
Abstract
Background:
Long-term absenteeism continues to rise in Belgium and musculoskeletal disorders (MSDs) have been considered a primary cause. However, there is still uncertainty about the prevalence of MSDs, and about the contribution of work-related factors in the etiology of MSDs. SALTSA, which was developed in 2001, is a European diagnostic criterion document that aims to standardize the reporting of work-related upper limb MSDs (ULMSDs). The purpose of this work-site study was to implement SALTSA in daily occupational health practice and to determine the prevalence of ULMSDs in a Belgian company.
Methods:
During health examinations, occupational health nurses and an occupational health physician screened employees in a company with ergonomically high-risk activities for the occurrence of ULMSDs using the SALTSA protocol. In order to explore associations between ULMSDs and lifestyle and work-related factors, bivariate and logistic regression analyses were performed.
Findings:
Three hundred and eight (94.0%, 308/328) employees were screened resulting in an ULMSD prevalence of 20.5% (95% CI = [16.0–25.3]). Rotator cuff syndrome was the most common condition. Prevalence varied significantly between men (9.6%, 95% CI = [5.6–14.9]) and women (35.0%, 95% CI = [26.9–43.9]). Being female (p < .001) and working in the cabling assembly unit (p = .002) were found to be significant predictors of ULMSDs.
Conclusion/Application to Practice:
By using the SALTSA protocol in occupational health practices, ULMSDs can be screened unequivocally, enabling comparisons between different occupational sectors and countries. Occupational health nurses can play an important role in detecting and screening MSDs among workers.
Background
Absenteeism due to illness, especially long-term absenteeism (>1 year), continues to rise in Belgium (Verlinden, 2018). The main causes have been attributed to musculoskeletal disorders (MSDs) and psychosocial problems (Verlinden, 2018). In 2016, 40% of all sick days in Belgium were due to musculoskeletal complaints (Verlinden, 2018).
MSDs have a significant impact on a number of levels. They represent a professional expense for the employee whose career is interrupted by the incapacity for work. For a Belgian employer with 100 employees in 2016, the mean sickness costs (direct and indirect) due to absenteeism was over €500.000 ($539.15 USD) (Verlinden, 2018). There is also a considerable cost to society. According to the National Institute for Health and Disability Insurance (RIZIV), the disability benefit expenditure in Belgium rose by 25% between 2010 and 2014, resulting in a cost increase of 1 billion euros. The number of disabled people suffering from MSDs and mental health disorders has risen considerably by 81% and 45%, respectively, for younger employees between 25 and 34 years of age (RIZIV, n.d.). A major shift related to occupational diseases in Belgium has also been observed. In 2016, MSDs made up 77% of all recognized occupational diseases (Fedris, 2016). This trend was not unique to Belgium. MSDs are also the most common recognized occupational diseases in France, Italy, and Spain (Kok et al., 2019). Across Europe, there has been a growing concern about the occurrence of work-related MSDs. In 2015, the proportion of workers in the European Union (EU) reporting MSD complaints was 58%. These proportions varied considerably between Member States, 62%, 40%, and 75% for Belgium, Hungary and France, respectively. The true extent of the costs and burdens associated with MSDs is difficult to assess and compare at EU level (Kok et al., 2019). It was estimated that in 2007 the total cost of lost productivity attributable to MSDs among people of working age in the EU could be as high as 2% of the gross domestic product (GDP) (Bevan, 2015).
The etiology of MSDs is multifactorial, with work-related factors often playing a significant role (Descatha et al., 2020). More analysis is still needed though to better explore the nature of the interrelationships between MSDs and the psychosocial and biomechanical risk factors (Kok et al., 2019). Also, the extent of work-related MSDs remains unclear as there is presently no gold standard available for occupational health surveillance for diagnosing MSDs. A number of studies describe a high prevalence of MSDs in various occupational groups (Epstein et al., 2018; Erick & Smith, 2011; Nørgaard Remmen et al., 2020; Osborne et al., 2012). Due to methodological challenges such as choice of case definitions and diagnostic criteria, it is difficult to compare MSD prevalence in different countries and economic sectors. To meet this need, a group of European experts published SALTSA (Sluiter et al., 2001) in 2001, a diagnostic criterion document aimed at standardizing data reporting on upper limb MSDs (ULMSD) in the EU. Surveillance of work-related ULMSDs by occupational health physicians (OHP) using the SALTSA protocol was applied first in 2002 in France in the Pays de la Loire study (Ha et al., 2009; Melchior et al., 2006; Roquelaure et al., 2006). Such an approach of the SALTSA protocol by an occupational health service in Belgium has not yet been described in literature.
The purpose of this work-site study was to (a) implement the SALTSA protocol into daily occupational health practice, (b) determine the prevalence of ULMSDs in a Belgian company with an ergonomically high-risk occupational activity, (i.e., high repetitiveness and/or extreme posture of neck, shoulder, elbow or wrist), and (c) explore associations of ULMSDs with lifestyle and work-related risk factors.
