
Abstract
Background:
There are adverse side effects associated with handling chemotherapy; however, using safe-handling precautions can minimize or prevent these potential effects. Despite availability of international guidelines for chemotherapy handling, adherence to precautions is below expectations. This study examined knowledge of safe-handling precautions among a sample of oncology nurses in Jordon.
Methods:
A cross-sectional study was employed that included a convenience sample of 153 oncology nurses. Oncology nurses from two hospitals completed the Chemotherapy Handling Questionnaire. Descriptive analysis, Spearman rank correlation coefficients, and regression analyses were performed to determine the predictors of precaution use when handling hazardous drugs among participants.
Findings:
We observed that age, number of patients for whom the worker administered chemotherapy per day, the number of patients receiving chemotherapy per day in the participant’s work unit, nurses’ knowledge about safe-handling precautions, perceived risk, perceived barriers, self-efficacy, organization influence/workplace safety climate, conflict of interest, and interpersonal influences were predictors of use of safe-handling precautions (adjusted R2 = .66, p < .001).
Conclusion/Application for Practice:
Several predictors for using safe-handling precautions were identified. Clinically, chemotherapy handling procedures should be evaluated frequently to identify barriers to safe practices and to improve worker safety.
Background
As direct patient care providers, nurses spend more time with patients than other health care professionals, serving as the gate keeper for patients during their cancer treatment journey (Westbrook et al., 2011). Previous literature suggests that cytotoxic drugs like chemotherapy may have compromised workplace safety in oncology wards in Jordon over the last three decades (Al-Azzam et al., 2015; Hazen et al., 2010). Safety standards for chemotherapy administration have been developed by the American Society of Clinical Oncology (ASCO) (Neuss et al., 2016) and the Oncology Nursing Society (ONS) (Conti-Kalchik et al., 2017). It is recommended that intensive educational program and clinical training, required by safety policies in cancer treatment centers or institutions, be employed to prepare nurses so they are competent in handling chemotherapeutic agents (Neuss et al., 2016). Cancer treatment centers in Jordan have no standard methods to evaluate the adherence and competencies of nurses regarding their handling of chemotherapy (Al-Azzam et al., 2015).
Evidence from previous studies indicate that chemotherapy drugs may contaminate work environments due to a deficit in knowledge and lack of compliance by nursing staff with regard to safe-handling (Polovich & Clark, 2012). This finding suggests a gap between current nurses’ practices and the evidence-based guidelines by ONS and ASCO. Continued education and evaluation of their knowledge and competencies may help to prevent or minimize unnecessary exposure to these hazards (Hon et al., 2015; Meade, 2014; Rizalar et al., 2012).
Nurses are primarily trained to protect their patients; unfortunately, the standards for chemotherapy administration developed by ASCO focus on patient safety rather than nurse safety (Polovich & Clark, 2012). Several factors have been identified to increase their risk for chemotherapy exposure, including a lack of policies by employers requiring safe-handling of these drugs and a lack of awareness and knowledge of safe practices among nurses (Boiano et al., 2014; Eisenberg, 2016; Friese et al., 2012; Walton et al., 2012). Some study findings indicate that a deficit in nurses’ compliance was positively associated with their limited knowledge of how to safely handle and administer these drugs (Khan et al., 2012; VerStrate, 2015). Different routes of contamination have been identified, including food, as well hand-to-mouth and dermal contact (Polovich & Clark, 2012). Occupational exposures to chemotherapeutic agents has been associated with health complications and serious illnesses among workers including dermatitis, abortion, fetal loss, chromosomal abnormalities, deoxyribonucleic acid (DNA) damage, and infertility (DeJoy et al., 2017; Lawson et al., 2013; Polovich & Clark, 2012).
In Jordan, the number of new cases of cancer have increased over the last decade (Abdel-Razeq et al., 2015), from 3,370 cases in 2000 to 5,409 cases in 2013 (60.5% increase over the 14 years) (Khader et al., 2018). It is the second leading cause of death after cardiovascular disease (Khader et al., 2018).
Cancer treatment modalities including surgery, radiation, and chemotherapy are widely available, and there is a sufficient number of specialized and trained medical, surgical, and radiation oncologists, Yet, there is a lack of nurses that specialize in cancer care (Abdel-Razeq et al., 2015). However, there is a shortage of certified oncology nurses, who are trained and specialized to meet the complex needs of cancer patients (Abdel-Razeq et al., 2015, 2020; Khader et al., 2018). Determining nurses’ competencies, adherence and knowledge with regard to chemotherapy handling are necessary for exposure prevention. The purpose of this study was to determine the predictors of practicing safe chemotherapeutic precautions among oncology nurses and to determine their level of knowledge pertaining to these practices.
Materials and Methods
We employed the Factors Predicting Use of Hazardous Drug Safe-Handling Precautions (PHDP) model (Lusk et al., 1997) as a framework to guide our work in which several factors were hypothesized as predictors for safe-handling precautions including knowledge, perceived risk, self-efficacy, perceived barriers, organization influence/workplace safety climate, and interpersonal influences.
