
Abstract
Background:
Professional bus drivers report a high prevalence of upper quadrant musculoskeletal pain which could be associated with scapular dyskinesis (SD). However, the evidence for valid and reliable screening methods for this condition is limited as SD among bus drivers is an emerging area of research. Therefore, the main aim of the study was to investigate the reliability of dynamic scapular motion test (DSMT) using video analysis as an accurate method to evaluate SD and to identify patterns of SD among bus drivers.
Methods:
In total, 32 bus drivers from a private bus company with unilateral upper quadrant musculoskeletal pain participated in the study. The DSMT was conducted and the SD was captured in the video during shoulder flexion–abduction movements. Two investigators analyzed the video recordings and identified the patterns of SD. The intra- and interrater reliability were determined using the percentage of agreement and weighted Kappa coefficients (Kw). Descriptive analysis was used to examine the patterns of SD.
Findings:
The intra- and interrater reliability of DSMT using video analysis were excellent (Kw coefficient: 0.762–0.878 and 0.87–1.00, respectively). About 56.2% and 53.1% of bus drivers presented SD with the shoulder flexion and abduction movements during DSMT. Medial border prominence (Type II pattern of SD) was identified as the common pattern of SD.
Conclusion/Application to practice:
The DSMT using video analysis showed excellent intra- and interrater reliability to evaluate SD. Occupational health practitioners can consider DSMT using video analysis to identify SD among people with upper quadrant musculoskeletal pain at the workplace.
Background
Scapular dyskinesis (SD) is a condition characterized by abnormal dynamic scapular control during shoulder movements and functional tasks (Burn et al., 2016). The scapula plays an important role in the upper quadrant region which involves the shoulder complex joints and cervical spine (Cools et al., 2014). The position and motor control of the scapula contributes to both mobility and stability of the neck and shoulder region (Cools et al., 2014). In clinical practice, the SD is identified by the presence of the prominence of the border of scapula which includes superior, medial, or inferior borders, and loss of scapula control during the bi-planar arm movements (Huang et al., 2015; Maor et al., 2017). Current clinical evidence suggests a strong relationship between SD with chronic neck and shoulder pain (Hickey et al., 2018; Kibler et al., 2013). A recent meta-analysis reported that individuals with SD had 43% greater risk of developing shoulder pain than those without SD (Hickey et al., 2018). Therefore, the clinical identification and therapeutic management of SD is important for the rehabilitation of individuals with chronic upper quadrant musculoskeletal pain (Panagiotopoulos & Crowther, 2019).
Occupations such as professional bus driving involve repetitive neck and shoulder movements (Rugbeer et al., 2016). The occupational tasks of bus drivers are stressful and have changed little over the decades (Golinko et al., 2020). It demands significant repetitive actions on the upper quadrant joints such as bending arms to control steering and frequent twisting of neck which can cause musculoskeletal stress to neck and shoulder regions resulting in significant occupational health hazards to the bus drivers (Golinko et al., 2020). A recent literature review found that a high prevalence of upper quadrant musculoskeletal pain in the neck (42.4%) and shoulder (39.2%) regions, respectively, among professional bus drivers was higher than the global 12-month prevalence of shoulder pain in the general public (36.7%) (Joseph et al., 2020). This finding along with other studies indicated that professional bus drivers are at a high risk of developing upper quadrant musculoskeletal pain (Geete et al., 2013; Joseph et al., 2020). However, to date, no studies have investigated the patterns of SD among professional bus drivers.
There are three different types of scapular examination techniques to detect SD, namely, observation, semi-dynamic examination, and dynamic examination (Kibler et al., 2002; Uhl et al., 2009). The observation test involves visual evaluation and measurement of scapular displacement from the trunk. However, it is highly challenging to observe the motions of the scapula beneath the muscle and overlying soft tissues. The semi-dynamic test involves static evaluation of scapula in a fixed plane of movement, but it provides only a static assessment of scapula position at one point in space. Therefore, the current recommendation for clinical assessment of SD advocates the use of dynamic scapular motion test (DSMT; Kibler et al., 2013). However, the reliability of the DSMT has not been tested in the population of professional bus drivers. Most of the evidence on DSMT to date has been with athletes with no reported studies examining SD among bus drivers’ population using DSMT. Thus, the reliability of the DSMT had to be established prior to the application of this test to investigate the patterns of SD among the bus drivers. Therefore, the main aims of the study were (a) to investigate the intra- and interrater reliability of the DSMT and (b) to investigate the patterns of SD among professional bus drivers with unilateral upper quadrant musculoskeletal pain.