SALTSA Diagnostic Criteria for Upper Limb MSDs
SALTSA is a criterion document that seeks to facilitate a more uniform collection, recording and reporting of information about work-related ULMSDs in the EU. It provides evidence- or consensus-based diagnostic criteria and case definitions for 11 specific ULMSDs such as carpal tunnel syndrome, rotator cuff syndrome, epicondylitis, as well as criteria to determine their work-relatedness (Sluiter et al., 2001). This document was drawn up by the Coronel Institute for Labor and Health (Amsterdam) on behalf of the European SALTSA program. Adjustments were made by the Institut National de Recherche et de Sécurité (INRS) in order to improve its practical feasibility (Aublet-Cuvelier et al., 2010). The criterion document is designed primarily for OHPs. It may also be useful to other health professionals including occupational health nurses (OHN), general practice and primary care physicians, physiotherapists and ergonomists.
Workplace health surveillance activities for work-related ULMSDs are often based on symptoms only, since medical examinations by an OHP are not always realistic or affordable. Therefore, this document provides surveillance case definitions and criteria based on symptoms alone. If resources permit and medical examinations might also be done, this would provide additional information on diagnostic signs. Physical examinations may be particularly important for high-risk groups as work-related ULMSDs may be more likely to occur in these workers. Considering different surveillance resources, the criterion document describes two case definitions for each specific ULMSD: one case definition based on symptoms only (the symptomatic case definition) and one based on both symptoms and signs (the sign or clinical case definition).
Diagrams included in Supplemental Figure 1 provide a visual aid to the decision process that occurs when criteria are applied to the case definitions. Symptoms in a certain body region form the entry point of each diagram for the symptomatic case definition. The symptom criteria should be checked one by one. When the criteria for the symptomatic case definition are met, a physical examination may reveal positive signs that fulfill the clinical case definition for that disorder. A symptomatic case is the entry marker to the flow diagram for this second case definition. As the diagram shows, both case definitions include temporal criteria: symptoms must be present now or for at least 4 days during the last 7 days or be present at least 4 days during at least 1 week over the last 12 months. In certain cases, symptoms may be present but do not meet the temporal criteria: these symptoms lead to a latent symptom case. When ULMSDs cannot be classified into specific diagnostic categories they are identified as non-specific or are considered as a “deviant case.”
Methods
The study took place in a microelectronics company that manufactured microscopes. There were 13 different job roles in the company, of which administration, quality control, cabling assembly, cabling and electrical technician were the job roles employing most of the workers. The work tasks in this company are considered ergonomic high-risk activities. For example electronic quality control requires dexterity, precision and rigor. Electrical technician uses small electrical tools, soldering iron and manual tools. Cabling and cabling assembly consists of wiring and assembly and requires dexterity and manual handling of loads. This study was carried out from February to December 2017 by an OHP and a team of OHNs of Mensura, a leading Occupational Health Service in Belgium. Employees were informed by the employer about the purpose of the study. They were asked to give their written informed consent.
ULMSD screening took place during the workers’ mandatory periodic health assessments, which comprised health history conducted by the OHN followed by a physical examination by the OHP (20 minutes each). During the consultation with the OHN, data were collected on lifestyle factors, work-related stress and the occurrence of musculoskeletal symptoms. Rating of lifestyle factors was assessed using single-item questions. Smoking status (smoker, non-smoker) was assessed and self-reported sleep quality was coded as poor if the employee answered positive to the question “Do you experience sleeping problems more than once a week?” Self-reported overall general health was rated positive if the employee answered yes to the question “Do you experience a good overall general health?” Physical activity was assessed by the question “On average, how many minutes per day and how many days per week do you dedicate to physical activity?” This was asked for moderate physical activity like walking or cycling, as well as for intensive physical activity like running, tennis, soccer, and swimming. According to the World Health Organization (WHO, 2010) guidelines, sufficient physical activity was defined as an average of at least 150 minutes of moderate intensity endurance activity or at least 75 minutes of sustained intensity endurance activity per week. Finally, body mass index (BMI) was calculated based on weight and length measured during the physical examination, formula BMI = weight (kg) /height (m)2. Rating of work-related stress (stress level minus ability to manage stress level) was assessed by the following questions, “In general, how do you rate your stress level in your work situation?” and “How do you rate your own ability to manage this stress?” The answers were scored on a scale from 1 (very low) to 5 (very high). The difference between the score on the stress level and the score on the ability to manage the stress level is used to assess the relative level of stress with values that could range between -4 and 4, with a higher score indicating a higher relative stress level.
