
Abstract
Background:
Burnout is a common phenomenon among health care providers known to adversely affect their mental health and clinical acumen. As mindfulness has been shown to diminish burnout with large-scale interventions, our aim was to assess whether smaller, on-shift activities aimed at increasing mindfulness could decrease burnout among staff in a pediatric emergency department (PED).
Methods:
Prior to the implementation of a series of mindfulness-based activities, a diverse cohort of PED staff including nurses, physicians, nurse practitioners, technicians, and administrative personnel completed electronic preintervention surveys about their demographics, personal mindfulness engagement, and individual baseline burnout level using the Maslach Burnout Inventory (MBI). Trained nurses and physicians served as champions who coordinated on-shift mindfulness activities, and burnout levels were subsequently reassessed using a postintervention survey.
Findings:
Among 83 eligible staff, 75 completed the preintervention and 69 completed the postintervention survey. For the MBI, the majority of staff had moderate to high burnout levels at baseline. Few staff engaged in personal mindfulness activities outside of work. Although 82% of staff participated in the on-shift interventions, no significant differences were found in scores before and after the intervention for emotional exhaustion (20.1 vs. 20, p = .93), depersonalization (7.6 vs. 7.3, p = .97), and personal accomplishment (36.1 vs. 34.8, p = .11).
Conclusion/Application to Practice:
While mindfulness effectively combats burnout, few PED providers regularly practice mindfulness activities. Brief, on-shift mindfulness activities were insufficient to significantly reduce burnout levels. Hospital leadership should consider dedicating resources to more intensive mindfulness activities to combat amplified burnout levels among emergency department staff.
Background
Burnout is increasingly recognized as an urgent issue due to the negative sequelae on provider well-being and its detrimental effect on patient care (Bragard et al., 2015; Westphal et al., 2015). According to Maslach et al, burnout has three key dimensions: emotional exhaustion (EE), depersonalization (DP), and a low level of personal accomplishment (PA; Maslach et al., 2001). National surveys estimate nearly half of the physicians meet criteria for burnout (Shanafelt et al., 2012; Westphal et al., 2015), and 40% to 44% of the emergency nurses experience high levels of the various subcategories of burnout (Li et al., 2018). Symptoms of burnout include physical exhaustion, cynicism, poor work performance, and poor interpersonal relationships with coworkers or patients (Arora et al., 2013). Burnout is associated with diminished professionalism, decreased quality of care, and increased errors (Shanafelt et al., 2010).
Pediatric emergency medicine providers are routinely exposed to severe occupational stress, including patient death, predisposing them to elevated risk of burnout (Arora et al., 2013; Bragard et al., 2015; Wilson et al., 2017). Research has focused primarily on burnout among physicians, (Gorelick et al., 2016; Patterson, 2017) or nurses (Pradas-Hernandez et al., 2018) rather than across a variety of roles within a pediatric emergency department (PED). Furthermore, many studies assess workplace or demographic risk factors (Escriba-Aguir et al., 2006; Potter, 2006; Schooley et al., 2016; Tarcan et al., 2017), but not personal mindfulness engagement to explain variations in burnout.
Mindfulness is defined as paying attention purposefully and nonjudgmentally to what is occurring in the present moment (Callahan et al., 2018; Kabat-Zinn et al., 1985). While mindfulness-based interventions have been shown to decrease burnout (Westphal et al., 2015), little is known about the personal mindfulness practices of PED staff. Furthermore, mindfulness interventions with documented success for health care providers are often time and resource intensive (Kriakous et al., 2020), so there is a need for innovative ways to implement mindfulness exercises to a diverse group of PED providers in a meaningful way. The aim of this study was to explore the relationship between current mindfulness-based practices and degree of burnout among PED staff. In addition, we aimed to measure the effectiveness of short, on-shift, mindfulness-based interventions on burnout among PED staff.
