
Abstract
Background: Uncontrolled bleeding is the leading cause of preventable death from trauma. The Stop the Bleed (STB) initiative provides basic education about bleeding to potential immediate responders. The present study aimed to assess the perceptions of self-efficacy and school preparedness related to responding to a life-threatening bleeding emergency in school personnel at an urban high school. Methods: High school personnel from an urban high school (N = 156) completed a 1-hour STB course that included a didactic and hands-on component. Participants rated their agreement with statements about self-efficacy and school preparedness on a 5-point Likert-type scale, responded to items regarding how school personnel could be better prepared for life-threatening emergencies, and had the option to provide written responses pre- and post-course. Findings: Independent samples t tests revealed that perceptions of self-efficacy and school preparedness increased after the course (p < .001). Before the course, 87% of participants felt they needed training, 80% felt the school needed clearer procedures, and 74% felt the school required more equipment for a life-threatening bleeding incident compared with 63%, 69%, and 78% post-course, respectively. Thematic analysis of written responses revealed that participants desired higher frequencies of STB training, more equipment, clearer school procedures, and realistic training scenarios with students. Conclusions/Application to Practice: The STB course increased both perceptions of self-efficacy and school preparedness in a sample of high school personnel. Qualitative analyses provided insight to personnel’s opinion of STB’s effectiveness and what is necessary to maintain or follow through with this knowledge after completion of the course.
Keywords
Background
The Centers for Disease Control and Prevention (CDC, 2017a) indicates that homicides are among the top 10 causes of death for individuals 15–24 years of age. In fact, 49,000 homicide deaths were recorded in 2017, making it the third most common cause of death (CDC, 2017b). When homicide is characterized by the specific cause of death, 4,391 homicides were caused by firearms and another 266 are due to cutting or piercing injuries (CDC, 2017b). This is especially concerning when considering the concentrated areas where these injuries are taking place.
According to the CDC, of the 12,979 total firearm homicides in 2014, 81% occurred in urban areas (CDC, 2015). Moreover, recent studies using Geographic Information Systems (GIS) have found that violent crimes are not only generally isolated to urban areas, but often negatively impact urban school safety due to their close proximity (Graif et al., 2014; Hermann, 2015; Yang, 2019). Because firearm and cutting/piercing-related injuries are a leading cause of death for those aged 15 to 24 years, and disproportionally impact persons and physical safety of those in urban environments (CDC, 2015), it is reasonable to believe that persons who meet both descriptions, such as high school students attending urban schools, may be at an extreme risk for violent injuries.
According to the 2017 Youth Risk Behavior Surveillance Survey, approximately 8.5% of high school students have been in at least one physical fight on school property (Kann et al., 2018). Other studies indicate that the rate of physical altercations is higher in urban school settings, citing that violent communities may give students access to weapons or cultivate poor psychosocial development leading to fights (Bowen & Van Dorn, 2002). As such, when examining only urban areas surveyed, the median percentage of high school students who have been in at least one fight on school grounds is 9.5% (Kann et al., 2018). Furthermore, the number of urban high school students who have been threatened or injured with a weapon on school property is 7.1% compared with the 6.0% national average (Graif et al., 2014). Based on these statistics, it is important to recognize that students are at risk for violent injuries at school, especially in urban settings.
After the 2012 mass shooting at Sandy Hook Elementary School in Newton, Connecticut, The Joint Committee to Create a National Policy to Enhance Survivability from Intentional Mass Casualty and Active Shooter Events was convened by the American College of Surgeons (2013). Their recommendations, collectively known as the Hartford Consensus, aimed to address education, prevention, and appropriate intervention for similar events to reduce morbidity and mortality in school settings. This laid the groundwork for the establishment of Stop the Bleed (STB), a national campaign enacted by the White House in 2015 (Emergency Medical Services [EMS], 2020). The goal of the STB campaign is to empower and educate potential first responders to life-threatening bleeding situations. Training focuses on identifying characteristics of life-threatening bleeding, while teaching techniques for controlling hemorrhages. These techniques include, but are not limited to, proper use of commercial tourniquets and hemostatic dressings (U.S. Department of Homeland Security, 2015). STB aims to educate individuals who may encounter scenarios where medical attention may not be readily available to treat violent injuries. For example, 7 of the 50 active shooter incidents that occurred in 2016 to 2017 occurred in schools; therefore, appropriate and early intervention is imperative for improved survival rates of victims in schools (Federal Bureau of investigation, U.S. Department of Justice, 2018). After school shooting incidents such as Sandy Hook Elementary School Newton, Connecticut, or Marjory Stoneman Douglas High School in Parkland, Florida, interventions, such as STB, are key to reduce mortality related to life-threatening bleeding when school personnel are educated (Leonard et al., 2016).
