
Abstract
Background
Many studies have reported an association between overwork, shift work, and chronic disease. However, there is little research on the influence of working hours and shift work and management of chronic diseases. The objective of this retrospective study was to examine the association between working hours, shift work type in workers with hypertension, diabetes, and dyslipidemia.
Methods
Among 18,513 hourly wageworkers from the Korea National Health and Nutrition Examination Survey, 4,313 with hypertension, diabetes, and hyperlipidemia were selected. An analysis of covariance with general linear modeling was used to estimate group differences in clinical indices of chronic diseases according to weekly working hours and types of shift work, both unadjusted and adjusted for gender, age, education, marital status, household income, and medication usage.
Findings
Clinical indicators were worse in workers with diabetes (differences in HbA1c = 0.15%; fasting blood glucose = 4.84 mg/dL), hypertension (differences in diastolic blood pressure = 1.2 mmHg), or dyslipidemia (differences in total cholesterol = 3.3 mg/dL) who worked for more than 40 hours/week compared with workers who worked less than 40 hours per week. Clinical indicators in workers with diabetes and hypertension were worse in shift workers, including evening and night shifts, relative to those who did not work shiftwork.
Conclusions/Application to Practice
Working more than 40 hours per week and shift work were negatively associated with adverse clinical indicators among workers with chronic diseases. To improve the health of workers with chronic diseases, these findings suggest that adjustment of working hours and shift work may be warranted.
Keywords
Background
Overwork is associated with suicide and sudden death caused by cardiovascular disease (Ke, 2012; Lin et al., 2018). South Korea has longer working hours than any other developed country, with an average time of 2,069 hours per worker per year, according to 2016 data collected by the Organization for Economic Co-operation and Development. Based on the current attention towards overwork, legislation on working hours is being implemented in South Korea. In July 2018, the government of Korea reduced the maximum weekly working hours from 68 to 52 hours among companies with more than 300 employees (Moulite, 2018). The definition of overwork by the International Labour Organization (ILO, 2020) is “the principle of the 40-hour workweek” which was adopted in 1935, but many countries have no national limits set for the maximum working hours per week.
Working to death (called “karoshi”) is a worldwide work-related hazard (Li, 2016), and studies have reported positive associations between overwork and cardiovascular disease (Kivimäki, Jokela, et al., 2015; Virtanen & Kivimäki, 2018), cerebrovascular disease (Kivimäki, Jokela, et al., 2015; Shin et al., 2017), and/or mental disorders (Takahashi, 2019) Furthermore, overwork has also been associated with an increase in the prevalence of chronic diseases such as hypertension (Yoo et al., 2014), diabetes (Kivimäki, Virtanen, et al., 2015), dyslipidemia (Muratsubaki et al., 2016), and cardiac arrhythmias (Kivimäki et al., 2017). Effects on psychological conditions, including depression and emotional status (Hsu et al., 2019; Virtanen et al., 2018), and on lifestyle behaviors such as alcohol consumption and smoking (Virtanen et al., 2015), sleep disturbances (Virtanen et al., 2009), and general health status (Cho et al., 2018) have also been observed. Although investigations of risk factors for cardiovascular disease and the incidence of other chronic diseases are documented, there is little research on the influence of working hours on clinical measures among those who have these diseases and work long hours and shift work.
Along with working hours, different types of shift work have been associated with negative health effects. Many studies have clarified the association between shift work such as day to night shift work and health; for instance, high body mass index (BMI; Buchvold et al., 2015), incidence of smoking (Buchvold et al., 2015), and increased risks for cardiovascular disease (Torquati et al., 2018; Wang et al., 2018), cancer (Hansen, 2017; Salamanca-Fernández et al., 2018), gastrointestinal disease (Chadolias et al., 2017; Papantoniou et al., 2017; Reynolds et al., 2017), and metabolic syndrome (Reynolds et al., 2017) are linked to shift work. In particular, shift work is investigated as an important risk factor in metabolic and chronic diseases (Balieiro et al., 2014; Barbadoro et al., 2013; Canuto et al., 2013). Previous findings show that shift workers experience circadian rhythm disorders, hormonal changes, and lifestyle changes, including changes in eating habits (Crispim et al., 2009; Padilha et al., 2010). These circumstances affect the incidence and management of chronic disease. However, as with working hours, studies on the effects of shift work on the management of chronic diseases are still underprovided.