Symptoms of ULMSD were assessed using the Nordic Musculoskeletal Questionnaire (NMQ) (Kuorinka et al., 1987). This questionnaire included a body chart divided into 7 body regions including neck, upper back, shoulder, elbow, forearm, wrist and hand. The question “Have you experienced a problem (pain, discomfort or tension) in the past year or last week?” was asked by the OHN for each region. Employees who reported pain in the NMQ over the past year underwent a standardized physical examination by the OHP. In accordance with the case definitions in the SALTA criterion document, the OHP categorized the symptoms as latent, clinical, or symptomatic. The OHP only considered a diagnosis for symptoms that met the SALTSA clinical case definition. Consequently, employees were referred to health professionals for clinical intervention.
In preparation for the implementation of the SALTSA protocol at Mensura, both the OHN and OHP completed training. OHN’s were trained in administering the NMQ. The OHP participated in a 3-day training course on the standardized physical examination at the INRS. In this study, the criterion document was not used to determine the work-relatedness of the ULMSD symptoms since this was not the main aim of our study. Instead, associations between ULMSDs and work-related risk factors like job role and work-related stress and between ULMSDs and lifestyle factors were explored.
Data Analysis
Descriptive analyses were carried out for the registered ULMSDs symptoms, work-related risk factors and lifestyle factors. Prevalence of ULMSDs was calculated by dividing the number of employees with at least one ULMSD by the total number of examined employees. In order to explore associations between ULMSDs, lifestyle and work-related risk factors, bivariate analyses were carried out using chi-square tests for categorical variables and t-test for continuous variables. A multivariate logistic regression model was constructed with job role as explanatory independent variable, controlling for gender. Odds ratios and 95% confidence intervals (CIs) were calculated. Analyses were performed in SPSS 24.0 (SPSS Inc., Chicago, IL, USA).
Results
