
Abstract
Background: Most of the previous studies on nursing practice environment and job burnout employed conventional analyses ignoring the impact of unit-level data clusters. This study addressed this gap by examining the effects of the nursing practice environments on dimensions of occupational burnout among a sample of Chinese nurses using multilevel logistic regression models and demonstrating the superiority of employing multilevel models over conventional models within this context. Methods: A proportionate stratified sampling method was applied in this cross-sectional study that invited 1,300 registered nurses (RNs) from nine clinical units of a large, academic hospital in urban China to complete the questionnaire. Nurse-reported information was obtained using the Practice Environment Scale of the Nursing Work Index (PES-NWI) and the Maslach Burnout Inventory (MBI). Findings: A total of 1,178 valid questionnaires were returned for a response rate of 90.62%. RNs generally perceived their nursing practice environment as favorable as measured by the PES-NWI. Approximately 40% of the respondents reported experiencing emotional exhaustion and depersonalization. The multivariate models indicated that nurse burnout was significantly associated with nurse participation in hospital affairs, nursing foundations for quality of care, and adequate staffing. In addition, our results illustrated the advantage of multilevel modeling over the conventional modeling for handling hierarchical data in terms of the accuracy of the estimates and the goodness-of-fit of the model. Conclusions/Application to Practice: These findings underscore the importance of measures aimed at enhancing nursing practice environments to prevent RNs from experiencing feelings of burnout and of considering multilevel analysis in future nursing research.
Keywords
Background
The past two decades have seen exponential growth in occupational health studies, among which job burnout is well documented. Occupational burnout, a prolonged response to excessive job stressors, is conceptualized as a tripartite construct comprised of exhaustion, cynicism, and inefficacy (Maslach et al., 2001). Exhaustion refers to feelings of being emotionally overextended; it reflects the stress aspect of burnout and is the most central component and most frequent manifestation of burnout. Cynicism (i.e., depersonalization), which represents the interpersonal aspect of burnout, describes callous, pessimistic, or detached responses to the job, while inefficacy, which represents the self-evaluation aspect of burnout, includes feelings of incompetence and lack of work productivity and achievement. Burnout happens when chronic mismatches occur between a person and critical areas of his or her professional life (Maslach et al., 2001). Because nurses are inherently engaged with overwhelmingly demanding work, they are especially vulnerable to burnout. As reported by the International Hospital Outcomes Study (IHOS), a high rate of nurse burnout was found in hospitals worldwide, and the incidence was over one third in most investigated countries; in South Korea and Japan, it was decidedly high, at approximately 60% (Aiken et al., 2011). Chinese nurses likewise confront burnout; approximately one in three of them are plagued by this negative mental state, and this rate is steadily increasing (Zhang et al., 2014). High degrees of burnout can compromise the physical soundness and career prospects of individual workers, thus triggering nurse absenteeism and turnover (Daouk-Öyry et al., 2014; Fragoso et al., 2016), and also compromise quality of care and even jeopardize patient safety (Prapanjaroensin et al., 2017).
Much effort has been invested in exploring the antecedents to nurse burnout. The latest consensus indicates that central to the feelings of job burnout among nurses is the immediate work environment (Aiken et al., 2011; Liu et al., 2012). An unfavorable practice environment is responsible for the high rates of nurse burnout and a consistent focus for mitigating the adverse effects of burnout (Aiken et al., 2012; Zhang et al., 2014; Zhou et al., 2015). A large-scale nurse workforce study (RN4CAST project) conducted in 12 European countries involving 33,731 employees highlighted the correlation between nursing practice environment and burnout and found that specific interventions to achieve excellent work environments should be considered to secure better outcomes for nurses, as well as for patients (Casalicchio et al., 2017). A multisite study in China also demonstrated that nurses in hospitals with poor practice environments had higher odds of complaining about burnout and were twice as likely to report job dissatisfaction and an intention to leave (Zhang et al., 2014). Nursing practice environments refer to the modifiable organizational features of a work setting that could facilitate or obstruct professional performance (Lake, 2002). Decentralization of decision making, autonomy over nursing practice, appropriate leadership and support, adequate staffing and resources, and collaborative nurse–physician relations are empirically thought of as the five essential elements of a positive practice environment (Twigg & McCullough, 2014).
Previous studies concerning practice environment and nurse burnout, although abundant, predominantly focused on hospital-level conditions, rather than on the potential variability of burnout across nursing units, and only a few studies have considered the data hierarchy of clustered observations (Leineweber et al., 2014). In addition, it is worth noting that a majority of burnout studies only focused on the emotional exhaustion dimension of the syndrome (Li et al., 2013), although the significance of the three-dimensional model has been underscored because it “clearly places the individual strain experience within the social context of the workplace and involves the person’s conception of both self and others” (Maslach & Leiter, 2008). Only measuring exhaustion would fail to capture the whole picture of nurses’ burnout syndrome. Therefore, we took all three burnout dimensions into account in this article.
