
Abstract
Work-related musculoskeletal (MS) disorders are considered one of the most frequent occupational diseases among dental workers. Dental work consists of static, demanding tasks that involve repeated gripping of small-sized instruments. The purpose of this study was to investigate the prevalence of MS pain, the areas of pain, and the risk factors for MS pain in dental workers. A self-administrated questionnaire was used as a data collection instrument for dental workers who voluntarily responded to the invitation. To determine the prevalence and severity location of MS pain, the Cornell Musculoskeletal Discomfort Questionnaire was administered among 87 dental workers, with a total of 79.8%, who reported at least one MS complaint. MS pain occurred in 82.6% of general dentists, 75.0% of dental specialists, 66.7% of dental assistants, and 33.3% of dental technicians. Pain most frequently occurred in the neck (60.7%), upper back (52.4%), right shoulder (44.0%), lower back (41.7%), hips/buttocks (29.8%), and the right wrist (23.8%). The prevalence of pain among dental workers could be reduced by ergonomic working environment, regular breaks, maintenance of health, and performing specific exercises designed to dental workers.
Introduction
Work-related musculoskeletal (MS) disorders are considered one of the most frequent occupational diseases among dental workers (Hayes, Cockrell, & Smith, 2009; Melhorn, 2000). Prior studies reported the frequency of MS disorders among dental workers, ranging from 63% to 93% (Isper Garbin, Barreto Soares, Moreira Arcieri, Saliba Garbin, & Siqueira, 2017; Nasl Saraji, Hosseini, Shahtaheri, Golbabaei, & Ghasemkhani, 2005; Rabei, Shakiba, Shahreza, & Talebzadeh, 2011). MS disorders are defined as inflammatory and degenerative diseases or disorders of muscles, ligaments, tendons, nerves, blood vessels, bones, and joints that can result in pain (Hayes et al., 2009; Melhorn, 2000). They can be defined as neuromuscular impairment, which develops increasingly or repeatedly at low-intensity loads (Duff, 2004; Gauthy, 2007).
The MS disorders are influenced by various factors, including physical characteristics (height and weight), and occupational and sociopsychological agents, such as overuse of a body region, uncomfortable posture, high work intensity, and insufficient breaks (T. S. Cho, Jeon, Lee, Seok, & Cho, 2014; Morse et al., 2007; Punnett & Wegman, 2004; Ylipää, Arnetz, Benko, & Rydén, 1997). One repetition does not cause inflammation or pain, but in case of overuse, the tissue does not have a sufficient amount of time to regenerate, resulting in the development of micro-injuries for specific body parts (Colombini et al., 2001; Novak & MacKinnon, 1997, 2002). MS disorders in dentistry can cause lower productivity due to absence from work, with some experiencing career-ending disability (Valachi & Valachi, 2003a).
Dental work consists of static, demanding tasks that involve repeated gripping of small-sized instruments that require precision. This and other risk factors contribute to dentists being among other professionals with the highest risk of developing MS disorders (Sanders & Michalak-Turcotte, 2004).
Prolonged incorrect working posture is the major contributor to MS problems among these workers. Constant repositioning (sitting/standing position, rotation of the spine), as well as frequent and repetitive static positions, can cause pain and MS and peripheral nervous system disorders (Szymańska, 2002). Static work includes long-term isotonic muscle contraction, where muscle fibers stand static for extended periods of time. During static muscle contraction, compression of blood vessels occurs in the muscle tissue, which results in reduced blood flow and ultimately reduced oxygen to the muscles. Furthermore, waste products accumulate in the muscles and result in fatigue and muscle pain, and the blood flow is reduced in proportion to the intensity and duration of the burden (Kroemer & Grandjean, 1997; Luopajärvi, 1990).
The method of work and/or body position may affect the area where the pain occurs. In sitting positions, dentists reported pain in the spine, as well as in the neck, shoulders, and upper limbs (Valachi & Valachi, 2003a). This same study reported that while working in the standing positions, lumbar pain, as well as varicose veins, poor posture, and flat feet may also occur.
Research among Slovenian dentists conducted from 1977 to 1978 showed a high incidence of professional diseases (Rode, Sušec-Michieli, & Vrbošek, 1978). It was established that 73.6% of the dentists experience chronic spine conditions (e.g., deviation, low back pain, cervicobrachial neuralgia, and thoracic deviation); 60% of those surveyed presented with varicose veins of the legs, 30% reported dyspnea upon exertion, and almost 20% reported edema of the arms and legs. Among them, only 6.8% reported that they are regularly physically active. Kumar, Kumar, and Baliga (2013) conducted a study on the prevalence of MS disorders among dentists in India. They found out that all 536 dentists included in their study had at least one work-related MS symptom in the previous year with an overall period prevalence rate of 100%. The types of symptoms reported included pain (99.1%), stiffness (3.4%), fatigue (8.39%), discomfort (12.9%), clicks/sounds (4.1%), and other neurological deviations (20.1%). The regions of symptoms were the neck (75.7%), wrist/hand (73.1%), lower back (72.0%), shoulder (69.4%), hip (29.9%), upper back (18.7%), ankle (12.3%), and elbow (7.5%). Studies among dentists in Australia (Leggat & Smith, 2006) and Taiwan, Lin et al. (2012) reported similar results with most participant dentists (87.2%) in the Australian study. Both studies indicated that a high proportion of dentists reported pain in the shoulders, lower back, and neck, while Lin et al. (2012) also reported that participants from Taiwan reported a lower prevalence (13%-15%) of pain in their hips/thighs/buttocks, knees, and ankles/feet.