Recently several studies have demonstrated STB’s efficacy as an education program. Specifically, one research group found that an STB course provided school nurses with significant improvements in their bleeding control knowledge, self-confidence for appropriate intervention in case of emergency, belief in school preparedness, and hands-on skills for tourniquet application and wound packing (Latuska et al., 2019). In nonmedical personnel, an STB course increased bleeding control knowledge, hands-on skill, and perceived ability to react in an emergency situation (Zwislewski et al., 2019). These two studies expanded upon Ross et al.’s (2018) original study that displayed how STB training could improve willingness and confidence to correctly apply a tourniquet in nonmedical personnel, while prior studies demonstrated that simply providing education and instruction can increase one’s ability to apply tourniquets (Goolsby et al., 2015, 2018; Ross et al., 2018).
Given the success of previous STB programs and the increasing rates of school violence, high school personnel could benefit greatly from STB courses. Yet, to date only one study has examined STB within an educational environment (Latuska et al., 2019). Due to a small sample size and the participants having preexisting medical knowledge (school nurses) in the aforementioned study, it was difficult to determine how STB improved high school personnel’s perception of school safety and preparedness in case of school violence (Latuska et al., 2019). This is especially important to consider when assessing perceptions of school preparedness since school nurses may have differing points of view from other high school personnel without a medical background. In addition, previous STB studies have only analyzed data through quantitative measures but have not utilized participant feedback through qualitative analyses. Therefore, it may be useful to not only analyze perception of skill development, but also understand what works and what does not by providing participants with the ability to reflect on the STB course. Therefore, the objectives of this program were to increase confidence in self-efficacy and perceptions of school preparedness in responding to a life-threatening bleeding event at an urban high school while shedding light on areas of the STB program that worked well or could be improved in the future.
Methods
This study used an explanatory sequential mixed-method approach. An explanatory sequential design allows for the use of traditional quantitative measures such as Likert-type scaled items to be given as the main mode of data collection, while being supported by qualitative responses such as short answer and reflection questions to understand more about the participants’ experiences (McCrudden & McTigue, 2019). While the quantitative data provides more robust findings pertinent to the research goals, the qualitative data can be used to understand why individuals answered items in particular ways or as a mechanism to understand how processes can be improved (McCrudden & McTigue, 2019).
Two classes were hosted in an auditorium at an urban high school that serves over 2,000 students annually in the northeast region of the United States at the school’s monthly Professional Development Day. Personnel (N = 156) comprised teachers, security, and ancillary staff. All personnel had the opportunity to participate in two 10-minute surveys that included Likert-type scale and open-ended items. Data related to perceptions of self-efficacy and school preparedness were collected from 156 personnel before the intervention and 126 personnel following the intervention. The response rate decreased for the post-survey due to collection upon exiting the course, which resulted in several not being completed or turned in. Institutional Review Board (IRB) approval was obtained from Drexel University prior to data collection.
Study Protocol
Following IRB approval, administrative personnel at an urban high school were contacted and provided permission to the research team to teach the STB course to school personnel. School personnel received two surveys, one before and one after the STB course. The school personnel rated their agreement with statements about perceptions of self-efficacy and school preparedness for a life-threatening bleeding event on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree) prior to the STB training on a pen-and-paper survey to determine baseline perceptions. In addition, personnel answered a check all that apply multiple-choice question related to how personnel could be more prepared to respond to a life-threatening emergency, with the following options: (a) equipment, (b) training, (c) establishing clear procedures, and (d) other for written responses. They were then asked to respond to an open-ended response where they were asked to reflect on what could be improved in their school related to emergency preparedness.