Methods
The sample for this study consisted of bus drivers who were recruited from one bus company in Thailand. The bus company was randomly selected from a pool of three bus companies which had participated in the Sustained Model of Assessment and Rehabilitation Training (SMART) Drive project (Apirati et al., 2021; Joseph et al., 2020). Bus drivers were recruited through an approved advertisement displayed at the bus depot. Eligibility criteria included presence of unilateral upper quadrant pain for the past 12 months, at least a year working 5 or more hours per day as a full-time professional bus driver and working for a minimum of 5 days per week. The exclusion criteria included history of any injuries to the upper extremity that prevented them from working, bilateral upper quadrant musculoskeletal pain, and inability to perform shoulder flexion and abduction more than 120 degrees. The bus drivers who participated in the study were driving both automatic buses and buses with gears, and used both types of buses interchangeably. The drivers worked in different routes as per their duty schedule and usually operated without a bus conductor. The study was conducted in the natural work setting of drivers in the bus depot during the period between August 2019 and August 2020. All participants received information about the study and signed the written informed consent forms before the commencement of the study. The study was approved by the Human Experimental Committee, Faculty of Associated Medical Sciences, Chiang Mai University, Thailand (Ethical Approval Number: AMSEC-62EX-007).
Participant Characteristics
Demographic characteristics including age in years, height in inches, and weight in pounds were collected using a self-administered questionnaire. Similarly, characteristics including daily driving duration (in hours), daily driving distance (in miles), and number of years’ experience were collected on the questionnaire. The Numerical Rating Scale (NRS), a commonly used and broadly validated tool, was used to measure the intensity of pain in the shoulder or upper back regions (Karcioglu et al., 2018). The participant rated their pain intensity on a scale ranging from 0 to 10, with 0 indicating no pain and 10 indicating the worst possible pain. A score of 1 to 3 indicates minimum pain, 4 to 6 indicates moderate intensity of pain, and 7 to 10 as severe intensity of pain. Along with pain intensity, the duration of the pain was also collected.
Dynamic Scapular Motion Test (DSMT)
The participants elevated their arms to 120 degrees in the frontal and scapular plans with and without holding weights (Kibler et al., 2002; Larsen et al., 2020). A scapular motion was considered as normal when the motion presents with bilateral posterior tilting, external rotation, and slight superior translation during arm elevation and reversal of these during lowering relative to the opposite side (Larsen et al., 2020). If the scapular motion was not normal, then the clinician observed the scapula for the presence of any of the four patterns of SD. The four patterns of SD were Type I pattern (prominence of the inferior medial scapular angle and would be associated with excessive anterior tilting of the scapula), Type II pattern (prominence of the entire medial border and would be associated with excessive scapular internal rotation), Type III pattern (prominence of the superior scapular border and would be associated with excessive upward translation of the scapula), and finally Type IV pattern (characterized as “normal,” indicating that no asymmetries were identified and no prominence of the medial or superior border was observed) (Kibler et al., 2002; Larsen et al., 2020).
Procedure of DSMT
The DSMT was performed according to a protocol developed by McClure et al. (2009). The DSMT was conducted with participants in the sitting position with both the arms hanging at the sides of the body with the elbow straight and shoulder in neutral position. The sitting position was controlled with their first metatarsophalangeal joint aligned with a marker on the floor to standardize the video recording. As a familiarization procedure, the participants were instructed to perform bilateral active movements of shoulder flexion and abduction in the sagittal and frontal planes carrying mini weights in the hand. The participants carried 1.5 kg if they weighed less than 68.1 kg, and 2.5 kg if they weighed 68.1 kg or more.
