
Abstract
Background:
Stress affects U.S. healthcare workers (HCWs) and costs US$191 billion annually. About 30% to 50% of healthcare providers report burnout. Based on an assessment of a U.S. rural hospital system, 94% of workers experienced negative health consequences. We conducted a quality improvement (QI) project for the purpose of implementing a stress management program for HCWs in a hospital system.
Methods:
A total of 500 HCWs were informed of the program through hospital communication channels. Using the Plan–Do–Study–Act (PDSA) process, we screened workers presenting to the occupational health clinic for care. Project team members recruited other workers for stress screening throughout the organization. Interventions included contacting workers with elevated scores on the Perceived Stress Survey (PSS; N = 213). The nurse practitioner scheduled them for a shared-decision-making (SDM) appointment (N = 33) where workers were informed of and encouraged to participate in stress reduction activities. Surveys were used to assess effectiveness of SDM appointments and the stress reduction activities. After each 2-week PDSA cycle, interventions were adjusted.
Findings:
Of the 42% (N = 213) of workers who were screened for stress, 24% (n = 52) had elevated scores. Fifty percent (n = 26) completed an SDM appointment. Participants reported an 86% assurance level that they would use personalized stress management plans. Participants utilizing the interventions (n = 271) reported 25% to 72% reduced stress levels.
Conclusions/Application to Practice:
This successful project, in a rural setting, included workers across job classifications. Team engagement, PSS screening, SDM opportunities, and stress management activities were project strengths. This low-cost project can be replicated.
Background
In 2015, the American Psychiatric Association reported 120,000 deaths in the United States and US$191 billion in annual healthcare costs resulting from workplace stress (American Psychiatric Association & Center for Workplace Mental Health, 2019; Goh et al., 2015). Among healthcare workers (HCWs), more than 50% of U.S. physicians, 30% to 50% of advanced practice providers, and 33% of nurses have reported burnout symptoms (Lyndon, 2016; Reith, 2018). In their 2019 National Physician Burnout, Depression, and Suicide Report, Medscape reported that from more than 15,000 physician respondents, 42% reported burnout, and 14% stated they had experienced thoughts of suicide (Kane, 2019). These findings indicate a significant toll on healthcare providers, which have also been shown to have a negative impact on the quality of patient care (Dewa et al., 2017).
In their 2017 systematic review and meta-analysis, which looked at interventions to reduce physician burnout, Panagioti et al. (2017) reported a small but significant reduction in burnout among physicians who participated in mindfulness-based stress reduction, exercise, and stress management educational programs. Further reductions in burnout were reported by physicians who also had access to organizational interventions, including scheduling adjustments, more autonomy, and improved teamwork. Ruotsalainen et al. (2015), in a systematic review of 54 randomized and four nonrandomized studies, reported that the most effective interventions for managing HCWs’ stress included cognitive-behavioral training and mental and physical relaxation. Organizational changes, such as scheduling adjustments, also brought some improvement, but with less effectiveness. Koinis et al. (2015) also found that many HCWs lacked effective workplace stress reduction strategies. Conversely, those with access to stress management programs benefited from workplace opportunities to receive education on stress management and reduction techniques.
Applications to Professional Practice
The occupational health professional working together with the administrators of healthcare facilities should ensure that HCWs have holistic wellness programs. The OHN-NP is an excellent resource for leading a project implementation team. Forming an interdisciplinary, multiskilled team will contribute to completing a system-wide, comprehensive needs analysis. A diverse team improves implementation by providing information throughout the organization among various departments and workers. Utilizing evidence-based strategies for team engagement improves communication and progress. Many healthcare organizations have annual wellness events for workers, and promoting mental wellness and stress management should become a part of those programs that have previously focused on physical health exclusively. Screening workers, assisting them to develop personalized stress management plans, and implementing educational and person-oriented, on-site stress reduction activities can be accomplished through the OHC. In addition, the OHN-NP can refer workers to specialists if more intensive, individual treatments are needed.
A rural Illinois hospital organization conducted an independent wellness assessment of their workforce in 2015. Of all the employees, managers, and administrators (N = 365) who were surveyed, 94% of respondents (n = 255) stated their health had been negatively affected by stress in the previous year. Respondents also stated that stress was their number one health concern (Cleveland Clinic Wellness Enterprise, 2015).
The findings from the literature were used to support a worksite intervention program in a rural health care organization in which we aimed to implement a stress management program for our workers.