Once all questionnaires were collected, school personnel completed the 1-hour STB basic bleeding control (BCON) training course that included didactic and hands-on components (National Association of Emergency Medical Technicians, 2015). The first portion of the lecture consisted of the STB presentation created by the ACS Committee on Trauma (The Committee on Trauma, 2017). Following the presentation, school personnel split into groups for hands-on training in a 10:1 student/trainer ratio. Each group practiced wound packing on a Hemorrhage Control Trainer (Z-Medica/QuikClot, Wallingford, CT; Z-Medica, 2020) and self-and-buddy rescue application with a Combat Application Tourniquet (CAT; C-A-T Resources, Inc, Rock Hill, SC; Combat Application Tourniquet, 2020). Following the lecture and hands-on portions of the course, school personnel returned to their seats and completed a post-course questionnaire with the same three questions as the pre-course questionnaire, as well as an open-ended question asking participants to reflect upon the program and provide suggestions on what worked well, what did not, and other general comments. School personnel were not asked to provide their name or any other identifying information to help encourage honesty about the school’s preparedness and to allow for participants to feel comfortable during open-ended responses.
Data Analysis
Initial data analyses included reviewing data and identifying outliers or cases where survey responses were incomplete. Descriptive preliminary analyses such as calculating means, standard deviations, and percent changes on Likert-type-scored items were calculated. To determine the impact of the training on school personnel’s perceptions of self-efficacy and school preparedness, independent samples t tests with associated effect sizes to display the magnitude of change were calculated using R Studio (R Core Team, 2017). Open-ended responses and qualitative data were thematically analyzed using QSR NVivo 12 software (QSR International, 2020). Thematic analyses involved identifying initial broad themes, clustering these based on similarity, and then grouping them into overarching and more encompassing themes with definitions (Braun & Clarke, 2006). Following Creswell and Plano Clark’s guidelines for holistic theme generation, the present study used deductive reasoning to apply themes to knowledge gained from quantitative analyses (Creswell & Plano Clark, 2014). It is important to note that data were analyzed by an author who did not participate in the training as to limit biases.
Findings
Quantitative Findings
Prior to the training, school personnel (n = 156) neither agreed nor disagreed that they had the ability to respond to a life-threatening bleeding situation (M = 3.04; SD = 1.61). Following the STB education, school personnel (n = 126) agreed that they felt better able to respond to a life-threatening bleeding situation (M = 4.05; SD = 1.08). The increase of self-efficacy from pre-to-post education was statistically significant and the training displayed a medium-to-large effect size; t(281) = −7.36, d = .74 (p < .001; Figure 1). In addition, school personnel rated their perceptions of school preparedness higher on the post-education questionnaire (M = 3.85; SD = 1.00) than on the pre-education questionnaire (M = 2.85; SD =1.23). This change from pre-to-post education was significant and a large effect size was reported; t(281) = −8.11, d = .89 (p < .001). Specific preparedness needs for training and clear procedures both decreased significantly (p < .001) after the STB course, while the need for equipment in the school increased slightly after the course (Figure 2).
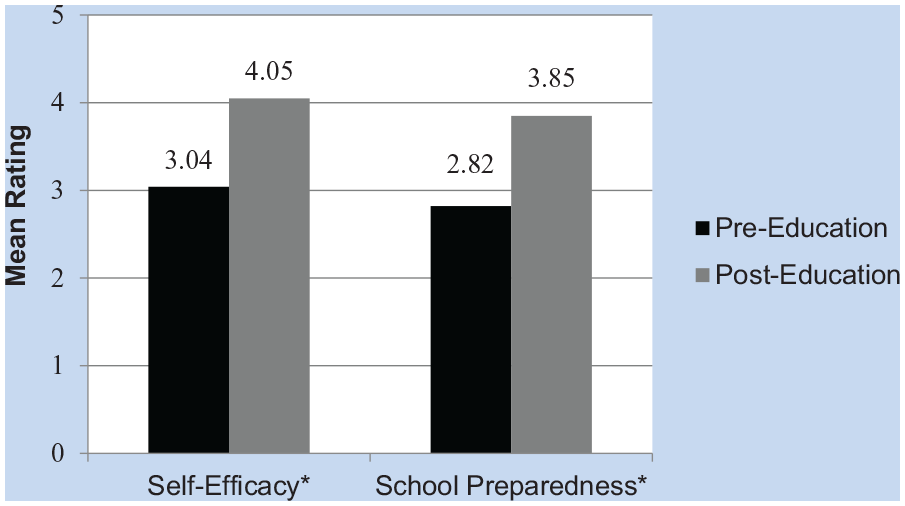
Pre- (n = 156) and post-education (n = 126) perceptions.
