
Abstract
Background: A drug-free workplace program (DFWP) has been shown to be effective in reducing workers’ drug misuse. The purpose of this project was to determine the need and capacity for a new or enhanced DFWP in a large health system. If determined to be needed, the next step would be to develop, implement, and evaluate a toolkit to assist occupational health nurses to promote a new or enhanced DFWP. Methods: A strategic prevention framework was used to assess the need and capacity for a toolkit to prepare occupational health nurses to promote a new or enhanced DFWP. The project was conducted in the occupational health services department at a large health system in the Midwest U.S. occupational health nurses and employee assistance counselors in the hospital system completed a survey assessing the need and capacity for a new or enhanced DFWP. Findings: A gap was identified in the perceived effectiveness of training about DFWP and current DFWP components. The findings reflect the need and capacity for a DFWP toolkit. Optimally, a DFWP toolkit would include evidence-based drug and alcohol screening tools. We found that a toolkit for occupational health nurses to promote a new or enhanced DFWP in the project site was warranted. Conclusion/Application to practice: A DFWP can be an effective method of promoting workplace health and safety. Occupational health nurses can contact state and national representatives to encourage monitoring of drug-related work injuries to provide evidence to influence health policies to support effective DFWPs.
Keywords
Background
Rarely does a day go by when we do not hear of the U.S. opioid crisis or drug crisis in the national news. The U.S. National Survey of Drug Use and Health ([NSDUH], Substance Abuse and Mental Health Services Administration [SAMHSA], 2017a) defines illicit drugs as including marijuana, cocaine (including crack), heroin, hallucinogens, inhalants, and methamphetamines, as well as the misuse of prescription pain relievers, tranquilizers, stimulants, and sedatives. In 2016, NSDUH (SAMHSA, 2017a), estimated that one in four (23.2%) young adults aged 18 to 25 years reported being current users of illicit drugs, representing about 8.0 million young adults. Of these, it was estimated that 1.8% (n = 631,000) had misused pain relievers in the past month, and 0.3% (n = 88,000) were current heroin users. In this same survey, approximately 8.9% of adults aged 26 years or older were current users of illicit drugs, representing about 18.6 million adults. It was estimated that 1.2% (or 2.5 million) were current misusers of prescription pain relievers (including opioid and nonopioid pain relievers).
The U.S. Bureau of Labor Statistics (2018) estimates that about 144 million U.S. workers aged 16 to 64 years were employed in 2017. Because this age group represents approximately 94% of the U.S. working population, it can be inferred that a significant percentage of the working population may be misusing prescription pain relievers or may be using illicit drugs. Illicit drug use and the misuse of prescription pain relievers among U.S. workers have been found to increase the risk of work-related injuries (Bush & Lipari, 2015). These findings warrant occupational health professionals, including occupational health nurses, nurse practitioners, and employee assistance program (EAP) counselors, to develop strategies for improving employee safety and health.
The American Association of Occupational Health Nurses (AAOHN) released a position statement in 2018, stating, OHNs are well positioned to lead the efforts in the fight against opioid dependence. They are able to provide employee training and education, identify and address opioid use and abuse in the workplace while ensuring confidentiality, and advocate for comprehensive corporate policy making, comprehensive drug testing, and benefit programs. (AAOHN, 2018, p. 3)
Randolph (2017) suggested that occupational health nurses have a responsibility to engage in a multifaceted approach to contribute to the fight against opioid misuse. According to Randolph (2017), the recommended approach includes a review of existing opioid and other drug testing policies in the workplace. Occupational health nurses can emphasize the importance of discussing, with a prescribing provider, whether the use opioids could impede safe performance of job tasks at work and whether a nonopioid medication instead could be prescribed for effective pain reduction. Occupational health nurses also should provide employee education regarding the risk of opioid dependence, possible signs and symptoms of opioid dependence, and resources available such as the workplace EAP and local addiction treatment opportunities.
According to SAMHSA (2019), a drug-free workplace program (DFWP) can assist employers with having workplaces which are safe and healthy. As a valuable component of a DFWP, Waehrer et al. (2016) demonstrated that the presence of a company-staffed EAP improved the health of the working population and reduced work injuries. EAPs were found to be related to a reduction in no lost work time injury rates per 10,000 full-time employee equivalents. Reductions of 17% for employers having more than 50 employees and 14% for employers with more than 100 employees were associated with having access to EAPs (Waehrer et al., 2016).
