
Abstract
Background
Nearly half of U.S. pediatricians have symptoms of burnout. This pilot study examined the feasibility of a 6-week yoga-based program (RISE) for neonatologists and obstetricians at Brigham and Women’s Hospital and studied the effects on burnout, professional fulfillment, and psychological health.
Methods
Participants were recruited via email to participate either in both program and research study, or exclusively the program. RISE was delivered 1 hour/week during the workday for 6 consecutive weeks either in-person or remotely; 18 physicians participated, 12 completed post-program, and 11 completed 2-month follow-up. The questionnaires assessed burnout and measures of psychological health, professional fulfillment, work exhaustion, interpersonal disengagement/burnout (PFI), mindfulness (FFMQ), perceived stress (PSS), positive/negative affect (PANAS), resilience (RS), anxiety/depression/sleep disturbances (PROMIS), at baseline, post-program, and 2 months after RISE.
Findings
Average attendance in-person was 2.8 sessions and remotely 1.4 sessions (4.2/6 sessions). Participants demonstrating total burnout reduced from 50.0% at baseline to 9.1% post-program. Participants demonstrating professional fulfillment were 8.3% at baseline and 27.3% post-program. Paired samples t-tests revealed statistically significant improvements in burnout, professional fulfillment, interpersonal disengagement, stress, resilience, anxiety, and depression at post-program compared with baseline (N = 12, all ps < .05). At 2-month follow-up, statistically significant improvements in interpersonal disengagement, resilience, and mindfulness (N = 11, all ps < .05) compared with baseline were reported.
Conclusions/Application to Practice
RISE is feasible within a workday and may address burnout and other psychological health measures in physicians with effects potentially sustainable over 2 months. Occupational health practitioners in health care should consider this type of intervention for their workers.
Background
Burnout is a work-related syndrome, which includes depersonalization, emotional exhaustion, and reduced sense of personal accomplishment (Lall et al., 2019), affecting approximately 50% of U.S. physicians (Shanafelt, West, et al., 2019). The well-documented consequences of physician burnout include a negative impact on physicians’ health and safety, quality of patient care (Tawfik et al., 2019), physician professionalism (Dyrbye et al., 2010, 2020), and compromise of the viability of health care systems (Shanafelt, Trockel, et al., 2019). Interventional trials to prevent or reduce physician burnout include individual-focused as well as organizational strategies, summarized in systematic reviews and meta-analyses (Kalani et al., 2018; West et al., 2016).
A recent study demonstrated burnout in neonatal intensive care units associated with high-patient volume and the use of electronic health records (Tawfik et al., 2017). Burnout rates were also high in physicians practicing in obstetrics and gynecology (OBGYN; Iorga et al., 2017). Medical professionals working in neonatal intensive care and obstetrics may be sensitive to burnout due to the high proportion of females. A sex-specific increased gap between ideal and actual lives being higher in women physicians, lack of workplace control, reproductive concerns, higher work contributions at home alongside work (Fronek & Brubaker, 2019), as well as decreased self-valuation in female physicians (Trockel et al., 2019) may be contributing factors toward gender-specific differences in burnout prevalence.
Individual-focused interventions can prevent or reduce burnout among physicians (West et al., 2016). Mindfulness-based approaches have demonstrably improved physician well-being and decreased burnout (Hamilton-West et al., 2018; van Wietmarschen et al., 2018). A recent review suggests yoga was effective in managing stress and burnout in health care workers, but more methodologically sound research is needed (Cocchiara et al., 2019). Mind–body interventions demonstrate an impressive effect on how stressful situations are experienced (Jeter et al., 2015; Ludwig & Kabat-Zinn, 2008). Yoga is a multicomponent mind–body practice comprised of postures, movement, breath regulation, relaxation, and meditation/mindfulness. Yoga practices are easily learned and implemented, simple, and cost-effective. The yoga-based RISE (Resilience Integration Self-awareness Engagement) program has been shown to reduce stress and anxiety while increasing resilience and mindfulness in professionals (Trent et al., 2018, 2019).
The purpose of this pilot study was to examine the feasibility of the yoga- and mindfulness-based RISE program for improving measures of burnout and psychological health in faculty neonatologists and obstetricians at a large medical center for high-risk pregnancies and medical care for very sick newborns and their mothers.