A video camera (Canon EOS 700D, Canon, Japan) was mounted on a tripod fixed at the level of scapula and was placed 204 cm away at the back of the participant to record the movements (Figure 1). After the familiarization procedure, the participants performed five repetitions of the shoulder flexion and abduction movements with the weights. All the movements were video recorded and used for analysis. All the trials were conducted by a trained investigator. After the trials, the video recordings were reviewed by two investigators (junior and senior investigators) and chosen the single most predominant pattern of SD. If any patterns of SD were observed, they were marked as “yes” and the type of SD was noted. If a normal scapular motion was observed, it was noted as Type IV, and then it was relabeled as “no” (Larsen et al., 2020). If the mixed patterns of scapular prominence were found during shoulder flexion and abduction movement, the investigators identified the SD as mixed patterns (i.e., Type I + II, Type II + III, Type I + III, or Type I + II + III; Huang et al., 2015). The two investigators rated the patterns of SD independently and no discussion was permitted during the rating procedure. The investigators were permitted to view the video second time if necessary and required. The same videotapes were reviewed again at 7 days later, and the patterns of SD were assessed again by the senior investigator.
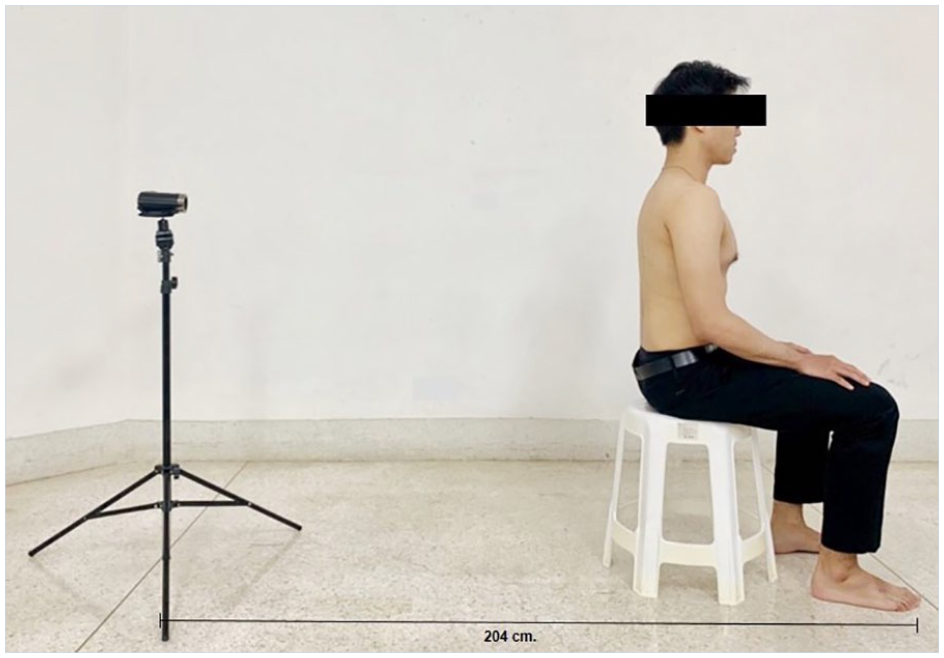
The participants sitting in normal resting posture with a camera on a tripod placed 204 cm away.
Statistical Analysis
The sample size calculation for the study was prepared using G*Power sample size calculator with a power of 0.8 and an effect size of 0.5. Thus, a sample size of 32 participants was considered appropriate for the study to evaluate the patterns of SD among professional bus drivers. In addition, prior to evaluation of patterns of SD, 10 participants were recruited in the study to investigate the reliability of the DSMT using video analysis. The statistical analysis was performed using the SPSS Version 23.0 for Windows. The intra- and interrater reliability of the DSMT were determined using percentage of agreement and weighted Kappa coefficients (Kw). The Kw coefficients were set as follows: 0.81 to 1.00, excellent; 0.61 to 0.80, substantial; 0.41 to 0.60, moderate; 0.21 to 0.40, fair; 0 to 0.20, slight; and less than zero as poor. The statistical significance was considered at an alpha level of p value < .05, with 95% confidence intervals. Descriptive statistics were used to describe the demographic characteristics of participants and the patterns of SD among the study participants.
Findings
Thirty-two long-distance professional bus drivers between 30 and 50 years old participated in the study. The mean age of the professional bus drivers in this study was 43.97 ± 5.20 years. The bus drivers reported a moderate intensity of unilateral upper quadrant musculoskeletal pain (NRS: 5.34 ± 1.29). Table 1 shows the demographic, work and pain characteristics of participants.