In considering the magnitude of the U.S. opioid crisis, it is evident opioid misuse affects the U.S. working population. Therefore, occupational health nurses in collaboration with other occupational health professionals are ideally positioned to provide substance use education and promote prevention of substance misuse among the population that he or she serves. Because substance use prevention strategies are not typically included in a general nursing curriculum, occupational health nurses might not be familiar with drug prevention strategies. Occupational health nurses could benefit from a toolkit that includes the tools they need to promote a new or enhanced DFWP in their places of employment.
DFWP
SAMHSA (1990) published guidelines for developing a DFWP to assist nonfederal employers acting on their own or in response to a Federal requirement or incentive. The model drug-free workplace plan was designed to use as a compass but allowing for modifications to fit the unique needs of the employer’s workplace. The model plan provides the essential five elements set out in Executive Order 12564: (a) development of a comprehensive written policy, (b) supervisory training, (c) employee education, (d) availability of EAPs, and (e) identification of illegal drug (Reagan, 1986).
A DFWP seeks to modify behaviors of employees who misuse drugs or fail to report the influence of substance use in coworkers whose roles have the potential to cause injuries to the worker and/or coworkers. In addition, a DFWP provides workplace education regarding the safe use, storage, and disposal of opioids in the home and the avoidance of sharing prescribed opioids (Randolph, 2017).
Although the U.S. Bureau of Labor Statistics (2017) provides data regarding nonmedical drug and alcohol use and related fatal and nonfatal overdoses, data specific to nonfatal drug-related work injuries is more difficult to obtain. In 2016, overdoses from the nonmedical use of drugs or alcohol during work hours increased by 32% from 165 in 2015 to 217 in 2016 (U.S. Bureau of Labor Statistics, 2017). A steady increase in overdose fatalities has been demonstrated by increases of at least 25% annually since 2012 (U.S. Bureau of Labor Statistics, 2017).
Due to the urgency of the need for strategies to reduce drug misuse in the United States, occupational health nurses must be prepared to do their part in contributing to efforts to reduce drug use among the population they serve, the working population. There are toolkits available for businesses and organizations to introduce and enhance a DFWP, but a search of U.S. government websites and the professional literature to find a toolkit designed specifically to equip occupational health nurses and other occupational health professionals to promote a new or enhanced DFWP produced no results. The gap in the literature led to the decision to first explore the need and capacity for developing a toolkit for occupational health nurses to promote a new or enhanced DFWP in their places of employment.
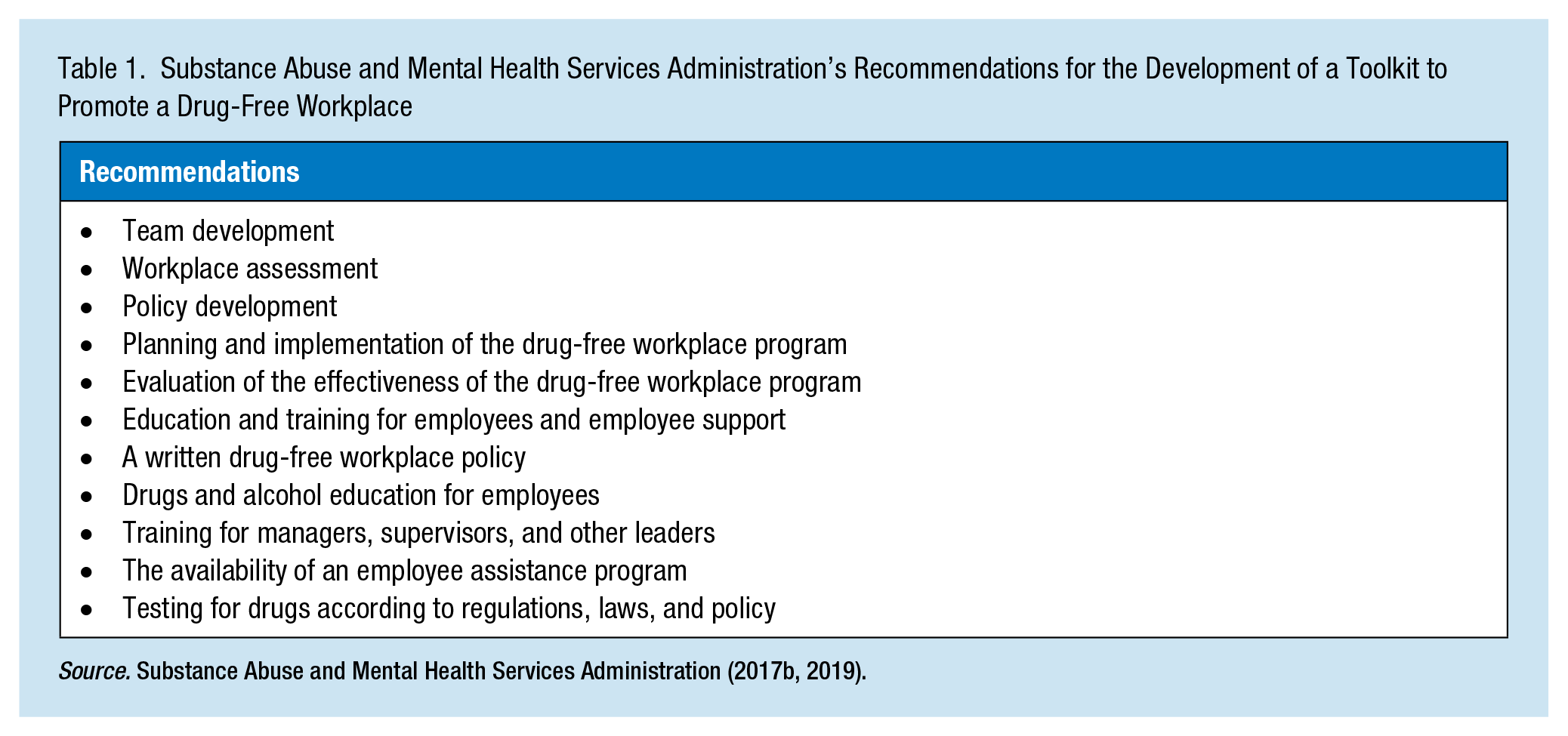
SAMHSA provides recommendations for the development of a toolkit for occupational health nurses, and other occupational health professionals to promote a DFWP are included in Table 1 (SAMHSA, 2017b, 2019). The need for a toolkit is supported by evidence that (a) drug use is a serious health problem in the United States, (b) this problem exists in the working population, (c) the problem increases risk of injury to the worker and others, and (d) a DFWP has been found to effectively reduce drug use among workers and thereby reduce drug-related worker injuries. The purpose of this project was to determine the need and capacity for developing a toolkit for occupational health nurses to promote a new or enhanced DFWP, and to explore if they felt it was beneficial or needed for their employee population.