Of the 328 employees working at the microelectronics company, 308 (94.0%) (average age 39.8 years; SD 11.4 years) participated in the study (Table 1). All were examined, including 177 (57.5%) men (average age 39.5; SD 10.1) and 131 (42.5%) women (average age 40.2; SD 12.3). Two-hundred and twenty six employees (73.4%) were on permanent contracts, 71 (23.0%) were temporary workers and 11 (3.6%) were subcontractors. A total of 191 ULMSD symptoms were registered, of which 106 (55.5%) were specific and 85 (44.5%) were non-specific ULMSD symptoms. Of the specific ULMSD symptoms, 84 (79.2%) met the clinical case definition, 9 (8.5%) met the symptomatic case definition and 13 (12.3%) the latent case definition.
Occupational and Demographic Characteristics of Microelectronics Workers, Prevalence of Upper Limb Musculoskeletal Disorders (n = 308) and Occurrence of Upper Limb Musculoskeletal Symptoms (n = 191)
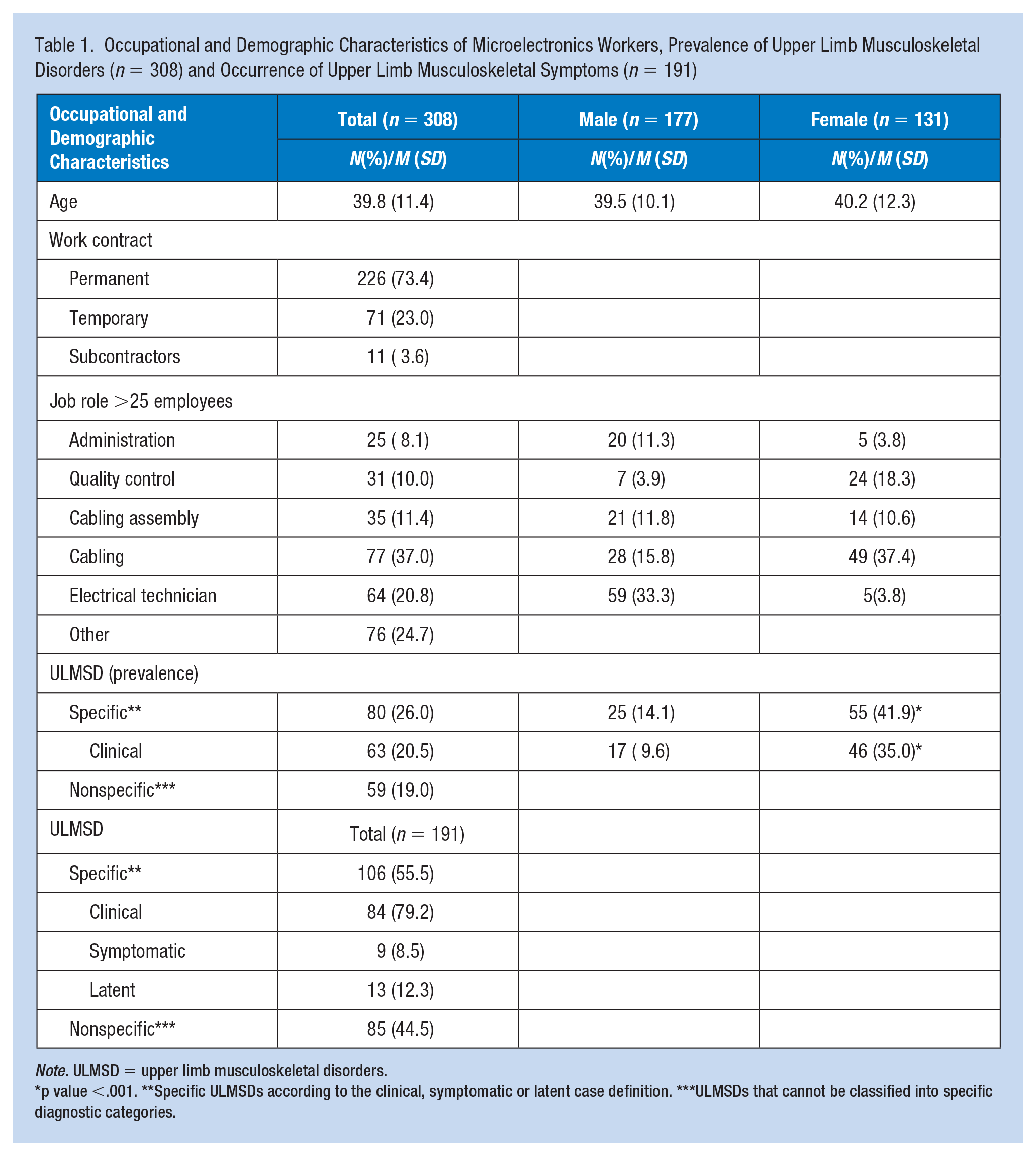
Note. ULMSD = upper limb musculoskeletal disorders.
p value <.001. **Specific ULMSDs according to the clinical, symptomatic or latent case definition. ***ULMSDs that cannot be classified into specific diagnostic categories.
Almost half (45.0%) of the employees reported at least one ULMSD symptom, non-specific or specific. Eighty (26.0%) employees experienced at least one specific ULMSD symptom of which 58 employees (72.5%) had one ULMSD, 18 employees (22.5%) had two ULMSDs and 4 employees (5.0%) had three ULMSDs. The prevalence of specific ULMSDs that met the clinical case definition was 20.5% (63/308), 95% CI = [16.0–25.3].
Specific ULMSD symptoms were distributed among 25 (14.1%) men and 55 (41.9%) women. Prevalence of specific ULMSDs that met the clinical case definition was 9.6% (17/177), 95% CI = [5.6–14.9] for men and 35.0% (46/131), 95% CI = [26.9–43.9] for women. The difference in prevalence between men and women was statistically significant (p < .001).
Rotator cuff and cervicalgia with radiation were the most diagnosed ULMSDs among women while epicondylitis was the most prevalent ULMSD among men (Figure 1).
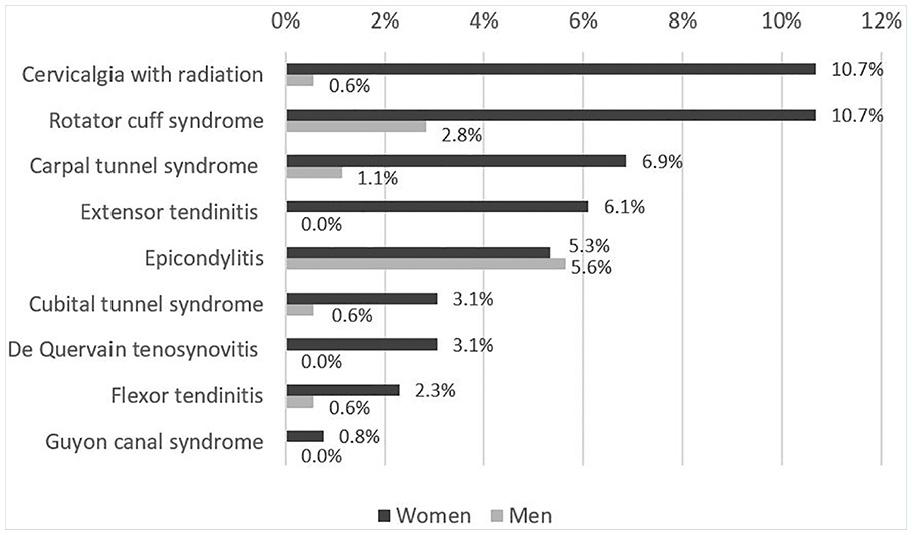
Occurrence* of specific upper limb musculoskeletal disorders according to the clinical case definition by gender (n = 177 and n = 131 for men and women, respectively).