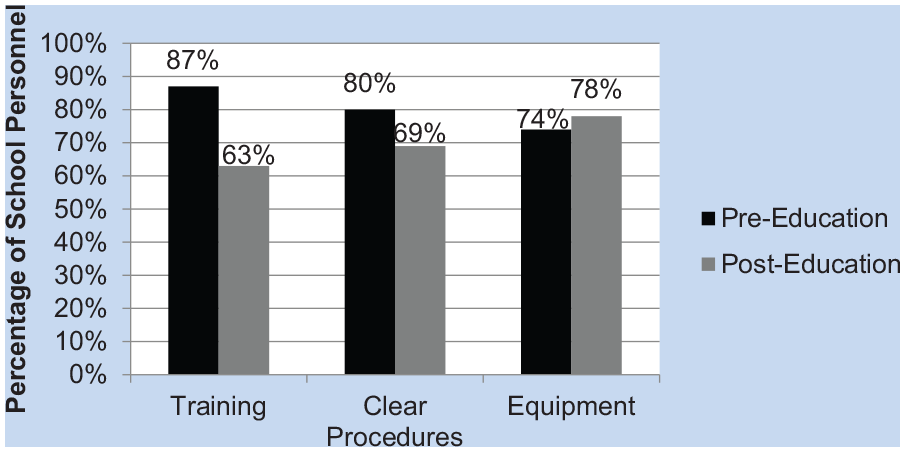
Pre- (n = 156) and post-education (n = 126) comparisons of specific preparedness needs.
Qualitative Findings
School personnel reported 14 unique themes related to their experiences during and recommendations following the STB course. During the data analysis process, these were condensed into four specific categories based on similarities and generalizability across participants. Each theme was defined, described, and exemplar quotations from the school personnel was introduced. The four themes were (a) frequency of trainings, (b) development of clearer school procedures, (c) equipment availability and location, and (d) realistic training integrating students.
Frequency of trainings
School personnel noted that while one training session was useful for learning purposes, regular trainings would be necessary to actually use this knowledge in practice. Specifically, personnel described that the information was helpful; however, it was slightly overwhelming for one session. One participant stated, “[We] need ongoing training . . . Maybe monthly or semi-annual to provide us with more information.” Another participant said that the training was appropriate for surface level learning but does not know if they would be able to recall the information, “This was just enough information to allow me to understand how to respond [in an emergency situation].” Moreover, participants said that STB training was effective for the current staff, but at urban schools, where turnover rates are high, more training was necessary so that all staff was up to date on the training. One participant said, “We need training every year . . . We have a lot of turnover at the school.”
Development of clearer school procedures
School personnel discussed in detail how the STB training alerted them to their school’s lack of preparedness and set procedures in the case of a life-threatening bleeding event. For example, one school personnel member stated, “I think we need to have clear procedures . . . Have everyone practice how to communicate in a life-threatening emergency.” While many felt communication was a potential issue, others felt the school needed to have specialized and trained staff on site to respond to emergency situations. One wrote, “Designated individuals should receive further training,” while another responded, “More nurses should be on call [in the case of an emergency] and involved [in the training].” Individualized training for special responders, and clearer procedures seemed to be a large portion of what was described in the responses. Yet, another participant stated that the training and procedures for designated staff may not be appropriate depending on where the emergency occurs and suggested that signage for nonspecialized members be posted around the school. They stated, “Our school needs to develop clear signage . . . Simple directions in multiple locations to help in these situations.”