Substance Abuse and Mental Health Services Administration’s Recommendations for the Development of a Toolkit to Promote a Drug-Free Workplace
Conceptual Framework
The strategic prevention framework (SPF; SAMHSA, 2019) served as the framework for this project. SPF was selected because of its utility for prevention in substance use and related programming. SPF includes five steps to guide prevention professionals whose focus is substance misuse and associated behaviors which include assessment, capacity, planning, implementation, and evaluation.
SAMHSA (2019) recommends in the assessment phase that prevention planners define the problem and use data to identify and rank the prevention needs of the local population. Prevention planners collect and analyze national and local substance use and behavioral health data and their effects on the community. The data can include problems with substance misuse and associated behaviors, risk factors and protective elements related to problems of highest priority, and prevention capacity that includes identifying needed human and material resources and the community’s readiness for prevention. In addition, during the assessment phase, organizations focus on assessing the extent, development, severity, and variability of local substance misuse problems and associated risky behaviors. Planners also seek to confirm the appropriateness of efforts aimed at substance misuse prevention in the community.
SAMHSA (2019) recommends in the building capacity phase that organizations develop and implement a drug misuse prevention strategy. They also suggested prevention professionals consider currently available resources and raise the awareness of stakeholders, engage the diverse population of stakeholders, improve efforts to achieve effective collaboration, and equip the prevention workforce. The planning phase includes selecting which risks are the most threatening to employee safety and health, and which protective measures in the DFWP most significantly protect workers from injury or illness and making them priorities in the planning. Endeavoring to collaborate with stakeholders in this phase of the process of selecting interventions also contributes to the sustainability of the interventions. In the implementation phase, prevention professionals should proceed with caution if the original DFWP design must be adapted. Based on their guidelines, SAMHSA (2019) suggests that the core components of the evidence-based program or intervention be retained as much as possible and, before modifying the program, opportunities to build capacity be explored so as to facilitate implementation without sacrificing core elements of the program. If changes are unavoidable, they recommend adding rather than deleting elements from the program plan. Cultural factors also must be considered and if diversity of cultures necessitate a change to the program, the prevention professionals are encouraged to consult experts prior to adapting the program or intervention. The final step is the evaluation process in which prevention practitioners assess the level of success achieved in strategy selection and implementation, while considering the risks and preventive components identified. This evaluation can include collecting and analyzing data about program activities, characteristics, and outcomes to determine program effectiveness. In addition, evaluators need to examine the involvement of representatives from the various partners in the community and identify and add new collaborators. Finally, those evaluating outcomes need to assess the quality of the data upon which decisions or recommendations will be made. To assess the utility of a toolkit, the authors partnered with an occupational health service to identify the need for a new or enhanced DFWP and their capacity for toolkit implementation.