Methods
A single-arm preintervention and postintervention study was conducted from October 2017 to January 2018 in an urban, tertiary care PED. An anonymous electronic survey was distributed via email to all 83 assigned PED staff including nurses, physicians, nurse practitioners, technicians, and administrative personnel; per diem staff were excluded. Participants enrolled on a voluntary basis and completed the Maslach Burnout Inventory for Human Services Survey (MBI-HSS) for Medical Personnel, before and after the 3 months of on-shift mindfulness activities. The MBI-HSS is a licensed tool to measure burnout for health care providers (Vanheule et al., 2007), which has demonstrated both reliability and validity among health care workers (Maslach & Jackson, 1996).
Workers were also asked to provide demographic information including age, gender, role within the PED, years worked, length of service in PED, and self-reported levels of burnout, which was collected before the intervention. Participation in personal mindfulness activities was measured at baseline including mindfulness, breathing exercises, meditation, yoga/stretching, and relaxation techniques. Frequency of participation was measured as (a) never, (b) once a month or less, (c) few times a month, (d) few times a week, and (e) daily. Similar to other studies which showed positive effects on burnout, our intervention occurred for 3 months (Goyal et al., 2014; Johnson et al., 2015). At the end of the 3-month period, staff were asked to report their frequency of participation with on-shift mindfulness activities. Workers were then assessed for their level of burnout at the end of the 3-month intervention period.
The MBI-HSS for Medical Personnel is a 22-item inventory that uses a 7-point frequency scale ranging from never to daily to assess its three subscales: EE, DP, and PA (Maslach & Jackson, 1996). The MBI-HSS categorizes levels of burnout as high, moderate, or low for each of the three subscales. High EE score (≥27), high DP score (≥13), and low PA score (<31) are associated with burnout.
Mindfulness interventions
Focus group meetings with a hospital-based wellness expert and PED staff identified interventions most likely to be efficiently employed in the PED and have a high impact on staff. After meeting with the wellness expert, a group of three physicians and three nurses who worked in the PED were trained to be mindfulness champions and led short, on-shift activities with any available staff on shift in the PED over a 3-month period. Given the high acuity and large volume of patients, as well as the rapidly changing nature of the emergency department (ED) environment, short activities were chosen to facilitate participation during shifts as longer duration activities are not feasible. These included dedicated time for body scanning and stretching during morning huddles, gratitude affirmation practices using sticky notes on the PED bulletin board to express something one felt grateful for, spontaneous candy handouts with suggestions to “savor sweet moments” several times a week, and a dedicated mindfulness space available 24/7 that staff was alerted to by email and by the PED mindfulness champions. On-demand meditation was available by phone such that staff on any shift could access an activity if a champion was not present. Any PED staff on shift at the time (typically between five and 15) participated voluntarily in up to 20 of these brief 1- to 3-minute guided mindfulness activities.
Data Analysis
Sociodemographic data, participation in mindfulness activities, and degrees of burnout in each of the three domains were summarized using descriptive statistics, expressed as frequencies, medians with interquartile ranges (IQRs), means, and standard deviations (SDs). Associations between burnout levels, self-reported mindfulness practices, burnout perceptions, and demographic factors were examined using ordinal logistic regression models adjusting for interactions between gender and role and reported as odds ratios (ORs) and 95% confidence intervals (CIs). Associations between frequency of reported participation in on-shift mindfulness intervention from PED staff and burnout levels were assessed. To evaluate the effectiveness of our mindfulness intervention on burnout levels, Wilcoxon rank sum test was performed. For all analyses, a value ofp < .05 was considered statistically significant.
Findings
Among 83 eligible staff members, 75 (90% response rate) completed the preintervention survey and 69 (83% response rate) completed the postintervention survey. The majority of participants were women (77%) and non-Hispanic White (77%), with a median age of 35 years (IQR: 30–46; Table 1).