Demographic, Work, and Pain Characteristics of the Professional Bus Drivers With Unilateral Upper Quadrant Musculoskeletal Pain (N = 32)
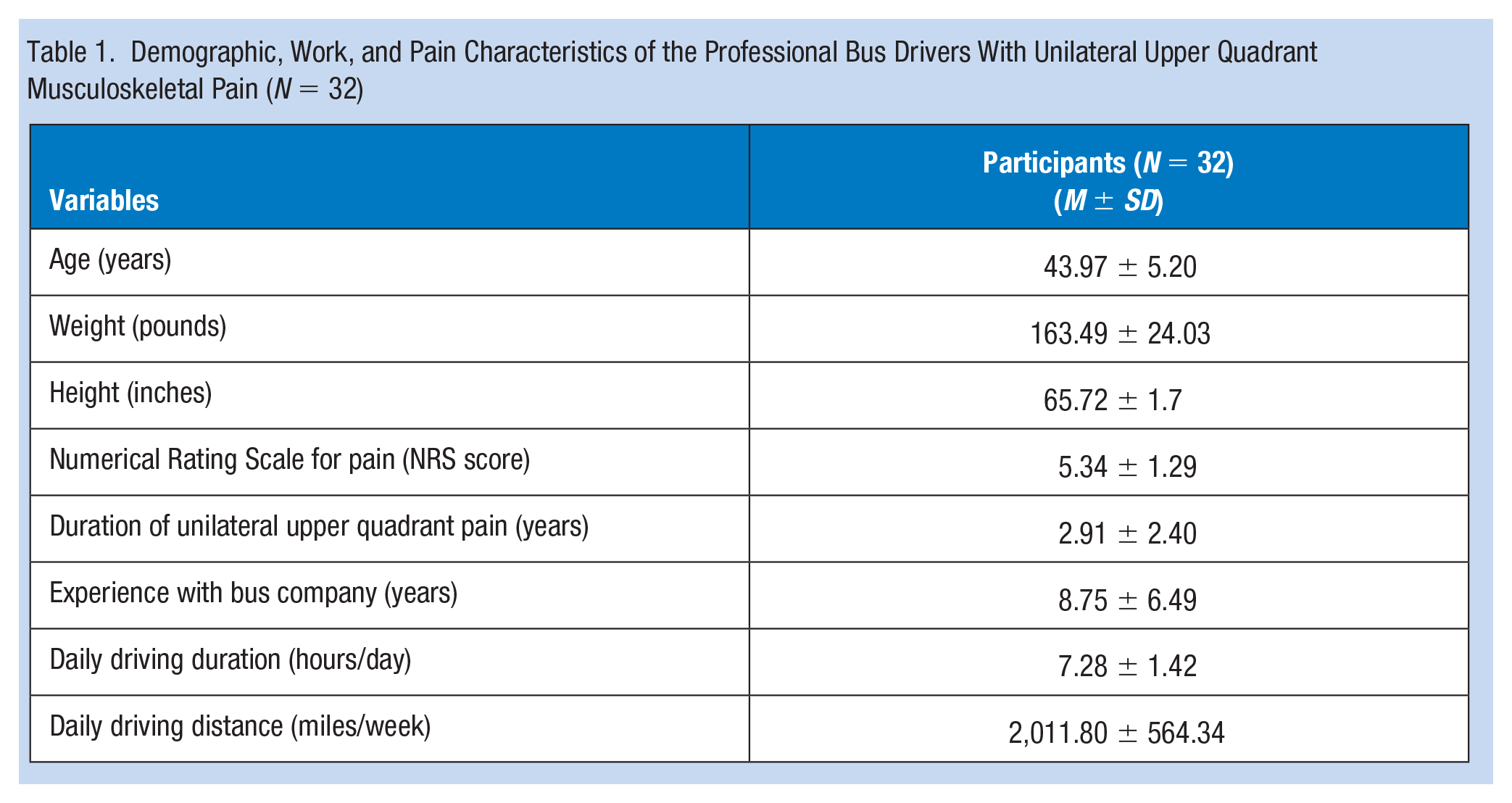
Table 2 shows the results of the reliability analysis for the DSMT using the video analysis to identify patterns of SD among the professional bus drivers with unilateral upper quadrant musculoskeletal pain. A total of 10 participants (age: 43.20 ± 5.75 years, weight: 71.60 ± 9.20 kg, height: 166.00 ± 4.21 cm) participated in the reliability study. The results of intrarater reliability of the DSMT using the video analysis to detect the patterns of SD among the professional bus drivers showed excellent reliability with 100 and 90 percentage of agreements in shoulder flexion and abduction with a Kappa coefficient of 1.00 and 0.878 for shoulder flexion and abduction, respectively (p < .001). The interrater reliability results between the two investigators presented substantial reliability for shoulder abduction and excellent reliability for shoulder flexion with Kappa coefficients of 0.762 to 0.878, respectively (p < .001) (Supplementary material).
