
Abstract
Background: In Costa Rica, the leading cause of preventable death is smoking. Adults spend one third of their lives at work making the workplace an optimal site for smoking cessation interventions. Therefore, we developed a workplace smoking cessation pilot program among Costa Rican Justice Department government employees based on key Costa Rican values and best practices. Methods: First, focus groups were conducted among exsmokers and smokers. Participants in the focus groups and in the subsequent smoking cessation pilot study were invited to take part in the study through flyers, information sheets, and announcements from the Justice Department. The focus groups revealed that social factors were fundamental to quitting. Therefore, based on these results two programs (14 participants) were conducted consisting of seven sessions encouraging employees to utilize their family and exsmokers. Data were collected before and after the seven sessions on smoking behavior, social influence, and other factors. Findings: Five of 14 (36%) quit smoking. None of the quitters lived with a smoker, as compared with 56% of nonquitters who lived with a smoker. Also, quitters were less likely to have friends (40% vs. 67%) and coworkers (20% vs. 33%) who smoked compared with nonquitters. Conclusion/Application to Practice: Workplace smoking cessation programs should help smokers to increase their social contacts with nonsmokers/exsmokers. Smoking cessation programs should assess not only smoking patterns, but also social contacts, such as family, friends, and coworkers. Based on these assessments, smokers should be encouraged to seek-out nonsmokers/exsmokers to assist them in quitting.
Background
The workplace is an optimal site for smoking cessation interventions for adult smokers (Cahill & Lancaster, 2014; Kilpatrick et al., 2016.) Most adults spend one third of their lives at work. In the workplace health programs can be promoted using emails, newsletters, and bulletin boards; meetings can be arranged to fit workers’ schedules; peer and social support can be utilized in smoking cessation programs; and no-smoking in workplace policies can further quitting (Albertsen et al., 2006; Moher et al., 2005).
In Costa Rica, cardiovascular disease has been the leading cause of death for the past 30 years (Pan American Health Organization [PAHO], 2017). An important factor contributing to this increase has been tobacco consumption (PAHO, 2017). Smoking is a major public health issue in Costa Rica. Approximately 10 smoking-related deaths caused by pulmonary and cardiovascular disease occur every day and the Costa Rican Social Security Association spends about US$110 million every year on smoking-related hospitalizations, care, and disability (Campos, 2010; Monge Bonilla, 2012).
In one of the few studies examining smoking among Costa Rican workers, it was found that 21.4% were smokers with 32.2% of all men and 8.0% of women (Arce et al., 2015). Research aimed at motivation to quit smoking indicated that 41.6% reported moderate motivation and 58.4% reported low motivation to quit smoking (Arce et al., 2015).
Key Costa Rican and Latin American values focus on the role of the family in influencing family members’ behavior (Khaddouma et al 2015; Streit et al., 2017). Among these values is “familismo”—the importance of the nuclear and extended family as referents and providers of emotional support. In addition, another principal value is “simpatia”—promoting smooth and pleasant social relations. This is particularly true in terms of smoking and smoking cessation (Gonzales, 2019; Rodríguez Esquivel et al., 2015).
To address the issue of smoking in Costa Rica, a collaboration was established between the Universidad de Iberoamérica (UNIBE) in San José, Costa Rica and the University of Maryland in the United States to develop and evaluate a workplace smoking cessation pilot program based on best practices in Costa Rica and the United States.
Methods
To better understand smoking in Costa Rica, the first step was to meet with the leading government agency involved with smoking research, and the development and implementation of smoking cessation programs: the Institute on Alcoholism and Drug Dependency (Instituto sobre Alcoholismo y Farmacodependencia [IAFA]). The IAFA shared their work on smoking and smoking cessation and made the recommendation that we work with the Justice Department (Poder Judicial) as this agency expressed interest in starting a smoking cessation program for their employees. Meetings were held with the director of Employee Health Services (a dentist) within the Justice Department who strongly supported the development of a workplace smoking cessation program for her employees.
In developing a Costa Rican workplace smoking cessation pilot program, it was necessary to understand the issues confronting smokers and exsmokers from their point of view. The Justice Department Director obtained approval for 15 employees to be invited to participate in one of two focus groups. Focus groups were conducted by a Costa Rican researcher in Spanish with smokers and exsmokers who were employees of the Justice Department. Institutional Review Board (IRB) approval was obtained from the University of Maryland; however, Costa Rica did not require IRB approval for focus group studies. The results of the focus groups indicated that the key cultural factors for both smokers and exsmokers were social factors—family and coworkers. Participants viewed family support as fundamental to successful quitting. The major barriers to quitting were reported as the presence of other smokers both inside and outside the workplace and workplace stress.
