
Abstract
Background: The work environment factors associated with nurses’ intention to leave their jobs are not well understood because most studies have used non-probabilistic sampling methods, thus restricting the generalizability of the results. This study examined the relationship between work environment factors and intent to leave among nurses working in acute care hospitals in Ontario, Canada. Methods: This study included a random sample of 1,427 registered nurses who were part of a larger cross-sectional study and who responded to a mailed survey that included measures of resource availability, interprofessional collaboration, job satisfaction, and demographics. Results: Most of the respondents were female (94.8%), with an average age of 45.6 years, and 14.5 years of nursing experience at their current workplace, which included mostly urban (94.6%) and non-teaching hospitals (61.8%). In the multivariate model, we observed that the work environment variables explained 45.5% of the variance in nurses’ intent to leave scores, F(9, 1362) =125.41, p < .01, with an R2 of .455 or 45.5%. Job satisfaction (p < .01), flexible interprofessional collaborative relationships (p = .030), and resource availability (p < .01) were significantly associated with nurses’ intent to leave scores. Conclusion/Application to Practice: Nurses who reported greater job satisfaction, flexible interprofessional relationships, and resource availability were less likely to express an intent to leave their hospital workplaces. Employers and health policy makers may use these findings as part of a broader strategy to improve the work environment of nurses. Occupational health nurses are ideally positioned to demonstrate leadership in promoting retention efforts in the workplace by advocating for the importance of job satisfaction, flexible interprofessional relationships, and resources.
Background
Hospitals are the largest employer of nurses and nurses represent the largest group of health professionals (College of Nurses of Ontario [CNO], 2017); however, a large body of research over the last 20 years has established that a persistent nursing labor shortage exists in Canada (Baumann et al., 2016), the United States (Buerhaus, Skinner, Auerbach, & Staiger, 2017; Juraschek, Zhang, Ranganathan, & Lin, 2012; Snavely, 2016), the United Kingdom (Buchan & Seccombe, 2018), and Australia (Drennan & Ross, 2019). In the United States, the average nurse turnover rate in 2017 was 18.2% (an increase from 16.2% in 2016) with 23.7% of hospitals reporting a vacancy rate exceeding 10% (Nursing Solutions, Inc., 2019). If the health needs of Canadians like many other Western nations continue to increase with an aging population, Canada will be short almost 11,000 full-time equivalent nurses by 2022 (Murphy et al., 2012). The estimated nursing workforce supply is less than the estimated increase in requirements over the same period (2007-2022; Murphy et al., 2012). The Canadian Nurses Association estimates that reducing the overall exit rate of nurses to 2% would minimize the shortage by close to 55,500 full-time equivalent nurses (Murphy, Birch, & Alder, 2009).
The principal concept of the nursing work environment stipulates that nurses join an organization with certain expectations such as good working relationships and adequate resources, and the assumption is that when these expectations are not met, they will leave their current workplaces (Borhani, Abbaszadeh, Nakhaee, & Roshanzadeh, 2014). Studies have shown that job dissatisfaction (Yarbrough, Martin, Alfred, & McNeill, 2017), poor interprofessional collaboration (Larrabee et al., 2010), hospital non-teaching status (Lacey et al., 2007; Staggs & Dunton, 2012), hospital rural region (Baernholdt & Mark, 2009; Nowrouzi et al., 2016), and a lack of resources (Boltz et al., 2008; Kim, Capezuti, Boltz, & Fairchild, 2009) are associated with nurses’ intent to leave their hospital workplaces. Because nurse retention is associated with better patient outcomes (Al-Hamdan, Manojlovich, & Tanima, 2017; Nowrouzi et al., 2016), understanding the work environment factors associated with nurses’ intent to leave their workplaces is vital.