Intra- and Interrater Reliability Analysis for the DSMT Using Video Analysis Technique to Identify the Pattern of SD in a Sample of Bus Drivers (n = 10)
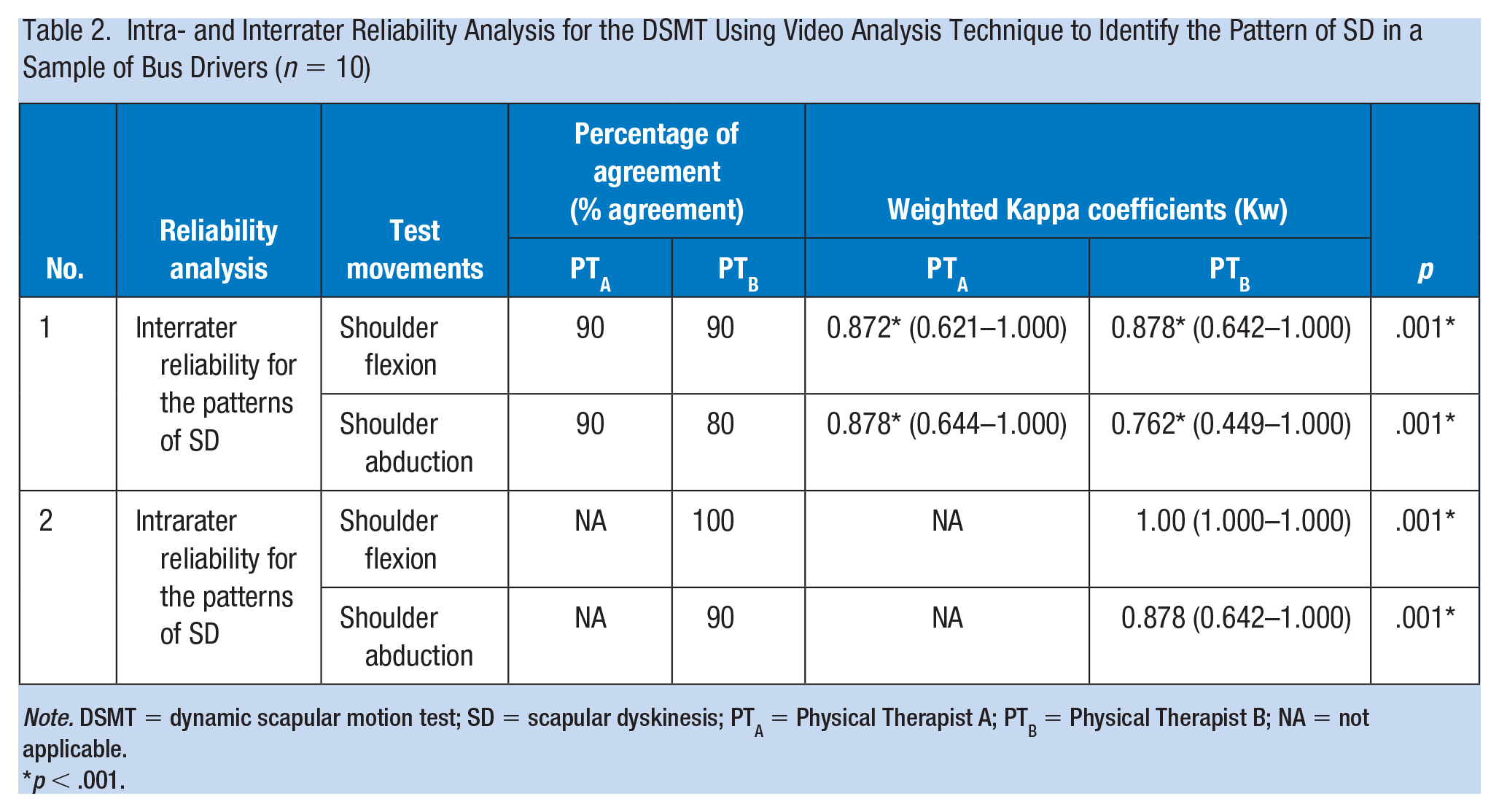
Note. DSMT = dynamic scapular motion test; SD = scapular dyskinesis; PTA = Physical Therapist A; PTB = Physical Therapist B; NA = not applicable.