Pediatric Emergency Department Participant Demographics (N = 75)
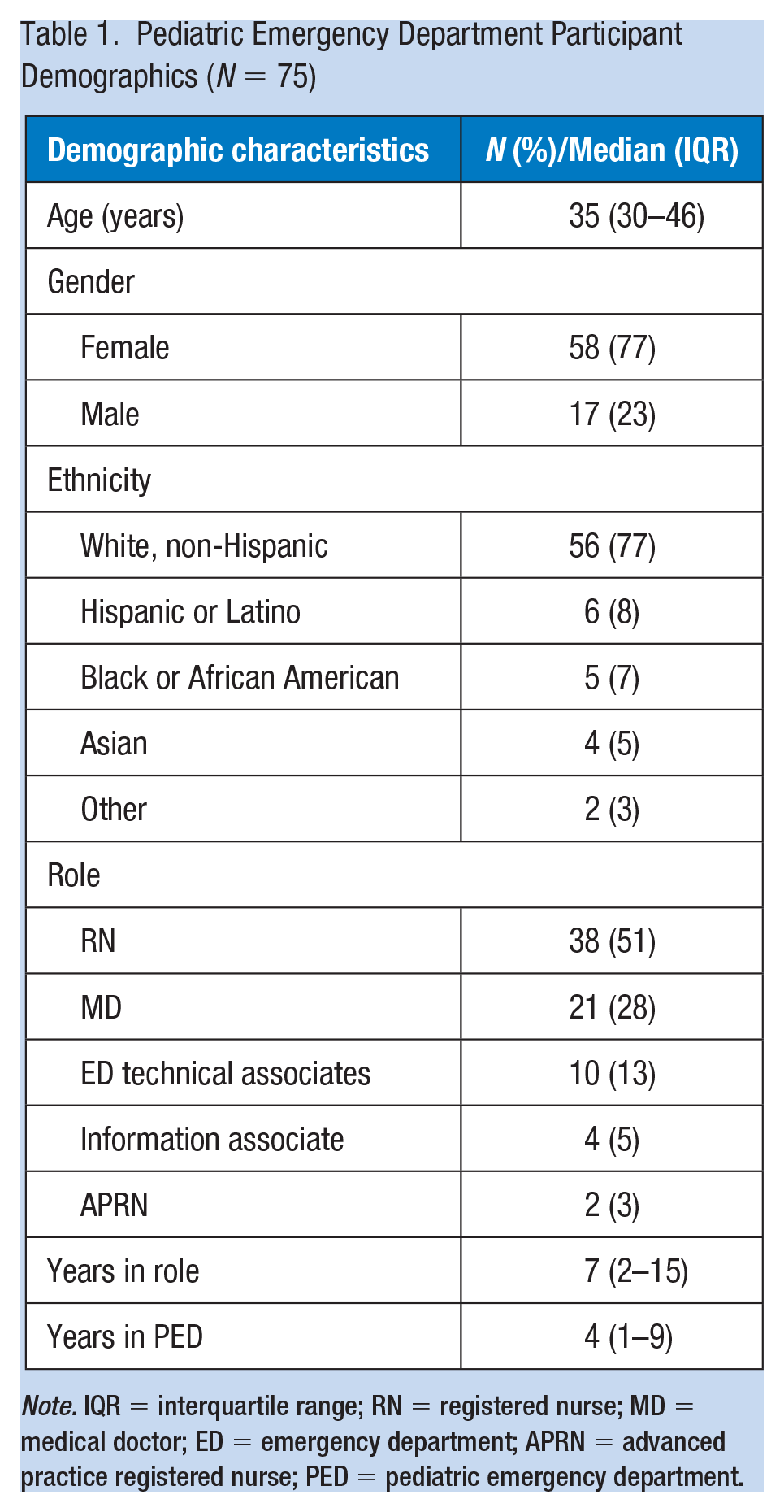
Note. IQR = interquartile range; RN = registered nurse; MD = medical doctor; ED = emergency department; APRN = advanced practice registered nurse; PED = pediatric emergency department.