The relative frequency of specific ULMSDs symptoms was higher for two specific job roles, cabling assembly and quality control compared to the company overall, which is the 13 job roles combined resp. 71.4%, 48.8%, and 34.4% (Table 2). With regard to the specific ULMSD symptoms, rotator cuff syndrome (19.4%) and cervicalgia with radiation (12.9%) were distinctly present in the quality control job role. Carpal tunnel syndrome (20.0%), epicondylitis (17.1%), extensor tendonitis (14.3%), and cubital tunnel syndrome (8.6%) were the four most common ULMSDs for the cabling assembly job role.
Frequency of Specific Upper Limb Musculoskeletal Disorders (Latent, Symptomatic or Clinical) Overall and by Job Role Among Microelectronics Workers (n = 308)
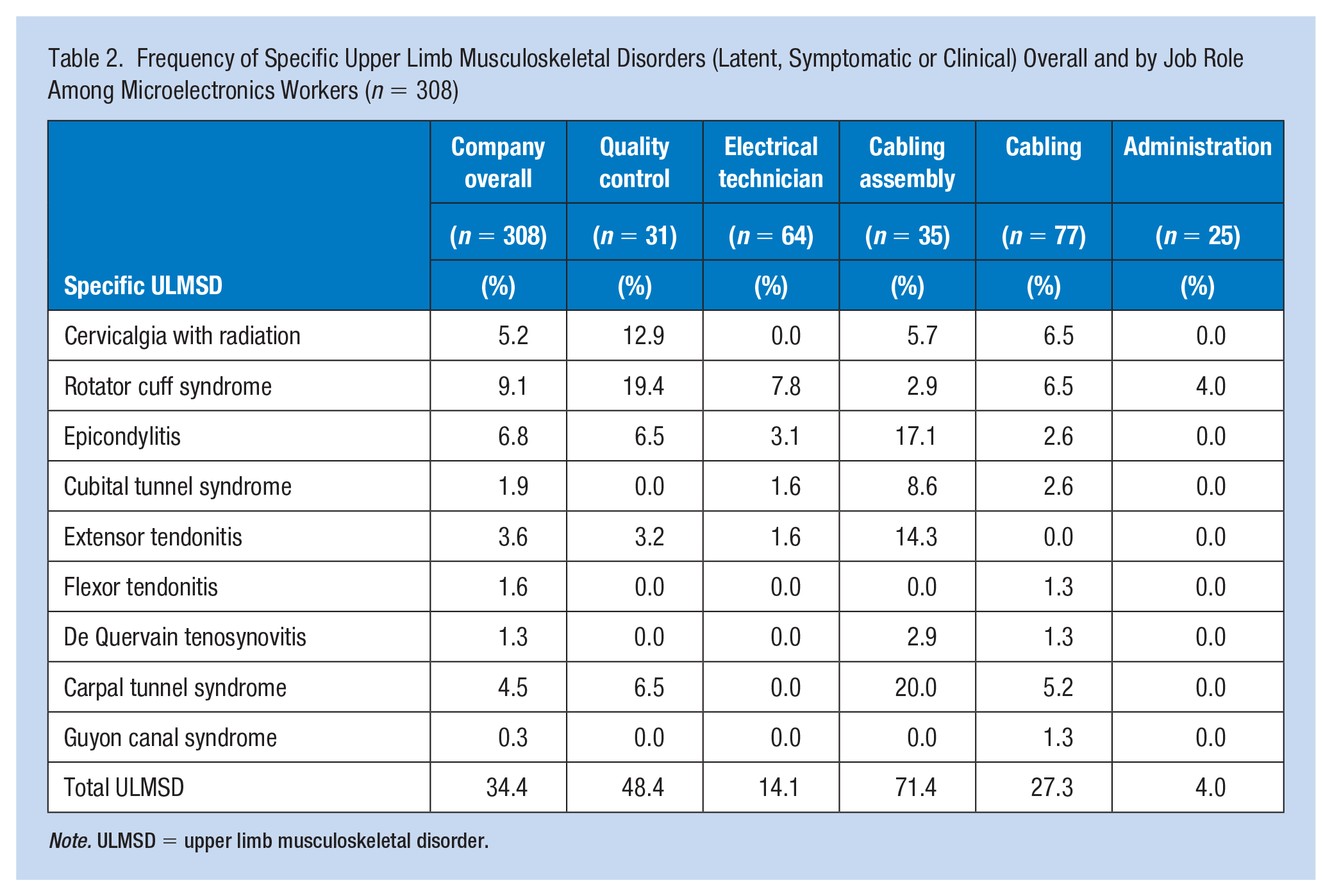
Note. ULMSD = upper limb musculoskeletal disorder.
A statistically significant association was found between specific ULMSDs and self-reported sleep quality and between specific ULMSDs and self-reported overall general health status (p = .004, p = .001 respectively) (Table 3). In addition, bivariate analyses showed a statistically significant association between work-related stress and specific ULMSDs (p < .001).