p < .001.
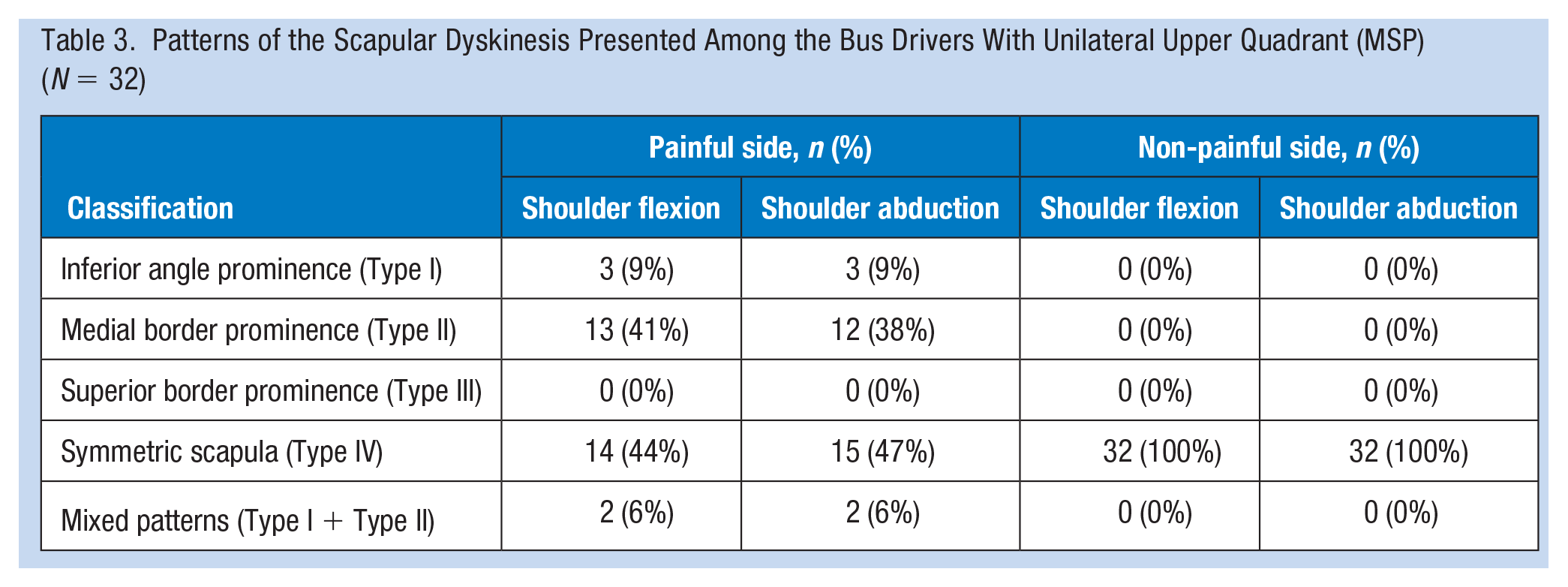
The patterns of the SD presented among the bus drivers with unilateral upper quadrant musculoskeletal pain are shown in Table 3. A symmetrical scapular motion (Type IV) was observed in all the participants in the non-painful side during both shoulder flexion and abduction movements. In the painful side, 56.2% (n = 18) of the bus drivers presented with SD during the shoulder flexion movement, while 53.1% (n = 17) presented with SD during the shoulder abduction movement. Type II was the common pattern of SD observed among the bus drivers during shoulder flexion (41%, n.= 13) and abduction (38%, n = 12) movements. Figure 2 shows a Type II pattern of SD observed among the bus drivers. Also, a mixed pattern of SD (Type I + Type II) was observed in 6% (n = 4) of the bus drivers.