A cross-sectional descriptive study was conducted, in which a 25- to 30-minute survey was administered in October 2018 to nurses who were employed in two governmental hospitals in Jordan. A convenience sample of 180 oncology nurses, who were (a) registered nurses and (b) administered chemotherapy as part of their job, were invited to participate.
Invitation posters containing information about the study methods, purposes, and significance of the study were distributed by the research team on the oncology units, nurses meeting rooms, rest rooms, and nurse manager offices. Unit managers and charge nurses were informed about the study approach and eligibility criteria for participation. The research team worked with a contact person in each unit that was responsible for questionnaire distribution and collection on their units. The participants were asked to return the completed survey to their contact person in a sealed envelope. No personal identifying information was collected (e.g., name, date of birth). Ethical approval was granted from AL-Zaytoonah University of Jordan and Ministry of Health ethics and research committees.
Chemotherapy Handling Questionnaire
The Chemotherapy Handling Questionnaire, developed by Polovich and Clark (2012), was used to measure chemotherapy handling practices. The questionnaire consists of nine subscales (predictors) including Chemotherapy Exposure Knowledge (12 items), Self-efficacy for Using PPE (six items), Barriers to Using PPE (13 items), Risks of Chemotherapy Exposure (three items), Organizational Influences (21 items), Perceived Conflict of Interest (six items), Interpersonal Norms (four items), and Interpersonal Modeling (three items). The instrument was valid and reliable when used among oncology nurses in a study by Polovich and Clark (2012), with Cronbach’s alpha for each scale ranging from .70 to .92. In this study, content validity was assessed by three experts in addition to the primary researcher. For this study, Cronbach’s alpha ranged from .72 to .91.
Chemotherapy Exposure Knowledge (12 items; for example, Oral forms of chemotherapy do not have the potential to be absorbed?) measured the participants’ knowledge about risks of exposure and effectiveness of precautions, with a possible score range from 0 and 12 (with items scored as correct = 1 and incorrect = 0), with a higher score indicating higher knowledge.
Barriers to Using PPE subscale (13 items; for example, There is no policy requiring PPE; I don’t think PPE works; and PPE makes me feel too hot) measures barriers of PPE. Participants could select 1 = strongly disagree to 4 = strongly agree, with the score range from 13 to 52 (higher score indicates higher perceived barriers).
Risks of Chemotherapy Exposure subscale (three items; for example, Chemotherapy exposure is not as harmful as some people claim; I am not worried about future negative health effects from chemotherapy exposure) with a Likert-type scale ranging from 1 = strongly disagree to 4 = strongly agree. Items were reverse-scored, with a higher score indicating greater perceived risk.
Self-efficacy for Using PPE subscale (six items; for example, I am confident that I can use PPE properly; I am confident that I can protect myself from chemotherapy exposure). Participants were asked to select from 1 = strongly agree to 4 = strongly disagree, with a summary score range of 6 to 24 (higher score indicating higher self-efficacy).
The Organizational Influences subscale (21 items; for example, chemotherapy gowns are readily available in my work area; all reasonable steps are taken to minimize hazardous job tasks; and on my unit, unsafe work practices are corrected by supervisors) with a Likert-type scale range from 1 = strongly disagree to 5 = strongly agree. The score ranges between 21 and 105, with higher score indicating better safety climate.
Perceived Conflict of Interest subscale (six items; Patient care often interferes with my being able to comply with using precautions, wearing personal protective equipment makes my patients worry), has a scale range from 1 = strongly disagree to 4 = strongly agree, with a sum between 6 and 24 (higher score indicating higher conflict of interest).
The last subscale was Interpersonal Influences (seven items; for example, How important is wearing PPE when handing chemotherapy to your coworkers), including the importance of PPE use to others (0 = not at all, 1 = sort of, 2 = a lot; higher score indicating higher belief that others think PPE is important), as well as Interpersonal Modeling (three items; for example, How often do the following people wear personal protective equipment when handling chemotherapy?) with responses of 0 = never to 3 = usually (higher score indicating higher use of PPE by coworkers).
The outcome measure (Safe-Handling Precaution Use) was measured using the Hazardous Drug Handling Questionnaire (Polovich & Clark, 2012). The questionnaire has four subscales including chemotherapy preparation (six items), administration (five items), disposal (five items), and excretion (six items). It has Likert-type scale range from 0 = never to 5 = always. Total precautions (mean score for Administration and Disposal) range from 0 to 5, with a higher score indicating greater use of safe-handling precautions.
Demographic information collected included age, education, years of nursing experience, years of oncology nursing experience, years of chemotherapy handling, number of patients for whom the participant typically administers chemotherapy to per day, and number of patients receiving chemotherapy per day at the participant’s work unit.