The objective of this retrospective study was to investigate the relationship between working hours, shift work type, clinical indicators of patients with hypertension, diabetes, and dyslipidemia. We compared clinical indicators in patients with diabetes, dyslipidemia, and hypertension by the weekly working hours and shiftwork.
Methods
This study was executed using cross-sectional data from the Korea National Health and Nutrition Examination Survey (KNHANES), which represents the entire Korean population. The division of Health and Nutrition Survey under the Korea Centers for Disease Control and Prevention administers this survey, and it is conducted periodically since 1998 based on the National Health Promotion Act. Participant data were stratified by geographic location, sex, and age according to a probability-clustered sampling design (Kweon et al., 2014). In this study, a total of 39,225 participants in KNHANES from 2013 to 2017 were chosen, and participants without information about working hours or types of shift work and those who did not work were excluded, with a total of 18,513 participants. Among those, 4,313 workers with one or more diseases of hypertension (n = 3,106), diabetes (n = 1,176), and hyperlipidemia (n = 1,786) were chosen for analysis. All participated voluntarily and provided informed consent before participating in the study. The KNHANES protocol was approved by the Korean Ministry of Health and Welfare, and the study was executed consistent with the guidelines of the Declaration of Helsinki. Ethical approval for this study was agreed by the institutional review board (IRB) of the KCDC Seoul, Korea. The KNHANES data are openly available at the KNHANES website: https://knhanes.cdc.go.kr/knhanes/eng/index.do.
Each study participant’s information was collected by face-to-face interviews regarding overall health and diet, a standardized physical examination, and administration of laboratory tests (Kweon et al., 2014). Sociodemographic and lifestyle variables of the participants were determined using a self-administered questionnaire through a face-to-face interview with an interviewer, including data on gender, age, household income, marital status, and education level. Household income was calculated based on total household income of residents and then divided into quartiles from poorest to wealthiest such as low, mid-low, mid-high, and high based on the representative study sample of households. Marital status was categorized as married, widowed or divorced, or never married. Education level was classified as graduation status of elementary school, middle school, high school, and college degree or further education. In the case of medication usage, it was coded as a person who takes medicine only when he or she is prescribed by the doctor versus taking the medicine for more than 20 days per month. History of diagnosis of diabetes, hypertension, and dyslipidemia was confirmed by a self-reported response whether it was diagnosed by a physician.
Information regarding the number of working hours per week was obtained through a self-measurement open-ended questionnaire in which participants were asked to report the average weekly work time, including overtime (mealtime was excluded) they worked. “Shift work” is an employment practice planned to make use of, or offer service across, all 24 hours of the clock each day of the week. In the case of shift work, the following options were included for participants to select: (a) no shift work, (b) evening shift or night shift, and (c) irregular shifts.
During the interview, diastolic and systolic blood pressures were performed 3 times at 5-minute intervals, and the resulting values were averaged. Systolic blood pressure level below 140 mmHg and diastolic blood pressure level below 90 mmHg is considered normal (Park, 2019). Trained laboratory specialists collected blood samples from the participants for biochemical analyses. Blood samples for each participant were taken after fasting for at least 8 hours. Glycated hemoglobin (HbA1c), serum fasting blood glucose, low-density lipoprotein cholesterol (LDL cholesterol), and total cholesterol were measured by an automated enzymatic analyzer and liquid chromatography. For participants without diabetes, the normal range for the hemoglobin A1c level is between 4% and 5.6% (Lee et al., 2019), and the normal range for fasting blood glucose level is between 70 and 100 mg/dL (Lee et al., 2019). Total cholesterol levels below 200 mg/dl and LDL cholesterol below 130 mg/dl are considered normal (Rhee et al., 2019).
Data Analyses
The KNHANES sampling weights were used to account for the complex survey design, survey nonresponses, and poststratification of data. Descriptive statistics were conducted for sociodemographic factors. The work hours variable was divided into three categories: more than 52 hours per week (the legal standard of Korea), between 40 and 52 hours per week, and less than 40 hours per week.