Equipment availability and location
School personnel described that the inability to train with equipment in the location where it would be during a life-threatening emergency was a downfall of the training. Participants described that the information session should occur on one day and then equipment would be placed in the locations in the school where it would be in case of an emergency, followed by hands-on training. Related to this, one participant said, “Practice on actually retrieving the supplies from the locations where it will be stored would be helpful.” Others echoed these concerns stating that the program gave them information, but not all of the appropriate supplies and information about who will have the safety kits after the program. One school personnel member noted, “I think we need more kits in a building with over 2,000 people . . . We also need follow up on where these kits are located.” Therefore, providing initial information was helpful, but school personnel agreed that follow-up related to the placement of kits from their administration was of utmost importance.
Realistic training and integrating students
School personnel indicated that while they felt the training provided them with appropriate knowledge of what to do in the event of life-threatening bleeding, they did not feel the hands-on portion of the STB training appropriately simulated the situations they would actually encounter. One participant noted this regarding the hands-on portion of the training, “Making the practice session more like a real-life emergency situation would be good.” Other participants reiterated this feeling by adding that students should be involved, as they may encounter these situations before school personnel could be available. Multiple participants described that students should be, “involved in the trainings” or that STB curriculum could be integrated in health class curriculums. One school personnel member asked, “Can health classes get teaching kits?” Making realistic training scenarios with student body involvement seemed like a way that information could be spread, and education could be self-driven by both students and school personnel.
Discussion
The high risk of violent injury seen in individuals aged 15–24 years, in school settings, and in urban environments, puts high school students attending urban schools at increased odds for life-threatening bleeding. Members of the community who may serve as potential first responders include teachers, school security guards, and other supporting school staff members. Thus, the need to provide and evaluate learning opportunities in this group is imperative to ensure school safety. This study aimed to assess the change in self-efficacy, perceptions of school preparedness, and allow school personnel to reflect on the program following an STB educational seminar with associated didactic, hands-on training.
Results from our study found that school personnel’s self-efficacy increased in terms of their perceived ability to respond appropriately to life-threatening bleeding after an STB education seminar and hands-on training. In the current sample, the training produced a significant (p < .001) change from pre-to-post with a large effect size, indicating the program’s effectiveness. These results are similar to those seen in school nurses following a similar intervention (Latuska et al., 2019). However, in the latter study, STB education and hands-on training also led to higher levels of knowledge and hands-on skills, which stood as a foundation to explore how these elements could impact perceived self-efficacy levels. It should be noted that the present study, where Latuska and colleagues (2019) used a small sample population that had preexisting medical backgrounds. For this reason, the present study extends literature by uncovering improvements in knowledge and life-saving techniques in laypersons (school personnel) following the same STB intervention.
The present study has similar findings of improvement in knowledge after STB training Zwislewski and colleagues (2019) who used STB in a sample of 298 nonmedical personnel. Regardless of whether or not participants received an educational seminar or an educational seminar and didactic, hands-on training, knowledge about life-threatening bleeding was higher when compared with preintervention findings (Zwislewski et al., 2019). Our findings also support Goolsby et al. who showed that knowledge alone has the ability to improve successful tourniquet application in laypersons (Goolsby et al., 2015, 2018). Ross and colleagues (2018) findings showed that knowledge and hands-on training had the ability to improve tourniquets application skills in nonmedical personnel. To appreciate the role of hands-on training, Zwislewski and colleagues (2019) provided evidence that didactic, hands-on training had the ability to improve tourniquet application skills with an educational seminar leads to better tourniquet application and wound packing techniques compared with an educational seminar alone. Given the increases in tourniquet application ability and knowledge after these studies, the present study measured perceived self-efficacy after these seminars, as simply teaching the knowledge and completing tourniquet application in a safe setting does not necessarily mean that those individuals will feel able to do that in a real scenario. Therefore, the present study provided initial evidence that didactic, hands-on STB training positively impacted perceived self-efficacy.