The majority of participants were nurses (registered nurse [RN]; 51%), followed by medical doctors (MDs; 28%), ED technical associates (13%), information associates (5%), and advanced practice registered nurses (APRNs; 3%). Emergency department technical associates, information associates, and APRNs were combined into the category “other” in further analysis, given their small numbers. Overall, the three groups were similar in terms of the median total years worked in their roles (MD: 8 years, RN: 12 years, Other: 7 years, p = .15), median years worked in PED (MD: 9 years, RN: 6 years, Other: 5 years, p = .24), or age (MD: 40 years, RN: 37 years, Other: 36 years, p = .45). There were no differences in burnout among the different professional groups.
Frequency of staff participation in PED mindfulness interventions is reported in Table 2. Eighty-two percent of staff participated overall: 23% participated several times per week, 12% participated weekly, and 30% only participated monthly. Overall, self-reported participation in mindfulness activities was low during the preintervention; 61% reported never practicing mindfulness, and in follow-up questions, workers also reported never practicing yoga (51%), meditation (77%), breathing exercises (57%), or even general relaxation techniques (41%). However, up to 18% of the participants reported participation in mindfulness activities a few times a week or daily with the most popular activity being relaxation techniques. There were no associations found between any demographic variable and participation in personal mindfulness activities.
Frequency of Participation Among PED Staff in Mindfulness Activities in Personal Life and During Guided On-Shift Exercises
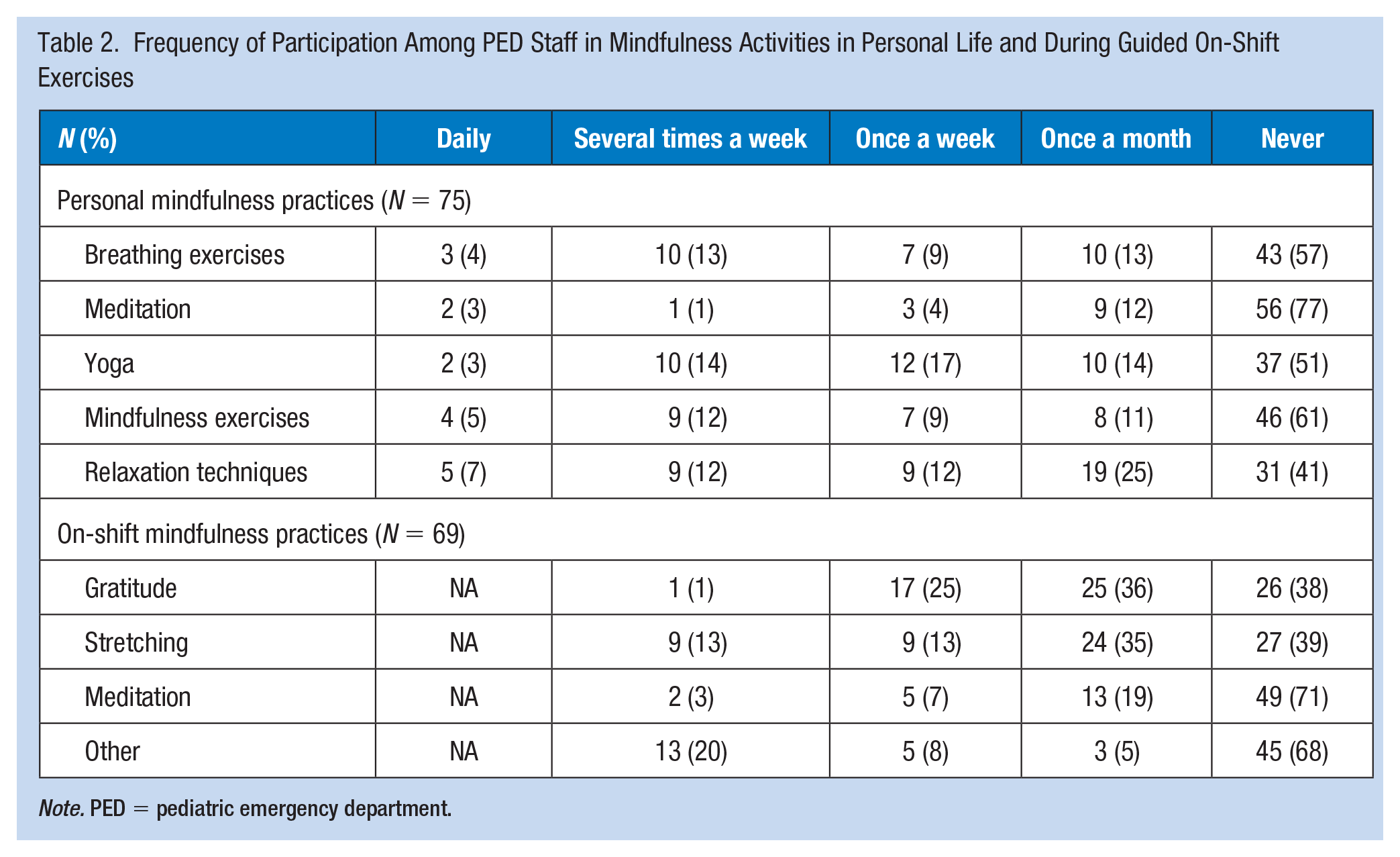
Note. PED = pediatric emergency department.