Methods
The Brigham and Women’s Hospital (BWH) OBGYN and Pediatric Newborn Medicine Departments have 50 and 43 faculty physicians, respectively. An email invitation to attend RISE with or without research participation was sent to all 93 physicians 2 weeks before the program started. Those who agreed to be in the research aspect of the program were sent a link to a survey 10 days prior to the program. A total of 18 physicians enrolled in the study and completed the baseline measures.
The RISE program consisted of six 1-hour sessions delivered over 6 weeks in accessible conference rooms. RISE included yoga postures, guided meditation, mindfulness practices, breathing techniques, and discussions about mindful eating/sleep practices. Gentle, accessible techniques were used because most participants were new to yoga and had undergone varying levels of stress or burnout. Live participation in RISE was encouraged; however, links to participate remotely via computer in real time or asynchronously were given. Participants were encouraged to practice RISE techniques daily for 20 to 30 minutes.
The study was approved by Partners Healthcare Institutional Review Board.
Data Collection
Surveys were administered online via the Research Electronic Data Capture (REDCap) electronic data capture tools at baseline (1–10 days pre-program), post-program (1–10 days following RISE), and 2 months post-program. Participants completed a demographic questionnaire pertaining to age, gender, race, and ethnicity. Professional fulfillment Index (PFI; Items 1–6), work exhaustion (Items 7–10), interpersonal disengagement (Items 11–16), and total burnout (Items 7–16) were assessed using the 16-item Stanford Professional Fulfillment Index, which is a valid and reliable scale (Trockel et al., 2018). Items are scored 0 to 4. Each dimension is treated as a continuous variable. Scale scores are calculated by averaging the item scores of all the items within the corresponding scale. Scale scores can then be multiplied by 25 to create a scale range from 0 to 100. Higher score on the professional fulfillment scale is more favorable. In contrast, higher scores on the work exhaustion or interpersonal disengagement scales are less favorable.
Mindfulness was measured using the 15-item Five Facet Mindfulness Questionnaire (FFMQ), which is a validated and reliable scale (Baer et al., 2008) across five dimensions of mindfulness (observation, description, acting with awareness, non-judgmental inner experience, and non-reactivity to inner experience) although only the total mindfulness score was reported. FFMQ is a predictor for positive thinking, an overall uplifted mood, and subjective feelings of well-being and tests whether mindfulness is related to a decrease in clinical symptoms of depression, anxiety, and stress. Responses in the scale are made on a 5-point Likert-type scale, without a direct cut point, and the summation of the direct and reverse-scored items gives the total score. A total possible score ranges from 3 to 15 for each of the five facets that in sum compose a total mindfulness score with a higher score indicating a higher degree of mindfulness.
The Perceived Stress Scale (PSS) is a reliable and valid 10-item scale (Cohen et al., 1983) used to identify how unpredictable, uncontrollable, and overloaded study participants find themselves. Participants are asked to respond to each item on a scale ranging from 0 (never) to 4 (very often). A total PSS score ranges from 0 to 40 with higher scores indicating higher perceived stress levels.
The Positive and Negative Affect Schedule (PANAS) is a valid and reliable measure consisting of 10 items of positive mood terms and 10 items of negative mood terms which participants were asked to assess the extent to which they experienced them (Watson et al., 1988). The mood terms are attentive, interested, alert, excited, enthusiastic, inspired, proud, determined strong, active, distressed, upset, hostile, irritable, scared, afraid, ashamed, guilty, nervous, and jittery. Scores for each item can range from 1 to 50 with higher positive mood scores representing higher levels of positive affect with momentary and weekly means being 29.7 (SD = 7.9) and 33.3 (SD = 7.2), respectively, and lower negative mood scores representing lower levels of negative affect. Mean scores for momentary and weekly negative mood scores are 14.8 and 17.4, respectively.