Dental team workers are predisposed to pain in different areas of their bodies (Valachi & Valachi, 2003a). Hayes et al. (2009) conducted a study on MS disorders and symptom severity among dentists, dental assistants, and dental medicine students, who reported pain most frequently occurred in the back (36.3%-60.1%) and neck (19.8%-8.05%) areas. It was noted that pain in the hands and wrists generally occurred among dental assistants (60.0%-69.5%), and that female dentists and dental assistants had a higher prevalence of symptoms of arm (Leggat & Smith, 2006), wrist, shoulder, and neck MS disorders relative to their male counterparts (Szymańska, 2002).
The aim of the study was to present the extent of MS pain as an occupational-related issue among dental workers who resided and practiced in Slovenia. The main goal was to examine the prevalence of MS pain among all dental workers employed in dental offices and dental laboratories. We also sought to examine associations of working conditions, gender, the use of magnifying glasses or loupes, and physical activity on the reporting of different types of MS pain.
Method
The sample of this cross-sectional study was obtained at the Densafe Congress attended by 400 Slovenian dental workers. All attendees were invited to participate in the study, which was described as a self-administrated questionnaire on specific health problems of dental workers. They were given the questionnaire, which they completed and returned. Dental workers who participated in the study were general dentists, dental specialists, dental assistants, and dental technicians. The term dentist denotes a dentist in a general dental office who performs all the common dental procedures in a patient’s mouth. A specialist only performs certain special procedures. Within dentistry, there are periodontists, orthodontics, endodontics, prosthetics, and oral surgeons. They each perform the same special procedures during their working day. Assistants in a dental office, on the contrary, help dentists during their provision of dental care of a patient. Dental technicians work in dental laboratory prosthetic restorations (artificial teeth) for a dental office.
A written informed consent of voluntary participation was obtained from all the participants prior to commencing the study. The participants were provided with sufficient details about the purpose of the study, the expected duration and procedures of the study, and the information on their right to decline or withdraw. The study was approved by the Slovenian National Medical Ethics Committee, which is responsible for the ethical aspects of all medical research in the Republic of Slovenia.
Data Collection
The survey questions were designed on the basis of a questionnaire developed by Kim-Fine, Woolley, Weaver, Killian, and Gebhart (2013), who investigated the work-related MS disorders of surgeons. The questionnaire was adapted to the work conditions and risk factors specific to dental health care providers. To determine the prevalence, severity, location of MS pain, and discomfort, the Cornell MS Discomfort Questionnaire was used (Hedge, Morimoto, & McCrobie, 1999). The questionnaire was anonymous, covering 29 questions. It contained 23 closed-ended questions, where 11 offered the option of choosing “another,” enabling the respondents to write an additional response or provide certain data.
The questionnaire initially inquired about demographic characteristics of the respondents, such as age, sex (male/female), and education level. Work-related questions included field of work, number of years of active professional practice, work duration per day and per week, the dominant arm (right/left), and the method of dental care delivery (two-handed/four-handed, direct/indirect, sitting/standing position, use of dental loupe—often/occasionally/never). Health-related question included the frequency of physical activity (never, once a week, 2-3 times a week, 4 times or more per week), intensity of physical activity (low to no sweating and no breathlessness, medium–moderate sweating and breathlessness, high–strong sweating and breathlessness), duration of physical activity (less than 30 minutes, 30-60 minutes, or more than 60 minutes), and type of physical activity (walking, swimming, running, aerobics, yoga, dance, fitness, cycling, work in the garden, cross-country skiing, mountaineering, tennis/other).
The last part of the questionnaire included two body maps. The first body map indicates the symptom sites in the dominant arm (anterior view of six regions—A: index finger, middle finger and first half of ring finger; B: second half of ring finger, little finger; C: thumb; D: palm area; E: thenar area; F: hypothenar area), and the second was the posterior view of a human figure, which was subdivided into nine anatomical regions to indicate the symptoms in the neck, shoulders, upper back, elbows, low back, wrist/hand, hips/thighs, knees, and ankles/feet. Subjects were also asked to report the frequency and intensity of pain in these areas and the impact of MS discomfort on their work performance. The respondents were asked to mark an affirmative or negative response (Yes or No) with an “X.”
Data Analysis
Descriptive statistics were employed for purposes of describing the demographics of the study population. The relationship between gender, type of work, and physical exercise to MS pain was analyzed using chi-square testing (p < .05, considered significant). The data were analyzed using IBM SPSS Statistics v21.
