
Abstract
Background
The majority of U.S. worksites are smaller worksites that often employ low-wage workers. Low-wage workers have limited access to, and participation in, workplace health promotion programs. Community-based participatory research (CBPR) has been identified as a key method to directly engage employers in identifying the health promotion needs of smaller workplaces. This article describes a four-phased process where CBPR was used to tailor a workplace health promotion program to meet the needs of a smaller workplace that employees low-wage workers. Outcomes of this program were measured and reported over time.
Methods
The CBPR approach was based on the Social Ecological Model along with two additional health promotion models. Publicly available evidence-based tools were also used for this four-phased process which included the following: (a) initial program assessment, (b) program planning, (c) program implementation, and (d) program evaluation. Key strategies for developing a comprehensive workplace health promotion program guided the process.
Findings
The workplace’s capacity for promoting health among its employees was improved. There were sustainable improvements in the health interventions and organizational supports in place.
Conclusion/Application to Practice
A CBPR approach may be a way to build the capacity of smaller workplaces with low-wage employees to address the health promotion needs of their workforces. The use of publicly available strategies and tools which incorporate the social ecological determinants of health is of equal importance.
Keywords
Background
Healthy People 2020 targets the occupational health and safety of the U.S. workforce (U.S. Department of Health and Human Services, 2015). Workplace health promotion programs (WHPP) provide the opportunity for employers to address both the health promotion and health protection of their employees (L. Linnan et al., 2008). Harris et al. (2014) explains that the majority of U.S. worksites are smaller organizations, which are described in the National Worksite Health Promotion as employing less than 1,000 employees. These smaller worksites employ half of U.S. working adults, yet, most do not offer health promotion programs (Harris, Hannon, Beresford, Linnan, & McLellan, 2014).
The health care and social assistance sector is one of the largest sectors (44.7%) of U.S. smaller workplaces with low-wage earners (U.S. Small Business Administration Office of Advocacy, 2019). This sector of employees is at increased risk for chronic diseases, morbidity, and mortality (Khullar & Chokshi, 2018). Within this sector, there is a workforce crisis in the long-term services and support (LTSS) industry among direct support professionals (DSPs) who assist people with intellectual disability/developmental disability (ID/DD) U.S. Department of Health and Human Services et al., 2017). There are not enough DSPs to support the work needed to care for individuals in institutional and community-based settings (U.S. Department of Health and Human Services & President’s Committee for People with Intellectual Disabilities, 2017). The shortage in DSPs is fueled by the increased survival rates of people with ID/DD as well as low retention rates among DSPs (Bogenschutz et al., 2014). Low wages, poor access to health insurance, lack of paid time off and other benefits, along with the high stress and demands of round-the-clock, 7-days-a-week work contribute to low retention rates among DSPs (U.S. Department of Health and Human Services & President’s Committee for People with Intellectual Disabilities, 2017). Hewitt and Larson (2007) identified the increased risk for infectious diseases, workplace violence, overexertion, chemical exposure, shift work and psychosocial stressors, such as stress and job burnout among DSPs which make this group a priority population for worksite health promotion efforts.
Barriers to WHPP implementation and employee participation vary across occupations and work settings (Tsai et al., 2019). Stiehl et al. (2018) identified limited research on WHPP among employers of low-wage workers. However, these researchers found that low-wage workers had limited access to WHPP and cited the need to better understand how to expand their access to and participation in WHPP.
Harris et al. (2014) identified community-based participatory research (CBPR) as a key method to directly engage employers to identify the health promotion needs that are of value to employees working in smaller worksites. Through CBPR, WHPPs can be tailored to increase participation and sustainability of programs.
This work contributes to a gap in the literature by describing how CBPR was used to tailor a WHPP to meet the needs of a smaller workplace that employs low-wage DSPs within the health and social assistance sector. The CBPR partnership and the health promotion models, strategies and tools implemented, along with the impact of the WHPP on the organization and its capacity to sustain the program were the foci of this article. The goals of this project were to: (a) identify the health promotion and protection needs of employees, (b) assess the organization’s current health promotion and protection strategies, and (c) build the organization’s capacity for promoting health among its employees.