Bivariate Analysis Between Specific Upper Limb Musculoskeletal Disorders, Lifestyle Factors and Work-Related Stress Among Microelectronics Workers (n = 308)
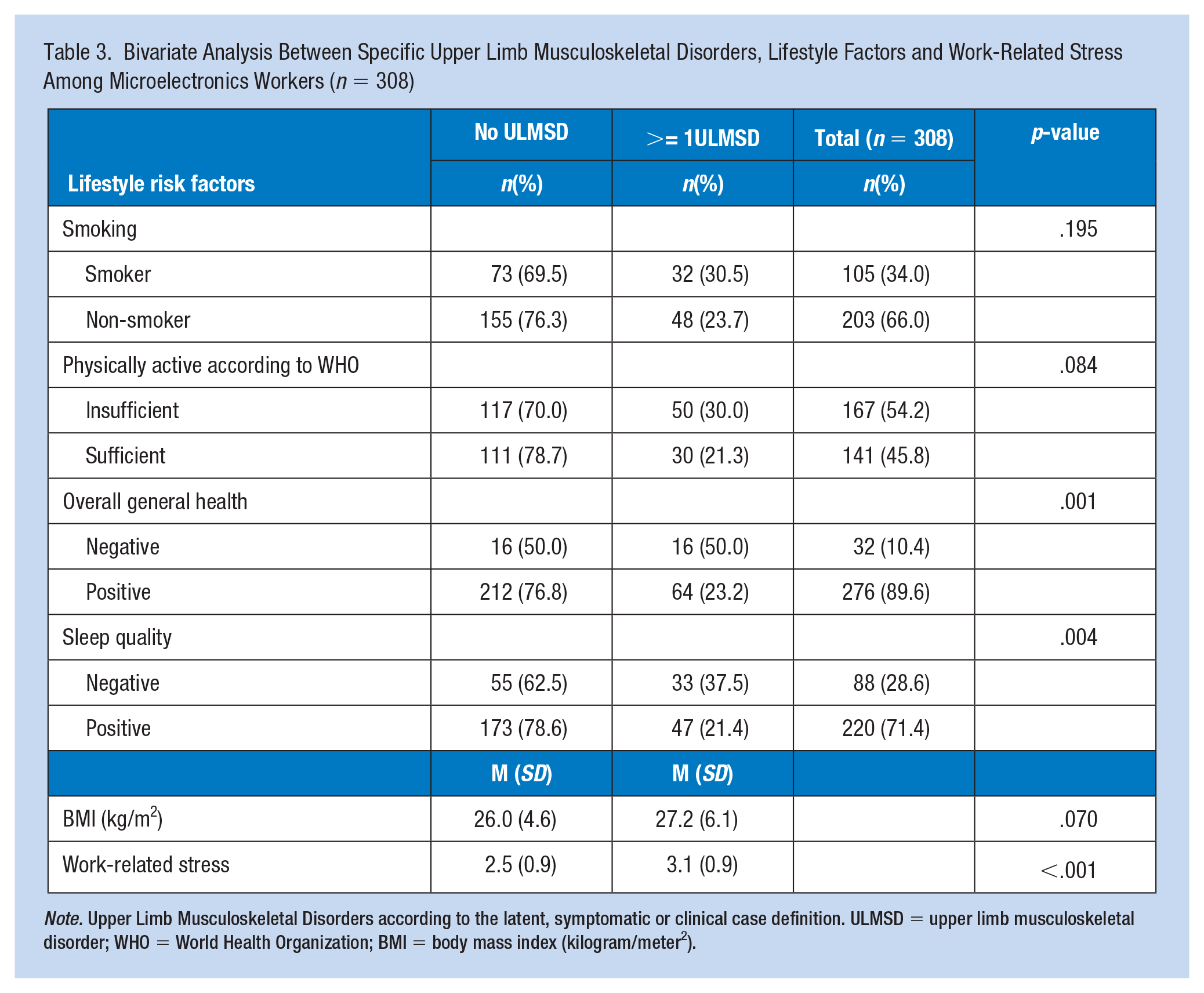
Note. Upper Limb Musculoskeletal Disorders according to the latent, symptomatic or clinical case definition. ULMSD = upper limb musculoskeletal disorder; WHO = World Health Organization; BMI = body mass index (kilogram/meter2).