While several studies have examined Canadian nurses’ intent to leave their hospital workplaces, most used non-probabilistic sampling methods (Gosselin, Bourgault, & Lavoie, 2016; Krebs, Madigan, & Tullai-McGuinness, 2008), thus limiting the generalizability of the results. Some studies have found nurses’ intent to leave to vary by primary area of practice but did not control for this variable (Hart, 2005; Rambur, Palumbo, McIntosh, & Mongeon, 2003; Rushton, Batcheller, Schroeder, & Donohue, 2015). This study overcomes these limitations by using a probability sample of nurses to examine the factors associated with intent to leave while controlling for nurses’ primary area of practice.
The objective of this study was to examine the relationship between the work environment factors (job satisfaction, interprofessional collaboration, hospital teaching status, hospital region, and resource availability) with intent to leave among hospital nurses in Ontario, Canada.
Methods
Design
The data for this study were obtained from a larger cross-sectional study that used Dillman’s tailored survey design method (Dillman, Smyth, & Christian, 2014) and was conducted in Ontario, Canada, in 2012. The survey invited nurses to respond to several measures of the work environment factors, nurses’ level of geriatric knowledge, nurses’ practices, and demographic characteristics.
In the larger study, the names of potential participants were randomly selected from the CNO database. Nurses were eligible to participate if (a) they were registered and “in good standing” with the CNO; (b) their clinical practice location was in Ontario; (c) they were employed in an acute care hospital; (d) their primary practice area was medicine, surgery, geriatrics, emergency, or critical care; and (e) they worked as staff nurses. In the larger study, we mailed 4,249 surveys; 629 were returned as undeliverable or the participant was no longer eligible (e.g., primary practice area) for a valid denominator of 3,620 in which 2,005 (55% response rate) eligible nurses responded (Fox et al., 2016). From the database of 2,005 nurses, we included the data from 1,427 registered nurses in this study and excluded 561 registered practical nurses.
Nurses were provided a mailed introductory letter informing them of the study, and that within a week, a subsequent package would be mailed to them containing the study cover letter, informed consent, and survey. Nurses who did not respond to the survey were sent up to two mailed reminders (Fox et al., 2016). The survey was approved by the Research Ethics Board of York University in Toronto, Ontario, Canada, and all participants provided informed written consent.
Study Measures
To characterize the sample, demographic characteristics were measured by standard questions on nurses’ age, sex, employment status (e.g., full- or part-time), years of work experience as a nurse, highest level of education in nursing, and shifts worked (e.g., days, evenings).
Intent to leave
Nurses’ intent to leave was measured by the Propensity to Leave Scale (Lyons, 1971). The scale contains three questions: (a) “If you were completely free to choose, would you prefer to continue working in this hospital or would you prefer not to?” (b) “How long would you like to stay in this hospital?” and (c) “If you had to quit work for a while (for example, because of pregnancy), would you return to this hospital?” (Lyons, 1971, 1981). A 5-point scale that contained different statements for each item, and ranged from 1 (e.g., I would prefer very much to continue working in this hospital) to 5 (e.g., I would prefer very much not to continue working here), was used in the rating. The scale scores were derived by summing the responses to the items and ranged from 3 to 15, with higher scores reflecting greater intention to leave. The psychometric properties of the scale have been previously validated (Brief & Aldag, 1976; Latack, 1986; Lyons, 1971; Sutton & Rousseau, 1979), and the scale has demonstrated internal consistency reliability with a Cronbach’s alpha of .83 (Koberg & Hood, 1991).
Work environment
Resource availability was measured by the Geriatric Resource Availability Subscale of the Geriatric Institutional Assessment Profile (Abraham et al., 1999). The subscale has eight items that measure nurses’ perceptions of the extent to which the lack of human and material resources interferes with their ability to provide care to hospitalized older adults. A 5-point scale that ranged from 1 (greatly interferes) to 5 (does not interfere) was used in the rating. Subscale scores, which were derived by summing the responses to the items, can range from 8 to 40 (lower scores reflect greater interference). The subscale previously demonstrated internal consistency reliability (Cronbach’s α = .90) and factorial validity (one factor structure with factor loadings ≥ .54) (Kim et al., 2007).