Method
Overview of Intervention Worksite
This worksite project took place in 2019 in a rural healthcare organization, Horizon Health, which employed approximately 500 workers. Based on the findings from a 2015 independent assessment of wellness program needs, we administered a survey to a small group (n = 15) of workers that revealed 60% had not received information about stress management from their employer, 93% desired information, and 40% were dissatisfied with access to stress management at work. A quality improvement (QI) project was therefore developed with the purpose of implementing an effective stress management and reduction program using four, 2-week Plan–Do–Study–Act (PDSA) cycles, spanning a total of 8 weeks for initial implementation. This program was coordinated through our rural occupational health clinic (OHC) with a goal of having a 20% minimum participation rate among the hospital workers. At this time point, no stress management program had existed within this organization. The organization aimed to have a minimum of 100 HCWs participate in a newly created stress management program.
Four core interventions were planned as follows: Step 1: using a project team to disseminate project information and recruit as many workers as possible throughout the 8-week implementation process; Step 2: screening all participating workers for perceived stress levels using the Perceived Stress Survey (PSS; Cohen et al., 1983); Step 3: offering shared-decision-making (SDM) meetings that included the occupational health nurse practitioner (OHN-NP) and workers with elevated PSS scores to discuss evidence-based ways to decrease or manage stress, and to educate them about available on-site alternatives for stress management; and Step 4: offering on-site stress reduction activities such as education sessions, a relaxation room, and yoga classes.
This worksite project was excused from review by the Institutional Review Board at Frontier Nursing University because it did not qualify as human subjects’ research and met federal requirements for QI. There are no conflicts of interest or outside funding sources to report.
Worksite Description
At the time of this project, the hospital system consisted of three rural outpatient clinics and a critical-access hospital, which is a designation given by the Centers for Medicare and Medicaid Services (CMS) to hospitals when federal funds are provided to keep critical health care services in rural communities (Rural Health Information Hub, 2020). All clinic and hospital workers, including physicians, advanced practice providers, nurses, and supporting staff, in addition to nonclinical staff, were invited to participate in screening, SDM appointments, and on-site stress reduction activities.
Project Team
The purpose of this QI project was to develop an effective stress management and reduction program, implemented through a rural OHC, and have a minimum of 20% HCW participation. A project implementation team was comprised of a hospital social worker, Chief Nursing Officer, two OHN-NPs, two registered nurses (RNs), a licensed practical nurse, and a pharmacy technician. Project team members were chosen from volunteers, and across disciplines, to help recruit workers to participate throughout the organization. The team assisted the project leader, an OHN-NP, in the planning and implementation of interventions.
Project team engagement and communication was important for project success. We employed recommended engagement approaches such as huddles, meetings, team-building activities, feedback, and recognition (Hansell & Kirby, 2015; Harvard University Human Resources, 2019; van Dongen et al., 2018). This project team held a huddle meeting every Monday morning, and minutes were emailed to all members following the meeting. This time was devoted to reviewing our progress, acknowledging individual team member accomplishments, and reminding each team member of available resources and upcoming educational programs so they could disseminate information throughout the facility. In addition, the project team leader sent personalized thank you notes, a team newsletter, and small gifts, such as candies or hand lotions, to each team member on Wednesdays to improve team engagement, increase communication, and express appreciation. Project team members completed surveys bi-weekly using the Goals, Roles, Processes, and Interpersonal (GRPI) Analysis to assess team engagement and satisfaction (Ogrinc et al., 2018).
Project Framework
The Institute of Medicine states that quality initiatives within healthcare organizations should focus on one or more of six specific domains such as safe care, effective care, patient-centered care, timely care, efficient care, and equitable care (Agency for Healthcare Research and Quality, 2018). The domain for this QI project was effective care which is defined as providing evidence-based services to those who could benefit. The QI project was then developed and implemented using four, 2-week PDSA cycles. Data-driven changes, in the attempt to make improvements as the project progressed, were made at the end of each of those 2-week cycles once qualitative and quantitative data were reviewed (Ogrinc et al., 2018).