The outcome variables were defined as estimated group difference of clinical indices. Clinical indices (HbA1c level and fasting blood glucose in patients with diabetes, systolic and diastolic blood pressure in patients with hypertension, and total cholesterol and LDL cholesterol level in patients with dyslipidemia) were analyzed in patients with each chronic disease condition; stratified analysis among each disease condition was conducted separately. Our analyses divided respondents’ working hours into three segments: the data based on 40 hours per week (the standard working time in the United States) and data based on 52 hours per week (the legal work time limit per week in Korea). We used analysis of covariance with general linear modeling to estimate group differences in clinical indices according to weekly working hours and types of shift work, both unadjusted and adjusted for gender, age, education, marital status, household income, and medication usage. All statistical analyses were performed using R version 3.5.1. All p values < .05 were considered significant.
Results
Baseline Characteristics of the Study Population
Of the total 4,313 participants, more than half (55.3%) worked <40 hours per week, whereas 20.0% worked 40 to 52 hours and one fourth worked more than 52 hours per week (Table 1). Most (86.6%) did not work shiftwork, whereas 12.1% worked shifts, including evening or night work, and 1.3% worked irregular shifts. The percentage of women who worked ≤40 hours per week (63.5%) was greater than men (48.6%), but female participants had a lower percentage of shift work, including evening or night work (12.7%). Compared with other income groups, the majority (70.2%) that worked <40 hours per week were in the lowest income quartile. The percentage of participants who worked <40 hours per week was highest in widowed or divorced people (65.7%), and participants who never married had a higher percentage of evening or night shift work (18.9%). The majority of participants (72.0%) had hypertension, with less than half (41.4%) that had dyslipidemia and with fewer (27.3%) that had diabetes.
General Characteristics of KNHANES Study Population According to Weekly Working Hours and Types of Shift Work (n = 4,313)
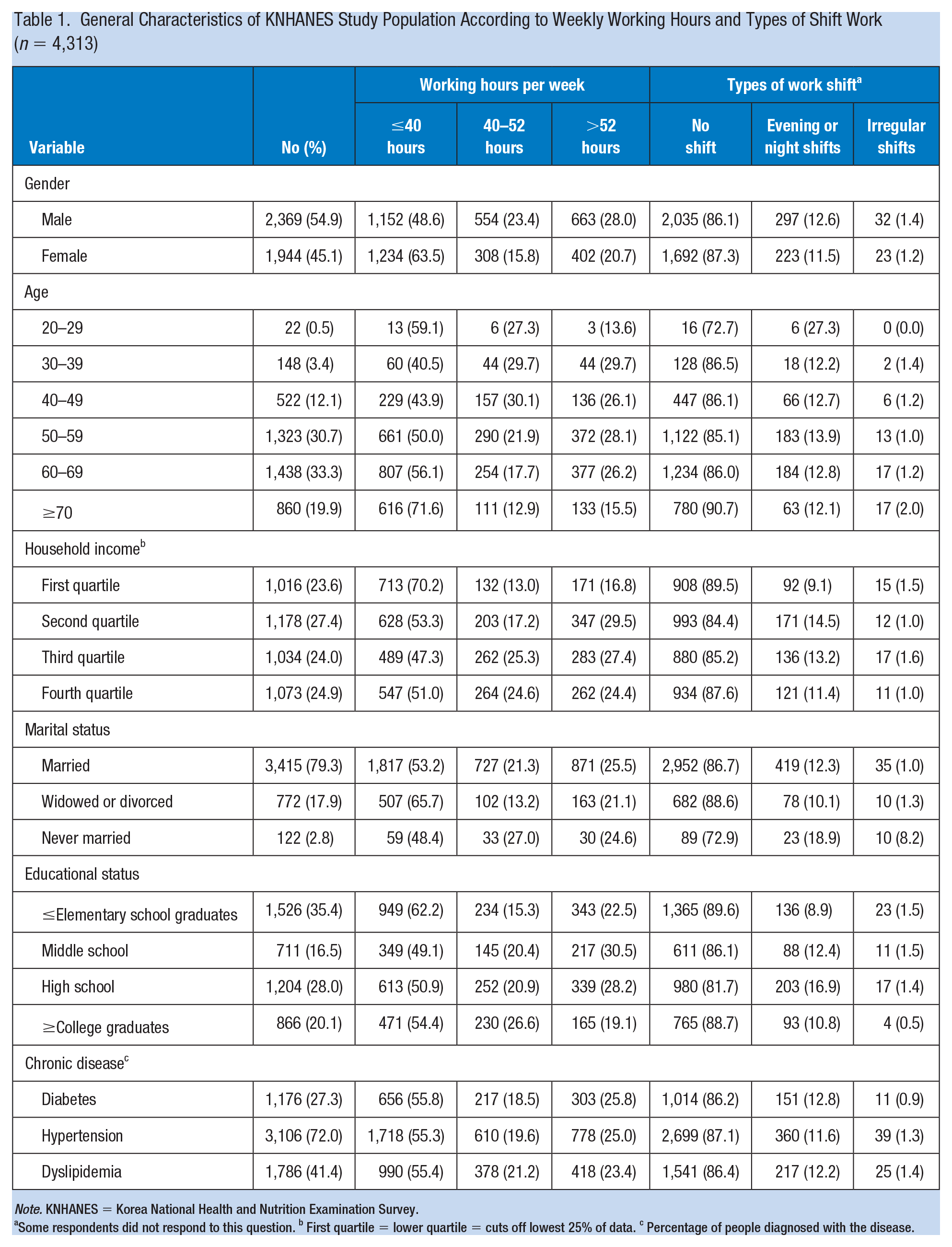
Note. KNHANES = Korea National Health and Nutrition Examination Survey.