Project Methods
This project evaluated the need and capacity for a new or enhanced DFWP as preparation for a DFWP toolkit. The evaluation took place in the occupational health services clinic of a large Midwestern U.S. acute care health system. Participants in this project were the occupational health nurses, employee assistance counselors, and business manager for the occupational health services department. The findings for this project followed the Strategic Planning Framework, focusing on the Assessment, Building Capacity, and Planning phases, while the Implementation and Evaluation phases of the framework were not operationalized, but recommendations for future implementation and evaluation were outlined. We chose the project site because the organization’s management team was supportive of the project, the staff members were enthusiastic about participating, and the employee health and wellness program, as well as the EAP clinic personnel at this site were accustomed to exploring new ideas and innovations for quality improvement.
Findings
Assessment—Clinic and EAP Staff Surveys
The employee health clinic team at the site included nurses, nurse practitioners, and a business manager, as well as EAP counselors in offices adjacent to the clinic. In discussions with a member of leadership, it became apparent that to consider the development of a toolkit to help occupational health nurses champion an enhancement to the existing DFWP, it was first necessary to assess the capacity for a DFWP toolkit. The existing DFWP was a policy primarily describing the workplace drugs and alcohol policy and employer expectations. The project team, in collaboration with a clinic representative, decided that the most effective way to explore capacity was to survey occupational health professionals, including nurses, nurse practitioners, and the business manager of the project site, as well as EAP counselors. Permission was sought and obtained from the department director to conduct the survey. Due to the differences in the services provided between the clinic and EAP staff, the survey for the occupational health nurses included questions regarding drugs and alcohol assessment, and the survey for EAP representatives ascertained more information regarding referrals made for additional evaluation and treatment.
We developed survey questions based on what we perceived might be potential barriers to promoting a new or enhanced DFWP in these settings (Table 1). The survey questions for the clinic nurses focused on assessment for workplace drugs and alcohol misuse. The questions also explored the nurses’ knowledge and comfort level with the current DFWP, and the frequency with which they believed the need to assess employees for drugs and alcohol misuse. The survey questions for the EAP staff focused on the origin of referrals to EAP, the frequency of drugs and alcohol counseling, and the adequacy of current DFWP training. Because the facility did not track suspected drugs and alcohol cases, the survey participants’ perceptions of frequency of workplace drugs and alcohol issues were the only data available.
Following the SPF guidelines (SAMHSA, 2019), factors that we considered in the assessment included discovering what and how often substance misuse problems occurred in the population of interest and how frequently they occurred. Additional factors that we considered were determining in which areas of the organization the problems were occurring and the specific segments of the population in which they were typically occurring.
Several steps were used to administer the clinic and EAP surveys. First, a confidential online survey was sent via email to nine occupational health clinic workers and five EAP staff; however, respondents identity was not linked to individual responses to allow for anonymity in the analysis. Second, reminder emails were sent to those who did not respond to the survey 1 and 2 weeks later. Third, paper versions of the survey were distributed to those who had not participated online 3 weeks later.
Of those surveyed, nine occupational health clinic workers and two EAP workers responded. Survey results demonstrated low level of confidence in assessing medical symptoms mimicking intoxication or altered mental status (Table 2). The results also revealed a high likelihood that clinic survey respondents would refer employees to the EAP if they needed assistance with drugs and alcohol misuse issues or dependence. The clinic survey respondents (n = 9) had a positive perception of the need for a preemployment assessment tool for drugs and alcohol issues and a toolkit to help occupational health professionals champion an enhancement to an existing DFWP. The majority infrequently saw employees in the clinic who they suspected of drug or alcohol misuse. Although perceived support from administration for a DFWP program was strong, most survey participants believed the training for staff and leadership regarding the existing DFWP appeared to be insufficient. The EAP staff survey respondents (n = 2) believed the DFWP training they had received for themselves was adequate and the development or enhancement to the current DFWP was important. The survey findings confirmed the need for a DFWP toolkit. It was concluded that a toolkit could improve the effectiveness of the current DFWP by providing education regarding the existing policy and drugs and alcohol screening training for occupational health nurses.