Four-Step Project Process
Step 1: Recruiting workers to participate
Information about the project, and who to contact to sign up to participate, was included in system-wide emails and the hospital weekly newsletter. On the first day of project implementation, project team members visited each department of the main campus at Horizon Health. Flyers containing project details were distributed to all available workers, and hand massages were offered using aromatherapy lotions. Mocktails and chocolates were distributed, and workers were asked to complete a PSS form. In addition, HCWs presenting to the OHC were invited to participate and, upon agreeing, were screened using the PSS. Employees who were not reached through the original department visits, or seen in the OHC for physicals, injuries, or other care, were recruited by members of the project team who continued to visit hospital departments and distribute information about the project throughout the implementation cycles. They also administered the PSS to workers and turned those into the project team leader for review. In PDSA 2, each team member was assigned certain departments to target for recruitment. In PDSA 3, team members were given their individual recruiting statistics, and competitions with small prizes were added to encourage further recruiting. In PDSA 4, individual team members’ recruiting achievements were recognized through a hospital-wide newsletter to encourage their continued recruiting efforts. In addition, Survey Monkey was used to reach workers, especially advanced practice providers and physicians, for recruitment and screening.
Step 2: Assess stress using the PSS
The PSS is a 10-question survey on which workers rated their perceived stress over the previous month using a Likert-type scale of 0 through 4, where 0 corresponds to never, 1 corresponds to almost never, 2 corresponds to sometimes, 3 corresponds to fairly often, and 4 corresponds to very often. Three examples of survey questions include the following: “How often have you been upset because of something that happened unexpectedly?” “How often have you felt unable to control the important things in your life?” and “How often have you felt nervous or stressed?” The survey has been widely used in research to measure perceived stress for decades and is considered psychometrically acceptable, reliable, and valid (Lee, 2012). For the purposes of this project, a score of 27 or above was initially used to define elevated stress. This triggered a follow-up email or phone call from the OHN-NP to the worker to invite them to an SDM appointment. In PDSA 2, the project team met to discuss specific departments and workers most likely to be experiencing a highly stressful work environment. Team members then concentrated on reaching those workers for screening. In PDSA 3, we expanded our follow-up efforts to include workers with lower scores on the PSS, reduced to 24 from 27, and those additional workers were then contacted by the OHN-NP for an SDM meeting. In PDSA 4, the trigger score was further reduced to 23. This now meant those with lesser perceived stress, although still considered moderate stress according to the PSS, would receive follow-up.
Step 3: Offering SDM
The OHN-NP project lead contacted participants scoring high on the PSS to arrange an SDM meeting to formulate an individualized stress management plan. They met with stressed workers who agreed to participate. Evidence-based methods for stress management and stress reduction were shared with these workers, and workers were made aware of newly implemented stress management interventions available at the worksite. An adaptation of the Ottawa Personal Decision Guide, a widely used guide for individuals making health-related decisions, was used to assist participants in developing a personalized stress management plan (O’Connor et al., 2015). Afterward, an adaptation of the SURE tool was used to measure the workers satisfaction with the personalized stress management plan they had created in cooperation with the OHN-NP. SURE stands for S- “Sure of myself,” U- “Understand information,” R- “Risk-benefit ratio,” and E- “Encouragement or enough information to make a choice?” (O’Connor & Legare, 2008). The SURE tool is another tool with acceptable validity and reliability (Parayre et al., 2014). During this project, it was used to measure not only the participant’s level of satisfaction with their personalized plan but also their likelihood to actually utilize that plan.
In PDSA 2, the SDM tool was slightly revised to make it easier for the workers and providers to use. In PDSA 3, the OHN-NP began offering some group SDM meetings in addition to personal meetings, and in PDSA 4, we targeted the emergency room staff for a group SDM meeting so they could offer each other peer support and the OHN-NP could talk with them as a group about ways to manage and reduce their stress.
Step 4: On-site stress reduction activities offered
On-site stress management and reduction activities were created and offered to all workers. Workers could choose from interventions which included a relaxation room equipped with a massage chair, aromatherapy, relaxation/meditation videos, and written handouts on stress management topics. Additional options included weekly yoga/mediation classes, and weekly Lunch and Learn sessions on topics such as mindfulness, resilience skills, progressive muscle relaxation, workplace trauma, and humor as a tool to reduce stress. A pre- and post-Likert-type-scale survey that we developed was completed by participants using the relaxation room to measure their stress levels, and a similar tool was used to measure the effectiveness of yoga classes. Educational sessions were evaluated by the participants’ completion of a survey assessing presenter effectiveness and content practicality.
In PDSA 2, the relaxation room activities were expanded to include a CD player and meditation and mindfulness CDs. In PDSA 3, we created a second relaxation room to be used by our medical coders and billers at their satellite work location (Financial Operations Center). In PDSA 4, we had a special emphasis on the practice of mindfulness. A special newsletter was distributed to workers with video links to educational materials on mindfulness, YouTube links were posted in the relaxation room to mindfulness educational videos, and a specialist in mindfulness practice was brought in to teach at the Lunch and Learn session.