Methods and Findings
A community partnership began when two university faculty members with expertise in health promotion and social work from different universities, and a nonprofit organization in Northeastern Pennsylvania partnered for a CBPR project. The nonprofit organization served individuals of all ages diagnosed with ID/DD, pregnant women, young families, couples hoping to adopt, and people who required outpatient therapy. It was the primary provider of ID/DD services within the community. The organization was concerned with low retention among direct care employees and was interested in a health promotion program that might reduce employee turnover.
The CBPR project included a four-phased process: assessment, planning, implementation, and evaluation. During assessment, standard tools used in workplace health promotion were used to gather baseline data. Data collection resulted in two reports: a site visit summary report and health fair survey report. These two reports guided the planning and changes implemented in the organization’s employee health and wellness initiatives. At the 3-year mark, the impact of the project was evaluated through improvement in multiple indicators of the organization’s scores from the Centers for Disease Control and Prevention’s (CDC) Health ScoreCard (HSC), Version 2 (CDC, 2014).
Bronfenbrenner’s (1994) Social Ecological Model and two planning models were introduced to guide the CBPR approach: Green and Kreuter’s (1992) PRECEDE-PROCEED Model (PPM) and the CDC’s Workplace Health Model (WHM; CDC, 2016). During the initial planning meeting, an overview of these two models and their role in ensuring a comprehensive workplace wellness program was discussed.
Phase I: Initial Program Assessment Methods
The initial assessment was organized using the Workplace Health Program Development Checklist, the Swift Worksite Assessment and Translation (SWAT) Evaluation Method, and the Enhanced SWAT Tool for Observing Worksite Environment (TOWE; CDC, 2019a; Dunet et al., 2008; Oldenburg et al., 2002). The SWAT method incorporated a rapid, systematic approach to evaluation which is user-friendly in business environments as well as supporting the CDC’s Evaluation Framework (CDC, 1999). Dunet et al. found the SWAT method to be useful to develop sound health promotion practices within small- to medium-sized workplace settings.
The organization’s main center and five satellite sites were visited to ensure a cross-section of different worksite environments. The organization’s president, five employee leaders (operations, human resources, occupational injuries, and community relations) and two employees from the Health and Leisure Committee were interviewed. The Workplace Health Site Visit Interview Questions guided each interview (CDC, 2019b). The site visit team worked with the organization and reviewed current data necessary to build the organization’s capacity to collect employee health-related information. The current year human resource policies, employee bulletins, and the Health and Leisure Committee meeting minutes were reviewed for health and wellness information. Health insurance usage data and 3 years of employee satisfaction survey data were also reviewed.
The health promotion faculty member designed two surveys to collect baseline aggregate data for program planning, which were the Employee Health and Wellness Survey and Health Fair Survey. The survey incorporated the CDC’s (2000) Healthy Days Measures and questions concerning employee demographics, their interest and preference of health topics as well as the timing, type, and format of programs. The first employee health fair was also developed during the initial assessment period. The health fair afforded the opportunity for participants to complete an employee health fair satisfaction survey. The health fair survey was used to collect data on employees’ satisfaction, learning, and their intention to participate in worksite health promotion programming. Finally, the organization’s scores from CDC’s Health ScoreCard (HSC), Version 2, were also included in the initial assessment (CDC, 2014). Descriptive analysis was run using SPSS, Version 24. The project was approved by the organization’s and universities’ institutional review boards. A cooperative grant between the two universities funded the initial CBPR project.
Phase I: Initial Program Assessment Findings
At the outset of the partnership, the organization employed 596 employees. The majority of employees were female (84%). Employee ages ranged from 18 to 34 years old (43%), from 35 to 54 years old (33%), and 55 or older (21%) with the remaining 3% preferred not to answer. The employees were Caucasian (86%), Black (6%), Hispanic (5%), and all others (<1%). No significant differences in the demographic characteristics of the employee population existed.
