
Abstract
Background
Cryogenic burns induced by coolant gases used in refrigerators and air conditioners are rarely encountered, despite the wide use of these gases. To date, only a few cases have been reported in the literature. This study examined the occupational circumstances leading to such injuries, relevant injury sites, types of chemicals involved, and treatment measures.
Methods
This study was conducted in a tertiary burn center in India between March 2015 and March 2019. The demographic details, chemicals involved, and burn regions and characteristics were analyzed.
Findings
There were 15 burn cases all involving injury to the hand. All injuries were managed initially with dressings and nonoperative management. One patient required anti-edema therapy with limb elevation and fingertip debridement, while another patient required skin grafting. All patients had satisfactory hand function after treatment.
Conclusions/Application to Practice
Cryogenic burn injuries caused by refrigerants are rare, and their etiology varies considerably. Exposure time is the primary factor that determines burn depth and severity; hence, reducing exposure time is important in first aid. Our findings suggest that after exposure, the patient should be treated in a specialized burn center. Adequate knowledge regarding the pathophysiology of these types of burn injuries and their management is necessary; otherwise, misjudgments in the treatment plan can lead to adverse consequences.
Background
Cryogenic burn injuries can range in severity from minor skin damage to deep frostbite-type burns. The severity of these burns is directly proportional to the area involved, the contact time, and the temperature gradient between the coolant gas and the intact skin (Wisler et al., 2010). Refrigerant gases, first developed in the early 1930s, were also occasionally used as aerosol propellants, dry cleaning agents, and chemical excipients (Sever et al., 2008). Gases previously used in refrigerators and air conditioners included ammonia (R717), sulfur dioxide (R-12), and freons (hydrochlorofluorocarbons). These gases were later found to be harmful to the environment and have been replaced in modern household appliances by hydrofluorocarbons like tetrafluoroethane (R-134a), Puron (R-410A), and difluoromethane (R-32), which are more environmentally safe but still hazardous to handlers (Wisler et al., 2010). Cryogenic burns caused by these compressed gases occur most commonly among workers involved in manufacturing and transportation, and among those involved in the maintenance and repair of appliances such as air conditioners and refrigerators (Astrom et al., 1987). Contact with these cryogens can cause cold burn injuries to the cutaneous tissues and to exposed body parts such as the eyes (Wisler et al., 2010). In addition, it can cause ice crystals to form in the water in the tissues, causing injury at the molecular level (Edling et al., 1990). Sudden explosion of these substances from a compressed liquid state into gas can also result in injury. In gaseous form, they can displace the oxygen in the environment; exposure to heavy vapors can cause suffocation, dizziness, weakness, fainting, and cardiac arrhythmia (Sjögren et al., 2002). The standard on-site first aid for those exposed to cryogens involves limiting exposure, washing exposed areas with running room-temperature water, shifting the patient to a well-ventilated area, and obtaining medical attention (Chaput et al., 2012).
Despite the widespread use of refrigerants, there are only a few reports on frostbite and other burn injuries caused by these substances (Wegener et al., 1991). In this article, we describe the circumstances, characteristics, outcomes, and complications of cryogenic burns caused by refrigerants in 15 patients treated at a tertiary burn center in India. We also discuss the current knowledge regarding such burns.
Methods
We conducted a retrospective review of outpatient and inpatient medical records at the Department of Burns, Plastic & Maxillofacial Surgery at Vardhman Mahavir Medical College & Safdarjung hospital, New Delhi, India between March 2015 and March 2019. We examined demographic details (age and sex), chemicals and gases involved, burn mechanism, burn area, and burn depth. Required approval was obtained for the study from the in-house institutional review board. All patients gave their informed consent to participating in this study.
Results
Fifteen cryogenic burns were reported during the study period. All patients were male, with a mean age of 28 years (Table 1), and all were of lower socioeconomic status according to the Modified Kuppuswamy Scale (Wani, 2019). All were daily wage laborers, with most (n = 10) working as mechanics on either refrigerators or air conditioners (33% each).