Results
The study included 87 (21.8%) of 400 dental workers, including 68 (78.1%) of which were women and 19 (21.8%) were men (Table 1). The age of the participants ranged from 26 to 72 years, with the mean age of 45.4 ± 10.2 SD years. The sample consisted of general dentists (79.3%), dental specialists (13.8%), dental technicians (3.4%), and dental assistants (3.4%).
Dental Workers and Prevalence of Musculoskeletal Pain
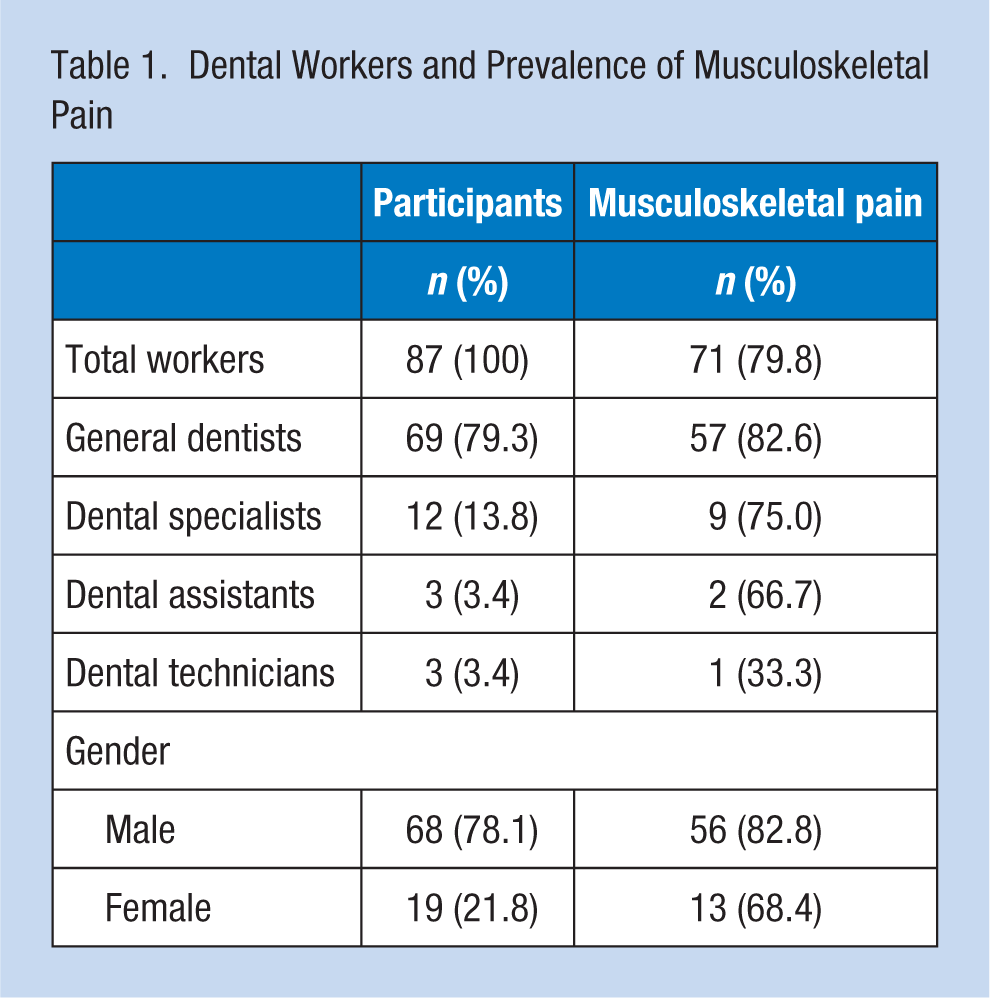
The majority of the respondents (79.8%) had experienced MS pain, while only 20.2% experienced no MS pain (Table 1). Most commonly, the MS pain occurred among general dentists (57/70; 82.6%), followed by dental specialists (9/12; 75%), dental assistants (2/3; 66.7%), and dental technicians (1/3 participant; 33.3%). The study findings indicated that MS pain occurred more frequently in women than in men (56; 82.8% and 13; 68.4%, respectively), but gender-related differences were not statistically significant.
Figure 1 presents the impact of standing and sitting working positions on the prevalence of MS pain among the participants. The difference between sitting and standing groups was not statistically significant. MS pain most frequently occurred in dentists who occasionally used a dental loupe. Relative to those who did not use the dental loupe, the difference, however, was not statistically significant (Figure 2).