The Resilience Scale (RS-14) is a valid and reliable 14-item scale used to measure participants’ level of resilience, a positive personality characteristic that enhances individual adaptation. Resilience as construed by Wagnild comprises of five essential characteristics: meaningful life, perseverance, self-reliance, equanimity, and existential aloneness. This 14-item scale assesses these characteristics on a scale from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating higher levels of resilience and has demonstrated high reliability and validity (Wagnild, 2009). Anxiety, depression, and sleep disturbance were measured using the valid and reliable PROMIS (Patient-Reported Outcomes Measurement Information System; Pilkonis et al., 2011). PROMIS covers 300 measures of physical, mental, and social health. Anxiety and depression are mental health measures (two items/questions); sleep disturbance is a physical health measure (two items/questions). Measures provide a common metric: the T-score (M = 50, SD = 10). In most cases, 50 equals the mean in the U.S. general population. The Credibility Expectancy Questionnaire (CEQ) is a two-item scale modified for this study, which measures the degree to which the individual feels that a treatment or program will be beneficial. Revised items asked: (a) “At this point, how much do you really feel that the Kripalu program will help enhance your quality of life?” (rate 1 = not at all to 9 = very much) and (b) “By the end of the Kripalu program, how much improvement in your quality of life do you really feel will occur?” (rate 0% to 100%).
Data Analysis
Online questionnaires were distributed at baseline (1–10 days pre-program), post-program (1–10 days following RISE), and 2 months post-program Paired samples t-tests were performed to compare the differences in questionnaires from baseline to post-program and from baseline to follow-up. A p-value less than .05 was considered significant. No adjustments were made for multiple outcome measures (e.g., Bonferroni) based on the relatively small sample size and the pilot nature of the study. All quantitative data were analyzed using IBM SPSS version 24.0 (IBM Corp., Armonk, NY).
Results