Summary of Patient Demographic Characteristics and Treatment
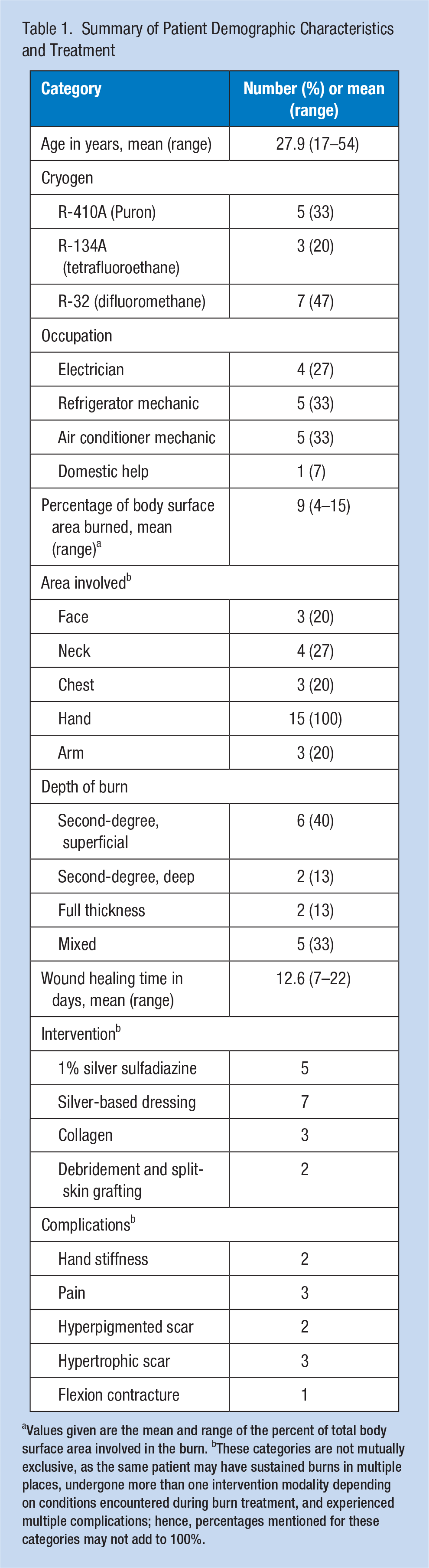
Values given are the mean and range of the percent of total body surface area involved in the burn. bThese categories are not mutually exclusive, as the same patient may have sustained burns in multiple places, undergone more than one intervention modality depending on conditions encountered during burn treatment, and experienced multiple complications; hence, percentages mentioned for these categories may not add to 100%.
All injuries were work-related refrigerant-induced cryogenic burns. Difluoromethane (R-32) was the most common refrigerant encountered (47%), followed by Puron (R-410A) (33%). The injuries were sustained during repair of house cooling equipment. Twelve (87%) injures occurred during refilling or repair of air conditioner condenser tanks, while two were sustained during refilling of refrigerant reservoir tanks. In all cases, patients had failed to follow standard precautions or wear personal protective equipment. All but one (n = 14) were not trained to handle refrigerants properly. When we inquired about their knowledge of cryogens and use of protective gear, all reported being unaware of the possibility of cold-related injuries and the appropriate first aid procedures.
The hand was the most common injury site (Figures 1 and 2). With regard to burn depth, second-degree burns were the most common assessment at presentation. The mean wound healing time was 12.6 days.

Burn conditions at presentation: (A) second-degree cryogenic burns of the right hand with blisters on the palm and flexor aspect of the fingers; (B) second- and third-degree cryogenic burns of the left hand involving the palm, fingers, and thumb; (C) Second-degree cryogenic burns of the right hand with blisters on the dorsal aspect of the fingers; (D) second-degree refrigerant burns involving the dorsum of both hands and fingers; and (E) a case of cryogenic refrigerant burns involving the face and neck.

Burn conditions after treatment: (A) healed hypopigmented cryogenic burn scars of the dorsum of both hands and fingers; early flexion contractures of the little and ring fingers of the right hand were managed with a splint and aggressive physiotherapy; (B) healed refrigerant burn scars involving the palm and thumb of both hands; (C, D) Follow-up photos of a cryogenic burn involving the dorsal and palmar aspects of both hands on post-burn Day 20, with satisfactory hand function; and (E) deep dorsal cryogenic burn wound on the dorsum of the left hand on post-burn Day 21; this burn required debridement and a split-skin graft for wound coverage.