Most employees (n = 408, 67%) were direct care staff, 246 (60%) were full-time, 96 (23%) were part-time, 56 (14%) were per diem, and 10 (3%) were seasonal. The hourly pay rate ranged from US$9.99 to US$17. The average salary was US$13.22 per hour. The overall retention rate for all employees at the 1-year point was 45%. Turnover was highest among new employees and direct care staff who earned lower salaries.
Wages and health benefits varied by employee status. Of 609 employees, 63% (n = 385) were full-time and eligible for health insurance with 70% (n = 268) of those eligible for “opting-in.” Employee coverage ranged from employee only (60%), family (15%), employee/spouse (14%), employee/child (6%), and employee/children (5%). In 2018, the organization changed to self-insured status.
Almost half of the employees (48%, n = 280) completed the initial health and wellness survey. The majority of respondents were female (88%) and Caucasian (90%). Respondents’ ages ranged from 18 to 34 (43%), from 35 to 54 (33%), and 55 or older (21%) with the remaining 3% of respondents preferring not to answer. Most respondents were single, never married (44%) followed by married/domestic partnerships (39%). Most respondents were high school graduates or equivalent (31%), whereas the remaining respondents indicated some college credit (24%) followed by 16% who indicated earning a bachelor’s degree. Most respondents represented direct care staff (67%), followed by administrative/clerical (14%) and other (12%).
Responses to health-related quality of life questions on the health survey indicated that most respondents felt they were either in “good” health (51%), “very good” health (27%), or “excellent” health (15%). The majority of respondents (80%) indicated that within the past 30 days, they felt “very healthy and full of energy some days.” Respondents indicated that within the past 30 days that either their “physical health was not good some days” (30%) or their mental health was “not good some days” (40%). While 16.4% of respondents indicated keeping from their usual activities due to poor physical or mental health. Survey respondents indicated that they “did not get enough rest/sleep” (66%), while remaining (54%) felt “worried, tense, or anxious,” and 38.6% reported feeling “sad, blue or depressed” in the past 30 days. Employees reported that the following limited their activity: back/neck problems (9%) followed by arthritis/rheumatism (9%), depression/anxiety/emotional (9%) problems. Survey results also revealed that most respondents were interested in self-managed (52%), onsite (67%) wellness activities in the areas of physical activity (67%), nutrition (65%), weight management (61%), and stress management (44%) offered after work (47%) or during work (38%).
Phase II: Program Planning Methods
Based on initial assessment recommendations, a health and wellness policy was put in place. The policy focused on the importance of employee self-care as a way to engage and retain employees and maintain positive morale in the workplace. The overall goal was to create a healthy, physically and psychologically safe and caring work environment by blending organizational and health/wellness program elements with organizational participation. Other assessment recommendations included incorporating health/wellness information into the new employee orientation, developing participation-based incentives, offering self-managed individual wellness opportunities, and utilizing the American Heart Association’s (AHA) My Life Check—Life’s Simple 7® and the CDC HSC for establishing baseline measures and for wellness program evaluation. The organization was also encouraged to use the CDC workplace health resources and to select and utilize national observances toolkits for annual wellness programming.
The committee branded the health and wellness program, CareSTRONG, to help employees connect with the organization’s core values of care, concern, compassion, and commitment and to highlight the importance of their own self-care. The organization’s logo was also incorporated into the “o” of the program name. The CareSTRONG mission statement was as follows: “The organization values the physical, emotional and spiritual health and wellness of all employees. The organization is committed to ensuring the availability of and access to resources which create and promote a culture of health and wellness.”
The program incorporated health/screening assessments (e.g., cholesterol, blood pressure, body composition), health/wellness interventions (e.g., physical activity and nutrition challenges, lunch/learn sessions, community walks), and environmental supports such as key human resource and occupational, health and safety policies and programs (e.g., the Employee Assistance Program, staff development, the employee benefits package, low cost fitness membership, a worksite “Weight Watchers” offering). The responsibility of developing, implementing, and evaluating the program was shared with the wellness committee, supervisors, and employee volunteers throughout the organization who were CareSTRONG Champions. All employees were encouraged to participate and take ownership by creating a culture of health and wellness within the organization. Program participation was voluntary and participation-based incentives were used (e.g., t-shirts, pedometers, food samples).