Patterns of the Scapular Dyskinesis Presented Among the Bus Drivers With Unilateral Upper Quadrant (MSP) (N = 32)

Type II pattern of SD (medial border of scapula prominence).
Discussion
This study examined the patterns of SD observed among professional bus drivers with upper quadrant musculoskeletal pain. The clinical consensus statement from a scapular summit suggests that the treatment strategies for SD can be effectively implemented by evaluation of the SD and recommends a comprehensive rehabilitation program to address SD (Kibler et al., 2013). Therefore, it was important to conduct the current study as it helped to establish a reliable clinical method and an understanding on the patterns of SD among bus drivers with upper quadrant musculoskeletal pain.
The findings from the current study demonstrated a reliable clinical method using video analysis of the scapula to identify patterns of SD among people involved in an occupation such as bus driving. The excellent reliability of the DSMT using video analysis for both interrater reliability (Kw = 0.762–0.878) and intrarater reliability (Kw = 0.878–1.00) suggested that the clinical method to investigate the patterns of SD was scientifically acceptable. The reliability findings of DSMT in this study were similar to a previous study (Kibler et al., 2002; McClure et al., 2009). Currently, some of the measurement techniques to evaluate SD require sophisticated equipment and procedures such as electromagnetic tracking device, three-dimensional motion analysis systems, and inclinometers (Nijs et al., 2007; Watson et al., 2005). These dynamic assessments to identify SD are expensive and require specialized equipment (laboratory methods) and specialized training, limiting their usefulness in clinical practice (Nijs et al., 2007). Furthermore, it is challenging to establish clinical assessment criteria to define SD especially when the scapula is moving in two planes. Therefore, video recording and analysis are more appropriate and reliable. Although the DSMT in this study was performed by physiotherapists, the procedure could easily be administered by health care professionals. Thus, the clinical assessment of SD using the DSMT through the video analysis presented in this study could be useful for clinicians in practice because it is a highly reliable, easy to perform, and affordable method.
In the current study, approximately 56.2% and 53.1% of the professional bus drivers who had unilateral upper quadrant musculoskeletal pain demonstrated alterations of scapular movement during the flexion and abduction movements of the DSMT with Type II pattern was identified as the common pattern of SD among the bus drivers. On the contrary, a symmetrical scapular motion was observed in all the participants in the non-painful side during both shoulder flexion and abduction movements. The abnormal motions of the scapula during SD are hypothesized to increase the angulation of the humerus on the glenoid and decrease the subacromial space, leading to MSP and shoulder pathology (Edmonds & Dengerink, 2014). Furthermore, the alterations in the scapula motions and abnormal patterns of SD may lead to a decrease in the performance of neck and shoulder movements (Kibler et al., 2012).
The nature of the professional bus drivers’ work involves driving buses for long distances potentially resulting in overuse and repetitive neck and shoulder movements which may result in SD and upper quadrant MSP. Therefore, the study findings suggest a need to develop appropriate management strategies such as a health awareness program, possibly a screening for upper quadrant musculoskeletal pain, and appropriate referrals for early diagnostic testing. Evidence-based exercises designed by a trained physical therapist could also be considered to alleviate the potential for injury and to manage early symptoms. The study findings also highlight the need for further research to prevent SD and musculoskeletal pain. For example, factors such as driving tasks, equipment used by the drivers, types of buses with and without gears, working hours, and rest breaks need to be studied in the context of SD to explore other risk factors and how they could be prevented. Also, the current study focused only on the scapular kinematics, and the kinetic measures such as strength and motor control of the scapular muscles were not considered. Therefore, further studies that comprehensively analyze both quantitative and qualitative evaluation of upper quadrant musculoskeletal pain and SD among bus drivers are needed.