Feasibility of a Toolkit for Occupational Health Nurses to Promote a DFWP Survey Results
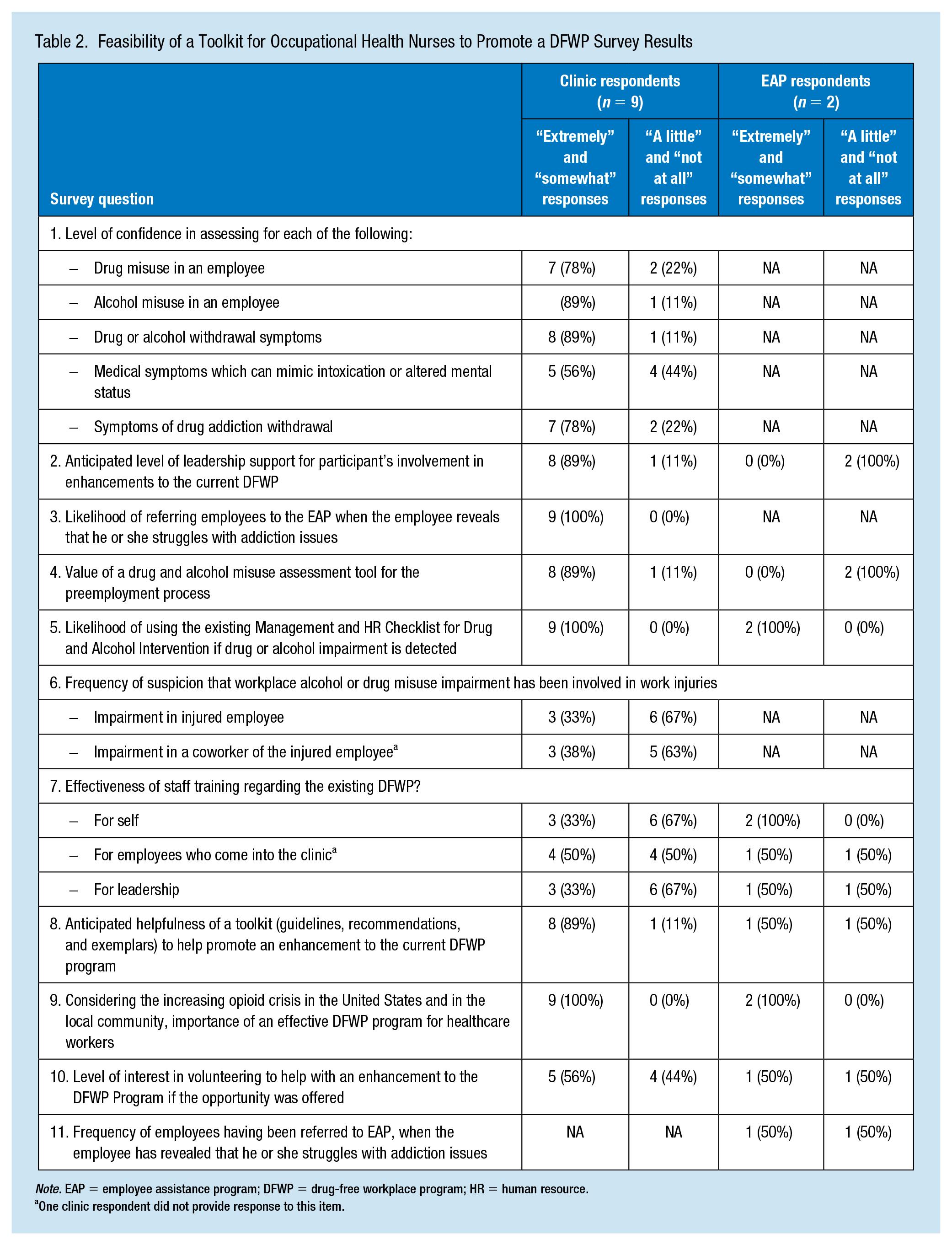
Note. EAP = employee assistance program; DFWP = drug-free workplace program; HR = human resource.
One clinic respondent did not provide response to this item.