Data Analysis
Data were analyzed using SPSS (version 23). Descriptive analysis, including frequencies, percentages, mean values, and standard deviations, were calculated to describe the sample characteristics and study scales. Frequencies and percentages of correct answers to knowledge-based questions were calculated to determine the nurses’ level of knowledge regarding chemotherapy exposure. Bivariate correlations using Spearman rank correlation coefficients (rs) were performed to determine the relationship between the sample characteristics and hypothesized predictors and safe-handling precautions. Linear regression analysis was performed to determine the predictors of precaution use when handling hazardous drugs among participants (Hair et al., 2006). The independent variables, correlated with use of safe-handling precautions in the bivariate analyses, included in the initial model were age, number of patients to whom the participant personally administered chemotherapy per day, number of patients receiving chemotherapy per day at the participant’s work, knowledge, perceived risk, self-efficacy, perceived barriers, organization influence/workplace safety climate, conflict of interest, and interpersonal influences. Partial correlation and multicollinearity (variance inflation factor [VIF] and tolerance) were checked (Hair et al., 2006). Theoretically, tolerance refers to the assumption that the variability of one independent variable is not explained by another, and tolerance close to 0 reveals a problem with multicollinearity. A standard cut-off point is a tolerance value of 0.10 and for VIF, if the value is above 10. In this study, the tolerance value for each independent variable was above the ceiling tolerance value of 0.10, and the VIF results were less than 10. Variables that correlated with safe-handling practices were included in the parsimonious model also.
Results
A total of 153 participants completed the study survey (response rate = 85%) (Table 1). The majority of the participants had a bachelor’s degree in nursing (60.4%), with an average age of 28.57 years (SD = 4.25), the average years of experience in nursing was 6.02 (SD = 3.76), and their average years of experience in oncology nurses was 4.43 (SD = 3.70). Most were not certified for chemotherapy administration (60.4%).
Demographic Characteristics of Sample of Oncology Nurses (N = 153)
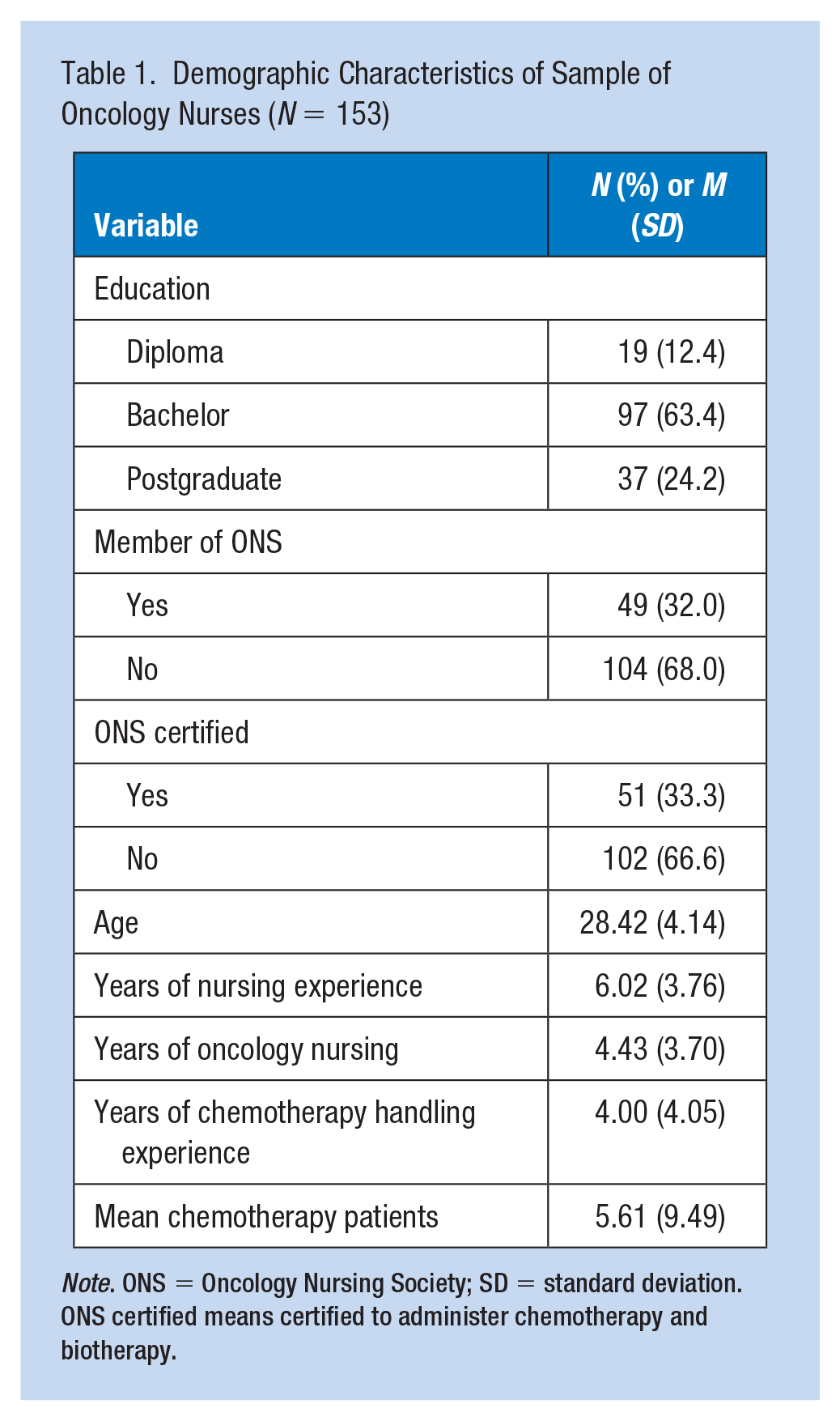
Note. ONS = Oncology Nursing Society; SD = standard deviation. ONS certified means certified to administer chemotherapy and biotherapy.