Some respondents did not respond to this question. b First quartile = lower quartile = cuts off lowest 25% of data. c Percentage of people diagnosed with the disease.
Indicators of Diabetes, Hypertension, and Dyslipidemia by Weekly Working Hours
Compared to participants with diabetes that worked <40 hours per week, those subjects who worked 40 to 52 hours did not show any differences in HbA1c and fasting blood glucose levels (Table 2). However, those who worked for more than 52 hours/week had higher HbA1c (0.26%; 95% confidence interval [CI] = [0.10, 0.42]; p = .001) and fasting blood glucose (6.3 mg/dL; 95% CI = [2.6, 9.9]; p = .001) compared with those study participants who worked less than 40 hours per week. For hypertension, there were no differences in systolic blood pressure among the study groups. However, compared with those that worked <40 hours/week, their diastolic blood pressure was 0.9 mmHg higher for those who worked for 40 to 52 hours/week (95% CI = [0.3, 1.5]; p = .002) and 1.4 mmHg higher for those who worked >52 hours/week (95% CI = [0.7, 2.0]; p < .001). For dyslipidemia, for workers with work times of 40 to 52 hours weekly compared with 52-hour or more workers showed no significant difference as compared with the group with less than 40 hours work time.
Multivariate Models Examining Differences in Clinical Measures of Diabetes, Hypertension, and Dyslipidemia by Weekly Working Hours Among KNHANES Participants (n = 4,313)
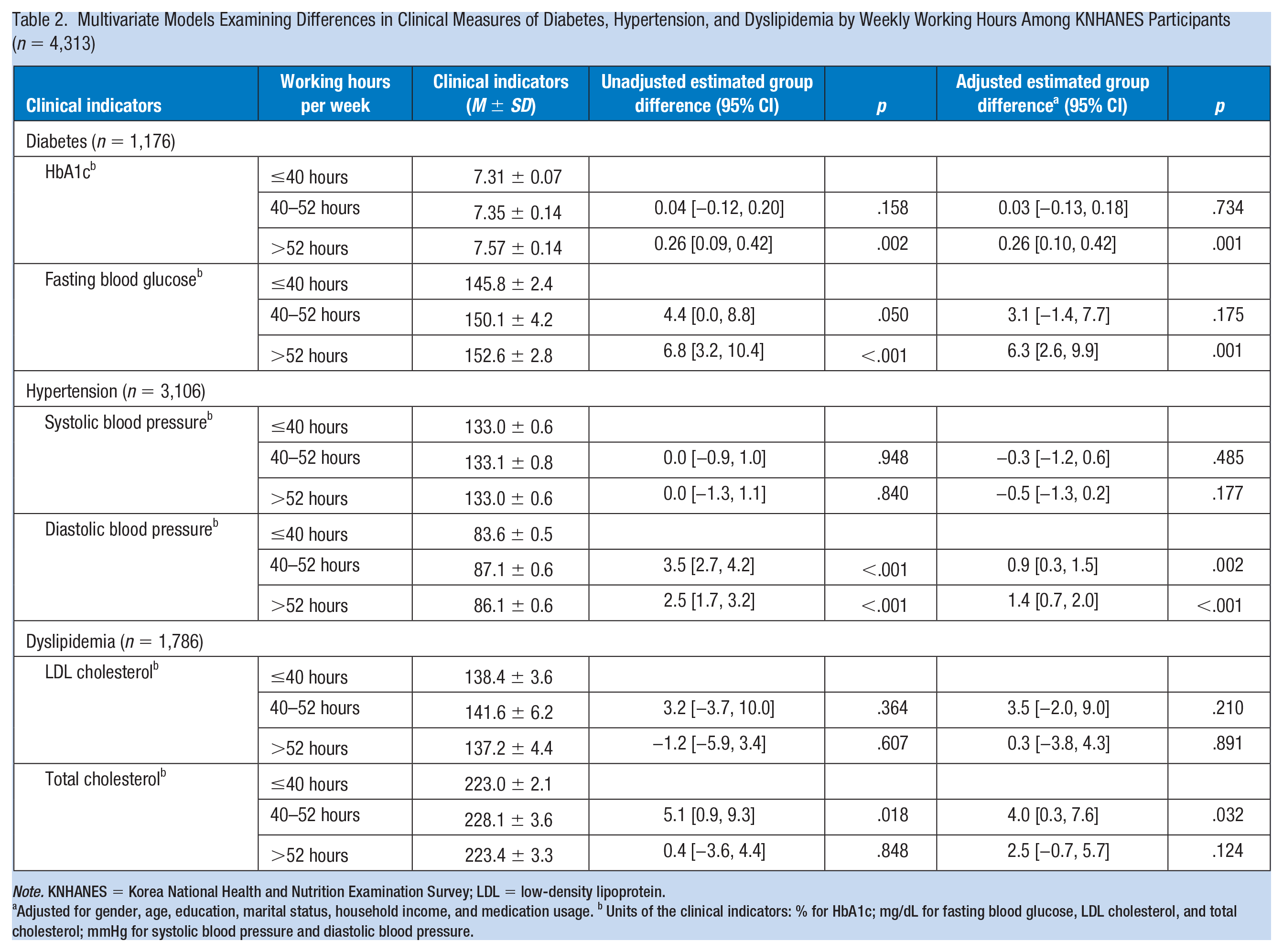
Note. KNHANES = Korea National Health and Nutrition Examination Survey; LDL = low-density lipoprotein.
Adjusted for gender, age, education, marital status, household income, and medication usage. b Units of the clinical indicators: % for HbA1c; mg/dL for fasting blood glucose, LDL cholesterol, and total cholesterol; mmHg for systolic blood pressure and diastolic blood pressure.
Indicators of Diabetes, Hypertension, and Dyslipidemia by Types of Shift Work
Among workers with diabetes, the shift workers who worked during the evening or night had a 0.29% higher Hb1Ac level (95% CI = [0.08, 0.55]; p = .037; Table 3) compared with day shift workers. In patients with hypertension, systolic blood pressure was 3.6 mmHg higher in evening or night shift workers (95% CI = [2.7, 4.6]; p < .001), but diastolic blood pressure was 1.1 mmHg lower (95% CI = [−1.8 to −0.4]; p = .003). Shift workers with irregular shifts also had a 3.4 mmHg higher systolic blood pressure than nonshift workers (95% CI = [0.1, 6.7]; p = .046). In patients with dyslipidemia, there were no significant differences according to the shift type.