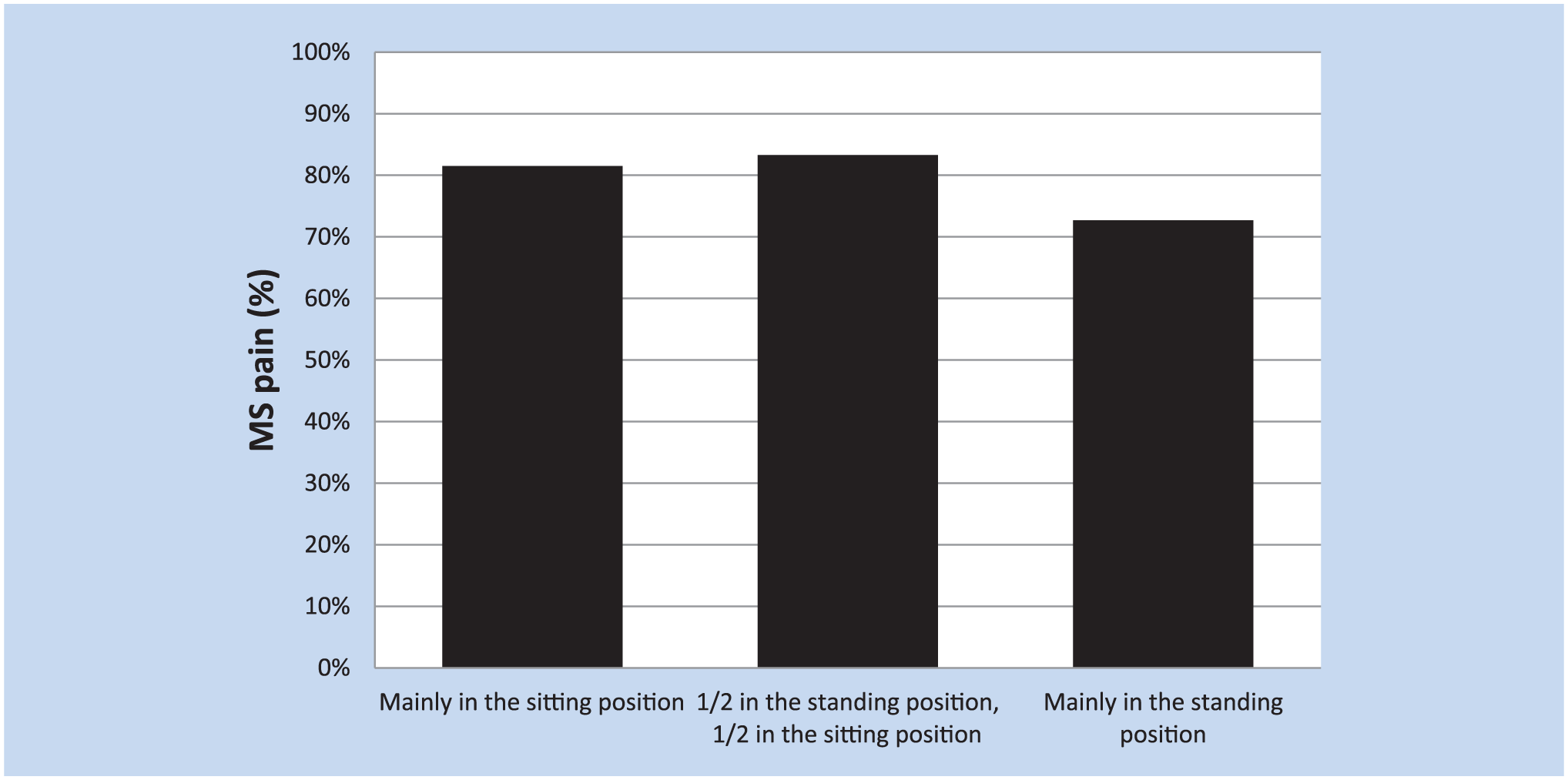
The prevalence of musculoskeletal (MS) pain by working posture.
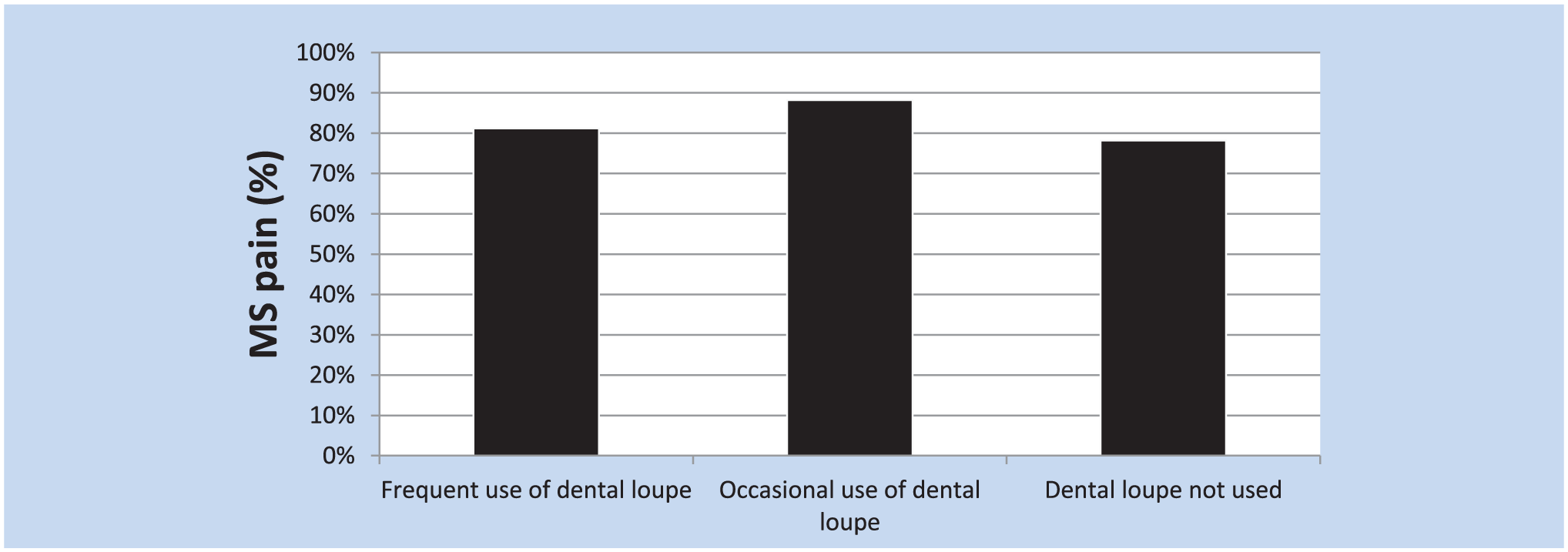
The prevalence of musculoskeletal (MS) pain by the use of dental loupe.