Interprofessional collaboration was measured by two subscales of the Modified Index of Interdisciplinary Collaboration (Oliver, Wittenberg-Lyles, & Day, 2007). The Interdependence subscale has 13 items that measure the extent to which nurses perceive that the members of their team are interdependent and collaborate to accomplish their goals and tasks. For example, respondents were asked to answer the following types of items: “I utilize other professionals in different disciplines for their particular expertise” and “I consistently give feedback to other professionals in my setting.” The Flexibility subscale contains five items that measure nurses’ perceptions of the extent to which members of their team work outside their defined job roles to accomplish their goals and tasks. For example, respondents were asked to respond to the following types of items: “I am willing to take on tasks outside of my job description when that seems important” and “I am not willing to sacrifice a degree of autonomy to support cooperative problem solving.” A 5-point scale that ranged from 1 (strongly disagree) to 5 (strongly agree) was used for both of these subscales. The mean responses to the items were taken in both subscales. Subscale scores can range from 1 to 5 with higher scores indicating higher interdependence and flexibility. Both subscales exhibited a Cronbach’s alpha of .87 or higher in prior research (Bronstein, 2002).
Job satisfaction was measured using the Job Satisfaction Scale (Hinshaw, Smeltzer, & Atwood, 1987). Respondents were asked to respond to three items: “All in all, I am satisfied with my job”; “In general, I don’t like my job”; and “In general, I like working here.” A 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree) was used in the rating. The scale score was calculated by summing the responses to the items after reverse coding the negatively worded item “In general, I don’t like my job.” The sum of scores can range from 3 to 21 with higher scores indicating higher job satisfaction. The subscale had a Cronbach’s alpha of .87 in prior research (O’Hara, Beehr, & Colarelli, 1994).
Hospital teaching status (non-teaching vs. teaching) was measured by asking nurses to indicate the name of the hospital in which they worked. We used this to determine the hospital’s membership in the Council of Academic Hospitals of Ontario (2018). Hospital region (rural vs. urban) was determined to be urban if the census agglomerations had at least 10,000 inhabitants, and the census metropolitan areas (Statistics Canada, 2006) had populations of at least 100,000 (Statistics Canada, 2013). All other hospitals were determined to be located in a rural region. Primary area of practice was measured by a single question that asked nurses to indicate which unit they worked on the most (e.g., emergency, medical, surgical).
Data Analysis
Descriptive statistics were tabulated to characterize the sample and to evaluate the variables for departures from normality and violation of the assumptions underlying the statistical modeling employed. Multiple regression was applied to examine the associations of nurses’ job satisfaction, hospital region (rural vs. urban), hospital teaching status (teaching vs. non-teaching), and interdependent and flexible interprofessional collaborative relationships (e.g., Interdependence and Flexibility subscales) with nurses’ intent to leave while controlling for nurses’ primary area of practice.
The goodness of fit for the model was calculated using the r2 equivalent (r2 is the proportion of explained variation) based on the difference between the likelihood ratio of the fitted model and the likelihood ratio of the null model (e.g., a regression model without any variables). We used STATA Version 11.0 (StataCorp, 2009) variance–covariance estimation bootstrap option to handle clustering and model-specific details. Percentile bootstrap confidence intervals (CIs) were enhanced by an alteration to the percentile values of the sorted distribution of bootstrap estimates used for determining the bounds of the interval using the bias-corrected (BC) and accelerated (BCa) intervals (Preacher & Hayes, 2008). The BCa is expected to perform better than BC but can be computationally prohibitive in large databases and/or non-linear estimation (Hansen, 2010; Table 1).