Nurses’ Knowledge About Chemotherapy Exposure
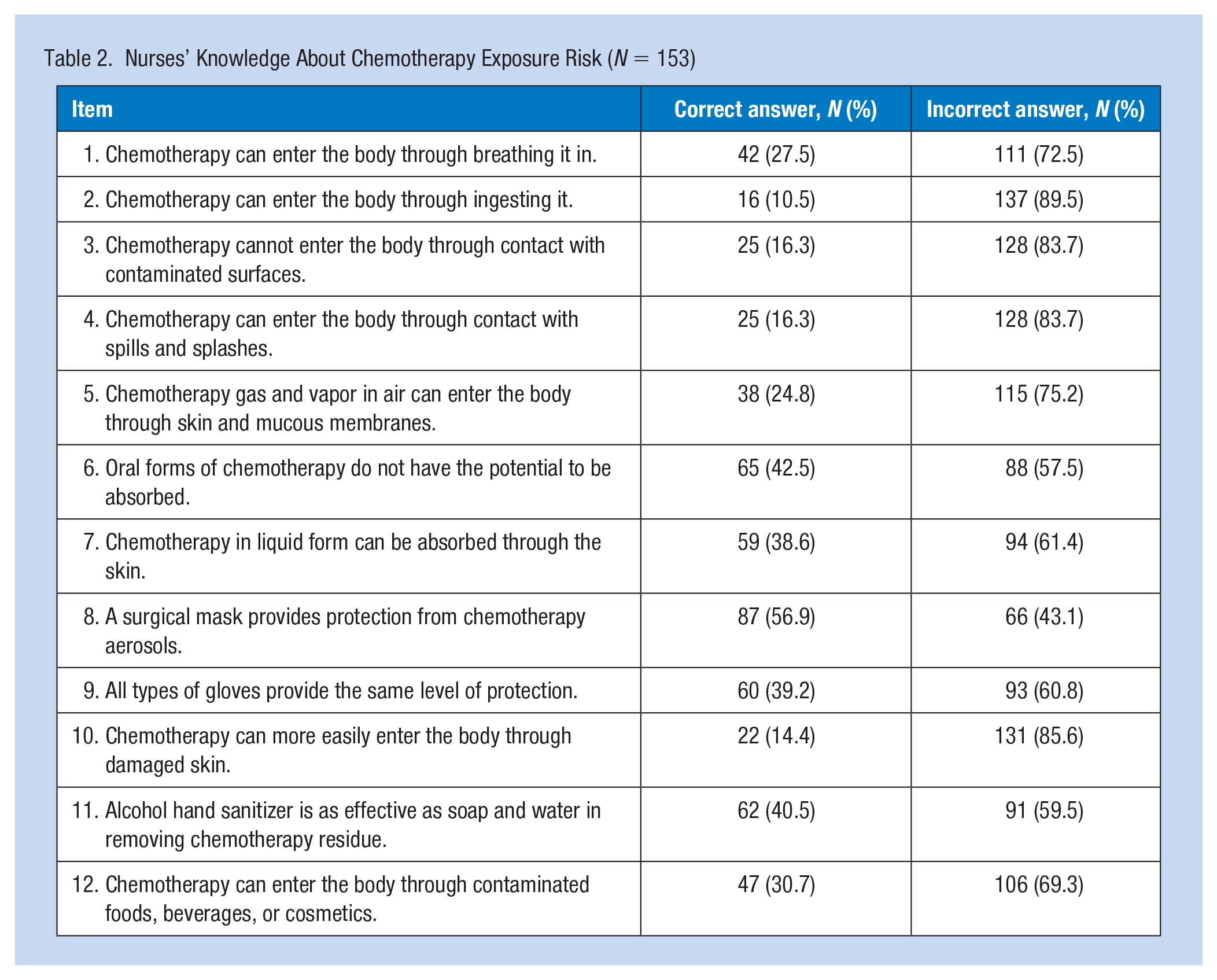
Measurements of nursing knowledge of chemotherapy exposure are included in Table 2. Overall, the participants’ level of knowledge related to chemotherapy exposure was unsatisfactory. The results showed that for 11 of the 12 questions, less than 50% of the participants answered correctly about exposure risk, with the average number of correct answers was 3.55 out of 12 questions (SD = 2.09) (data not shown).
Nurses’ Knowledge About Chemotherapy Exposure Risk (N = 153)
With regard to safe-handing precautions (Table 3), wearing double gloves was commonly used by the participants (91.5%), followed by wearing a mask (73.2%). Eye protection was rarely used (19.6%), and one third (29.4%) reported wearing a gown. Participants had an insufficient level of knowledge about chemotherapy exposure (M = 3.55, SD = 2.09), but reported high self-efficacy for using PPE (M = 19.56, SD = 2.98), and moderate barriers for using PPE (M = 28.20, SD = 9.82).