Multivariate Models Examining Differences in Clinical Indicates of Diabetes, Hypertension, and Dyslipidemia by Types of Shift Work Among KNHANES Participants (n = 4,313)
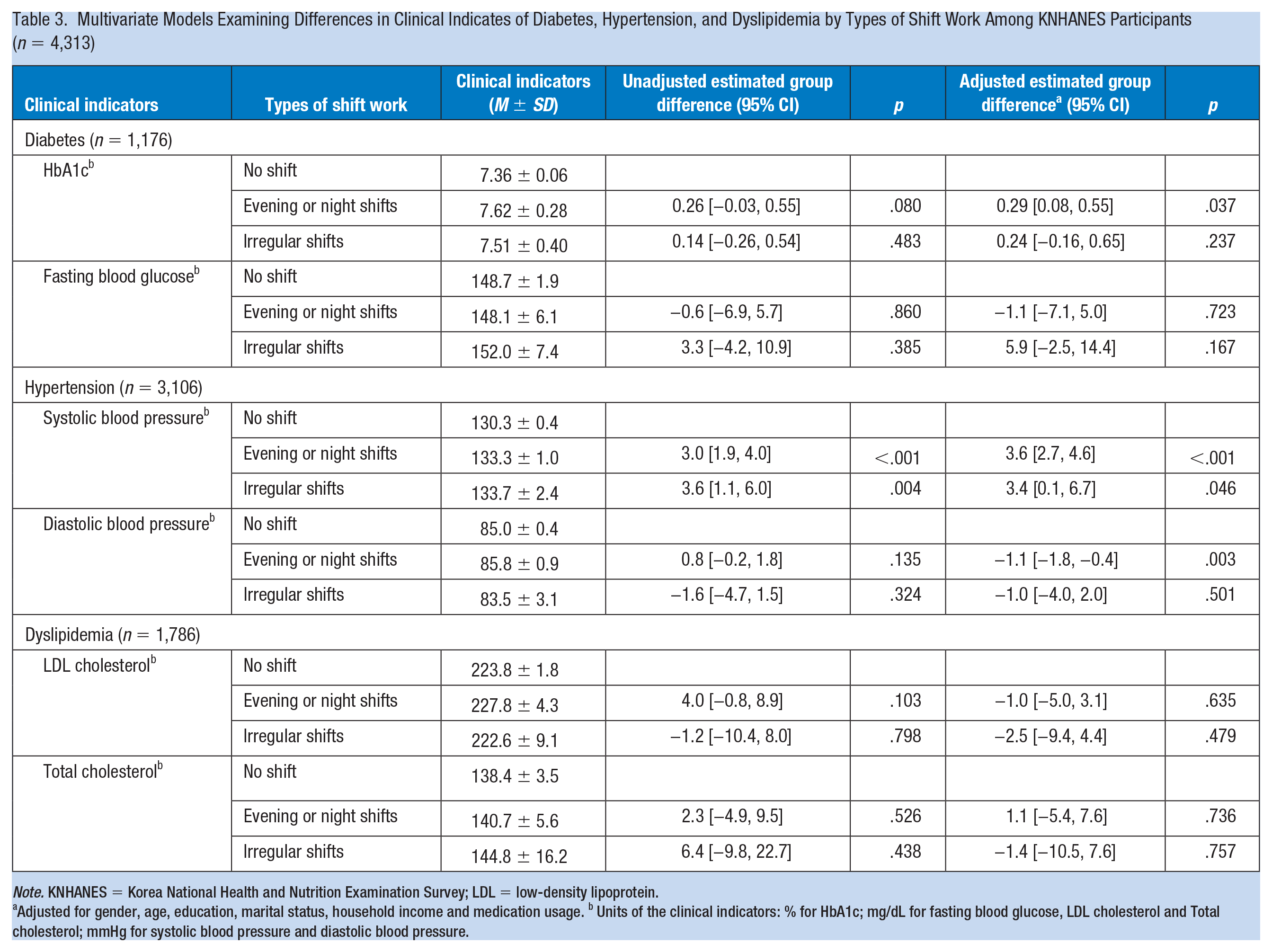
Note. KNHANES = Korea National Health and Nutrition Examination Survey; LDL = low-density lipoprotein.
Adjusted for gender, age, education, marital status, household income and medication usage. b Units of the clinical indicators: % for HbA1c; mg/dL for fasting blood glucose, LDL cholesterol and Total cholesterol; mmHg for systolic blood pressure and diastolic blood pressure.
Discussion
In this study, we found that clinical indicators were worse in workers with diabetes, hypertension, or dyslipidemia who worked for more than 40 hours per week compared with patients who worked less than 40 hours per week. Shift work, including evening or night shifts, has been associated with less control of clinical indicators in diabetic and hypertensive patients. The difference in clinical values in this study is significant both clinically and statistically; when there is a change in health behavior, such as exercise or diet control, glycated hemoglobin changes to near 0.15 (Benham et al., 2020), and according to the 2018 U.S. hypertension guidelines, losing 1 kg of body weight could lower systolic or diastolic blood pressure by 1 mmHg. This evidence suggests that working hours and shiftwork may adversely affect the management of chronic diseases.