Nurse Demographic Characteristics and Primary Area of Practice (N = 1,427)
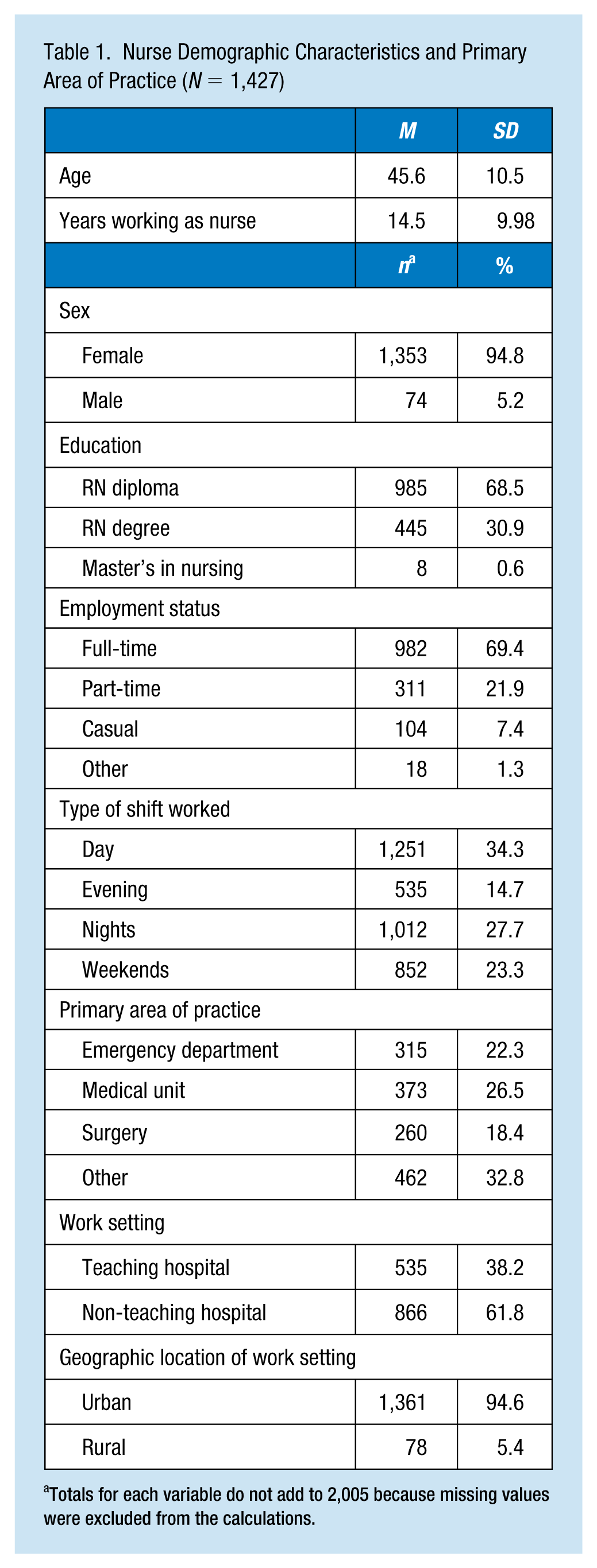
Totals for each variable do not add to 2,005 because missing values were excluded from the calculations.
Results
Descriptive Results
Table 1 presents the demographic characteristics of the sample. The average nurse age was 45.6 years (SD = 10.5) and female (94.8%). Most of the nurses were educated at the diploma level (68.5%). Almost 31% had a bachelor’s degree in nursing and 0.6% of the sample had a master’s degree. Most worked full-time (69.4%) but close to 30% worked part-time or other non-full-time arrangements (e.g., casual work). Furthermore, the most predominant shift worked was day (34.3%), with 14.7% working evenings, 27.7% working nights, and 23.3% working weekends. The primary areas of practice for this sample were emergency departments (22.3%), and medical (26.5%) and surgical (18.4) units, and other (32.8%). In addition, the participants had an average of 14.5 years (SD = 9.98) of experience as a nurse at their current workplace. Most nurses worked in a non-teaching hospital (61.8%) located in an urban area (94.6%). The sample’s demographic profile presented in Table 1 is comparable with the nursing workforce in Ontario (CNO, 2017) and across Canada (Canadian Nurses Association, 2018).