Physical activity and its influence on the occurrence of MS pain was answered by 71 out of 87 dental care providers. The MS conditions were most common in those participants who were physically active 2 to 3 times a week (83.3%), but similar to those workers who were physically active only once a week or less (82.1%). The prevalence of MS pain was lower (72.2%) among participants in the highest physical activity group (physically active 4 times a week or more; 72.2%). Higher frequency of physical activity was not significantly related to the lower risk of MS pain.
With regard to intensity of physical activity and MS pain, it was established that 14 (16.1%) respondents usually performed low-intensity exercises (which were characterized by no sweating or shortness of breath), 59 (67.8%) respondents reported that they performed medium-intensity exercises (moderate sweating and shortness of breath), and only 15 (17.2%) performed high-intensity exercises (sweating heavily and strong shortness of breath). The participants who regularly performed low-intensity exercises were found to experience the least pain (nine participants; 64.3%), followed by those who performed high-intensity exercises (12 participants; 80%). The highest percentage of pain (49 participants; 83.1%) was reported in the respondents who perform medium-intensity exercises.
The prevalence of MS pain in different body regions is shown in Table 2. The body region where workers most experienced pain occurred in the neck (60.71%), followed by the upper back (52.38%), the right shoulder (44.04%), the lower back (41.66%), the hip and buttocks (29.76%), and the right wrist (23.81%).
The Prevalence of Musculoskeletal Pain by Body Regions Among Dental Workers (n = 87)
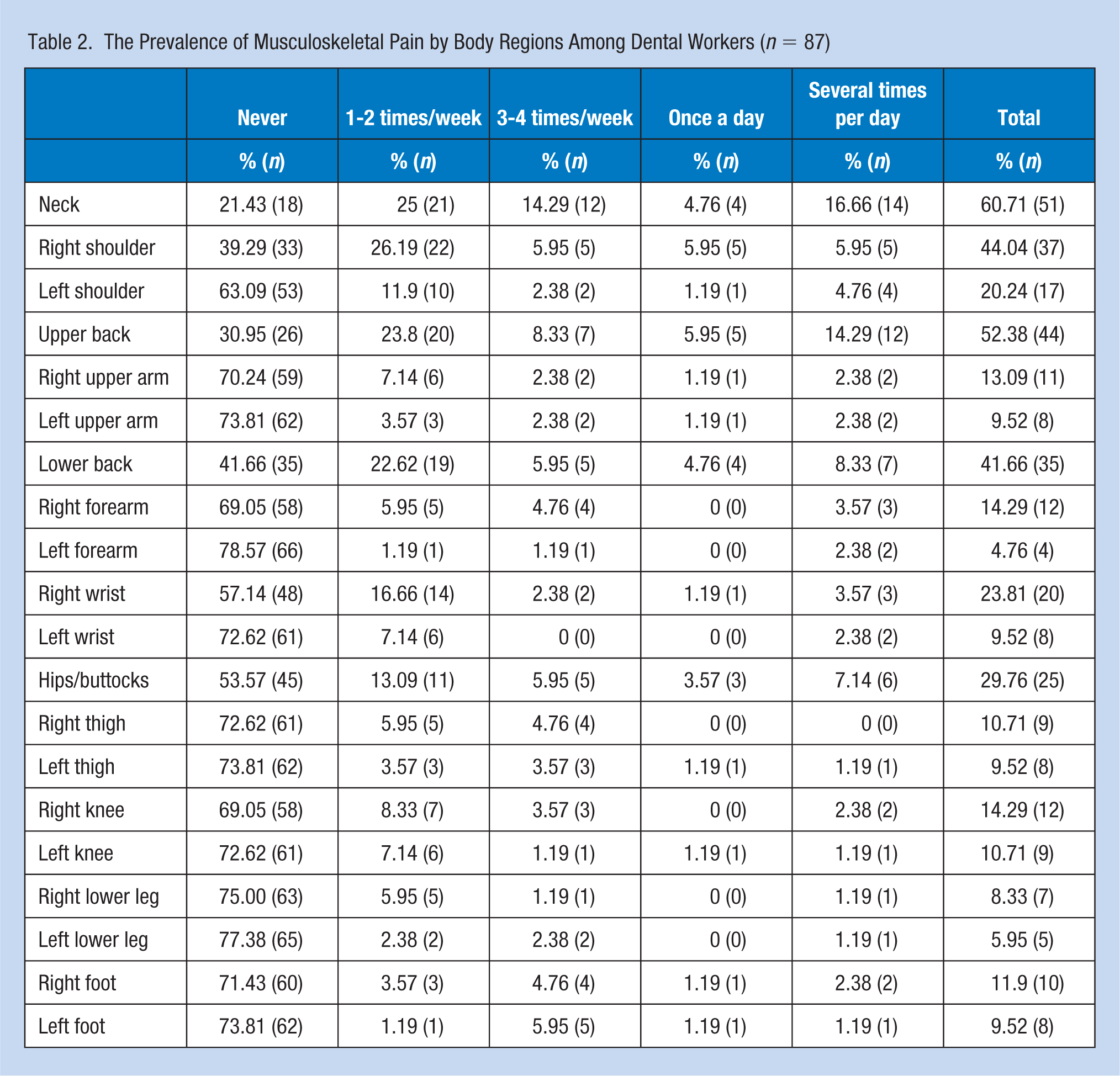
Table 3 presents sites and frequency of MS pain in the dominant hand of the participants. According to the site of the hand, 32.14% of the respondents experienced pain in the thenar area (E area) and 23.8% in the thumb area (C area).
The Prevalence of Musculoskeletal Pain by Area in the Dominant Hand
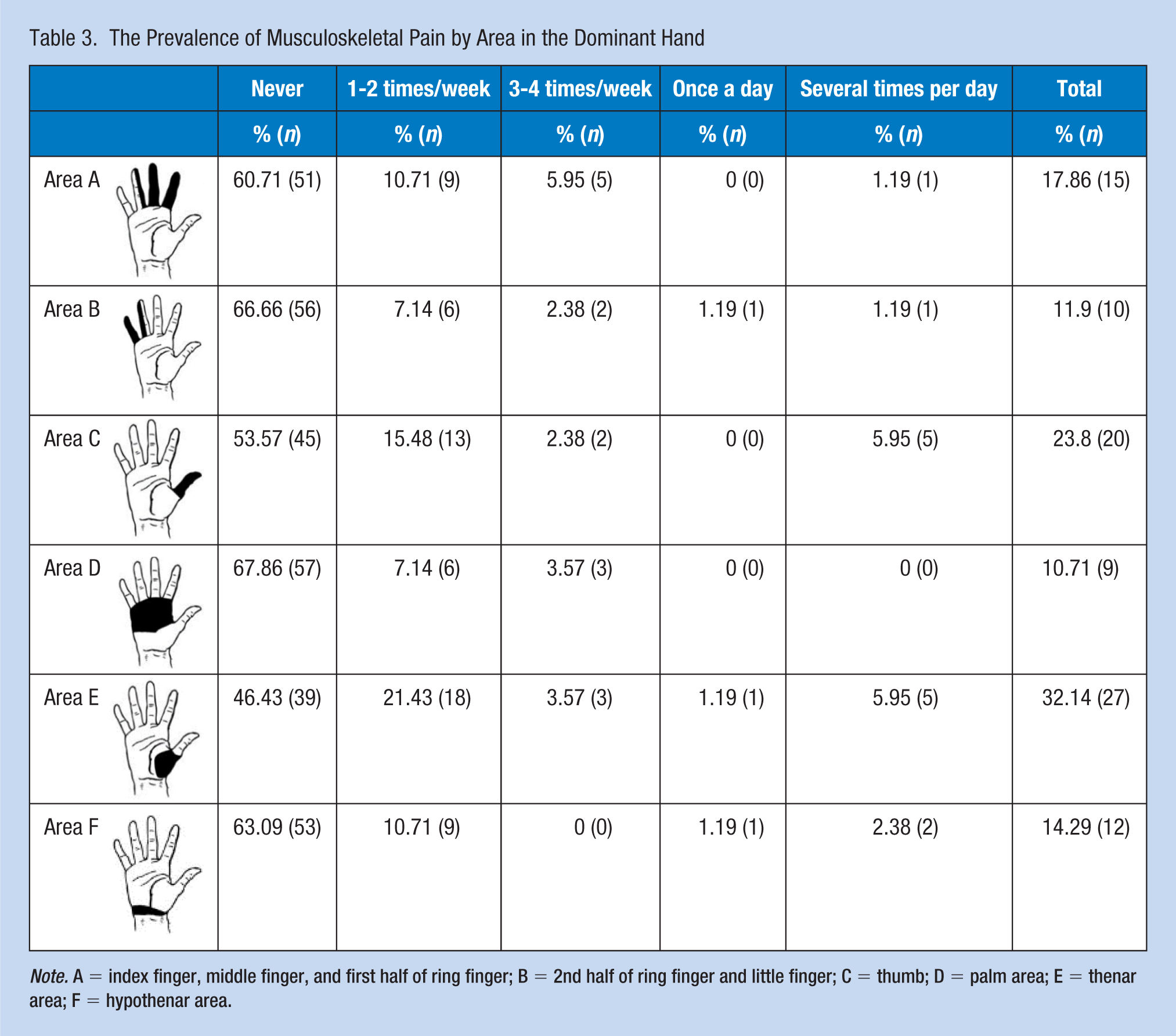
Note. A = index finger, middle finger, and first half of ring finger; B = 2nd half of ring finger and little finger; C = thumb; D = palm area; E = thenar area; F = hypothenar area.
