serves as the CEO for Proteus, Inc., a federally qualified health center serving agricultural workers and their families.
Claudia Corwin is an occupational and environmental medicine physician who is committed to health equity and the care of people who fall into the porous health care safety net.