Data with a hierarchical structure occur frequently in scientific studies about populations, public health, and health care services (Austin & Merlo, 2017). Examples include workers clustered within workplaces and repeated measurements of the same subject. Under such circumstances, workers and repeated measurements are at Level 1, and workplaces and subjects are at Level 2. Responses obtained from individuals within the same cluster usually bear some similarity due to the influence of a common context (Austin & Merlo, 2017); statistical dependencies can thus occur. However, traditional statistical techniques are based on the assumption of independence (Cohen et al., 2014). Application of a conventional regression model when processing clustered data could lead to neglect of the clustering present in hierarchical data (Hox et al., 2017). In contrast, multilevel modeling (MLM), an advanced statistical technique, possesses attractive features for discerning the hierarchical structure of data and quantifying the total variance explained by different levels of the data, making it preferable for handling such data (Cohen et al., 2014). However, a limited number of nursing studies have attempted to account for statistical dependency or have taken advantage of MLM, although MLM was introduced into nursing research more than 20 years ago (Wu, 1995). In our study, given that participants were grouped by units with distinct organizational characteristics, we speculated that nurses working in a particular patient unit would have more in common with each other than with their counterparts from other units in terms of their perceptions about their workplaces, and their feelings about their jobs due to their shared physical and psychosocial work environments.
The aim of this study was to investigate the impact of the unit-level nursing practice environment on dimensions of occupational burnout among a sample of Chinese nurses and to demonstrate that multilevel logistic regression models generate better estimates than conventional logistic regression models using the same sample data.
Method
Setting and Sample
This cross-sectional study targeted clinical nurses employed in a large, academic, urban medical center in China, which has a 4,300-bed capacity. The eligible nurses met the following criteria: (a) full-time registered nurse (RNs), (b) worked in their present unit for at least 6 months, and (c) engaged in direct patient care. Nurses with administrative positions or on leave during the survey period were excluded. We collected the lists of all eligible nurses after the official permission was granted by the nursing department. To maximize the sample representativeness, a proportionate stratified sampling method was implemented to recruit participants. Each of the nine adult inpatient units in the hospital was regarded as a stratum, and in each stratum, computer-generated random digits were used to select nurses to participate. Specifically, 50% of the staff nurses in each stratum, namely, a total of 1,300 nurses, were randomly selected and invited to participate. The data had a two-level structure with nurses (Level 1) clustered within their respective unit (Level 2).
Prior to commencing our study, ethical approval (IRB no. 2015-48) was obtained from the Institutional Review Board for Clinical Trials and Biomedical Research in West China Hospital, Sichuan University. All participants voluntarily signed the written informed consent and were promised that their privacy would be maintained and they had the right to withdraw from the study at any time without any consequences. Permission to use the specific instruments in this study was obtained from the copyright holders by email.
Data Collection
The investigation was conducted from April to September 2016. Structured questionnaire packages, including a recruiting notice, an informed consent form, and an anonymous questionnaire, were distributed by the research assistants to the individual participating nurse. Before potential participants were asked to sign the informed consent form, the study objectives and detailed instructions had been reiterated. Every participant was expected to take his or her own time to complete the questionnaire and to return it to the designated mailbox in a sealed envelope within 1 week. Research assistants were responsible for retrieving the questionnaires.
Measures
The data collection instrument consisted of three parts, which include the following: (a) nurse-level information about the nurses’ sociodemographic characteristics, including gender, age, marital status, number of minor children (≤18), years of nursing experience, highest educational level, and current work unit; (b) the nursing practice environment, which was aggregated to the nursing unit level; and (c) the outcome variables including three dimensions of nurse burnout.
Nursing practice environment
The Practice Environment Scale of the Nursing Work Index (PES-NWI) is a parsimonious, psychometrically sound instrument for discerning the contribution of modifiable organizational features of a work setting to nurse job outcomes, as well as patient care outcomes (Lake, 2002). The validated Chinese version (You et al., 2012) was applied in the present study. The following five subdomains constitute this self-administered questionnaire: (a) nurse participation in hospital affairs (nine items); (b) nursing foundations for quality of care (10 items); (c) nurse manager ability, leadership, and support of nurses (five items); (d) staffing and resource adequacy (four items); and (e) collegial nurse–physician relations (three items)—totaling 31 items rated on a 4-point Likert-type style (1 = strongly disagree, 4 = strongly agree). Each subscale score is derived by averaging the item values, with higher scores indicating a better practice environment (Lake, 2002). Relevant studies adopting the PES-NWI mostly endorsed the composite score (Warshawsky & Havens, 2011). Instead, we chose to take advantage of each subscale, with the intention of identifying the impact of each subdimension on the components of burnout to provide more actionable targets for enhancing nursing practice environments. This instrument has demonstrated adequate reliability and validity in the Chinese context. In our study, the overall Cronbach’s α was .96, and the subscale coefficients ranged from .78 to .90.