Predictors of Chemotherapy Safe-Handling Precaution Use (N = 153)
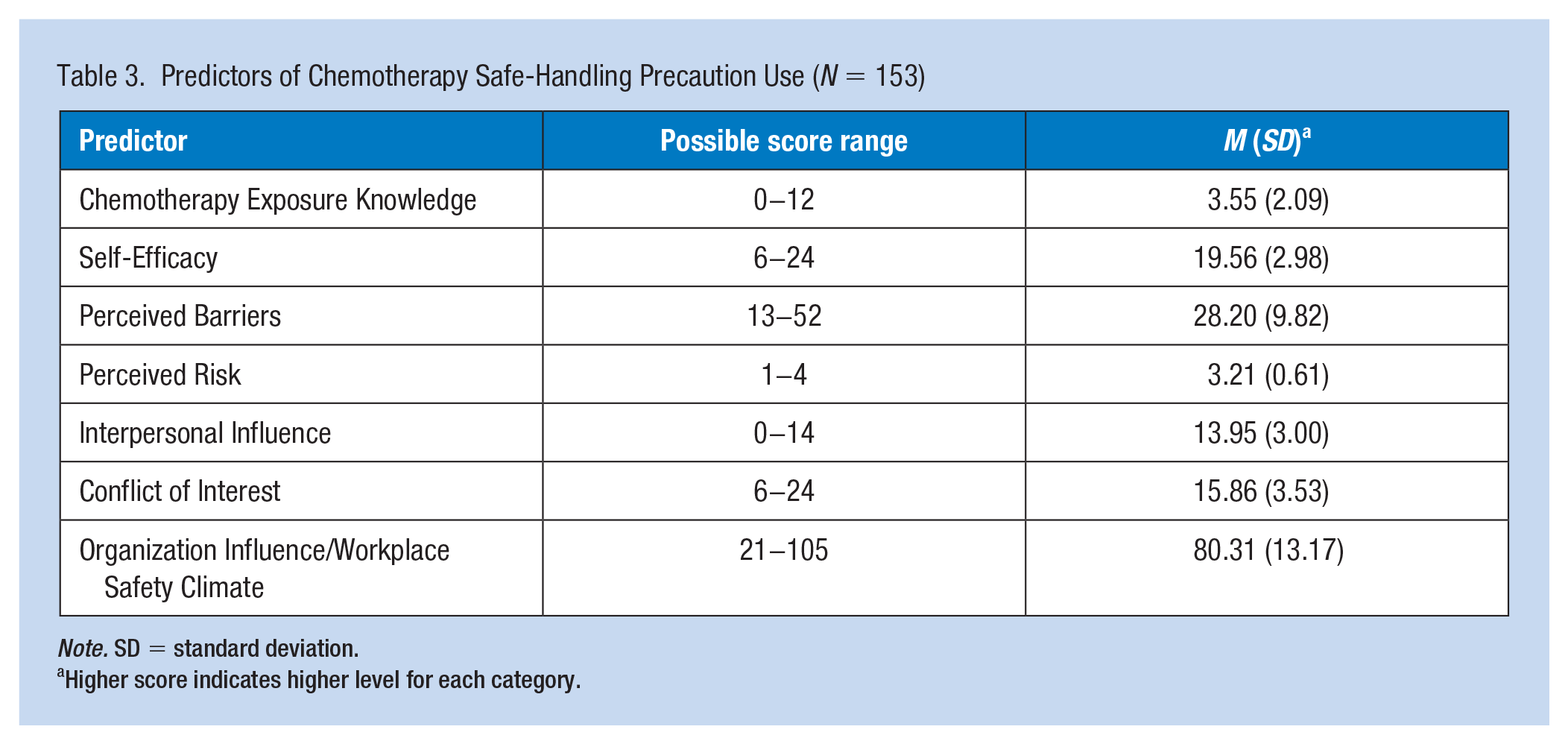
Note. SD = standard deviation.
Higher score indicates higher level for each category.
Years of nursing experience correlated negatively with chemotherapy exposure knowledge, Spearman’s rho (rs) = −.26, self-efficacy (rs = −.25), and perceived risk (rs = −.26), and positively with interpersonal influence (rs = .27) and organization influence/workplace safety climate (rs = .40) (Table 4). In addition, safe-handling precautions was correlated negatively with age (rs = − .23), number of patients to whom the participant personally administered chemotherapy per day (rs = −.35), and number of patients receiving chemotherapy per day at the participant’s work place (rs = −.19).