This relationship could be explained in two ways. First, effective management of chronic diseases requires good health behaviors such as proper diet and exercise (Kirwan et al., 2017; Quick et al., 2013). In addition, proper sleep and weight management may also affect the management of chronic diseases (Cohen, 2017; Igel et al., 2018; Thomas & Calhoun, 2017; Van Gaal & Scheen, 2015). Shift work and overwork make it difficult to manage such health behaviors (Buchvold et al., 2015; Virtanen et al., 2015). In other words, these factors may adversely affect clinical indicators for patients with persistent diseases who are overworked or have worked on shift. Second, because the socioeconomic status is worse for those who work shifts or overwork, chronic disease may not be managed sufficiently under those conditions. We controlled our analyses of clinical indicators with an adjustment for socioeconomic status which still showed significant differences.
Long working hours have been associated with adverse health outcomes in previous studies. Overwork was found to be associated with increased blood pressure, including those of advanced age and those with work stress (Liu et al., 2019; Yoo et al., 2014). The incidence of diabetes has also been associated with overwork, especially in those with low socioeconomic classes (Kivimäki, Virtanen, et al., 2015). Moreover, the risk of cerebrocardiovascular disease may be higher in personnel with long working hours (Jang et al., 2015; Lin et al., 2018). In this study, shorter working hours had better clinical outcomes for diabetes, hypertension, and dyslipidemia. With attention to overwork conditions, the Occupational Safety and Health Act was enacted in many countries to prevent the occurrence of overwork-related cardiovascular disease (Chang & Lin, 2019; Kim et al., 2019; Yamauchi et al., 2017).
In the larger cohort, shift work was associated with diabetes and dyslipidemia, after adjustment for sociodemographic factors (Tucker et al., 2019). Shift work may also be connected to higher rates of hypertension (Ferguson et al., 2019). However, the impact of shift work on cardiovascular disease is controversial. Most studies report that shift work adversely affects cardiovascular disease (Torquati et al., 2018; Wang et al., 2018). In contrast, according to Hublin et al. (2010), their study results did not support an association between shift work and cardiovascular morbidity. In our study, shift workers with evening or night shifts showed poor clinical indicators, in line with findings by others that suggest that shift work may adversely affect the management of chronic diseases. Further studies on the effects of shift work are needed to corroborate our observations and provide more evidence of the impact and influence of shift work on health and deleterious health conditions.
The present retrospective study has some limitations worth noting. First, this study was unable to identify a causal relationship between working hours, shift work type, and disease management in patients with hypertension, diabetes, and dyslipidemia as the study design was cross sectional. Thus, prospective cohort studies are required to investigate possible causal relationships or the impacts of working hours and type of shift work on these outcomes. Second, we adjusted for medication use but we could not adjust for key factors such as the number of medications taken or the duration of illnesses. Third, there were statistical differences in our study results; however, it might not be clinically relevant. Finally, we did not reflect the specific type of work the respondents were engaged in. According to previous literature, the actual type of work may have an impact on health (Kawabe et al., 2015; Mościcka-Teske et al., 2017), so it is necessary to conduct further research which considers the type of work performed.
Despite the abovementioned limitations, our study has meaningful strengths. Our findings suggest the importance of controlling overwork and shift work in the management of chronic diseases, as there are an increasing number of patients with chronic illnesses. Data from future prospective studies of the effects of overwork and shift work on the chronic disease management should be presented in the development of national regulatory policies/legislation for overwork and shift work in prevention of exacerbation of diseases.
Implications for Occupational Health Practice
Occupational health managers or practitioners play a pivotal role in promoting the health of workers with chronic disease. Occupational health managers could also plan health promotion programs that are appropriate for people with different types of work, such as overwork or shift workers. In addition, occupational health managers may anticipate the adverse effects of overwork and shift work and may ask the company for additional health checks. Occupational health managers can inform employers of the health consequences of overwork and shift work and provide guidance on how to implement workplace health care. Findings from our research could provide evidence for this guide.
Applying Research to Occupational Health Practice
This Korean study including a national sample of workers provides an understanding of overwork and shift work influences on management of chronic disease in workers. Workers with chronic illnesses may have difficulty managing chronic diseases related to overwork or shift work. To improve the health of workers with chronic diseases, it is necessary to maintain reasonable working hours and reduce shift work. In addition, workplace interventions that target shift workers with chronic disease are needed to help workers maintain their health and remain at work.
Footnotes
Author Contributions
EunKyo Kang, the only author, contributed to the study concept and design, analysis and interpretation of the data, statistical analysis, and interpretation of the study results and wrote the paper. The author confirmed the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
EunKyo Kang is an assistant professor at Seoul National University Hospital, working in the public health field. She has mainly researched workplace health care, health care for chronically ill patients, and public health.