Team PDSA process
Throughout the project, the effectiveness of interventions was studied by completing daily field notes, reviewing all collected surveys, compiling data into aggregate data charts, and plotting mean data points onto run charts every 2 to 3 days. Run charts were then studied for runs, shifts (meaning at least seven serial points occurring on the same side of the median), and trends (meaning at least seven points consistently rising or declining; Ogrinc et al., 2018). Based upon the findings from this continuous review, at the conclusion of each 2-week PDSA cycle, needed changes were made to interventions, and a new cycle began. Field notes, team discussions, and free-text feedback sections on surveys served as qualitative data. Aggregate data charts and run charts, showing mean percentages with median and goal values displayed, served as quantitative data.
The project team attempted to monitor for any unintended negative consequences occurring from the implementation of this project. One concern was that managers may be dissatisfied with potential interruptions of the workers’ workflow caused by participation in the project’s interventions. A balancing measure, specifically managers’ satisfaction, was chosen to assess management’s perceptions of benefits or disruptions caused by the program. A survey with Likert-type-scale questions and an area for free text was emailed to, and collected bi-weekly from, managers who were willing to complete the surveys.
Consistent efforts were made to maintain the accuracy and completeness of all data collected. Table 1 describes the operational definitions. Qualitative and quantitative data were collected and evaluated using field notes, run charts, and aggregate data reviews; data-driven changes were made, both during and after each cycle. These small changes were made during each PDSA cycle in response to the reviewed data throughout the project implementation.
The Measures and Results Employed During the Stress Management Process
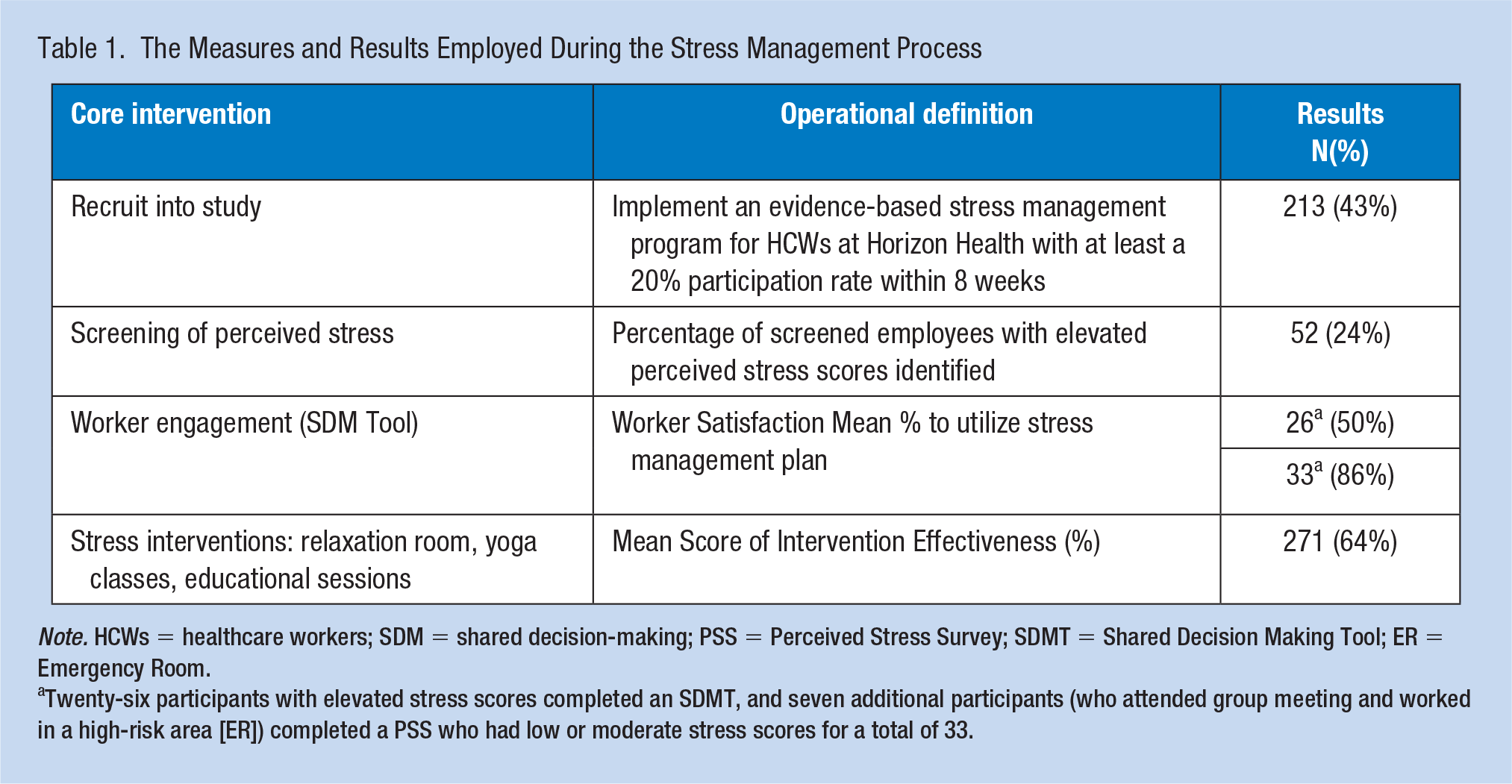
Note. HCWs = healthcare workers; SDM = shared decision-making; PSS = Perceived Stress Survey; SDMT = Shared Decision Making Tool; ER = Emergency Room.