Correlation Between Sample Characteristics and Predictors Chemotherapy Safe-Handling Precaution Use (N = 153)
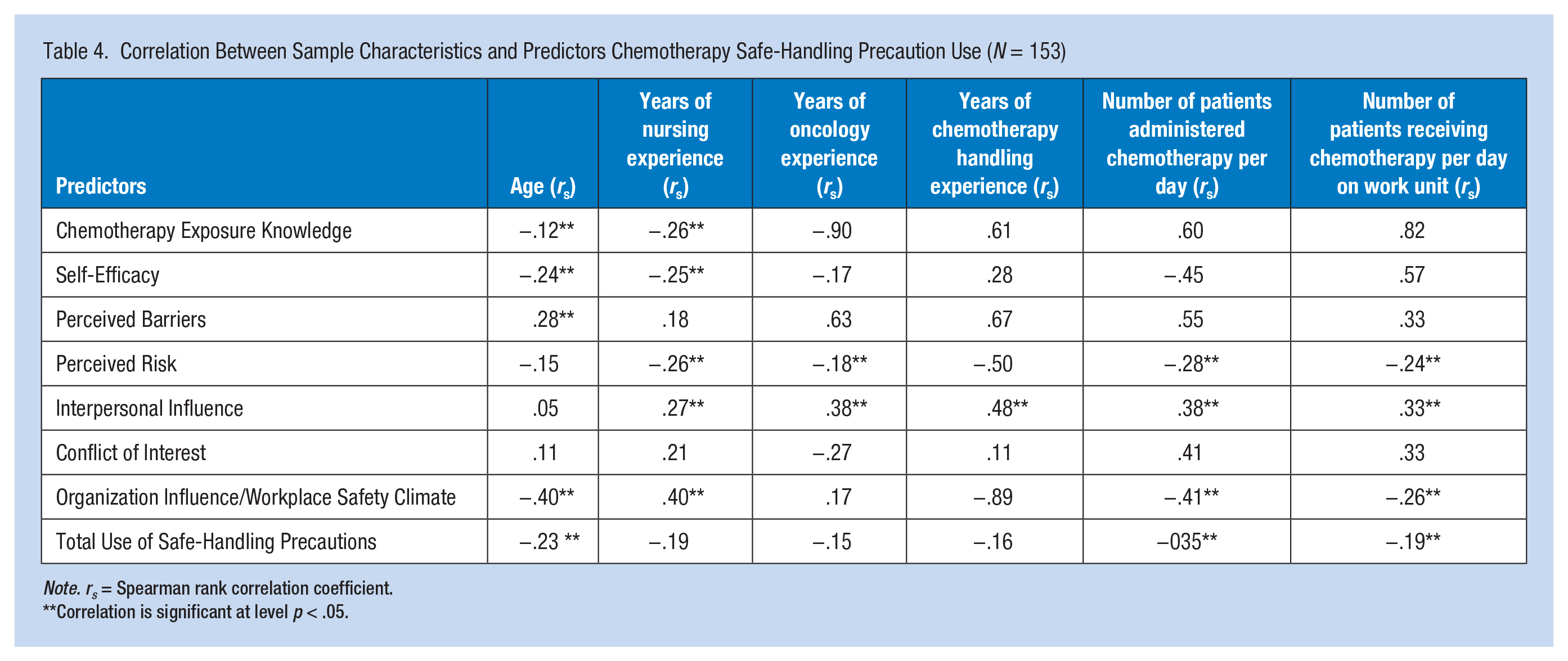
Note. rs = Spearman rank correlation coefficient.
Correlation is significant at level p < .05.
In the predictive model (Table 5), several items positively predicted safe-handling precautions among the sample including number of patients to whom the participant personally administered chemotherapy per day (β = .72, p < .001), number of patients receiving chemotherapy per day at the participant’s work (β = .92, p < .001), greater knowledge (β = .26, p < .001), higher self-efficacy (β = .45, p < .001), reduced perceived barriers (β = .19, p < .001), higher organization influence/workplace safety climate (β = .34, p < .001), and greater interpersonal influences (β = .23, p < .001). In contrast, three predictors negatively predicted safe-handling precautions including age (β = −.08, p < .001), perceived risk (β = −.27, p < .001) and conflict of interest (β = .93, p < .001).
Regression Analysis for Predictors of Safe Chemotherapy Handling Precautions Among Nurses (N =153)
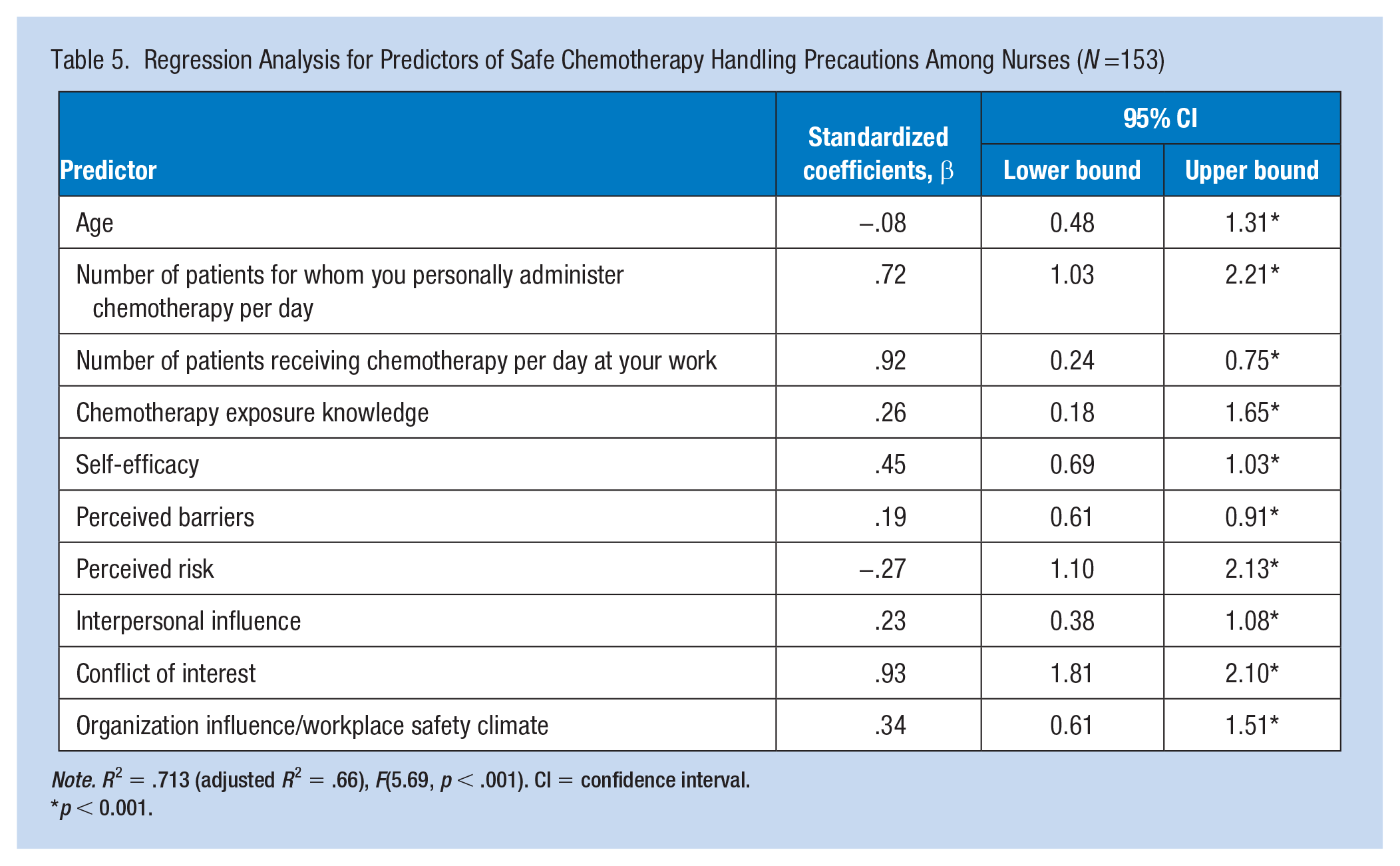
Note. R2 = .713 (adjusted R2 = .66), F(5.69, p < .001). CI = confidence interval.
p < 0.001.
The results revealed an R2 = .713 (adjusted R2 = .66), F(5.69, p < .001). Finally, the above-mentioned independent variables accounted for 71.3% of the variance in safe-handling precautions.
Discussion
Chemotherapy handling, a complicated and unavoidable procedure for oncology nurses, has been associated with exposure-related adverse health effects (Oliphant et al., 2015). The preparation, administration, disposal, and excretion of chemotherapy drugs pose dangerous occupational risks to the nurse (VerStrate, 2015). Thus, identifying the factors that affect their use of hazardous drug precautions has become necessary to maintain safe-handling. This study provides preliminary information regarding predictors of using safe-handling precautions among a sample of Jordanian oncology nurses, which can be used as fundamental data for future research with larger sample size.