The wellness committee continued to develop an annual program plan. Each month the committee met to revise and update the plan. A month-to-month wellness committee calendar helped with implementation. The committee used results from the HSC, annual health fair survey, and employee satisfaction survey to plan strategies for the upcoming year. Employee answers or suggestions received through a monthly question posed by the committee allowed the committee to better understand the “pulse” of employees. Employees participated in this initiative called, The Pulse, by submitting their responses anonymously through breakroom boxes. These anonymous responses also helped with program design. The CDC HSC tool was used to identify objectives, strategies and record progress.
Phase II: Program Planning Findings
Ninety-four percent of health fair participants completed the employee health fair survey (n = 118/126). The majority (86%) of respondents indicated learning something new about their health and wellness, whereas 99% planned on using the wellness information. The majority (88%) also indicated that they planned on participating in future worksite wellness activities and 99% planned to attend the health fair the following year. These findings coupled with the baseline employee health survey findings and site visit report informed not only the program planning but the program implementation, as well.
Phase III: Program Implementation Methods
The site visit report recommendations guided the initial implementation of the program, which was carried out by wellness committee members. The CDC HSC was also used on an annual basis to evaluate the implementation of evidence-based strategies and practices. To help with implementation, the human resources department created a new employee position specific to health promotion, a position that was filled within the first year. Initial program elements included the following: CareSTRONG Champions, monthly employee bulletin articles based on national observances which targeted employees’ needs and interests (e.g., nutrition, dental, and influenza), The Pulse (employees were given a monthly wellness question to voluntarily answer anonymously with results published in the newsletter), annual employee health and information fair, AHA My Life Check—Life’s Simple 7®, a stairwell initiative, organization-wide health promotion kiosks/folders, and two breakroom makeovers were put into place. Breakrooms were redecorated to create a restful, calming home-like space (i.e., warm yellow wall colors, area carpets added, rocking chairs, and cheery hand-painted artwork).
In subsequent years, the wellness committee recruited other employees and community members to build and sustain the program. Community-based learning (CBL) projects and an academic health promotion internship were incorporated to help support program initiatives. Undergraduate community health education students were faculty-led and worked to support each of the CBL projects. Initiatives included lunch/learn sessions, health fair stations, health challenges, health risk assessments, health screenings, and pop-up health promotion events on hydration, brain health, sleep, and mindfulness. Employee champions created and implemented a monthly health topic calendar which included fun, interactive health promotion activities and information. Community health promotion professionals and providers led smoking cessation groups and health lectures. Additional elements included the following: self-administered blood pressure screening stations, walking initiatives, and a lactation policy. Program activities and interventions were offered at different locations, days, and times to meet a variety of work shifts.
The annual health and information fair were the interventions in which most employees participated in the WHPP. The health fair stations included a variety of health topics (e.g., smoking cessation, e-cigarettes, hydration, mindfulness, stress management). Employees were engaged in a fun, interactive activity at each station such as a game or quiz. The CBL students used motivational interviewing strategies to discuss topics with employees. Health fair screenings included blood pressure, cholesterol, glucose, flexibility, balance, and body composition. An employee assistance program informational booth was included along with financial wellness, women’s resources, vision, and dental health booths.