The mean score and standard deviation for the Propensity to Leave Scale were 5.59 (SD = 2.71) (data not shown). Given that the scale scores can range from 3 to 15 and higher mean scores reflect greater intention to leave, the average nurse reported a low intention of leaving their current position. The Geriatric Resource Availability average score was at the midpoint of the possible scale scores of 8 to 40 (M = 22.0, SD = 6.23); considering that lower scores indicate greater interference in nurses’ ability to provide care, this average score suggests that the lack of resources somewhat interfered with nurses’ ability to provide care.
The mean score and standard deviation for the Interdependence subscale was 4.02 (SD = 0.47) (data not shown). Bearing in mind that the scale scores can range from 1 to 5 with higher scores indicating higher interdependence, the average nurse agreed that the members of their team are interdependent and collaborate to accomplish their goals and tasks. Similarly, the Flexibility subscale, with identical scale scores as the Interdependence subscale, had a mean and standard deviation of 3.60 (SD = 0.51). This mean score, which is above the midpoint of the scale, indicated that the average nurse did not quite agree but was approaching agreement that team members work outside their defined job roles to accomplish their goals and tasks.
The Job Satisfaction Scale had a mean score and standard deviation of 16.6 (SD = 3.62) (data not shown). Given that the scores can range from 3 to 21 with higher scores reflecting higher job satisfaction, the average nurse was satisfied with their job.
In the multivariate model (Table 2), the work environment variables explained 45.5% of the variance in nurses’ intent to leave scores, F(9, 1362) = 125.41, p < .01, with an R2 of .455 or 45.5%. Job satisfaction (p < .01), flexible interprofessional collaborative relationships (p = .030), and resource availability (p < .01) were significantly associated with nurses’ intent to leave scores. For every unit decrease in job satisfaction, there was a 0.047 predicted increase in intent to leave scores as indicated by the associated parameter estimate. For every unit increase in flexible collaborative relationships, there was a 0.26 increase in intent to leave scores. Similarly, for every unit decrease in resource availability, there was a predicted 0.043 increase in intent to leave scores.
Multiple Regression and Approximate 95% CIs Using Bootstrapping for Nurses’ Work Environment Factors Associated With Intent to Leave
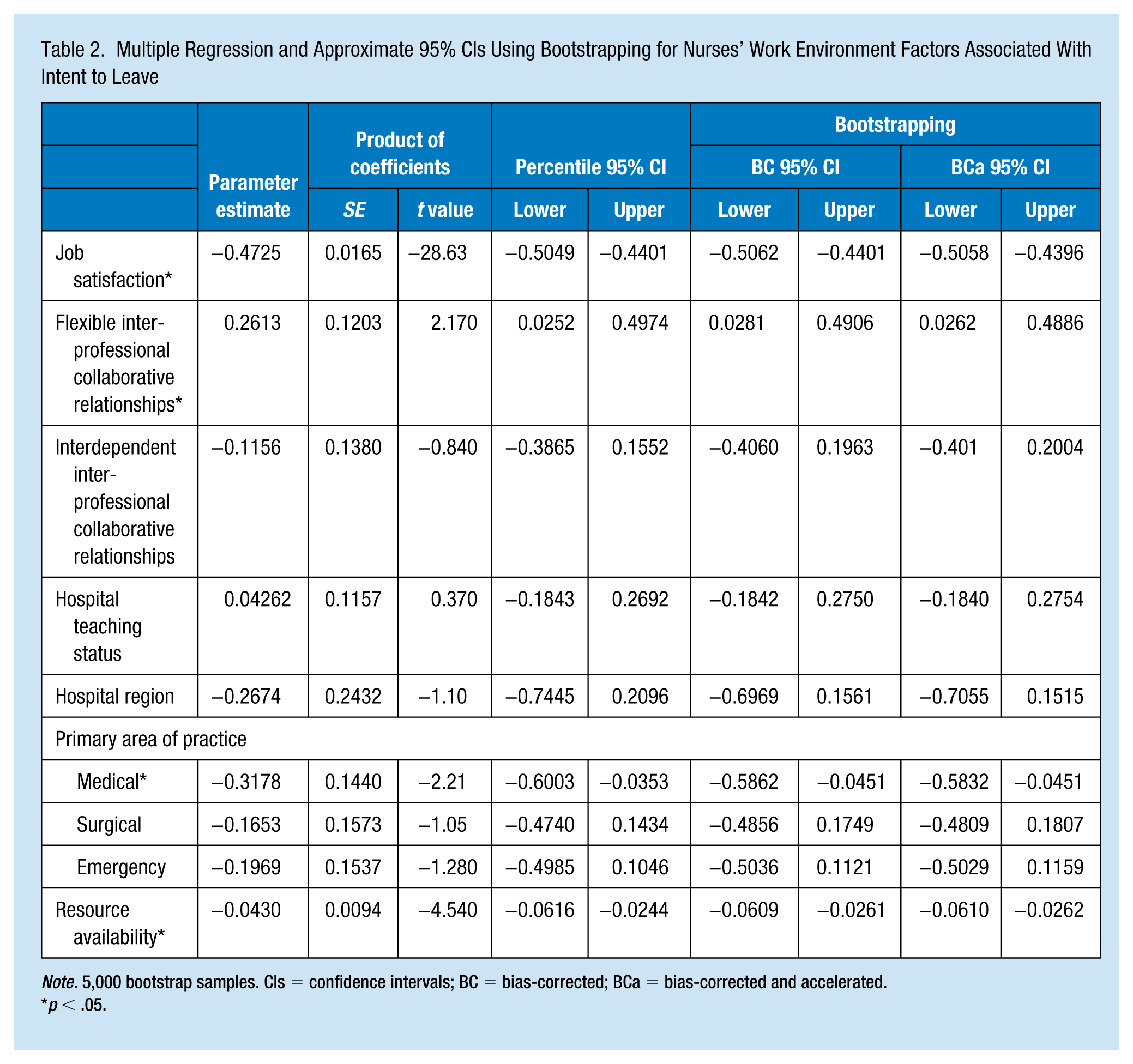