In general, the results showed that participants’ level of knowledge related to chemotherapy exposure was unsatisfactory. A lack of knowledge could lead to unsafe practices and put nurses and patients at risk and could decrease nurses’ compliance with the safety measures (Khan et al., 2012). In Jordan, chemotherapy drugs are handled mainly by nurses. Lack of training, in-service education and poor undergraduate preparation could be reasons for the unsatisfactory level of knowledge (Kyprianou et al., 2010; Topçu & Beşer, 2017). The results from this study highlight the need for improving oncology nurses’ knowledge through conducting educational/training programs about safe-handling of chemotherapeutic agents. The previous literature acknowledged the effectiveness of such a program on nurses’ knowledge and compliance to safety measures (Keat et al., 2013; Khan et al., 2012; Yanqin et al., 2012).
The regression results showed that nurses’ characteristics, including age, and years of experience could predict the use of safe-handling precautions. Younger nurses with fewer years of experience were more likely to use safety measures than older nurses with more years of experience. The relationship between participants’ age, years of experience, and safe-handling precautions is inconsistent in the literature (Callahan et al., 2016; Polovich & Clark, 2012; Rizalar et al., 2012). Lack of experience can increase risk for unnecessary exposure of cytotoxic drugs and contribute to the nurses’ safety (Rizalar et al., 2012). Our results support the previous results and are consistent with Martin’s (2006) study and indicated that age and years of experience for the oncology nurses were significant predictors for safe-handling precautions. In their study, Martin (2006) conducted a cross-sectional study to evaluate the safe-handing precautions among oncology nurses in outpatient clinic; 500 participants completed the study’s survey, and the results indicated that age and years of experience predicated the safe-handling precautions.