Based on the focus group results and a comprehensive review of the smoking cessation literature in Costa Rica, Latin America, and the United States, a pilot study was designed. The program incorporated best practices from the Centers for Disease Control and Prevention, the American Lung Association, the Truth Initiative, and IAFA and combined them with the results of the Costa Rican Justice Department focus group results to form a program utilizing best practices and Costa Rican viewpoints. The programs were in Spanish led by two Costa Rican health psychologists from UNIBE who were trained by the senior author who has more than 30 years of experience conducting research and leading smoking cessation programs. For the pilot study, the Justice Department Director assisted in obtaining IRB approval from the Justice Department. In addition, she obtained approval for another set of smoking employees to attend the workplace smoking cessation program, recruited participants, and supplied snacks. IRB approval for the pilot study was obtained from the University of Maryland.
The workplace smoking cessation programs consisted of seven sessions conducted at offices in the Justice Department building in downtown San José. Each session lasted 1.5 hours. The program was entitled: Si Se Puede—Costa Rica. Table 1 shows an outline of the major components of the program.
Lesson Plan Smoking Cessation Training
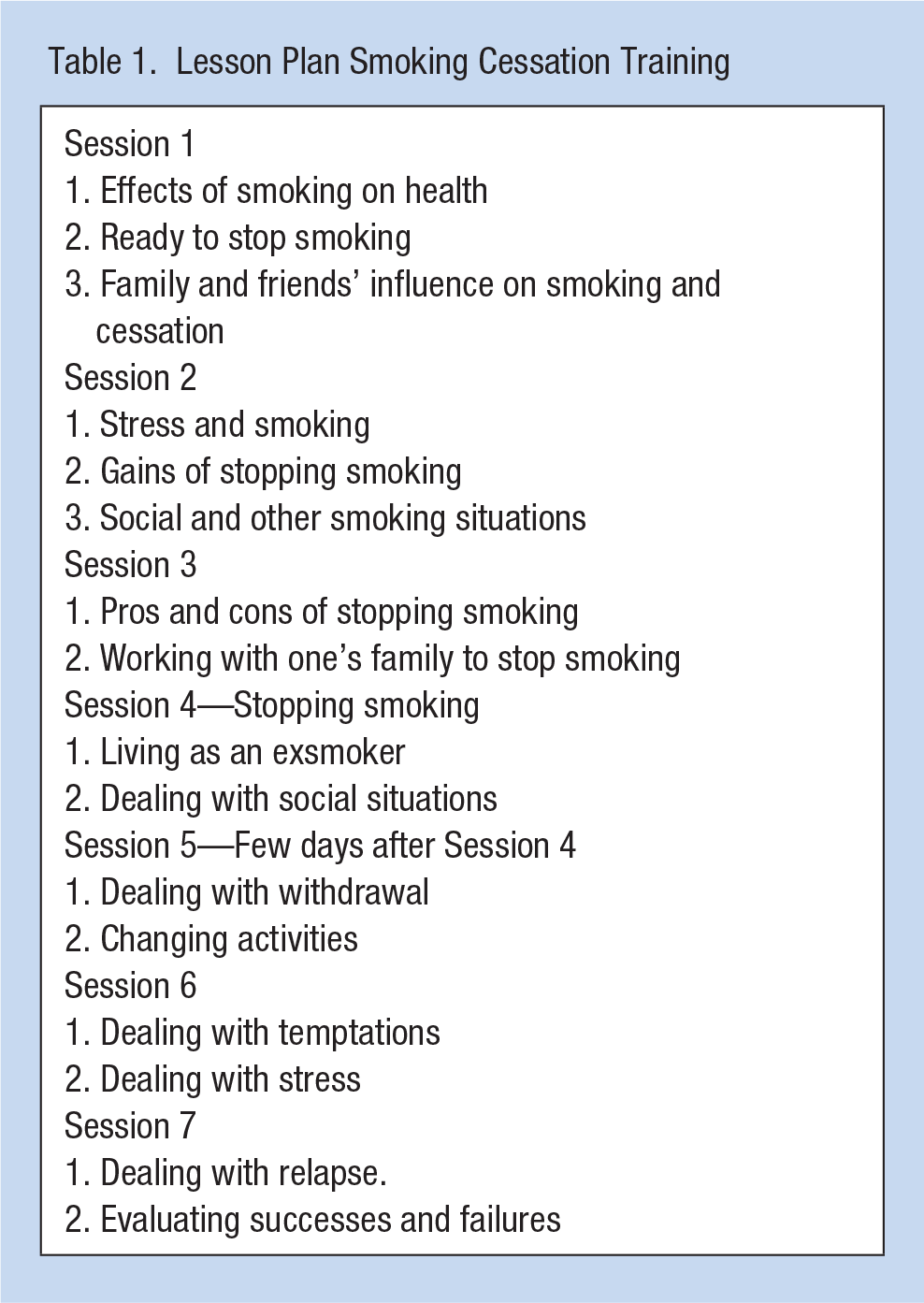
Each session contained a social component to assist quitting, such as, spending more time with one’s family. The programs encouraged the smoking employees to strongly utilize their family and exsmokers in their social environments to assist them in the quitting process. For example, they were urged to discuss with their family and exsmokers their reasons for quitting, how to avoid tempting situations, how to cope with urges, and to seek social