Occupational burnout
The Maslach Burnout Inventory (MBI) is widely accepted as the leading measurement of burnout in human services and health care fields (Maslach et al., 1996). The Chinese version was validated by You et al. (2012) and was used here to operationalize the three dimensions of occupational burnout: emotional exhaustion (EE, nine items), depersonalization (DP, five items), and personal accomplishment (PA, eight items). The standardized questionnaire is composed of 22 items and answered with a 7-point, fully anchored scale (0 = never, 6 = every day). Subtotals of each dimension are computed separately by summing the corresponding items. For the EE and DP dimensions, higher scores indicate more severe burnout, while the PA dimension does the opposite. Scores of ≥27 on EE, ≥10 on DP, or ≤33 on PA were indicative of high burnout for the associated dimension (Maslach et al., 1996). In the study, the overall Cronbach’s α was .86, and the subscales also yielded acceptable estimates of internal consistency, with a Cronbach’s α of .79–.87.
Data Analysis
Descriptive statistics (means and standard deviations for continuous variables; sample sizes and frequencies for categorical variables) were used to delineate nurse characteristics, practice environment, and occupational burnout. Analysis of variance (ANOVA) and Scheffe’s post hoc test were used to compare the nursing practice environment across different clinical units. Student’s t-test or ANOVA was performed to identify the potential confounders among sociodemographic variables, with a p-value of less than .05 being considered statistically significant; those identified were controlled for in subsequent multivariate analyses. Conventional and multilevel logistic regression models were used to separately examine the associations between the practice environment and each dimension of nurse burnout, and then the statistical estimates of the two models were compared with each other. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated from the fitted models.
To verify the suitability of conducting MLM, the data were initially fitted to a null model without any explanatory variables, which were not intended to explain any variance in nurse burnout but rather to divide the variance into two independent components: variance at the unit level