Twenty-six participants with elevated stress scores completed an SDMT, and seven additional participants (who attended group meeting and worked in a high-risk area [ER]) completed a PSS who had low or moderate stress scores for a total of 33.
Findings
Step 1: Recruiting Participants
Our team goal to recruit at least 20% (n = 100) of Horizon Health employees was exceeded, as we had a total of 42% (n = 213) of employees participating. Twenty-four of these workers were screened within the OHC when they presented there as patients, whereas the remaining 189 were recruited by project team members. Some participants only completed screening, whereas others went on to use the created stress management activities provided on-site. The initial kick-off activities resulted in 15% (n = 75) of workers being recruited into the project. Reaching out by use of Survey Monkey during the fourth PDSA cycle also greatly increased participation recruitment rates from 30% (n = 150) to 42% (n = 213) of workers.
Step 2: Assessing Stress Using the PSS
At the conclusion of the 8-week implementation, 24% (n = 52) of screened workers had been identified as having elevated stress. Redesignating how we defined elevated stress in PDSA 3, from a PSS score of 27 to 24, naturally increased the number of workers being defined as having elevated stress. We further decreased the definition to a score of 23 by PDSA Cycle 4. This also triggered an increased number of workers being contacted and invited to participate in SDM meetings. However, when averaged in with the scores from the previous PDSA cycles, the actual percentage of workers identified with elevated stress fell from 27% at the end of PDSA 2 to 24% at the end of PDSA 4. This was an unexpected finding, as we had expected that the more workers we screened, the higher the percentage of stressed workers we would identify.
Step 3: SDM
Among the 52 workers who had elevated PSS scores, 50% (n = 26) completed an SDM appointment with the OHN-NP. In addition, seven other workers had requested, and completed, an SDM appointment to proactively develop personalized stress management plans. Results from the SURE tool revealed that workers’ satisfaction scores with the SDM appointments were at 86%, 11% higher than the project goal.
Step 4: On-Site Stress Reduction Activities
Process scores, which reflected success at getting workers to complete evaluation forms of the intervention for which they participated, improved throughout the course of all four PDSA cycles from 0% baseline to 84% at project completion. Overall outcome scores, describing intervention effectiveness, improved from 33% baseline to 64% at the project end, with more than 200 visits to the relaxation room, 27 combined attendances at yoga, and nearly 100 combined attendances at the educational sessions. Effectiveness scores ranged from 25% to 72% over the course of all four PDSA cycles. Effectiveness scores were combined and averaged for the relaxation room, yoga classes, and educational sessions. Surveys were easily distributed and collected at yoga classes and educational sessions, but more difficult to collect from those using the relaxation room because workers used this independently and without supervision. Scores increased each week as additional interventions occurred; on Mondays and Tuesdays, the relaxation room was available exclusively; on Wednesdays yoga classes were also offered; and on Thursdays or Fridays, the educational sessions occurred. The addition of a second relaxation room, at a satellite location during Cycle 3, increased access and participation rates, and effectiveness scores trended higher with each PDSA cycle.
Team Processes
Process scores, which measured attendance at meetings, or receipt of electronic communications was initially erratic because individual schedules and availability were variable. Most interactions were changed to electronic and face-to-face, which worked better for this team, resulting in a shift and trend on the process run chart. Team engagement scores were measured through a Likert-type-scale survey bi-weekly and ranged from 93 to 98. The team worked well together, and satisfaction scores rose from 50% at baseline to 98% at project completion.