We estimated an unadjusted OR for the two jobs roles of quality control and cabling assembling each compared to the other 12 job roles combined as reference group (Table 4). Unadjusted logistic regression analysis showed that the occurrence of specific ULMSDs was significantly associated with being female (ORunadj = 4.4, 95% CI = [2.5–7.6]), as well as with working in the cabling assembly job role (ORunadj = 3.1, 95% CI = [1.5–6.5]), but not with working in the quality control job role (ORunadj = 1.7, 95% CI = [0.8–3.6]). The findings remained approximately the same in the adjusted multivariate logistic regression model with an elevated odds of specific ULMSDs for gender (ORadj = 4.1, 95% CI = [2.3–7.1]) and cabling assembly job role (ORadj = 2.7, 95% CI = [1.3–5.9]), but with no elevation for quality control job role (ORadj = 1.2, 95% CI = [0.5–2.8]).
Logistic Regression Analysis for Specific Upper Limb Musculoskeletal Disorders Among Microelectronics Workers (n = 308)
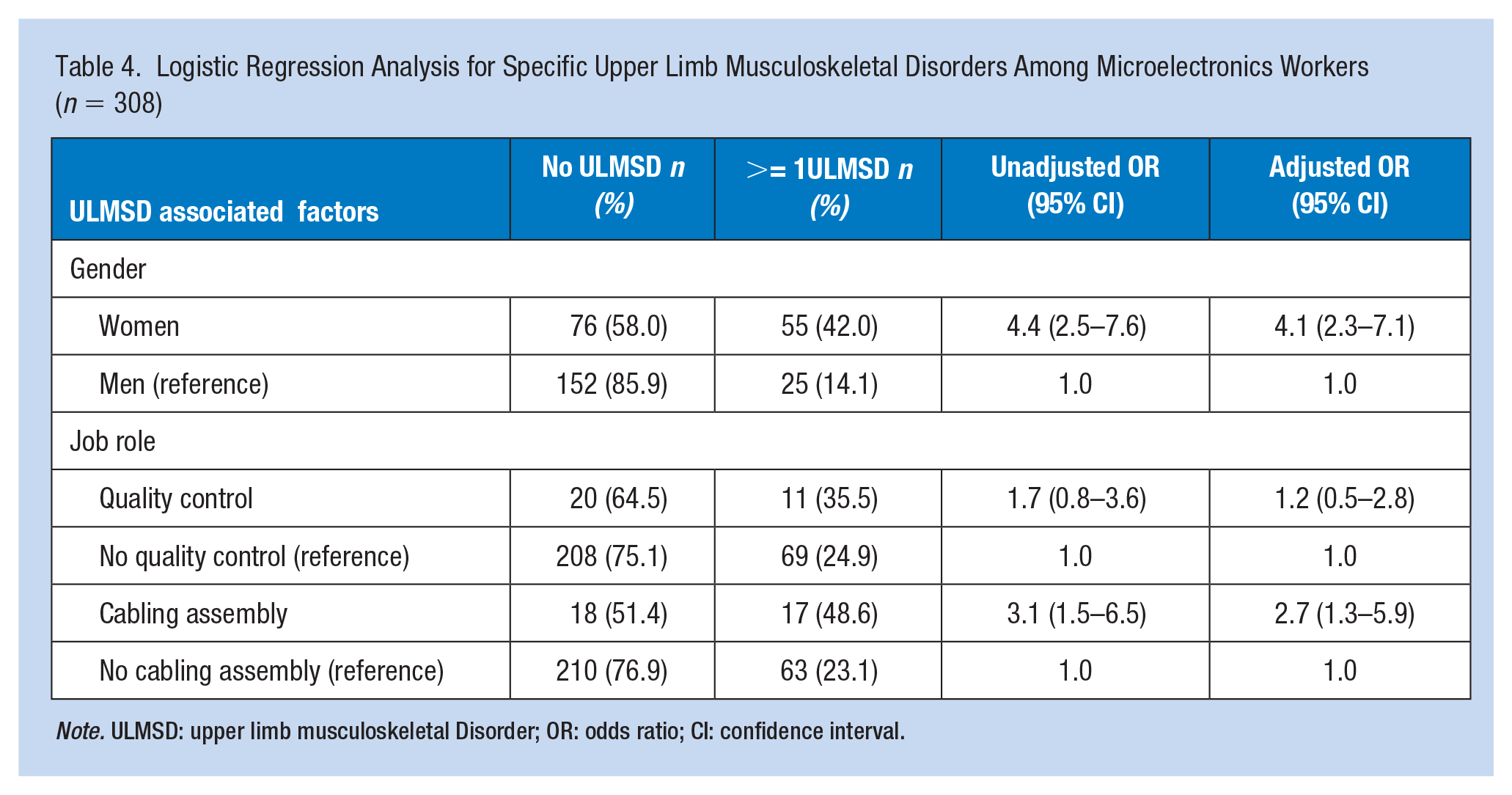
Note. ULMSD: upper limb musculoskeletal Disorder; OR: odds ratio; CI: confidence interval.