Frequencies of different levels of MBI scores for all participants are shown in Table 3. Prevalence of burnout manifestations subjectively and within the three subscales was high. Several demographic characteristics seemed to portend a higher risk for burnout. After adjusting for professional role, women had significantly higher levels of EE (OR: 7, 95% CI = [1.6, 30.6]) and lower levels of PA (OR: 3.4, 95% CI = [1.01, 11.3]) compared with men at the start of the study. More cumulative years worked in PED also seemed to carry a higher risk of EE (OR: 1.3, 95% CI = [1.1, 1.5]) at the start of the study. Workers who worked in their respective role for increasing number of years demonstrated lower levels of PA preintervention (OR: 0.84, 95% CI = [0.73, 0.97]) as well as postintervention (OR: 0.82, 95% CI = [0.69, 0.97]).
Frequency of Different Levels of Burnout Across all Groups Between Pre- and Post-Mindfulness Interventions Among PED Participants (N = 69)
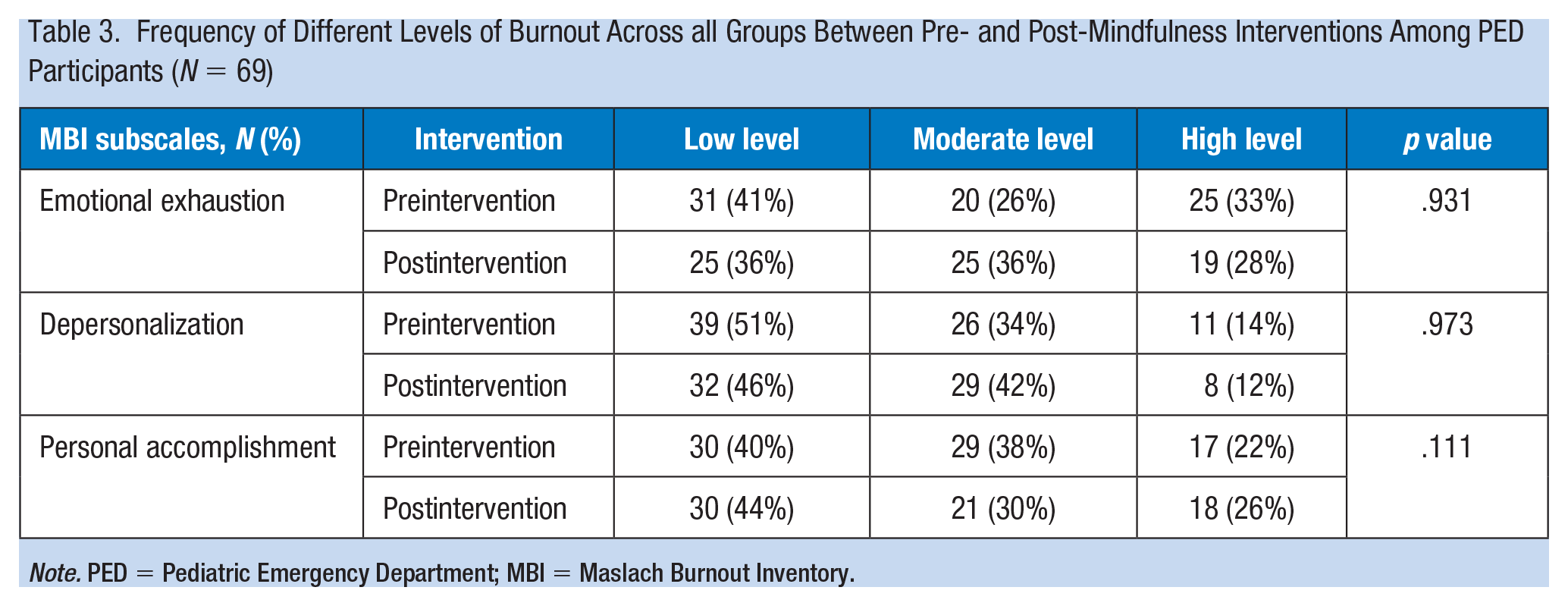
Note. PED = Pediatric Emergency Department; MBI = Maslach Burnout Inventory.
Prior to our intervention, the mean EE score was 20 (SD: 12.2), DP score was 7.3 (SD: 5.7), and PA score was 34.8 (SD: 10.4; data not shown). Among the small proportion of staff who participated in personal mindfulness practices, they did not demonstrate significantly lower burnout levels. Staff members with perceived burnout were less likely to ever participate in any mindfulness intervention (OR: 22.6, 95% CI = [10.8, 47.3]). After our intervention, the mean EE score was 20.1 (SD: 11.8), DP score was 7.6 (SD: 5.1), and PA score was 36.1 (SD: 7.8). There were no significant differences found in MBI levels before and after the on-shift mindfulness intervention.