Participants’ self-efficacy for using safety measures was measured in this study. The results showed that participants had a moderate level of self-efficacy, which was associated with safe-handling precautions in the final regression model. It was also a predictor for safe climate and an important factor for encouraging oncology nurses’ safe-handling precautions during chemotherapy handling. Self-efficacy was defined as ability of nurses to complete their tasks and duties successfully and completely (Edwards et al., 2016). In addition, self-efficacy is positively related to the level of knowledge. Importantly, a higher level of self-efficacy decreases sensitivity to the barriers and obstacles for implementing health-protective behaviors and using safety measures (Polovich & Clark, 2012; Topçu & Beşer, 2017).
A moderate perceived conflict of interest was reported in this study. Theoretically, it was defined as a conflict between the health worker’s need to protect themselves and their job to provide optimal care for sick patients (Gershon et al., 2007). This conflict of interest was a predictor for safe-handling precautions and was associated with the final regression model. Supporting results were obtained by Callahan et al., (2016). Nurses with lower perceived conflicts of interest reported fewer barriers for using HD precautions, more confidence in using safety measures such as PPE, and had safer workplace environments (Callahan et al., 2016).
Organization influence/workplace safety climate, perceived risk, and interpersonal influences were also associated positively with safe-handling precautions among Jordanian oncology nurses. Ability of the health organization to create a safe climate through standard policies, continue education and training, make available necessary equipment and supplies, provide feedback and safety reinforcement, and offer continued support is associated with better usage of HD precautions (Callahan et al., 2016; Khan et al., 2012; Polovich & Clark, 2012). Interpersonal influence was defined as the impact of other important people, such as coworkers, on the nurses’ practices and behaviors, in particular skills on chemotherapy handling. The results from this study supported the previous studies in concluding that oncology nurses are more likely to use HD precautions if their work colleagues use them (Callahan et al., 2016; Hon et al., 2015; Hong et al., 2005; Polovich & Clark, 2012). Perceived risk and sense of hazards related to the exposure also motivated the oncology nurse to use safe-handling precautions and was considered as a predictor in final model. Increased risk expectation lead to a higher level of engagement in protective behaviors (Brewer et al., 2007; Ferrer et al., 2018). In this study, risk perception refers to the oncology nurses’ beliefs about the possibility of adverse effects or harm related to the handling of chemotherapy. This feeling had a central role in changing their health behaviors and use of safe-handling precautions during their daily practices.
Despite the limitations of our study, including small sample size and use of one method (structured questionnaire), the results of this study add to the Jordanian literature regarding the factors affecting the use of safe-handling precautions among Jordanian oncology nurses. Nurses in Jordan, as bedside care providers, have an active role in chemotherapy handling; therefore, they must do so correctly and safely to prevent potential adverse effects and harm. Our findings determined the factors that can predict the use of safe-handling precautions; it is clear that responsibility for safe practice is shared between the nurses and their organizations. Engaging stakeholders and leaders in designing strategies for building safe environments and advancing the nurses safe-handling precautions are recommended. Further research with a larger sample size and a mixed-method approach are recommended to gain in-depth understanding of the nurses’ experience and perceptions regarding the use of safe-handling precautions. Addressing chemotherapy handling in undergraduate nursing curriculum is also recommended.
Implications for Occupational Health Nursing Practice
The contribution of this study is to highlight the predictors and difficulties of using safe-handling precautions from the oncology nurses’ perspectives. Both nurses and employers would benefit from the present results to inform safe workplace climate, prevent incidence, decrease barriers, and supply the units with necessary PPE material. Continued monitoring of nurses practices during chemotherapy handling is essential. Continued education in the clinical setting is needed to ensure nurse’s knowledge and clinical skills to avoid chemotherapy-related unsafe practices such splash, leakage, and nonuse of PPE. These findings also suggest focusing on organizational, in addition to individuals factors, when considering safe-handling precautions. Clear policy-related safe-handling precautions must be established and enforced.
Applying Research to Practice
Implementation of standard guidelines for chemotherapy handling is needed to reduce adverse exposures among oncology nurses. Proper PPE, training, and continuous education could demonstrate health care system support and reduce nurses’ concerns during chemotherapy handling. Increasing oncology nurses’ knowledge through training will ensure safe practices, decrease their risk to adverse exposures, and increase their compliance with the safety measures.
Footnotes
Acknowledgements
The authors thank the participants for their effort and time.
Author Contributions
All authors participated in study design, analysis, interpretation of the data, and approved the submitted.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Loai. Abu Sharour, BSN, MSN (Hon), PhD, associate professor, Faculty of Nursing, AL-Zaytoonah University of Jordan. His area or research is psychosocial aspects and quality of life among cancer patients. He interested in qualitative, quantitative, and mixed-method.
Maha Subih, assistant professor, Faculty of Nursing, AL-Zaytoonah University of Jordan (ZUJ). Dr. Subih is interested QOL and Coping concepts.
Ayman Bani Salameh, RN, PhD, assistant professor, Faculty of Nursing, Al-Zaytoonah University of Jordan (ZUJ). Amman-Jordan.
Dr Ayman, is interested in quantitative research in nursing focusing mainly of quality of life domain.Malakah Malak, RN, BSN, PhD, associate professor, Faculty of Nursing, AL-Zaytoonah University of Jordan (ZUJ). Dr. Malakah is interested in psychosocial aspect among chronic illness patients and Quality of Life.