Policy Assessment
In 1986, President Ronald Reagan signed the executive order to establish drug-free federal workplaces (Reagan, 1986). SAMHSA (1990) recommends the Federal Employee DFWP as a model plan for private sector employers for a comprehensive DFWP; therefore, we compared the clinic’s current DFWP to the federal employee DFWP (see Table 3). Four gaps were noted for the clinic policy including: (a) screening for law enforcement and first responders, (b) verification of positive results, (c) right for an organization to change the policy, and (d) designated medical review officer to be responsible for receiving and interpreting results. A toolkit designed to educate occupational health nurses and EAP counselors regarding client assessment for potential drug misuse could increase the overall DFWP outcomes.
Comparison of Current Alcohol and Drug Policy to Policy Guidelines in Model Plan for Drug-Free Workplace Program
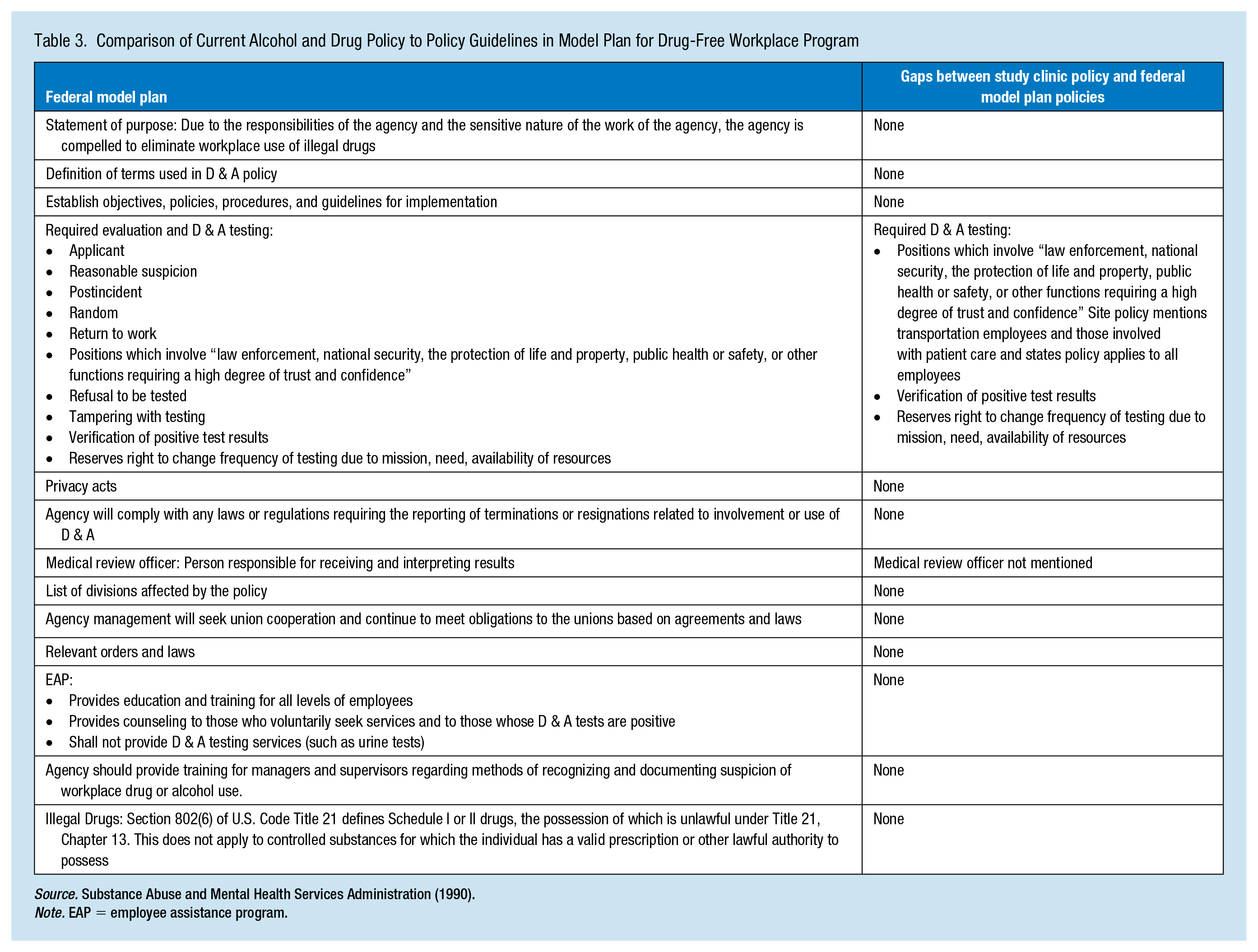
Note. EAP = employee assistance program.