Discussion
These results support prior studies showing high burnout rates in EDs, and further demonstrate that professionals across all roles suffer from burnout (Bragard et al., 2015; Gorelick et al., 2016). Overall, MBI scores among the PED staff showed greater similarities to those of general EM staff but were higher than for general pediatric staff, pointing to the unique stresses found in the ED (Gomez-Urquiza et al., 2017; Jacobs et al., 2012; Wilson et al., 2017). Despite this, personal mindfulness practices are not incorporated by individuals to combat the risk that burnout poses to provider and patient well-being. Unfortunately, exposure to targeted mindfulness interventions was insufficient to significantly affect the level of burnout among these providers.
While prior work has varied concerning whether differences in MBI scores exist among providers of various roles (Escriba-Aguir et al., 2006; Marques et al., 2018; Schooley et al., 2016), our results indicate no significant difference among burnout by role. There are similar inconsistencies in the literature regarding the effect of gender on burnout (Kawamura et al., 2018; Schooley et al., 2016; Soltanifar et al., 2018; West et al., 2018; Wilson et al., 2017), though we found significantly higher levels of EE and lower levels of PA among women. Among our sample, there were higher EE levels and lower PA levels associated with increasing number of years of experience. In contrast, other studies have found years of experience to be a protective factor (Kawamura et al., 2018; Shanafelt et al., 2012; West et al., 2018).