Results
Participant Characteristics
Of the 1,300 RNs, 93.8% (n = 1,219) responded to the survey and a total of 1,178 returned questionnaires that were considered valid, giving an overall effective response rate of 90.6%. Our sample was highly skewed with respect to gender, with females accounting for 96.0% of the RNs (Table 1). On average, the respondents were 29.63 years old and had 8.76 years of work experience as an RN. More than half of the RNs were unmarried and had no minor child. Approximately 64% of the RNs had a baccalaureate degree or higher, and the majority of the RNs were from surgical units (25.0%), medical units (23.9%), or integrated units (10.4%).
Demographic Characteristics and Burnout Domains of Nurses (N = 1,178)
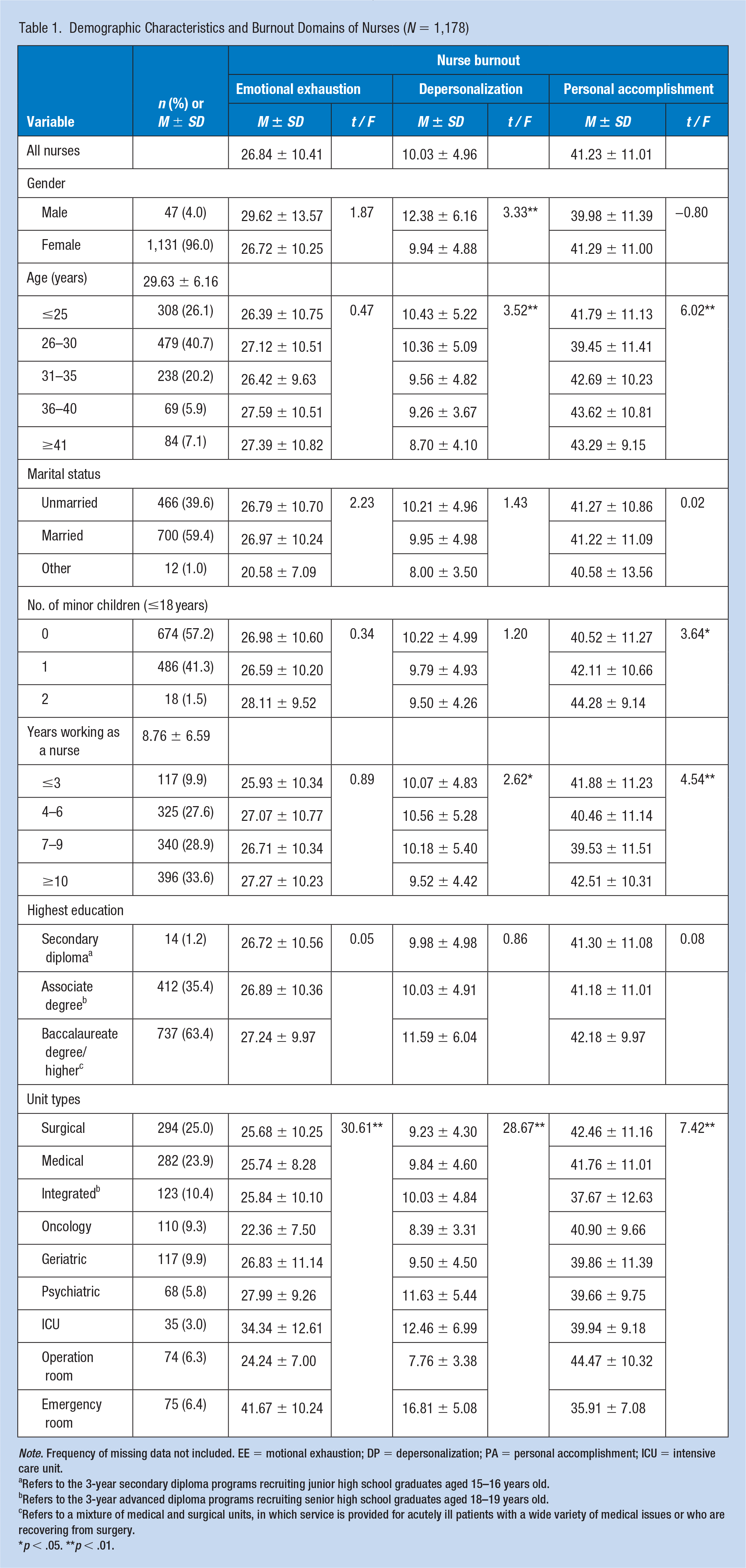
Note. Frequency of missing data not included. EE = motional exhaustion; DP = depersonalization; PA = personal accomplishment; ICU = intensive care unit.
Refers to the 3-year secondary diploma programs recruiting junior high school graduates aged 15–16 years old.
Refers to the 3-year advanced diploma programs recruiting senior high school graduates aged 18–19 years old.
Refers to a mixture of medical and surgical units, in which service is provided for acutely ill patients with a wide variety of medical issues or who are recovering from surgery.
p < .05. **p < .01.
Nurse Burnout and Practice Environment
Regarding the interpretation of the nurse burnout data, the continuous outcome variables were dichotomized as high burnout in any MBI subscale versus not. The EE scores averaged at 26.84, and 42.5% (not shown) of the RNs reported high levels of emotional exhaustion. Significant differences in EE scores were seen across different units (F = 30.61, p < .01). The mean DP score was 10.03, and 41.5% (not shown) of RNs felt highly depersonalized. The variance of the DP scores reached statistical significance according to participants’ gender (F = 3.33, p < .01), age groups (F = 3.52, p < .01), work experience (F = 2.62, p < .05), and unit types (F = 28.67, p < .01). With regard