Note. 5,000 bootstrap samples. CIs = confidence intervals; BC = bias-corrected; BCa = bias-corrected and accelerated.
p < .05.
Discussion
This study examined the relationship between nurses’ intent to leave and work environment factors defined by nurses’ job satisfaction, flexible interprofessional collaborative relationships, as well as their hospital teaching status, region, and resource availability, while controlling for nurses’ primary area of practice. We identified that nurses who reported greater job satisfaction, flexible interprofessional relationships, and resource availability are less likely to express an intent to leave their hospital workplaces. These findings concur with international research, which has shown an association between nurses’ intent to leave and these three work environment factors (Al-Hamdan et al., 2017). Specifically, a recent systematic review supported the negative relationship between job satisfaction and intent to leave (Council of Academic Hospitals of Ontario, 2018) as have individual studies spanning the last three decades (Applebaum, Fowler, Fiedler, Osinubi, & Robson, 2010; Cavanagh & Coffin, 1992; Hayes et al., 2006; Lu, Barriball, Zhang, & While, 2012; Lu, Zhao, & While, 2019).
With regard to interprofessional collaboration, our study findings suggest that flexible interprofessional relationships, but not interdependent interprofessional relationships, are important to nurses’ intent to leave. In seeking to explain why flexible and not interdependent interprofessional relationships are associated with nurses’ intent to leave, we consider the items of the subscales. The items in the Flexible subscale tapped nurses’ perspectives on the extent to which they themselves are willing to take on tasks outside their job descriptions and make sacrifices to support cooperative problem solving. Although further research is needed, it is possible that these items may be measuring an attitude toward compromise which may be related to nurses’ intent to stay in their current positions. However, the subscale also contained items that solicited nurses’ perspectives on the extent to which their interprofessional colleagues do not strictly adhere to their roles and work together in diverse ways. It is possible that working with interprofessional colleagues who are perceived by nurses as flexible in their roles or to have a blurring of roles may be more important to mitigating nurses’ intent to leave their current positions than are having relationships that are interdependent in accomplishing work goals and tasks as measured by the items of the Interdependence subscale.