Participant demographics are displayed in Table 1. Of the 18 RISE participants who enrolled in the study and completed the baseline measure survey, 12 participants (67%) completed the post-measure surveys and 11 (61%) completed the 2-month follow-up survey.
Participant Demographics, and Professional Fulfillment Index (PFI) at Baseline.
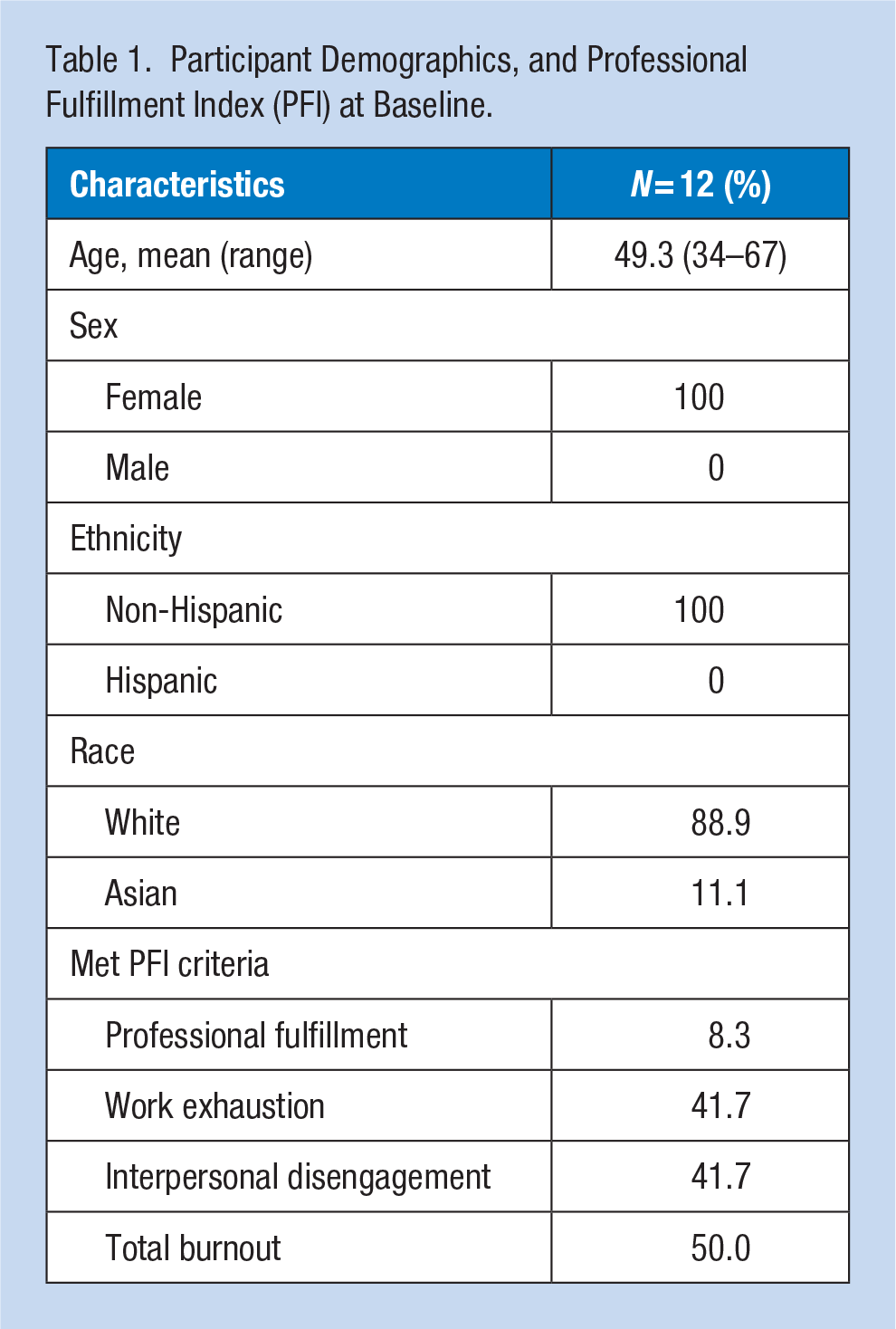
For the PFI results, at baseline, 41.7% of participants met criteria for burnout for work exhaustion, 41.7% for interpersonal disengagement, 50% for total burnout, and 8.33% for professional fulfillment. At 1 to 10 days post program, 9.1% of participants met criteria for work exhaustion, 0% of participants for interpersonal disengagement, 9.1% of participants for total burnout, and 27.3% of participants for professional fulfillment. At 2-month follow-up, 30% of participants met criteria for work exhaustion, 10% of participants for interpersonal disengagement, 20% of participants for total burnout, and 30% of participants for professional fulfillment. From baseline to post, there were statistically significant improvements in professional fulfillment, t(10) = 2.81, p = .018, interpersonal disengagement dimensions of burnout, t(10) = −2.50, p = .031, and total burnout, t(10) = −2.27, p = .047, compared with baseline (Figure 1). At the 2-month follow-up compared with baseline, there were statistically significant improvements in interpersonal disengagement, t(9) = 2.43, p = .038, but no longer outcome measure (all ps > .05).
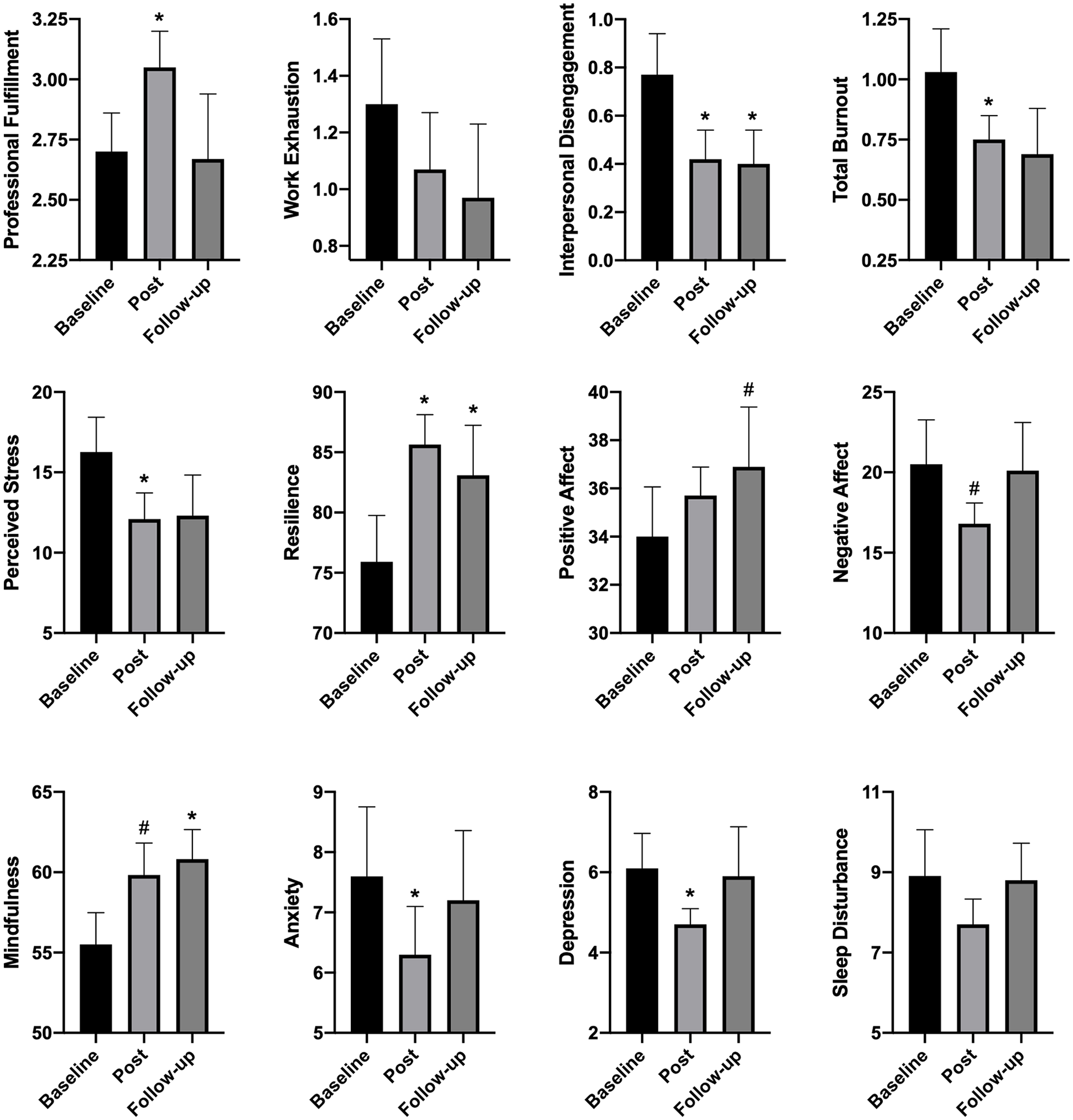
Participant mean scores and standard errors on psychological health and well-being measures at baseline, post-program, and follow-up.
At post-program compared with baseline, there were statistically significant improvements in perceived stress, t(10) = −2.52, p = .031; resilience, t(10) = 3.57, p = .005; anxiety, t(9) = −2.33, p = .045; and depression, t(9) = −2.59, p = .029. There was also a trend for an increase in mindfulness, t(11) = 2.05, p = .065. At the 2-month follow-up compared with baseline, there were statistically significant improvements in mindfulness, t(10) = 3.06, p = .012, and resilience, t(9) = 2.72, p = .024. There was also a trend for an