Building Capacity
Key stakeholders were the staff of the clinic and EAP services as well as the department director. The director of the employee health services gave permission for this project to take place indicating his awareness in the importance of evaluating the need and capacity for a DFWP. In addition, the organization had a high capacity to implement enhancements to their DFWP. The anticipated capacity to implement the recommendations was based on (a) respondent survey results indicating strong administrative support for DFWP; (b) respondents were mostly favorable to the introduction of a toolkit to equip occupational health professionals to promote the DFWP program enhancements; and (c) a formal process to change the employer’s drug and alcohol policy being identified. The survey participants also indicated that they were likely to refer general employees to the EAP if drugs and alcohol misuse was suspected. They communicated their support for enhanced training and education regarding the current DFWP policy. It also was deemed that this training, particularly that of recognizing medical symptoms that could mimic intoxication or altered mental status, could be provided to the employee health clinic staff by EAP counselors who were located in close physical proximity to the clinic staff.
Planning Phase
The proposed intervention for this project was a series of recommendations for enhancements to the current DFWP. To accomplish this phase, we met with a member of the clinic staff to discuss strategies to enhance their DFWP, which related to the gaps identified in their policy. For example, there was not a process to validate positive test results. According to Wong (2017), while employers are reevaluating their drug policies and testing procedures, they should be aware of the potential legal implications. A recommendation for the health system based on our assessment was, upon positive test notification, there needs to be a process for retesting the employee specimen. The employer also can modify drug testing to test legal prescription meds. To avoid a violation of the Americans with Disabilities Act, the employer must permit the opportunity for the applicant or employee to explain a positive drug test, such as a prescribed medication (Wong, 2017). Furthermore, to avoid any kind of disability discrimination claim, employers must realize there may be an underlying medical condition necessitating the use of prescription medication (Wong, 2017).
Future Implementation and Evaluation
For the anticipated future implementation, the toolkit can be executed with fidelity to SAMHSA (1990) guidelines but with adaptations to consider unique characteristics of the population and setting. For example, recommendations would be provided with a list of benefits of program enhancement to empower occupational health nurses to promote DFWP enhancements to leadership. The AAOHN (2018) opioid crisis position statement would be included to equip occupational health nurses to defend their support of DFWP enhancements. Sensitivity to cultural diversity would be emphasized during the implementation phase as drugs and alcohol education and training regarding screening tools are presented to the clinic staff. This sensitivity can be addressed by recognizing cultural differences in herbal medications, use of controlled substances for pain management, learning styles, and so on.
Recommendations for an evaluation of the effectiveness of the occupational health nurse toolkit for a DFWP can include obtaining stakeholder input from clinic and EAP staff, hospital administration, and general employers. In addition, a follow up clinic staff survey can compare current and future familiarity with the site’s existing DFWP and their level of comfort with drugs and alcohol screening. A second evaluation strategy could include assessing improvement of the effectiveness of drugs and alcohol education for employees and leadership by using a pretest and posttest following the enhanced drugs and alcohol education. The anticipated short-term outcome, immediately following the initial implementation of the drugs and alcohol education, would be a 50% improvement in pretest to posttest scores. The anticipated long-term outcomes of both educational presentations when repeated in 6 months would be a 75% improvement in posttest scores compared with pretest scores. These scores can be further validated by changes in clinic and EAP practice for management of employees in general with suspected drug use/misuse and perceptions of employees in general using their service.
Discussion
The purpose of this project was to determine the need and capacity for a new or enhanced DFWP in a large health system that would ultimately lead to the design of a toolkit for the occupational health clinic to use. We observed that occupational health clinic workers respondents to the surveys supported the need and capacity for an enhanced program and toolkit that would help them champion a DFWP. The survey findings indicated that most of the clinic staff believed a toolkit would help to promote DFWP enhancements, and all clinic and EAP respondents considered an effective DFWP to be important. We also observed that the resources were in place and the need and capacity for a toolkit for occupational health nurses and other occupational health professionals was supported by this project.
A recommendation based on the results of this project was to explore whether a particular department or area of health care services might be more at risk for developing drug misuse among employees than other departments within the health care system. For example, in the acute care setting, health care providers have access to Schedule I and II drugs. According to Baldisseri (2007), health care professionals in specialty areas including anesthesia, emergency care, and psychiatric medicine tend to have higher rates of drug misuse, most likely attributable to the high-risk environments, the baseline personalities of health care clinicians in these specialty areas, and ease of access to controlled drugs in these environments. Interventions such as education can be targeted to workers in these settings.