to the PA dimension, the mean score was 41.23, and 21.8% (not shown) of the RNs suffered feelings of highly diminished personal accomplishment; significant differences in PA scores existed among RNs from various age groups (F = 6.02, p < .01), those with different numbers of minor children (F = 3.64, p < .05) and work experience (F = 4.54, p < .01), and those engaged in separate units (F = 7.42, p < .01). These results identified significant sociodemographic factors in RNs’ burnout dimensions.
The nurses’ perceived practice environments are displayed in Table 2. The mean scores for the subscales of the PES-NWI varied marginally, and all ranged between 3 and 4. Significant differences were identified among RNs from different work units (F = 36.01, p < .01). Pairwise between-unit comparisons of the PES-NWI score further revealed that RNs working in the emergency room and the psychiatric unit rated their practice environments significantly lower than did others, with mean values of 3.00 and 3.22, respectively.
The Practice Environment Scale (PES-NWI) Among Nurse Participants and Work Units (N = 1,178)
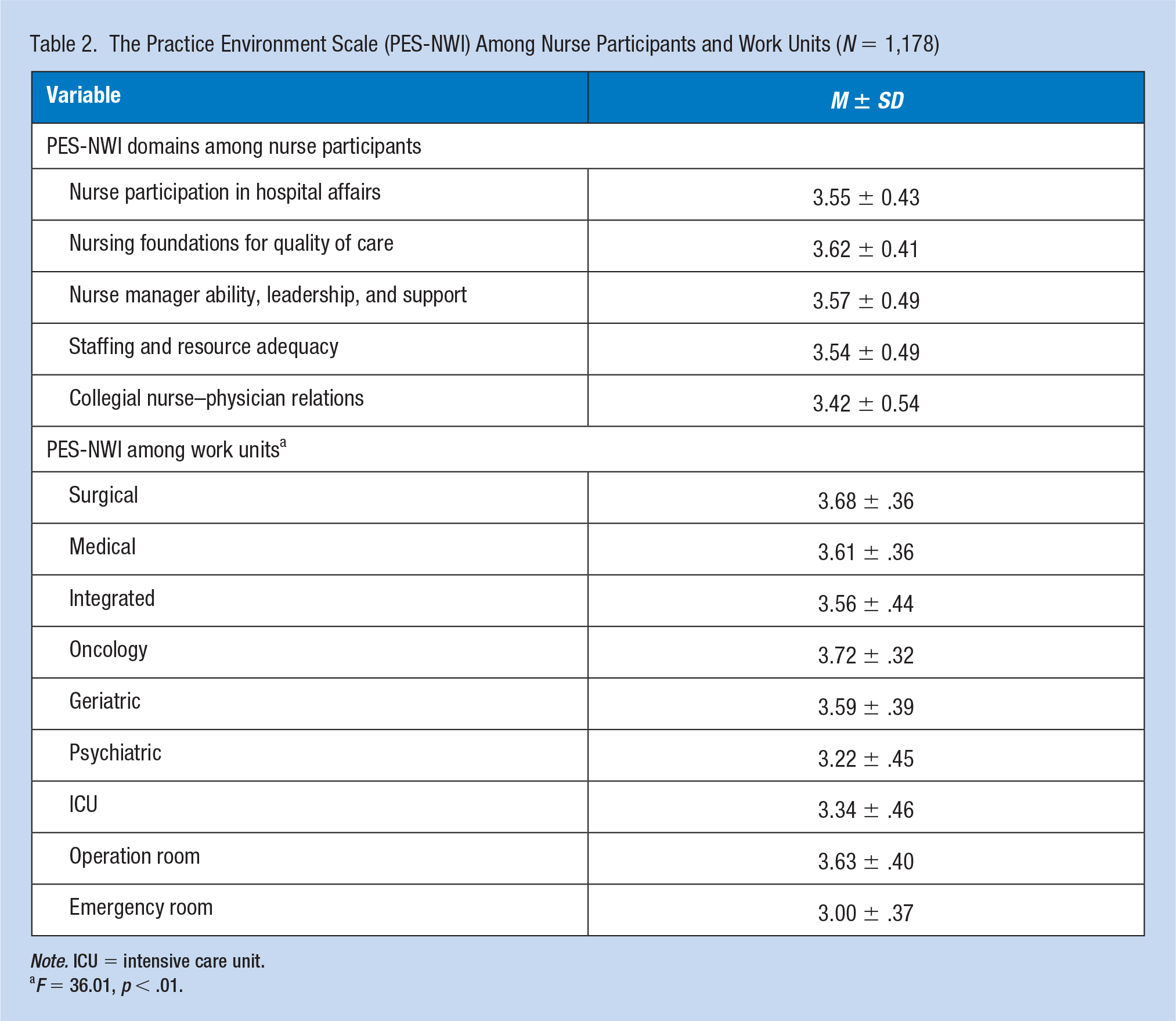
Note. ICU = intensive care unit.
F = 36.01, p < .01.
Impact of the Practice Environment on Nurse Burnout
Table 3 presents the results of the logistic regression models. The findings from the conventional models indicated that emotional exhaustion was negatively related to nurse participation in hospital affairs (OR = 0.48, 95% CI = [0.31, 0.76]), nursing foundations for quality of care (OR = 0.45, 95% CI = [0.24, 0.84]), and staffing and resource adequacy (OR = 0.43, 95% CI = [0.31, 0.61]). The possibility of perceiving depersonalization was lower in RNs who reported higher levels of nursing foundations for quality of care (OR = 0.13, 95% CI = [0.07, 0.25]) and staffing and resource adequacy (OR = 0.57, 95% CI = [0.40, 0.80]) than other RNs. In addition, in models controlled for individual participant characteristics, personal accomplishment was found to be significantly associated with nursing foundations for quality of care (OR = 0.28, 95% CI = [0.15, 0.55]) and staffing and resource adequacy (OR = 1.76, 95% CI = [1.18, 2.64]).