A unique barrier that could explain our results is that our population was much more varied than that in studies with documented decreases in burnout. Our intervention was targeted broadly; any of the 80+ medical professionals in the PED were invited to join in different mindfulness activities. Many mindfulness-based, highly effective interventions like the Mindfulness-Based Stress Reduction program are time intensive—2.5-hour practice sessions weekly for 8 weeks, a full-day retreat, and recommended 45 minutes of meditating daily (Gilmartin et al., 2017; Kabat-Zinn, 1982; Lomas et al., 2018)—and thus, participation at a unit level would be challenging. Modified, shorter programs have also had some effect on burnout, (Fortney et al., 2013; West et al., 2018), but our smaller program, though targeted, may not have reached the threshold to effect significant change. Furthermore, prior studies had dedicated treatment groups between 12 and 30 and targeted professionals in one particular role (Cohen-Katz et al., 2005; dos Santos et al., 2016; Fortney et al., 2013). The lack of significant change in burnout in our population may reflect the difficulty of engaging a larger, broader range of people in a consistent and meaningful way, given the time constraints of many ED providers both at work and when at home. Furthermore, several prior studies illuminated confounding variables that could also play a role in perpetuating burnout that mindfulness may not effectively combat. Work–family conflict, low exercise levels, job dissatisfaction, and alcohol consumption correlated with higher levels of burnout (Arora et al., 2013; Goldberg et al., 1996), whereas resilience, economic well-being, being married, and overall job satisfaction appear to be protective (Arora et al., 2013; Goldberg et al., 1996; Harker et al., 2016; Shanafelt et al., 2012; Tarcan et al., 2017). Controlling for these in our interventions could have yielded more significant results.
This was a single-center study, and therefore, its generalizability is limited. While overall 82% of staff members participated in the mindfulness activities, almost half reported that they participated once weekly or less, and one third only participated monthly; participants were not asked about their degree of engagement with the interventions, which could have also varied. Probable reasons include varying shift times of individual staff members, patient care demands, or personal preferences. Staff may have also exhibited recall bias in their estimations of mindfulness participation both before and during the study. Interestingly, staff who had perceived burnout were also less likely to participate, which may indicate general fatigue in work-related tasks. Given the small changes seen in some prior studies, we may have also been underpowered to detect this change, despite our high rate of engagement of unit staff members.
Implications for Occupational Health Practice
Overall, burnout is a significant problem in the PED across roles, genders, and years of experience. Unfortunately, few PED providers in our study were engaged in mindfulness activities, and targeted, brief, on-shift interventions were likely not intensive enough to create meaningful shifts in overall burnout levels across a diverse group of providers. Occupational health leadership trying to support staff suffering from burnout should consider either investing in the more intensive mindfulness-based interventions or helping staff cultivate mindfulness skills that they can integrate into their personal routines, as our study showed that very few staff engaged in mindfulness outside of work. Future interventions also could specifically target those staff members in the higher risk groups, engaging motivated individuals, having more frequently scheduled mindfulness activities, or continuing the current mindfulness intervention for a longer period of time.
Applying Research to Occupational Health Practice
This research illustrates that across all types of health care workers in this pediatric emergency department (PED), burnout levels were significantly elevated, and most personnel did not practice mindfulness activities, which have been shown to decrease this burnout. While lengthy mindfulness training sessions can be effective in lowering occupational burnout, this study showed that smaller, on-shift activities that may be easier for PED leaders to implement were not sufficient to alter staff’s burnout levels. This suggests that to appropriately address the burnout that affects health professionals’ ability to care for themselves and their patients, institutions may need to invest more significantly in burnout-combating initiatives. Especially during this current pandemic as emergency department personnel are stretched to unprecedented limits, having frequent conversations about mental well-being and taking tangible steps to support mindfulness practices are paramount.
Footnotes
Acknowledgements
The authors would like to graciously acknowledge the staff of the Yale New Haven Children’s Hospital Emergency Department who participated, the nursing leadership who assisted in the on-shift mindfulness exercises, and the Yale Employee & Family Resource Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kei U. Wong, MD, is an assistant professor of emergency medicine in the Division of Pediatric Emergency Medicine at Rutgers University New Jersey Medical School.
Lauren Palladino, MD, is a first-year Pediatric Emergency Medicine and Global Health Fellow at Children’s Hospital of Philadelphia.
Melissa L. Langhan, MD, MHS, is an attending physician in the Yale New Haven Children’s Emergency Department, and also acts as the Pediatric Emergency Medicine Fellowship Program Director and PED Director of Operations.