The balancing measure showed that management satisfaction did not decrease due to the program. Fortunately, management satisfaction actually rose substantially from a baseline of 20% to 97% at project completion. Efforts were made consistently by the team leader to account for any missing data.
Discussion
The participation aim was exceeded as 42% of employees participated in the stress screening. The OHC staff and the project team screened HCW throughout the organization and brought about success. Effective, consistent project team communication was a strength of this project. Team satisfaction scores remained high with the use of contests, small incentives, prizes, and recognition. In addition, worker engagement through individual and group SDM meetings proved to also be a strength of this project. SDM outcome scores were high, and despite a small score decrease with the addition of group SDM meetings, these meetings did improve participation rates, efficiency, and social support opportunities. The creation of relaxation rooms provided a means for improved stress levels from 25% to 38% and reinforced a culture of caring and wellness within the Horizon Health organization. Yoga classes further increased effectiveness rates to 36% to 56%, and educational sessions raised effectiveness scores further to 60% to 72%.
There were limitations that included the rural setting, predominant Caucasian sample, and use of some nonvalidated measurement tools. This could limit study generalizability. Although efforts were made to gather complete data, the potential for bias existed because participants were not always completing surveys anonymously. Various working conditions, hours, and other confounding factors could affect individual employees’ stress perceptions. Efforts were made to communicate opportunities for participation throughout the facility through newsletters and unit staff meetings, and by meeting with leaders and administrators to generate support for the project. The short time frame of this project and small sample size created further limitations.
HCWs’ well-being can be improved by implementing effective stress management programs. The potential cost savings from reduced burnout, absenteeism, and turnover make these inexpensive interventions sustainable. Occupational health staff can orchestrate screening, SDM, and stress management interventions that increase staff resilience and address the crisis of elevated stress and burnout among HCWs. Increased awareness and understanding of interventions could be established through further studies. Horizon Health plans to screen employees annually provide appropriate follow-up and continue project interventions through the OHC. Monthly educational sessions on stress management, weekly yoga classes, and the relaxation room will continue for workers. Screening of HCW is an important first step in identifying elevated stress and promoting a holistic view of employee wellness (Brand et al., 2017). The Horizon Health screenings were conducted through an OHC by reaching out to employees in their respective departments. Although fewer than expected participants had elevated PSS scores, recent efforts at Horizon Health to promote a culture of caring and wellness likely affected previous assessment findings.
Individual and group SDM meetings assisted HCW in developing a stress management plan the worker felt they understood and could use to manage or reduce their stress. Studies have shown that group SDM can improve efficiency and provide increased social support without causing harm (American College of Obstetricians and Gynecologists, 2018).
Person-oriented stress interventions, including relaxation rooms, yoga classes, and education on mindfulness, meditation, and physical and mental relaxation, effectively reduced HCW perceived stress levels; this is consistent with previous studies (Ruotsalainen et al., 2015). The project implementation demonstrated to employees an organizational commitment to their improved overall well-being. The benefits of addressing elevated stress with effective interventions can include decreased turnover, health costs, absenteeism, and injuries (The American Institute of Stress, 2019). The financial impact of reducing the negative stress and burnout on HCW cannot be overstated, given that the cost of replacing just one RN averages US$52,100 (NSI Nursing Solutions, Inc., 2019).
Footnotes
Acknowledgements
A special thank you to the project team members and intervention educational presenters: Sara Spesard, FNP; Tiffany Turner, FNP; Abby Barrett, LSW; Leighsa Cornwell, RN, CDE; Kyle Mohon, Pharmacy Technician; Somer Nagrodski, RN; Tiffany Sallee, LPN; Karyssa Haase; John Holley; Barbara Kendall; Johanna Westin; Ellen Auten; Stephanie Lorenzen; Beth Graham; and John Christian White.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Crystal H. White is a family nurse practitioner within the occupational medicine department at Horizon Health in Paris, Illinois; adjunct faculty at Ferrum College in Ferrum, Virginia; and Clinical Evaluator at Indiana Wesleyan University in Marion, Indiana. She was the project leader for this Quality Improvement Initiative.
Niessa Meier is a member of the Doctorate of Nursing Practice Clinical Faculty at Frontier Nursing University in Hyden, Kentucky, and a certified nurse midwife. She served as the faculty advisor for this project.
Charlotte Swint is an associate professor in the MSN and DNP programs at Frontier Nursing University in Hyden, Kentucky. She served as the project mentor through the planning and implementation of this project.