support. Participants were challenged to be better role models for their children by quitting smoking. In addition, they were encouraged to request assistance from their family on how to handle social situations, especially those with smokers. Participants were urged to request the help of their family in how to modify their home environments to remove possible triggers.
Seven employees signed up for each program for a total of 14 participants. Attendance was mixed. A total of six attended four to seven sessions and eight attended one to three sessions. Data were collected before and after the seven sessions on smoking behavior, readiness to quit smoking, self-efficacy (confidence in quitting), perceived barriers to quitting, and social influence and social support. Smoking behavior was measured by a number of scales. Examples include: (a). Have you smoked at least 100 cigarettes in your entire life? (b) For approximately how many years have you been smoking regularly? (c) Do you now smoke cigarettes every day, some days, or not at all? (d) On average, about how many cigarettes do you smoke a day? (e) How soon after you wake up do you have your first cigarette? To determine their readiness to change (quit smoking) we used items from the Transtheoretical Model (Prochaska & DiClemente, 1983). For self-efficacy we asked each participant whether “At the end of the program, I am confident that I can keep from smoking when” followed by a 17-item 5-point agree–disagree Likert-type Scale describing different situations where participants may smoke. Perceived barriers were measured by a list of reasons why some people have not been able to stop smoking. Participants were asked on a seven-item 5-point agree–disagree Likert-type Scale whether these reasons are why they have not been able to stop smoking. Social influence was measured by three items: how many of your friends and how many of your coworkers smoke?