Overall, the perceptions of the school preparedness also significantly increased following the STB intervention (p < .001). While the current study sample reported a high baseline response for school preparedness, the large effect size conveys a significant magnitude of effectiveness of the STB program where personnel felt more prepared in the case of a hemorrhagic emergency. This was supported by qualitative analyses where participants indicated that they felt the STB program gave them appropriate initial education in the case of emergencies. These findings are similar to previously mentioned studies that assessed school nurses, which to our knowledge is the only other study assessing STB efficacy in a school environment (Latuska et al., 2019). In particular, areas that participants improved upon were the participant’s feelings toward their school establishing clearer protocol (see Figure 2). This was supported by qualitative analyses where participants indicated that the STB course illuminated the gaps in their school’s current structure to handle life-threatening events. Perhaps one solution could integrate the student body and security into the discussion to spark conversations among administration around violence prevention, which has been shown to promote awareness and education in school settings (Connell, 2018). This was also described by school personnel who felt that the education’s impact would be more salient if specialized staff and students received the training.
The desire for additional training following the intervention decreased from 87% to 63%. While fewer participants thought they needed training, 63% was still a substantial number who indicated that further training was necessary in school settings. Specifically, this 63% was represented through qualitative analyses where they indicated that monthly, semi-annual, or annual training was necessary for school personnel to recall information and to introduce them to these topics again. This is especially important for urban school settings, where turnover rate is significantly higher than schools not located in cities (Hanushek et al., 2004). Qualitative analyses from the present study revealed that school personnel felt like specialized staff should receive more training on STB, such as health and physical education teachers, nurses, or security guards. This could serve as a fruitful avenue for future research and possibly a way that schools could have trainers on staff to speak with new employees.
There was a slight increase from 74% to 78% in the number of participants who believed their school needed more equipment following training. Other studies have noted that not having appropriate equipment after the training was a common response after STB education (Latuska et al., 2019; Zwislewski et al., 2019). However, this should not come as a surprise when considering the emphasis in the training related to the use of proven, commercial tourniquets and medicated gauze for adequate bleeding control, along with the convenience of having multiple bleeding control stations throughout a campus to ensure rapid intervention or easy accessibility during a lockdown event. This was echoed by school personnel in the present sample who felt that while the education was great, their student population was too great for the amount of kits (n =18) that were provided to them after the course. Future considerations should potentially bring kits to the trainings and discuss their placement with all of the school personnel to bring clarity on their locations.
To speak to this, the research team returned to the school following the STB course to donate bleeding control kits and stations. Key stakeholders from the school met with the research team to determine optimal placement for bleeding control stations and kits. A decision was made to place two bleeding stations, containing eight bleeding control kits, at both of the main entrances to the school so they could be accessed easily by responders. The group also decided that the 18 individual kits would be placed at each corner of the main hallways at security stations for easy accessibility for classrooms. The research team strongly recommended sending a form of mass communication to all school personnel to let them know the location of each of the stations and kits to close the loop on the need for clear procedures and additional equipment; however, it is unclear whether this happened or not.
Demographic data were not collected as a part of these educational training sessions, which limits the generalizability of the findings. The inability to track participant responses also limited the ability to perform advanced statistical testing to understand which staff members changed the most. Although all of the school personnel in this training seminar were from the same urban high school located in the northeast region of the United States, personnel varied in occupation (e.g., teachers, security, or aides), which does help to increase the external validity of our findings to other large school settings that may have many different staff members participating in the course. Another limitation was that the auditorium where the training was held was rather large with uncontrollable acoustics and a small projector screen; therefore, individuals who arrived just before the training started sat in the back as to not distract those in the closer rows, and might not have had a seat with an appropriate view of the projector. Given the voluntary and unpaid nature of the survey component, school personnel may have had limited investment in completing the pre-and-post course assessments, which may partially explain the decrease in the number of pre-to-post course responses.
Future studies should consider investigating follow-up with schools after the STB course to see if school personnel were made aware of the locations of the training kits and their perceptions of self-efficacy were long-lasting. Furthermore, future investigations are necessary to understand which school personnel group benefits the most from the trainings and to implement school specific needs, through the implementation of semistructure interviews and case-study designs. This would help inform future researchers and practitioners in ways they can appropriately structure the STB programming and to improve its quality. Methodologically, STB literature would benefit greatly from a longitudinal design where self-efficacy, school preparedness, and skills assessments were completed over the course of several years. Moreover, understanding how school personnel’s perceptions of school safety and how providing these trainings can impact administrative changes (e.g., gun safety plans or mandatory trainings) should be a key tenant of future community outreach work using the STB curriculum.