Discussion
This study investigated the extent of work-related MS pain among dental professionals employed in Slovenia and found that most of the participants suffered from pain. The study findings were similar to several previous research studies that reported MS disorders ranging from 63% to 93% (K. Cho, Cho, & Han, 2016; Estrich, 2014; Hayes et al., 2009; Kierklo, Kobus, Jaworska, & Botuliński, 2011; Leggat & Smith, 2006; Muralidharan, Fareed, & Shanthi, 2012; Nasl Saraji et al., 2005; Rabei et al., 2011; Simu, Bocănet, Mesaroş, & Borzan, 2014). A slightly lower prevalence of MS disorders in dentists (62%) was reported in a cross-sectional study conducted by Alexopoulos, Stathi, and Charizani (2004).
The results of the current study indicated that MS pain among dental practitioners most commonly occurred in the neck, upper back, shoulder, and the right lower back. Quite frequently, the pain also developed in the hip, buttocks, and the right wrist, which is similar to prior studies (Aminian, Alemohammad, & Sadeghniiat-Haghighi, 2012; K. Cho et al., 2016; Estrich, 2014; Hayes, Smith, & Taylor, 2013; Kierklo et al., 2011; Muralidharan et al., 2012; Rafeemanesh, Jafari, Kashani, & Rahimpour, 2013; Rucker & Sunell, 2002; Shrestha, Singh, & Niraula, 2008; Tirgar, Javanshir, Talebian, Amini, & Parhiz, 2015).
The present research results indicate that MS pain is most common in general dentists, followed by dental specialists, dental assistants, and dental technicians. According to Leggat and Smith (2006), the MS pain, especially in the neck, most commonly occurred in general dentists among all dental care providers in Australia. Rice, Nindl, and Pentikis (1996), however, concluded that dental practitioners had a lower risk of developing MS diseases relative to dental hygienists and dental assistants. The latter were found to develop pain in the upper limbs and lumbar spine. Similar results were reported by Åkesson, Johnsson, Rylander, Moritz, and Skerfving (1999) and Lalumandier and McPhee (2001), who found that dental hygienists in comparison with other dental workers had a higher risk of developing pain in the neck, shoulder, arm, and wrist.
The results of this study identified a slightly higher prevalence of MS symptoms and potential risk factors in women, but the gender-related differences were not statistically significant. In contrast, Rundcrantz, Johnsson, and Moritz (1991); Kerosuo, Kerosuo, and Kanerva (2000); and Marshall, Duncombe, Robinson, and Kilbreath (1977) reported that the prevalence of MS disorders was higher in female than in male dental workers. Aminian et al. (2012) reported that 91.6% of female dentists had symptoms of pain in at least one part of the body. These findings support the results of other studies, which have shown that the occurrence of symptoms in the arm, wrist, shoulder girdle, neck, spine, hip, and thigh were higher among female relative to male dental health workers (Alexopoulos et al., 2004; Leggat & Smith, 2006; Simu et al., 2014; Szymańska, 2002; Tirgar et al., 2015). Kim-Fine et al. (2013) reported that female surgeons had more frequent and more severe MS disorders in the neck, dominant shoulder, and upper back than their male colleagues.
The current study found no associations between the frequency of MS pain and the work position while sitting in a dental chair. These findings are in agreement with the results obtained by Shrestha et al. (2008), who found no difference in the prevalence of MS disorders between the dentists working mainly in a sitting position, and the dentists adjusting sitting and standing positions. Ratzon, Yaros, Mizlik, and Kanner (2000) reported that dentists who worked in a sitting position had more severe pain in the lumbar spine. Rafeemanesh et al. (2013) conducted a study on job postures and MS disorders in dentists, and concluded that maintaining balance in a standing position during surgery presented the greatest risk of developing MS symptoms. These findings are supported by those of Kierklo et al. (2011), who reported that standing work position is a risk factor for pain in knees and feet.