Phase III: Program Implementation Findings
Findings from implementation of the second and third annual health fairs continued to guide overall program implementation. Health fair participants (second health fair, N = 150, third health fair N = 110) who completed the health fair surveys represented a (92%, 94%) response rate for 2017 and 2018, respectively. Both years, 83% of participants were female. The majority of respondents were administrative/clerical (second = 28%, third = 30%) and direct care staff (second = 36%, third = 37%), 2017 and 2018, respectively. Respondents indicated their intention to participate in the health fair challenge the following year, 97% and 97%, 2017 and 2018, respectively. Participants also indicated they would recommend the health fair to a coworker, 99% for both 2017 and 2018. The Top 4 areas which motivated participants to attend the fairs were the following: health screenings (66%, 66%), free information (43%, 58%), learn about health issues (36%, 50%), and to improve health (45%, 48%), 2017 and 2018, respectively. A majority (86%, 87%) of respondents indicated their intention to participate in other wellness activities at the worksite while remaining (40%, 46%) indicated their plan to change an unhealthy behavior, 2017 and 2018, respectively.
Phase IV: Ongoing Program Evaluation Methods
The evaluation process was based on the CDC (1999) framework for program evaluation in public health. Process measures included employees’ participation, interest, and satisfaction; use of health promotion materials and cost of materials through simple surveys, attendance, and inventory methods. The organization built its capacity to survey employees through the use of SurveyMonkey®. These surveys have determined the most successful types, times, and locations of programs.
The HSC was been the primary tool used to measure the intermediate progress of the program and to guide program implementation. The HSC was a reliable and valid tool designed to help employers assess whether they had implemented evidence-based health promotion interventions or strategies in their worksites to prevent heart disease, stroke, and related conditions (Roemer et al., 2013).
Long-term measures were not yet in place to quantify program effectiveness on the reduction of the healthcare costs, worker productivity, and health outcomes. Employees had been encouraged to complete the AHA Life’s Simple 7® through participation-based incentives (AHA, 2017). Life’s Simple 7® had been identified as a strategy to assess aggregate employee data on reductions in healthy lifestyle risks for health disease (Folsom et al., 2015). Changes in employee lifestyle risks were another area for future CBPR projects. The AHA Workplace Health Achievement Index had also been used to assess the comprehensiveness of the program with the organization being recognized as an “Early Adopter” and “Completer” (AHA, 2019). Adoption of AHA resources had been limited due to AHA website updates. Program data collected to date had been instrumental in securing a community grant for US$2,000 to support the cost of operating the WHPP and another grant for US$500,000 which enabled the organization to increase DSP wages.