Implications for Occupational Health Practice
While not in a traditional allied health setting, the current study extends the literature describing the efficacy of prevention programs, such as STB, in workplace environments to ensure safety when medical assistance is not readily available. Researchers from different countries (see Qureshi et al., 2018) have attempted to integrate first aid skills and life-threatening bleeding prevention into school settings; yet, the United States has yet to make this a requirement for school personnel. The present study is the first to measure STB’s effectiveness in nonmedical personnel in school settings and provides a foundation of how a short course could be beneficial for individuals’ perceptions of their ability to respond in a life-threatening bleeding situation. In the present study, school personnel received a 1-hour training which improved their self-efficacy and perceptions of school preparedness. This 1-hour training can be made available at relatively low cost through government or EMS resources (Jacobs et al., 2014) and could possibly be integrated into all school’s mandatory in-service training days.
Moreover, the present study utilized multiple forms of data collection, through a mixed-method design, which is a novel approach to examine STB. Because of this, qualitative themes have provided possible insight on how this training could be applied to other schools and settings. Specifically, participants indicated that the training could be combined into other forms of learning such as classroom settings for students or school personnel training days, rather than an annual training, to provide this education more frequently and make it a part of school readiness. Therefore, STB could be extended outside of school settings, such as sports or daycare, where adults are supervising children and ensuring their safety.
Conclusion
With increases in school violence, especially in urban areas, and with teenagers (aged 15–24 years) being at the greatest risk for violence, STB training for school personnel should be endorsed to help protect students and staff. The present study displayed STB training’s ability to improve self-efficacy and perceptions of school preparedness. This study used an exploratory sequential mixed-method approach to provide qualitative data to support quantitative findings. The novel use of a mixed-method design provided additional explanation of the quality of the STB program and how it could be improved from the perspective of the participants which fills in a critical gap in the literature. The levels of perception for school preparedness can be improved upon by developing clear school-wide protocols, providing more frequent STB training sessions, increasing the availability of equipment, and giving school personnel more realistic training scenarios. Furthermore, endorsing STB, or similar basic bleeding control training programs, should occur at the level of both policymakers and educators to ensure personnel are prepared for such life-threatening bleeding emergencies on school grounds. Overall, in the event of an emergency from which uncontrolled hemorrhage is the result, being adequately informed and trained may assist in saving lives.
Applications to Professional Practice
After several violent school shootings, ensuring safety of both students and school personnel is essential. Schools in urban settings are more likely to experience violence and have an increased risk to experience life-threatening bleeding events. The present study measured the effectiveness of a Stop the Bleed (STB) course on urban school personnel’s perceptions of self-efficacy and school preparedness in the case of a life-threatening bleeding event. The program found that a 1-hour course significantly increased perceptions of self-efficacy and school preparedness, while qualitative responses revealed ways to improve the program, such as integrating it into course curriculums or offering it more frequently. Findings show the importance of offering such information to nonmedical personnel, even if it is just for a short period of time. The present study’s findings show the importance of STB education to all nonmedical personnel who may serve as first responders in the event of life-threatening bleeding.
Footnotes
Acknowledgements
The authors would like thank the American Trauma Society-Pennsylvania Division for funding to provide school personnel with bleeding control kits and stations
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Autumn D. Nanassy is the sponsored programs coordinator at St. Christopher’s Hospital for Children in Philadelphia, PA, and is also a part-time lecturer in psychology at Rutgers University-Camden.
Richard L. Graf is a medical student at Drexel University’s College of Medicine.
Ross Budziszewski is the trauma research coordinator at St. Christopher’s Hospital for Children in Philadelphia, PA.
Rochelle Thompson is the injury prevention coordinator at St. Christopher’s Hospital for Children in Philadelphia, PA.
Adam Zwislewski is the trauma educator and outreach coordinator at Hahnemann University Hospital in Philadelphia, PA.
Loreen Meyer is the trauma program manager at St. Christopher’s Hospital for Children in Philadelphia, PA.
Harsh Grewal is the director of trauma services at St. Christopher’s Hospital for Children in Philadelphia, PA, and a professor of surgery and pediatrics at Drexel University’s College of Medicine.