The study has some limitations. The examination of patterns of SD among the bus drivers was conducted from only one bus company from a specific geographic location; hence, the wider applications of the study findings on the bus drivers need to be interpreted with caution. The small sample size of the study was another limitation. Further studies that investigate SD in a larger population of professional drivers are required. The current study did not control for the types of buses, steering components, and the driving conditions of the bus drivers. The drivers from the bus company used both types of buses with and without gears, driving them interchangeably as allocated by their shift managers and it was possible that the different models of buses might have different engineering features. It needs to be acknowledged that it was challenging to control the types of bus and related variables especially in developing countries where the bus companies and drivers were delivering services to society in spite of the socioeconomic challenges which influence the conditions of the busses used by drivers.
Implications for Occupational Health Practice
The DSMT using the video analysis is a highly reliable clinical method to evaluate the patterns of SD among a sample of bus drivers with upper quadrant musculoskeletal pain. About half of the sample with upper quadrant musculoskeletal pain presented with SD with Type II pattern being the commonly observed pattern of SD. The study provided preliminary evidence of SD among professional drivers with upper quadrant musculoskeletal pain which could serve as a catalyst to design and develop appropriate clinical screening assessments and to frame effective rehabilitation strategies. Practitioners who encounter bus drivers should include an assessment of upper quadrant pain and make appropriate referrals if SD is suspected and if exercises for musculoskeletal pain are indicated. The study provided a clear and reproducible clinical method to evaluate SD which could eventually enable clinicians and occupational health practitioners to apply the clinical test in a wide variety of occupational settings with people with upper quadrant musculoskeletal pain. Further qualitative and quantitative studies encompassing additional assessments of upper quadrant musculoskeletal pain among professional bus drivers are necessary for deeper understanding of the problem in this occupation.
Applying Research to Occupational Health Practice
Upper quadrant musculoskeletal pain is a workplace health issue reported among professional bus drivers. Scapular dyskinesis was suggested to contribute to upper quadrant musculoskeletal pain. The current study presented a reliable clinical evaluation method to examine scapular dyskinesis using a video analysis technique in the workplace setting. The clinical method demonstrated in the study can be translated to any occupational setting to examine scapular dyskinesis for any population who suffers with upper quadrant musculoskeletal pain. Furthermore, the study presented different patterns of scapular dyskinesis with Type II pattern being the commonly observed pattern of scapular dyskinesis. The study invites practitioners to consider a comprehensive assessment to evaluate scapular dyskinesis among people with upper quadrant musculoskeletal pain.
Supplemental Material
sj-xlsx-1-whs-10.1177_21650799211003562 – Supplemental material for A Clinical Evaluation of Scapular Dyskinesis Among Professional Bus Drivers With Unilateral Upper Quadrant Musculoskeletal Pain
Supplemental material, sj-xlsx-1-whs-10.1177_21650799211003562 for A Clinical Evaluation of Scapular Dyskinesis Among Professional Bus Drivers With Unilateral Upper Quadrant Musculoskeletal Pain by Wipawee Sattasuk, Patraporn Sitilertpisan, Leonard Joseph, Aatit Paungmali and Ubon Pirunsan in Workplace Health & Safety
Footnotes
Acknowledgements
The authors express sincere thanks to the bus drivers, supervisors, and managers of the bus company for their support and participation in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an internal university research grant by the Faculty of Associated Medical Sciences and the Graduate School, Chiang Mai University, Chiang Mai, Thailand, and the Rising Star Funding Award by the Research and Enterprise Office, University of Brighton, the United Kingdom.
Supplementary Material
Any underlying research materials related to the paper will be available upon request.
Author Biographies
Wipawee Sattasuk is a qualified physiotherapist who is currently a master’s student in physiotherapy at the Faculty of Associated Medical Sciences, Chiang Mai University, Thailand.
Patraporn Sitilertpisan is an assistant professor at the Department of Physical Therapy, Chiang Mai University. She earned her PhD in biomedical science from Chiang Mai University, Thailand, in 2011.
Leonard Joseph is a senior lecturer at the University of Brighton. He received his master’s degree from the University of South Australia in 2000, and PhD from Chiang Mai University, Thailand, in 2014.
Aatit Paungmali is an associate professor at Chiang Mai University. He received his PhD in physiotherapy at the University of Queensland in 2004.
Ubon Pirunsan is an assistant professor at the Department of Physical Therapy, Chiang Mai University, Thailand. She earned her PhD in health science from the University of South Australia in 2003.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.