increase in positive affect, t(9), p = .054. There were no changes in sleep disturbance or work exhaustion at any time point (all ps > .05). In addition, there were significant positive correlations between baseline program expectation and improvements in psychological health measures, including mindfulness, r(11) = .64, p = .033; stress, r(11) = −.67, p = .024; resilience, r(11) = .73, p = .011; positive affect, r(10) = .83, p = .003; and depression, r(10) = −.67, p = .035.
Program Evaluation
At baseline, participants rated that the RISE program would help enhance their quality of life with a mean of 4.83 (SD = 1.38), and their expected improvement in quality of life as a mean of 34.4% (SD = 14.23). Post program, participants (n = 12) reported that they attended a mean of 2.8 sessions (SD = 1.47) in person and a mean of 1.4 sessions (SD = 1.29) remotely. Post program, participants reported practicing RISE 2.4 days (SD = 1.89) per week for an average of 9.6 minutes (SD = 6.50). At the 2-month follow-up, the results were sustained.
Discussion
This pilot study aimed to examine the feasibility of delivering a 6-week workplace yoga-based program (RISE) to faculty neonatologists and obstetricians and to study the effects on physician burnout and professional fulfillment. Physicians could attend the weekly RISE session in person or via remote viewing. After the program, the 12 participants reported that they attended a mean of 2.8 sessions in person and a mean of 1.4 sessions remotely (for a total of 4.2 out of 6 sessions), which was considered to be evidence of feasibility.
The authors demonstrated that participation in the RISE program improved stress, resilience, mindfulness, negative affect, anxiety, depression, professional fulfillment, interpersonal disengagement, and total burnout compared with baseline. Many of these effects were sustained over 2 months. These results were concordant with the authors’ prior two studies on RISE with professionals (Trent et al., 2018, 2019). Participants reported less burnout at baseline (1.03) than the norm (1.18) reported by Trockel et al. (2018). Selection bias cannot be excluded, as less burned-out physicians may have participated in the study.