For most patients (n = 12), toothpaste had been used as the first aid treatment by the injured and bystanders. When treated in our Center, we used various dressings which included silver sulfadiazine, wet collagen, and silver-based dressings for superficial wound treatment. We also conducted deep wound debridement of the dead tissue, as well as split-skin grafting for select patients. All patients received silver sulfadiazine cream dressings, physiotherapy, splinting, and scar prevention therapy, along with anti-edema measures, according to case requirements. Those patients whose wounds did not heal in 3 weeks were later treated with skin grafts. One patient required split-thickness skin grafting, while another required debridement of the fingertips and skin grafting for wound closure. Scar-related complications were observed in five patients. Chronic pain was reported in three patients, and stiffness of the interphalangeal and metacarpophalangeal joints of the hand was encountered in two patients. One patient developed early flexion contracture of the interphalangeal joints of the ring and little fingers, which was managed with physiotherapy and serial splinting. All patients recovered well after therapy and were rehabilitated to pre-injury function. All patients were followed up for 6 months.
Discussion
In this study, we reviewed the data of 15 patients over a period of 4 years who sustained cryogenic burns. In our analysis, the hand was involved in all cases, with the neck and forearm being the next most frequent parts injured. Koljonen et al. (2004) stated that the fingers are particularly susceptible to cryogenic burns. Sever et al. (2008) described similar patterns of injuries in a retrospective analysis of 17 patients, with most involving the hand. The hands are commonly involved because they are the area most likely exposed to cryogens in the course of work. The hands also have a thin soft tissue cover and an end-arterial blood supply, making them even more susceptible to cryogenic burns.
There is some debate regarding the effect of duration of exposure with regard to severity of tissue damage from exposure to refrigerants. Kumar and Chirayil (1999) were of the opinion that since refrigerant fluid can penetrate deep into the tissues, the superficial tissue’s appearance is a poor indicator of the injury’s extent and depth, which are usually severe. Unlike in thermal burns, refrigerants can continue to damage the tissues even after the exposure ends. Only two of our patients were initially assessed to have full-thickness burns. However, we had five patients who experienced scar-related complications, three who developed stiffness and early flexion contracture, and two patients underwent debridement and skin grafting. Second-degree burns of the hand do not usually lead to morbid scar-related complications and stiffness; these complications are usually encountered in deeper burns. In retrospect, it seems our initial assessments of burn depth as superficial were flawed and that many burns were more severe than they appeared at presentation. Hence, physicians should consider that their initial assessment of cryogenic burn depth might not be accurate and that the wound is likely to be deeper than it first appears.
Herndon (1996) and Imray et al. (2009) state that as a part of first aid, the patient should be removed from the area where the injury occurred, and refrigerant-soaked clothes should be removed to minimize contact. When the injured individual is brought to a health facility, the exposed area should be washed with saline and immediately rewarmed to 40°C to 42°C for 15 to 30 minutes. This temperature range must be achieved to avoid suboptimal rewarming at lower temperatures and burns at higher temperatures. Active motion during warming is helpful, but massage should be avoided because it can cause the injured skin to peel. Frostbite-like symptoms were not seen in our patients; rather, the wounds resembled thermal burns. Moreover, because of unfamiliarity with appropriate first aid measures, some patients had applied readily available substances like toothpaste before arriving at the health care facility; this should be avoided.
Hurley (1957) stated that in frostbite, a certain number of cells are injured irreversibly, but other cells surrounding this area are injured reversibly and may recover and survive if appropriate treatment is provided at the right time. However, in cryogenic burns, the damage is usually irreversible despite a smaller area of exposure. Immediate surgical debridement or amputation is not recommended until the line of demarcation is clear. Fasciotomy or escharotomy may be required when vascularity is compromised due to massive edema or circumferential involvement of the digits. In our patients, we waited for the depth of the burns and the demarcation between viable and nonviable tissues to become clear. Likewise, the dressing materials used should also change depending on wound depth. Collagen and silver-based dressings were used in most of the burns initially assessed as superficial. However, if the wounds later proved to be deeper, the use of collagen dressings was discontinued, and we switched to 1% silver sulfadiazine cream and other silver-based dressings. Once the line of demarcation appeared, we proceeded with definitive surgical interventions like debridement and skin grafting.