Logistic Regression Models Examining the Nurse Work Environment and Burnout Domains: A Comparison of Conventional Versus Multilevel Models (N = 1,178)
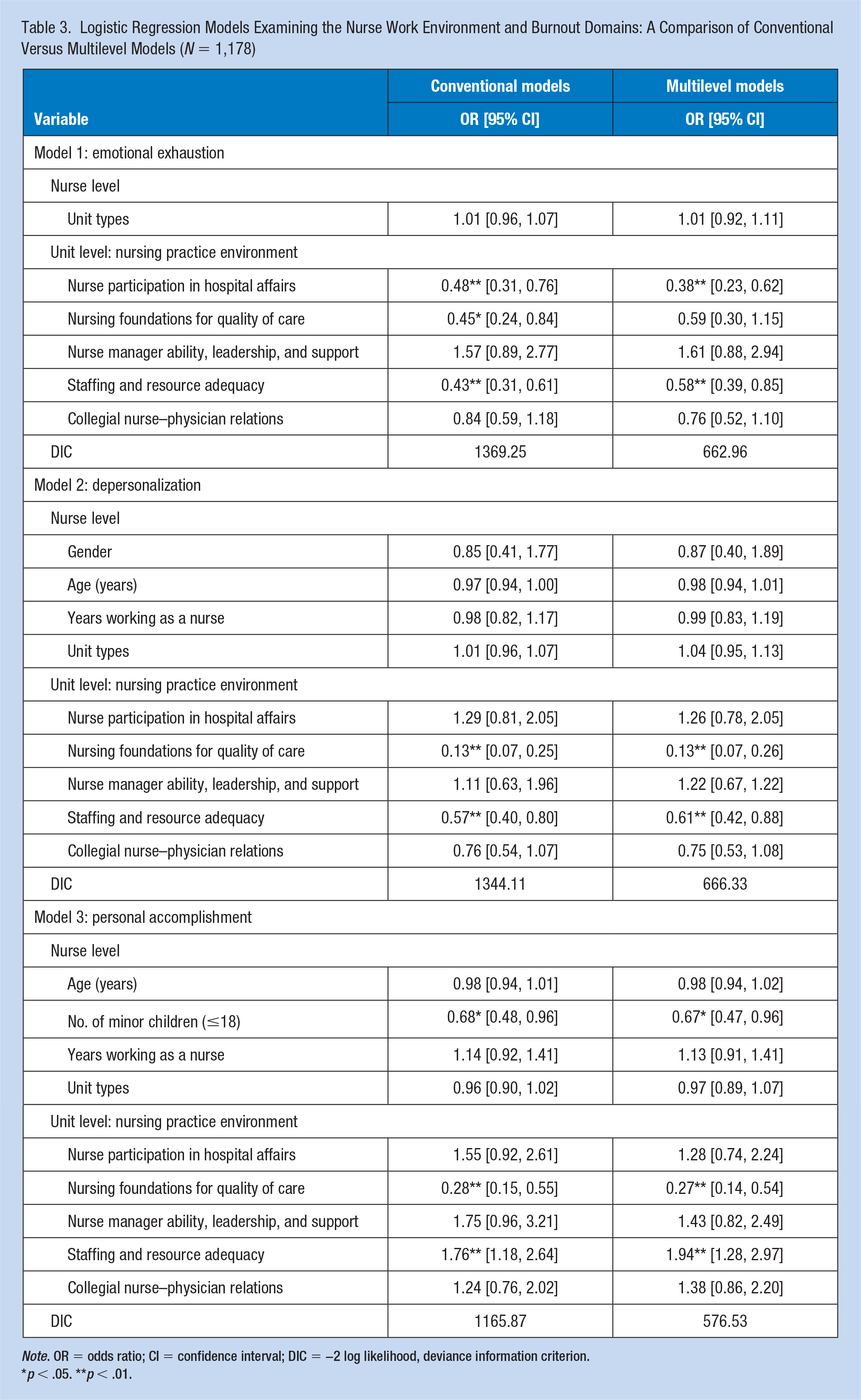
Note. OR = odds ratio; CI = confidence interval; DIC = −2 log likelihood, deviance information criterion.
p < .05. **p < .01.
Results from the null models showed that the unit-level variance regarding the three dimensions of occupational burnout all yielded p-values of less than .05, indicating that the study data were hierarchically structured and thus justified the application of an MLM approach. Besides, the proportion of total variance that was attributed to the unit level (ICC) was 20.31% for EE, 13.55% for DP, and 6.48% for PA.
The findings derived from the multilevel logistic regression models found that unit-level nurse participation in hospital affairs (OR = 0.38, 95% CI = [0.23, 0.62]) and adequate staffing and resources (OR = 0.58, 95% CI = [0.39, 0.85]) were negatively related to emotional exhaustion. Unit-level nursing foundations for quality of care (OR = 0.13, 95% CI = [0.07, 0.26]) and staffing adequacy (OR = 0.61, 95% CI = [0.42, 0.88]) were negatively related to depersonalization. Significant effects on personal accomplishment were found for nursing foundations for quality of care (OR = 0.27, 95% CI = [0.14, 0.54]) and adequacy of staffing (OR = 1.94, 95% CI = [1.28, 2.97]) on unit level.
As for the DIC, modeling each dimension of job burnout with conventional analyses yielded DIC estimates of 1369.25, 1344.11, and 1165.87 for EE, DP, and PA, respectively, while in the multilevel analyses yielded DIC estimates of 662.96, 666.33, and 576.53, respectively (Table 3). It was evident that the DIC values from the MLM were less than half the magnitude of those from the conventional analyses.
Discussion
We studied the impact of the unit-level practice environments on nurse burnout dimensions using both conventional and multilevel logistic regression models. The findings provide practical information for combating occupational burnout among nurses and highlight the appropriateness and effectiveness of applying MLM in relevant nursing research.
The nursing practice environment was generally perceived as favorable in our study as measured by the PES-NWI, with that of the emergency room and the psychiatric unit lagging somewhat behind. This finding supports previous studies indicating that unit-specific interventions should be contemplated to achieve better practice environments (Li et al., 2013). In addition, our study showed that many Chinese nurses suffered high degrees of burnout, and among them, symptoms of EE or DP were the most common. The alarming increase in the number of patients, along with their increased demands for better-quality services, and the relatively deficient and unevenly distributed medical resources in China might explain the high burnout prevalence among Chinese RNs (Huang, 2016; Sun & Luo, 2017).