RISE resulted in similar improvements in measures of psychological health when delivered over 6 weeks in a hospital setting as compared with a residential 5-day program at a retreat center (Trent et al., 2018), an observation speaking to the value of the content of the program rather than environmental benefits. Accessible mindfulness and yoga practice applied in 1-hour weekly sessions within the work environment appears to induce a sustained increase in resilience. The practices from the program can also be performed by physicians on call as a simple and sustainable practice. Demonstrating this improvement in neonatologists and OBGYN physicians, specialties ranking high in national burnout rates (Iorga et al., 2017) is promising.
This is one of few interventional studies of a yoga- and mindfulness-based program for physicians’ psychological health. One previous study of a combined yoga–mindfulness program also reported decreased burnout as well as increased empathy in physicians (Asuero et al., 2014). Randomized controlled trials of mindfulness-based interventions have demonstrated improvements in burnout in physicians, including facilitated group curricula (West et al., 2014), stress management and self-care training (Martins et al., 2011), and communication skills training (Bragard et al., 2010).
The current pilot study has several limitations. First, use of a single-arm trial with a small sample size is a weak experimental design. Second, participant attendance was low and retention rate for completing the research surveys lower than expected. Third, significant relationships between program expectation and improvements in some measures of psychological health were observed, which highlights the importance of education regarding possible program benefits. Finally, all participants being female and mostly non-Hispanic White limit the generalizability of the study’s findings. Future research will seek to enroll more male participants and individuals with more racial diversity.
In summary, this pilot study may provide initial evidence that physician burnout and other measures of psychological health may be improved following a yoga- and mindfulness-based intervention. This does not imply that systemic and organizational causes of burnout do not have to be addressed. Combining individual-focused and systems-orientated change would be a promising approach for future studies on physician burnout. Future work will include a randomized controlled clinical trial with a larger sample size.
Implications for Occupational Health Nursing Practice
Burnout among health care providers has been linked to suicidality, broken relationships, decreased productivity, unprofessional behavior, and turnover. Increasing attention is being paid to the relationship between health care provider burnout and reduced quality of care. Efficient teamwork and close collaboration between all health care provider types are crucial to work environments that promote the mental and physical health of providers, as well as the quality of care. Additional research is needed to clarify beneficial interventions to reduce physician burnout and well-designed controlled trials to build evidence on their efficacy. The findings of the study suggest that RISE is feasible within a workplace health care setting for improving physician burnout and other measures of psychological health up to 2 months; post program, however, a controlled trial is necessary to confirm these findings.
Applying Research to Occupational Health Practice
Burnout prevalence among health care providers is approximately 50% nationally. This pilot study examined the feasibility of a 6-week, 1-hour per week, Kripalu yoga-based program within the workplace and studied the effects on burnout and psychological health. Participation in RISE led to statistically significant improvements in psychological health at post-program compared with baseline with some effects sustained at 2 months. Simple, brief mindfulness and yoga exercises can be incorporated into the work lives of highly stressed physicians and may demonstrate sustained benefits on burnout and psychological health. Workplace systems-level changes to address this epidemic must continue to be explored.
Footnotes
Acknowledgements
We would like to thank all study participants for their engagement as well as Dr. Terrie Inder, Chair of the Department of Pediatric Newborn Medicine, for her continued support.
Authors’ Note
The yoga program (RISE) being evaluated was developed by and is owned and administered by Kripalu Center for Yoga & Health.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.B.S.K. was funded by a research contract from the Kripalu Center for Yoga & Health to Brigham and Women’s Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Kripalu Center for Yoga & Health and BWH BWell grant (grant recipient AS).
Author Biographies
Annette Scheid is a neonatologist who participated in the program but whose data were excluded from the study.
Natalie L. Dyer is a paid postdoctoral consultant for Kripalu Center for Yoga & Health.
Jeffery A. Dusek was an employee of Kripalu Center for Yoga & Health during the course of the study.
Sat Bir S. Khalsa, PhD, is director of Yoga Research for the Yoga Alliance and Kundalini Research Institute, and assistant professor of Medicine, Harvard Medical School. He has conducted scientific research on yoga for insomnia, stress, anxiety disorders, and workplace and school settings. He coordinates the annual Symposium on Yoga Research, is editor-in-chief of the International Journal of Yoga Therapy, medical editor of the Harvard report Introduction to Yoga, and chief editor of the medical textbook The Principles and Practice of Yoga in Health Care