The use of prophylactic antibiotics is controversial and usually not recommended unless signs of infection develop. In our patients, no prophylactic antibiotics were used.
Özkaya et al. (2011) reported that hyperbaric oxygen therapy may successfully be used to treat cryogenic burn injuries. Hyperbaric oxygen therapy has been shown to increase the production of antimicrobial agents, reduce microbial proliferation, activate the immune system, and significantly improve the partial pressure of oxygen in reversibly damaged cells. However, we did not use hyperbaric oxygen in any of our cases because our medical center does not have the necessary equipment.
Although refrigerants are dangerous chemicals, most of the patients in our study were not formally trained to handle them, and none were wearing personal protective equipment when they were injured. Prevention is the simplest and best strategy for reducing morbidity due to cryogenic burn injuries. The first step should be to educate workers regarding the risk of injuries, appropriate protective precautions (eyewear, gloves, boots), and appropriate first aid (Uygur et al., 2009). Furthermore, cylinders containing compressed refrigerants should be kept in well-ventilated areas in an upright position according to the manufacturer’s instructions, and the task of transferring these chemicals should be performed by at least two persons.
In conclusion, brief exposure to refrigerants resulted in severe and deep burns among several of our patients. Although cryogenic burns are uncommon, it must be emphasized that the removal of injured individuals from exposure and transport to a specialized burn center is essential for treatment. The rarity of such cases compounds the lack of knowledge about treating these injuries, and the mismanagement of cryogenic burns might have grievous consequences. Furthermore, prevention and first aid measures must be taught to persons handling refrigerants as part of their occupational education.
Applying Research to Occupational Health Practices
Cryogenic burns are rare; very few cases have been reported in the literature. We examined the causes and treatment of 15 cases of cryogenic burns. All patients were men and sustained workplace injuries caused by refrigerants, with the hands being the most common burn site. Most injuries occurred during the refilling or repair of an air conditioner condenser tank. Of the 15 patiensts, 14 were not trained to handle refrigerants, and no standard precautions, such as wearing of personal protective equipment, were followed. The initial assessments of burn depth may have underestimated the true degree of burns sustained, as these injuries were painless. Removal from refrigerant exposure, transport to a specialized burn center, and subsequent anti-edema measures, analgesia, and rewarming remain the mainstay of treatment. The mismanagement of cryogenic burns may have grievous consequences. Prevention and first aid measures must be the frontline of cryogenic burn management.
Footnotes
Acknowledgements
The authors acknowledge the professional language editing services provided by the SAGE Author Services.
Author Contributions
D.K. contributed in the form of concept and design and drafting the manuscript. S.D., V.M., and R.R. contributed by drafting the manuscript, collection, and analysis of data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Suvashis Dash is Board cerified plastic surgeon trained from Vardhman Mahavir Medical College & Safdarjung Hospital, Delhi, India. He takes keen interest in Burns and reconstructive surgery.
Vamseedharan Muthukumar was a postgraduate intrainee in Plastic and Reconstructive Surgery in Department of Plastic, Burns & Maxillofacial Surgery, Vardhman Mahavir Medical College & Safdarjung Hospital, Delhi, India. His special interests are Burn and Diabetic Foot.
Rajkumar R is Board cerified plastic surgeon trained from Vardhman Mahavir Medical College & Safdarjung Hospital, Delhi, India. His areas of focus is burns and aesthetic surgery.
Durga Karki is professor, Department of Plastic, Burns & Maxillofacial Surgery, Vardhman Mahavir Medical College & Safdarjung Hospital, Delhi, India. She takes keen interest in Burns, Reconstruction, Brachial plexus and Aesthetic surgery.