Impact of the Unit-Level Practice Environment on Nurse Burnout
Since the estimated parameters obtained from the conventional and multilevel models did not substantially deviate, only the MLM results are discussed here. In the two-level model fitted to our data, positive ratings for unit-level nurse participation in hospital affairs and adequate staffing were tied to lower levels of emotional exhaustion. This finding is in line with that of Nantsupawat et al. (2015), who concluded that nurses who complained about unfavorable practice environments were far more likely than others to experience emotional exhaustion. If nurses had an equal voice and vote in decision-making for hospital affairs, they perceived themselves as empowered and that they mattered, which could increase their organizational commitment and decrease their risk of feeling emotionally depleted. In addition, adequate staff and timely supportive resources could help employees avoid hectic work situations; thus, the exhausted feelings might be altogether prevented or at least mitigated (Leiter & Laschinger, 2006). These findings suggest that fostering an organizational environment of involvement with sufficient resource support, nurses would be less susceptible to emotional exhaustion.
Depersonalization implies excessively detached responses to various facets of the job (Maslach et al., 2001). Our results suggested that unit-level nursing foundations for quality of care, together with staffing and resource adequacy, were significantly and negatively related to such untoward reactions, which reinforced the previous evidence of Li et al. (2013). When working in an environment with more consolidated foundations for patient care, that is, one in which the nursing employees are sufficiently competent and the hospital is committed to a nursing (rather than a medical) model, nurses tend to enjoy a greater congruence between personal and organizational values. While in an environment with personnel deficiencies, each nurse has to intensify their workload to try and cover the daily assigned tasks. In the long term, such conditions predispose them to depersonalization and to gradually alienate themselves from others (Leiter & Laschinger, 2006). Such results highlight the necessity of shared values and sufficient staffing in workplaces to ensure desirable nurse job outcomes and high-quality patient care.
A sense of personal accomplishment is an important buffer against the whole range of burnout syndrome (Maslach et al., 2001). Staffing and resource adequacy on unit level was found to be positively related to feelings of personal accomplishment. Similar findings were also seen in an earlier study using cross-sectional RN survey data from the Swedish part of RN4CAST project (Leineweber et al., 2014). Yet, the enduring nurse shortage has maintained a substantial problem for Chinese hospitals. As stated by National Development and Reform Commission (2016), the nurse-to-physician ratio was 1.07:1 and there were only 2.36 RNs per 1000 people in China, far behind that in developed countries. A shortfall in staffing and resources was a major concern of RNs as they are unable to meet all the demands of their work. Chronic understaffing obviously increases the workload and has been listed among the driving forces behind the reduced personal accomplishment (Liu et al., 2012; Topcu et al., 2016). In contrast, when working in a well-resourced/staffed environment, nurses would be more likely to develop feelings of efficacy. Accordingly, it is crucial to reasonably increase nurse staffing levels in units to prevent employees from experiencing feelings of incompetence.
Of note in our study is the negative correlations between nursing foundations for quality of care and personal accomplishment. The findings are inconsistent with previous studies. Leiter and Laschinger (2006) have reported that employees who recognized elements of a nursing model of patient care within their professional environment could derive a deeper sense of accomplishment from their jobs. Nursing foundations for quality of care emphasizes the nursing foundations for a high standard of patient care (Lake, 2002), which not only implies a pervasive nursing philosophy and a nursing (rather than a medical) model of care but also implies requirements for nurses’ clinical competence. For example, two of the items of this dimension are stated as “an active quality assurance program” and “high standards of nursing care are expected by the administration.” High-standard patient care requiring highly skilled staff, continuous nurse training, and some inspection procedures may possibly intensify the already demanding nursing work, which could be one of the explanations to this result. On the contrary, prior studies tended to group the hospital environment into different categories (i.e., unfavorable, mixed, or favorable) according to the composite score of the PES-NWI, and these groupings roughly indicated that an unfavorable work environment was associated with professional incompetence (Liu et al., 2012; Topcu et al., 2016). Instead, we studied the impact of each dimension of work environment dynamics on nurse burnout. The present results, however, warrant further confirmation.
Comparison Between the Conventional and Multilevel Logistic Models
The results from the null models verified that individual RNs’ responses (for nurse burnout) shared a hierarchical structure and therefore justified the application of MLM in the present study. This finding is consistent with those published elsewhere (Gutacker et al., 2018; Hox et al., 2017; Zhu et al., 2017), which examined the responses of students within classes, doctors within hospitals, and patients within communities. For studies undertaken in a multilevel context, the conventional analytical techniques may be suboptimal because they ignore the statistical dependency of the nested observations.