—both measured by a five-item scale: (1) most or all, (2) about half, (3) less than half, (4) a few, (5) none. The third item asked how many people do you live with? The alternatives were I live by myself, none, one, two, three or more. Descriptive analysis was conducted for all measures ascertained for the study. The sample size was too small to conduct further statistical analysis.
Results
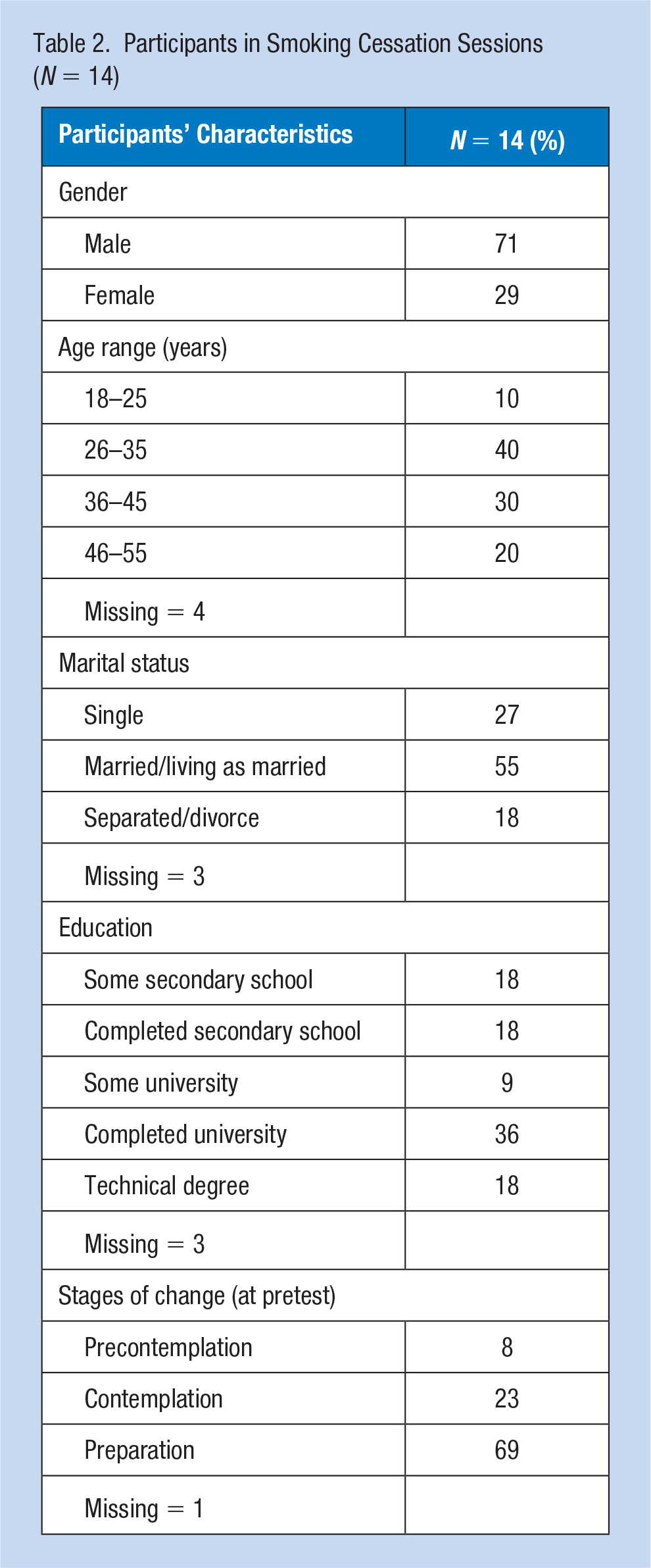
We conducted two separate programs and had seven participants in each program with a total of 14 participants (Table 2). The smokers were 71% male and 29% female. In terms of age, 50% were aged 18 to 35 years and 50% were aged 36 to 55 years. A total of 55% were married or living as married, 27% single, 18% separated or divorced. In total, 36% completed or had some secondary school, 45% completed or had some university education, 18% had a technical degree. Therefore, it was a diverse sample. To determine their readiness to quit smoking the Stages of Change measures indicated that one participant (8%) was in the precontemplation stage, three participants (23%) were in the contemplation stage, nine participants (69%) were in the preparation stage.
Participants in Smoking Cessation Sessions (N = 14)
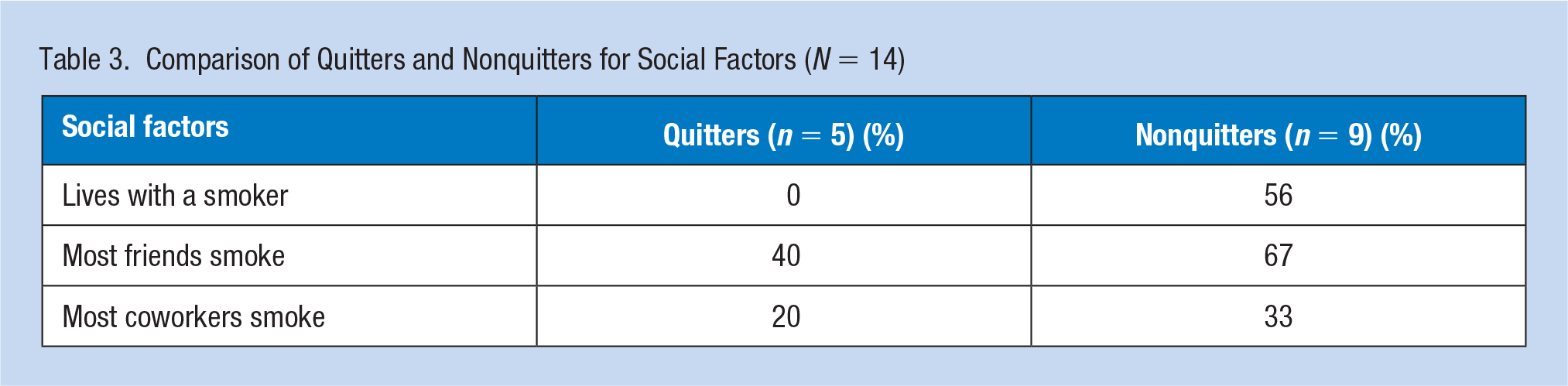
At the end of the program, five of 14 or 36% of the Justice Department smokers quit. We observed that none (0%) of the smokers who quit smoking lived with a smoker as compared with five of the nine of the nonquitters who lived with a smoker (Table 3). Also, 40% of the quitters reported that most of their friends smoked compared with 67% of the nonquitters. In addition, 20% of the quitters mentioned that most of their coworkers smoked compared with 33% of the nonquitters. That is, the employees who quit smoking were less likely to live with a smoker, have friends that smoke, and have coworkers that smoke.