Phase IV: Ongoing Program Evaluation Findings
After 3 years of the CBPR partnership, the organization’s CDC HSC total score increased from 61 to 182, representing a 198% increase in the points scored. See Table 1 for CDC ScoreCard Results, Percentage of Total Points Possible by Topic, 2016–2019. At baseline, the organization’s HSC score was 38% lower than the overall average total score for other medium worksites and 37% lower than the overall average total score for all worksites. In 2019, when compared with other similarly sized worksites, the organization’s HSC score was 13% lower than the overall average score for medium worksites and 7% lower than the overall average score for all worksites.
HSC Results, % of Total Points Possible by Topic, 2016–2019
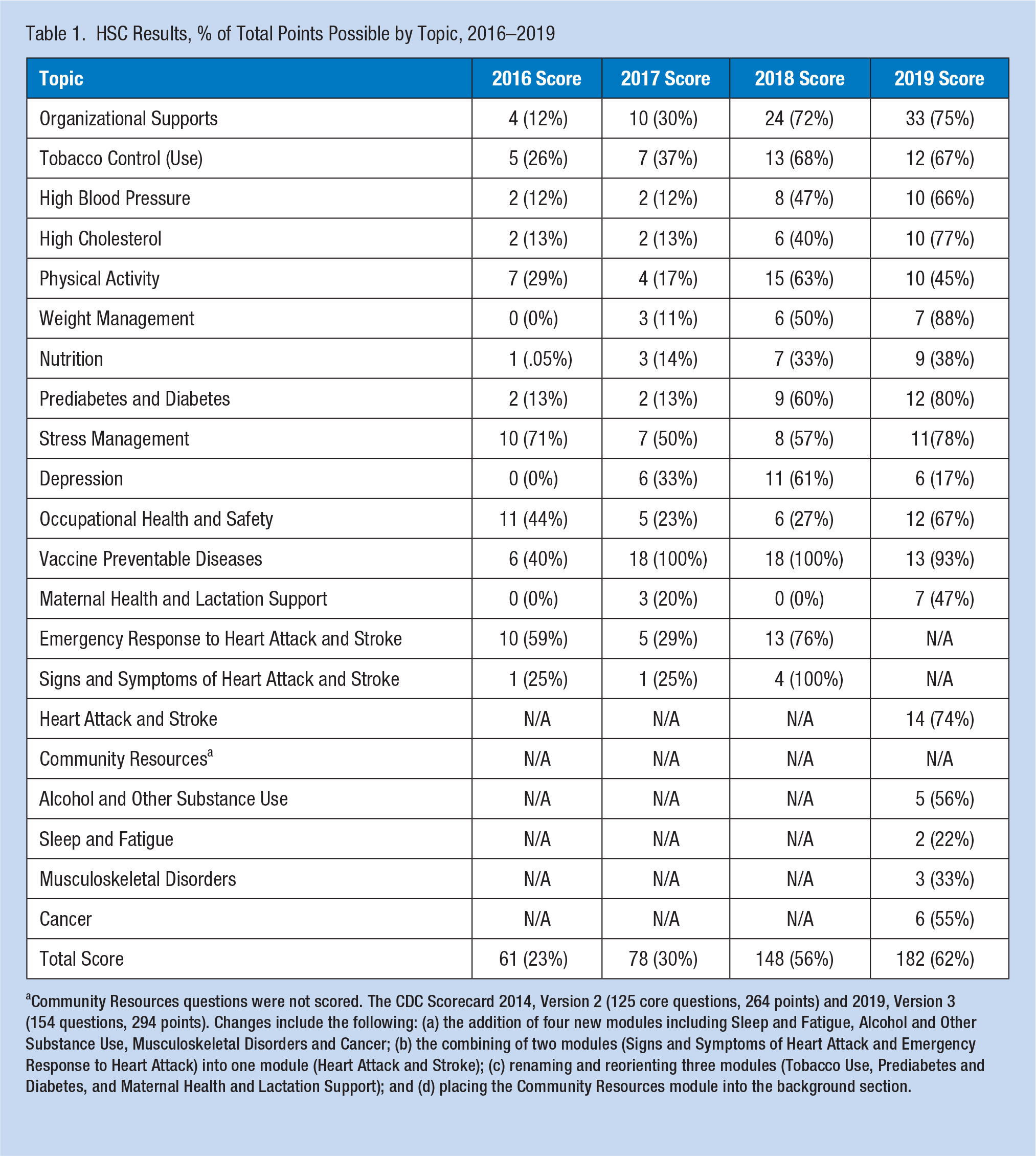
Community Resources questions were not scored. The CDC Scorecard 2014, Version 2 (125 core questions, 264 points) and 2019, Version 3 (154 questions, 294 points). Changes include the following: (a) the addition of four new modules including Sleep and Fatigue, Alcohol and Other Substance Use, Musculoskeletal Disorders and Cancer; (b) the combining of two modules (Signs and Symptoms of Heart Attack and Emergency Response to Heart Attack) into one module (Heart Attack and Stroke); (c) renaming and reorienting three modules (Tobacco Use, Prediabetes and Diabetes, and Maternal Health and Lactation Support); and (d) placing the Community Resources module into the background section.
The organization also developed sustainable changes in health interventions and organizational supports, which are provided in Table 1. Each of the 125 HSC questions represents an individual health promotion strategy or intervention. Values ranging from 1 to 3 points are given for each question, based on whether the strategy was a good practice (1 point), better practice (2 points), or a best practice (3 points). In 2015, there were a total of 264 points possible, and currently, there were a total of 294 points possible. At baseline, the organization’s initial total score of 61 points represented 23% of the HSC’s total possible points. In 2019, the organization’s total score of 182 represented 62% of the HSC’s total points possible. From 2015 to 2019, the organization increased in place “best,” “better,” and “good” practices by 154%, 255%, and 240%, respectively. As a result, the number of interventions not in place, rated as “best,” “better,” and “good,” decreased by 57%, 33%, and 4%, respectively.