Regarding resource availability, the existing literature has demonstrated that nurse’ intent to leave decreases in adequately resourced environments (Abou Hashish, 2017; Ulrich et al., 2007). Tschannen et al. (2010) examined the underpinnings of resource availability on nurses’ intent to leave and found that units with fewer resources had more staff who reported the intention to leave their position.
Our study did not find that hospital teaching status or region to be significantly associated with nurses’ intent to leave. These findings are in contrast to a study of over 25,000 American nurses, which reported lower intent to leave scores in nurses working in teaching hospitals than those in non-teaching hospitals (Kelly, McHugh, & Aiken, 2011). The disparities between studies may be due to differences in health care settings in the United States and Canada, and in how intent to leave was measured in each study.
This study has some limitations. First, the study was reliant on self-reported data, which may have led to inaccuracies of the results. However, we used validated instruments with strong psychometric proprieties. The study sample included nurses working in hospital settings in one Canadian province and may not be representative of those working in other provinces or work settings.
Future studies are warranted to examine the causal relationship between various work environment factors such as job satisfaction, resource availability, and interprofessional collaboration. These studies should employ rigorous methodological approaches such as longitudinal designs to identify work environment factors and identify strategies to retain the nursing workforce. Such initiatives may also offer insight on potential interventions to promote a healthy work environment and ultimately lead to better health care delivery and patient outcomes.
The study findings add to a growing body of literature that employers and health policy makers may use as part of a broader strategy to improve the work environment of nurses. Intent to stay is an important issue for ensuring the delivery of quality nursing care. We call on hospital administrators to improve nurses’ work environment as it has the potential to improve the delivery and quality of health care services. Hospital administrators can use the findings to cultivate strategies to prevent or mitigate these work environment factors which may have the potential to improve retention efforts.
Implications for Occupational Health Nursing Practice
The work environment plays a significant role in the health and well-being of nurses and can have deleterious physical and mental health effects. Given their training and qualifications, occupational health nurses have a profound understanding of the work environment and health human resources, and are ideally positioned to address workforce issues related to retention. Occupational health nurses can directly influence the present and future nursing work environment through their intimate knowledge of the occupational health and safety practices. Through a collaborative approach with employers, occupational health nurses will be able to exert a significant degree of influence within the work environment and the broader health care system. Occupational health nurses may also seek opportunities to increase interprofessional relationships across nursing disciplines and with other health professionals, and may examine strategies to improve the work environment and increase job satisfaction.
Applying Research to Occupational Health Practice
This study used a methodologically rigorous approach to identify key factors associated with nurses’ intent to stay in their current position. It further provides validation of key factors associated with a positive and healthy work environment. Occupational nurses along with employers may work together to foster workplaces that promote high job satisfaction, resource availability, and flexible interprofessional collaborative relationships to enhance nurse retention. In turn, a positive work environment is expected to bolster the delivery of health services, including patient care and safety. From an employer perspective, initiatives that support a healthy work environment may reduce training and work absenteeism costs. Moreover, a healthy work environment can inform occupational health policy to support nursing retention initiatives to combat against the workforce shortage experienced in numerous countries.
Footnotes
Author Contributions
All authors made substantive intellectual contributions to this study to qualify as authors. All authors participated in the analysis, interpretation of data, and writing of this manuscript. All authors reviewed the final version, gave the final approval of the version to be published, and agreed to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work will be appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ontario Ministry of Health and Long-Term Care (Grant 06651), the Ontario Ministry of Research and Innovation, and York University.
Author Biographies
Behdin Nowrouzi-Kia is a postdoctoral visitor in the School of Nursing, Faculty of Health at York University.
Mary T. Fox is an associate professor in the School of Nursing, York University.