In recent years, some authors offered recommendations on the use of dental loupe to maintain correct position of the lumbar spine. Proper selection, adjustment, and the use of dental loupe have been associated with decreased pain in the neck and lower back as they enable the dentists to maintain healthier postures (Chang, 2002; Valachi & Valachi, 2003b). In contrast, the results of the current study indicate that frequent use of dental loupe did not significantly reduce the risk for MS pain. However, with a small sample size using dental loupe, these findings should be interpreted with caution. However, prior study findings have been mixed with a higher prevalence of MS symptoms among dental practitioners regularly using dental loupe was reported by Estrich (2014), while Maillet et al. (2008) reported a significant improvement of posture when dental workers used dental loupe.
In most studies, strong and significant correlations between physical activity and the reduced risk for MS pain were affirmed. Regular and frequent practice of activity reduced the number of affected body parts (Simu et al., 2014). Dental practitioners who do not regularly perform physical activities have a significantly higher number of MS pain areas than those who regularly perform physical activities. Droeze and Jonsson (2005) reported that workers who were not physically active were at risk of developing MS disorders, due, in part, to a reduced flow of nutrients and oxygen to the muscles. For this reason, 20 minutes of aerobic exercise 3 to 4 times a week is recommended for dental workers (Valachi & Valachi, 2003a).
The goal of our study was also to determine whether the intensity of exercise increased or reduced the risk for MS pain, which we found to be associated but did not reach statistical significance. In contrast to these findings, the study by Chatzitheodorou, Kabitsis, Malliou, and Mougios (2007) observed that high-intensity aerobic exercise reduces pain, inability of movement, and psychological stress among workers with chronic MS pain in the spine.
The findings of the study prompted us to develop guidelines and instructions to avoid MS pain in dentistry. To reduce multifactorial risk factors, certain preventive measures and ergonomic principles must be applied. Improper and prolonged static or constrained postures may result in gradual damaging physiological changes, leading the muscle imbalances, joint stiffness, muscle damage, and degeneration of spinal discs. The incidence of MS diseases and their risks can be reduced by proper positioning of both patient and dental worker, periodic breaks and stretching, health promotion and good general health, as well as targeted and tailored physical activity (Gupta, Ankola, & Hebbal, 2013).
Implications for Occupational Health Nursing Practice
Dentistry does not lend itself to good posture; however, it is possible with instruction and consistent practice to correct the harmful postural habits that may be the cause of such stress and pain. Dental professionals are prone to unique muscle imbalances and require special exercise and ergonomic interventions to maintain optimal health during the course of their career. It is important to not only know what are effective interventions but also in what sequence to implement them.
Proper body mechanics and ergonomics are essential to dental workers throughout their working life. To reduce multifactorial risk factors, certain preventive measures and ergonomic principles must be applied. For personnel working in dentistry, the most important guidelines and instructions to avoid MS disorders relate to correct body position, changing sitting and standing positions during the workday, positioning patients in a position conducive to safe work practices, having ergonomically designed working stations, taking regular breaks, performing stretching exercises during and after work, utilization of a dental loupe, as well as engaging in physical activity. Dental workers benefit from adapting to the use of proper working postures, maintaining sufficient lighting, and ensuring easy access to the required instrumentation and materials for different working practices, clinical procedures, and patient types.
Conclusion
This study found a high prevalence of MS pain among Slovenian dental professionals, which was most common among general dentists, followed by specialists, dental assistants, and dental technicians. The most frequent areas of MS pain among dental workers occurred in the neck, upper back, right shoulder, lower back, hip, buttock, and right wrist. It was established that standing work position did not significantly reduce the risk for MS pain. Statistically significant correlation between the occurrence of MS pain and use of a dental loupe, female gender, frequency, and intensity of physical activity was not confirmed. It is necessary to introduce prevention programs into dental education to prevent MS discomfort during educational and professional years.
Applying Research to Practice
Work-related MS disorders are considered one of the most frequent occupational diseases among dental workers, which have been attributed to prolonged incorrect working postures. Our study among Slovenian dental professionals showed a high prevalence of MS pain, especially among general dentists. Their MS pain can be reduced by proper positioning of both patient and dental worker, periodic breaks and stretching, health promotion and good general health, as well as targeted and tailored physical activity. It is necessary to introduce prevention programs into dental education programs to prevent MS discomfort.
Footnotes
Ethical Approval
The study protocol was approved by the National Medical Ethics Committee of Slovenia (No 113/02/15). Anonymity and confidentiality were guaranteed to participants in the study.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Darija Šćepanović, MSc, is a physiotherapist specialized in women’s health at the University Medical Center Ljubljana, Department of Obstetrics and Gynaecology, and senior lecturer at the Faculty of Health Sciences of the University of Ljubljana, Slovenia.
Tina Klavs, BSc, is a physiotherapist of respiratory care at Clinical Department for Anesthesiology and Intensive Care at University Medical Center Ljubljana, Slovenia.
Ivan Verdenik, PhD, is a researcher and a statistician at the University Medical Center Ljubljana, Slovenia, with expertise in gynecology and obstetrics.
Čedomir Oblak, PhD, DMD, is an assistant professor at the Medical Faculty of the University of Ljubljana and the specialist of prosthodontics of the University Medical Center Ljubljana, Slovenia.