Comparison of Quitters and Nonquitters for Social Factors (N = 14)
Discussion
The results of this study give suggestions for the development of workplace smoking cessation programs in Costa Rica. Both the qualitative focus group data and the quantitative survey data from the smoking cessation programs indicated that social factors were key to successful quitting. Employees who attended a workplace smoking cessation program and successfully quit smoking were more likely not to live with a smoker and less likely to have friends and coworkers who smoke. The earlier focus group study also found social factors to be important and that family support was fundamental to successful quitting. However, the modest results of our study and the important finding of the influence of social factors on quitting demand a stronger approach. For example, in smoking cessation programs, (a) in addition to assessing the smoking behaviors of the participant it would also be helpful to assess the smoking status and behaviors of participant’s family and significant others, (b) if possible, involve family members in the actual smoking cessation program, and (c) provide “homework” assignments to participants that involves interacting with family and significant others.
Smoking literature also indicates that smokers tend to congregate with other smokers and the presence of smoking coworkers is a major barrier to quitting. Also, coworkers who are exsmokers are seen as important change agents and should be included as well in workplace smoking cessation programs (McEwen et al., 2008; van den Brand et al., 2019). Therefore, many smoking cessation programs recommend that smokers trying to quit seek out and socialize more with nonsmokers and exsmokers (Agency for Health care Research and Quality, 2018). In addition, effective workplace smoking restrictive policies would enhance employees in their efforts to stop smoking. Based on the results of this study, we strongly recommend that smokers trying to quit seek out and socialize more with nonsmoking and exsmoking family members, friends, and coworkers.
Implications for Occupational Health Nursing Practice and Occupational Health Practice
Occupational health nurses and other occupational health professionals frequently work in the area of workplace health promotion including workplace-smoking cessation. In addition, they are engaged with diverse populations in the United States and in international settings. When involved with these populations it is important to be cognizant of cultural differences. In working with U.S. Latino and with people from Latin America, occupational heath professionals need to be aware of the centrality of the family and social factors. Therefore, in designing smoking cessation programs they need to carefully gather information about social influences that affect smoking and smoking cessation. Based upon that information they can then strongly encourage workers who are trying to quit smoking to reach out beyond their current social environments to exsmokers and nonsmokers to assist them to stop smoking.
Applying Research to Occupational Health Practice
Adults spend one third of their lives at work. Therefore, the workplace is an excellent site for smoking cessation interventions for adult smokers. To reduce smoking among Costa Rican government workers, a workplace smoking cessation pilot study was developed based on key Costa Rican values and best practices in Costa Rica and the United States. Focus groups among smokers and exsmokers indicated that the influence of the family and coworkers were most important in quitting smoking. Consequently, our smoking cessation program emphasized these social factors. Quitting rates were higher among employees who did not live with a smoker and who had fewer friends and coworkers who smoked. Thus, cessation programs should assess not only the smoking patterns of smokers, but also their social contacts, such as, family, friends, and coworkers. Programs should encourage smokers to reach out beyond their social contacts to nonsmokers and exsmokers to assist them in quitting.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding and support from the Universidad de Iberoamérica, Costa Rica and the University of Maryland.
Author Biographies
Robert H. Feldman is a professor at the University of Maryland. His research interests are in smoking and smoking cessation, cross-cultural research, and occupational health psychology.
Alfonso Villalobos-Pérez is professor at the Universidad de Costa Rica and the Universidad de Iberoamérica, Costa Rica. His research interests are in health psychology, bullying and cognitive-behavioral therapy.
Roberto G. Rodríguez is currently the chancellor at Universidad Fidélitas, in Costa Rica. His research interests are in health education and cross-cultural research.