To avoid legal complications, SAMHSA (2015) suggests that employers create clear penalties for workplace drug and alcohol policy violations and put in writing the drug-free workplace policy and employee expectations. In addition, SAMHSA (2015) recommends being consistent with all employees, protecting employee privacy regarding suspected policy violations, training of supervisors in detecting drug and alcohol use, avoiding hasty judgment, involving employees in policy development, and documentation of employee performance. This recommendation could be incorporated into a toolkit.
A toolkit would provide training for use of CAGE-AID, an SAMHSA-recommended drug and alcohol misuse screening tool (SAMHSA, 2018a). CAGE-AID is advantageous, because it is brief and can be easily incorporated into a general assessment (SAMHSA, 2018a). The CAGE-AID questionnaire includes four simple questions which focus on whether the individual has ever felt they should cut down (“C”) on alcohol or drug use and whether he or she had ever felt annoyed (“A”) by the criticism of others regarding his or her drug or alcohol use. The CAGE-AID tool also asks the individual if he or she has ever felt guilty (“G”) about personal level of drug or alcohol use or has ever felt the need for drug or alcohol use as a first morning activity (“Eye-opener”) to soothe nerves or relieve a hangover (Basu et al., 2016).
In addition to the CAGE-AID, ASSERT (Alcohol and Substance Abuse Services, Education, and Referral to Treatment) is an evidence-based assessment, brief intervention, and treatment referral model which can be completed in approximately 15 minutes in health clinics or emergency departments (D’Onofrio & Degutis, 2010). ASSERT is a component of the SBIRT treatment model. SBIRT (Screening, Brief Intervention, and Referral to Treatment) is an evidence-supported practice applied to identify, decrease, and prevent misuse and dependence on alcohol and use of and addiction to illicit drugs (SAMHSA, 2018b). The SBIRT model was inspired by an Institute of Medicine recommendation, which encouraged community-based screening for health risk behaviors, including alcohol misuse and use of illegal drugs. Using a standardized screening tool, such as CAGE-AID, a health care provider in any health care setting assesses a client for potentially problematic substance use behaviors. The brief intervention is a short discussion during which the health care professional provides feedback and guidance for the client displaying risky behaviors related to substance use. In cases where the screening results indicate a need for additional services, the health care professional provides a referral to treatment, the last phase of the SBIRT (SAMHSA, 2018b) and ASSERT (D’Onofrio & Degutis, 2010) models.
Application to Practice
Considering the current U.S. opioid crisis, prevention efforts must be implemented in the occupational health setting. A DFWP can effectively reduce drug use among workers and thereby reduce drug-related worker injuries. A “kit” is one approach for the workplace and this study determined there is a need and capacity for an enhanced DFWP program which can be accomplished through a toolkit for occupational health nurses. Optimally, the toolkit will address the potential barriers occupational health nurses need to overcome to effectively promote the new or existing DFWP. In addition, the proposed toolkit would provide drugs and alcohol education and drugs and alcohol screening education for clinic staff members and other occupational health professionals in a health care environment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Dr. Gillespie’s time for this study was partially supported by the National Institute for Occupational Safety and Health through the University of Cincinnati Education and Research Center grant #T42-OH008432. Its contents are solely the responsibility of the authors and do no necessarily represent the official view of the CDC-NIOSH.
Author Biographies
Cynthia A. Betcher’s is an assistant professor of Nursing and background includes serving as a hospital staff nurse, nurse case manager for injured workers, claims auditing manager, school nurse, and occupational health nurse. As an instructor at the University of Cincinnati, Dr. Betcher has taught community health nursing and occupational health nursing.
Michele D. Standish graduated in 1984 from Deaconess Hospital School of Nursing and practiced in a variety of settings for 5 years before embarking on a 12-year career in travel nursing. In 2012, Ms. Standish completed a master’s in nursing science with an emphasis on Acute Care Clinical Nurse Specialist with the University of Cincinnati and practices as an RN at University of Cincinnati Employee Health & Wellness.
Gordon Lee Gillespie is professor and deputy director of the Graduate Occupational Health Nursing Program at the University of Cincinnati. His research has been funded by the Centers for Disease Control and Prevention (CDC)-National Institute for Occupational Safety and Health, Robert Wood Johnson Foundation, American Nurses Foundation, and Emergency Nurses Association Foundation. His work has been cited by the Occupational Safety and Health Administration, U.S. Government Accountability Office, American Nurses Association, and practitioners and researchers across six continents. He also is a national director of the Emergency Nurses Association.