Discussion
Small workplaces have fewer resources and as a result, less variety of programs and fewer WHPPs (Linnan et al., 2019). Low-wage industries often face compounding factors which limit implementation of WHPPs, such as employees’ lack of personal experience with health promotion and their doubt whether employers would make employee health a priority (Hammerback et al., 2015; Hannon et al., 2012). In our case, health promotion faculty provided expert assistance to help organizations navigate and use the many public health tools available for designing, implementing, and evaluating WHPPs (Witt et al., 2013). The organization made employee health a priority and demonstrated its commitment to employee health.
To create these improvements, the organization engaged with community health promotion resources and relationships in new ways. Environmental supports such as policies and the organization of work were modified by utilizing wellness champions and adding employee wellness responsibilities to the human resource function. Use of an integrated approach has been shown to reduce health inequities among low-wage workers (Baron et al., 2014).
Our findings suggest that CBPR was a promising strategy to increase the capability of small workplaces to adopt and sustain WHPPs. Recruiting small, low-wage worksites for community-based health promotion research partnerships were more successful through personal relationships (Hammerback et al., 2018). Hannon et al. (2017) suggested use of a workplace readiness questionnaire to determine organizational readiness to implement a WHPP. Laing et al. (2012) also found that small- and low-wage workplaces increased implementation of comprehensive WHPPs when presented with easily accessible resources and support.
Our CBPR partnership has been sustained for over 4 years. The university faculty member with expertise in health promotion continues to serve on the organization’s health promotion committee and has connected with other faculty. Two additional CBPR projects have been completed which focus on developing physical activity interventions to improve employee physical activity behaviors. For over 2 decades, health promoters and researchers have identified community partnerships as a way for organizations, health promotion professionals, and researchers to build healthy communities and reduce health disparities through CBPR (Minkler, 2000, 2005; Stoto et al., 1996).
Conclusion
Partnerships between small workplaces and university faculty members were viable strategies to tailor WHPPs to meet the needs of low-wage workers employed at small workplaces. These CBPR partnerships provided small workplaces the opportunities to address relevant employee health priorities, and provided the organization an authentic role in the designing, implementation, and evaluation of WHPPs. Providing small workplaces with the data and tools to help inform decision-making processes about their employees’ health is a critical first step. It is of equal importance to use publicly available strategies and tools which incorporate the many social ecological determinants of health.
Applications to Professional Practice
The majority of U.S. worksites are smaller worksites who often employ low-wage workers. Low-wage workers have limited access to and participation in workplace health promotion programs. A CBPR approach was used to engage the organization and its employees. Health promotion planning models and publicly available evidence-based tools were used to assess, plan, implement, and evaluate a workplace health promotion program. The workplace’s capacity for promoting health among its employees was improved. There were sustainable improvements in the health interventions and organizational supports in place. A CBPR approach may be a valuable way for occupational health professionals to build the capacity of smaller workplaces with low-wage employees to address the health promotion needs of their workforces.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Debra Fetherman is an Associate Professor and Director for the Health Promotion Program at The University of Scranton, Scranton, PA. She is a Master Certified Health Education Specialist (MCHES®), American College of Sports Medicine - Certified Exercise Physiologist (ACSM EP-C) and Wellcoaches® Certified Health and Wellness Coach. She has over 29 years of experience in health promotion.
Timothy McGrane is the Director of Human Resources at St. Joseph’s Center, an independent Catholic agency sponsored by the Congregation of the Sisters, Servants of the Immaculate Heart of Mary. Tim is a Society for Human Resource Management Senior Certified Professional, with 17 years’ experience in Human Resources and Staff Development.
Joan Cebrick Grossman, RDN, is an Associate Professor of Kinesiology/Nutrition at The University of Scranton, Scranton, PA. She is a registered dietitian/nutritionist and has more than 25 years combined experience in the field of health promotion.