Discrepancies between the two methods in our sample indicated that, for one thing, the conventional models invariably produced smaller standard errors than the multilevel logistic models. For another, the statistically significant relationship identified by the conventional model no longer existed when the data were fitted to the multilevel model. Specifically, in the conventional model, nursing foundations for quality of care was significantly related to the emotional exhaustion dimension, yet it failed to approach statistical significance in the multilevel model. Taken together, the conventional models tended to underestimate the standard error, thereby risking making a type I error, that is, falsely rejecting a true null hypothesis, and are less robust in comparison with the MLM approach for handling the hierarchical data. In addition, comparing the DIC of the two analytical methods for each dimension of burnout highlighted the better fit and parsimony of the multilevel models. Similar findings have also been reported in studies of other disciplines such as sociology, anthropology, and pedagogy (Yusuf et al., 2011; Zhu et al., 2017). The results of our study agreed with others in the literature suggesting the efficiency and precision of MLM for dealing with hierarchically structured data.
Although the results yielded by the conventional and multilevel models did not differ substantially in this study, we revealed that recognizing and accounting for the data structure could produce more accurate results and generate more reliable inferences. Hierarchical data constitute an increasingly common evidence base in a wide range of research fields (Austin & Merlo, 2017), with no exception in nursing; as such, it is imperative that nursing researchers should routinely consider incorporating this statistical methodology in their analysis.
The study is of rigorous conception and precise implementation, yet it is not free from limitations. First, given that the respondents are only from one tertiary hospital in urban Chinese areas, the generalizability of our study is somewhat limited. Conducting research pursued in a wider range of hospitals would allow exploration of both hospital-level and unit-level effects using MLM. Second, inclusion of self-reported multilevel data as well as organizational construct data from other sources (e.g., nurse-to-patient ratios, night-shift frequency, and work time per shift) in analyses could provide broader insights into the impact of independent variables on the outcomes. Third, with the cross-sectional design, inferences of causality cannot be confirmed; thus, additional investigations with longitudinal or interventional designs are warranted to offer broader insights into related topics.
Implications for Occupational Health Nursing Practice
Nurse burnout is highly prevalent among Chinese nurses, which could lead to a variety of undesirable outcomes, from psychologic distress, somatic complaints, and decreased performance to poorer quality of patient care and occupational attrition. Our findings provide actionable strategies for combating nurse burnout symptoms. Specifically, hospital managers could prioritize policies and practices involving RNs in the decision-making process and properly reinforcing nursing foundations for care quality. In addition, an integrated vision promoting quality care in tune with the actual workforce merits administrative attention. The results also imply that recognizing and accounting for the data structure in a statistical analysis could generate more accurate results, thereby yielding more reliable inferences.
Conclusion
Our findings have strengthened previous knowledge about the impact of the practice environment on nurse burnout and provided encouraging support for advancing efforts to build healthier work conditions. Specifically, effective measures contributing to a better organizational environment, such as facilitating nurse decision latitude and keeping staffing in tune with the actual job demands, should be actively embraced to counterbalance employee burnout. Properly reinforcing nursing foundations for care quality should also be highly advocated. In addition, erroneous inferences may arise from the neglect of data structure, so caution should be intensified when analyzing data from clustered observations. We recommend that in nursing research, the MLM technique should be routinely taken into consideration when performing statistical analyses.
Applying Research to Practice
Occupational burnout is highly prevalent among Chinese nurses. Our findings suggest that effective measures contributing to a better organizational environment, such as facilitating nurse participation in hospital affairs, reinforcing nursing foundations for care quality, and keeping staffing in tune with the actual job demands, should be actively embraced to counterbalance nurse burnout. The findings also suggest that there generally exist hierarchical effects within data that are hierarchically structured. Erroneous inferences may arise from the neglect of data structure. Therefore, when analyzing data, recognizing and accounting for the data structure is of significant importance and can lead to more accurate and reliable results.
Footnotes
Acknowledgements
We acknowledge the valuable contribution of Jiaqiang Liao from the Department of Health Statistics of Sichuan University for his technical support about the application of the multilevel analysis.
Author Contributions
F.J., C.Y., and L.Y. were responsible for study design. C.Y., L.Y., and Z.C. were responsible for data collection. C.Y. and Z.C. were responsible for data analysis. L.Y. and F.J. were responsible for manuscript writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Li Yuan, PhD Candidate, RN, is a doctoral student at West China Hospital/West China School of Nursing, Sichuan University, and has a keen interest in occupational health research in nursing.
Chen Yumeng, MSN, RN, is a senior nurse, currently working at the Department of Geriatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. Her research interests are focused on the health effects of modifiable workplace factors and the elderly care.
Zhou Chunfen, MSN, RN, is a junior nurse working at Mental Health Center of West China Hospital, Sichuan University. Her research interests are focused on the quality of care for psychiatric patients.
Fang Jinbo, PhD, RN, is a professor at Nursing Department, West China Hospital, Sichuan University, whose researches focus on the effects of work-related factors on nurse fatigue, job satisfaction, and occupational attrition and also the management project of cardiovascular disease patients.