Discussion
Almost half of the employees in this Belgian company reported non-specific or specific ULMSD symptoms. Specific ULMSDs that met the clinical case definition occurred in one-fifth of the participants. Rotator cuff syndrome was the most common condition, followed by epicondylitis and cervicalgia radiation. Carpal tunnel syndrome followed in fourth place. In the Pays de la Loire study, more than 50% of the employees experienced non-specific symptoms and a prevalence of 13.0% (341/2685) was found for specific clinical ULMSDs (Roquelaure et al., 2006). Rotator cuff syndrome, carpal tunnel syndrome and epicondylitis were also the most common disorders in the Pays de la Loire study. It was possible that we found a higher prevalence of specific clinical ULMSDs during our study due to the fact that we screened in a high-risk occupational group, while the Pays de la Loire study included various economic sectors.
Another difference with the Pays de la Loire study concerned the comparison of prevalence between men and women. In our study, 35.0% of women and 9.6% of men experienced at least one specific ULMSD that met the clinical case definition. In de Pays de la Loire study this was 11.0% of men and 15.0% of women. In our study, the prevalence of ULMSDs in women was significantly higher than in men.
We explored the work-relatedness of symptoms by looking at the occurrence of ULMSDs for each job role. After multivariate logistic regression, cabling assembly proved to be a significant predictor of ULMSDs. This suggested that the ULMSDs were work-related. Our results also suggested a link between specific ULMSDs and work-related stress as psychosocial factor.
We also found a statistically significant association between ULMSDs and two lifestyle factors: self-reported sleep quality and self-reported overall general health. This was probably “reversed causation” as it was plausible that experiencing ULMSD symptoms led to reduced sleep quality. Likewise, overall general health status may be assessed more negatively when suffering from ULMSD symptoms.
The SALTSA protocol was effective and practical in detecting ULMSDs in an occupational health service. Although the use of symptomatic case definition was sufficient in occupational medicine, physical examination of clinical signs could offer added value when screening high-risk occupational groups. In addition, the application of the SALTSA protocol was practically feasible. The health assessment by the OHN and OHP took 40 min total time, which was a common amount of time in a Belgian occupational health practice.
It is expected that the prevalence of ULMSDs will rise in the future due to the aging population, more intense working conditions and longer working lives. It is therefore recommended that future studies, as well as the occupational health services, use consistently unequivocal diagnostic criteria for screening ULMSDs in the working population. Prevention of ULMSDs is clearly one of the major challenges for occupational health services, with a focus on a global approach based on biomechanical and psychosocial factors. This universal method of assessment may improve validity and facilitate comparison between different professional sectors.
Applying Research to Occupational Health Practice
Occupational health nurses and an occupational medicine physician screened employees with ergonomically high-risk occupational activities in a Belgian company during their regular periodical health examination. The prevalence of upper limb MSDs was determined using the SALTSA protocol, a European diagnostic criteria document. The result was an ULMSDs prevalence of 20.5%. Rotator cuff syndrome, epicondylitis, cervicalgia with radiation, and carpal tunnel syndrome were the most common conditions. The prevalence varied significantly between men and women (9.6% and 35.0%, respectively, p < .001). Based on multivariate logistic regression, being female and the cabling assembly job role proved to be statistically significant predictors of upper limb MSDs, with a p-value of p <.001, p = .002 respectively. By using the SALTSA protocol in occupational health practices, ULMSDs can be screened unequivocally in different occupational sectors and countries. The occupational health nurse was ideally suited to play a prominent role in the screening of ULMSDs with a focus on a global approach based on biomechanical and psychosocial factors.
Supplemental Material
sj-docx-1-whs-10.1177_21650799211019432 – Supplemental material for Screening of Work-Related Musculoskeletal Upper Limb Disorders Using the SALTSA Protocol: A Work-Site Study in Belgium
Supplemental material, sj-docx-1-whs-10.1177_21650799211019432 for Screening of Work-Related Musculoskeletal Upper Limb Disorders Using the SALTSA Protocol: A Work-Site Study in Belgium by Lieve Van Dyck, Monique Baecke, Marie Grosjean, Habyalimana Isaie, Yannick Gregoire, Christine Barbieux, Ryan Tock and Mathieu Verbrugghe in Workplace Health & Safety
Footnotes
Acknowledgements
We thank all participating workers.
Author Contributions
Mathieu Verbrugghe: design of the work, data analysis, interpretation of the data, revision of the article; Monique Baecke: conception and design of the work, data collection, drafting of the work; Marie Grosjean: drafting of the work, design of the work, interpretation of the data, revision of the article; Habyalimana Isaie: data collection, approval of article; Yannick Gregoire: data collection, approval of article; Christine Barbieux: data collection, approval of article; Ryan Tock: data collection, approval of article; Lieve Van Dyck: data analysis, interpretation of the data, writing of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics committee
As this study was carried out during the statutory periodic medical examinations by an occupational health service, it was not submitted to an ethics committee. Informed consent was obtained from the employees.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.