
Abstract
Background: Uncontrolled blood loss is a primary source of preventable death after injury. Workplace injuries and fatalities are common, with most occurring in the agricultural/fishing/forestry/hunting or transportation/warehousing industries. Stop the Bleed (STB) training provides instruction on application of bleeding control methods to injured persons and is available to the general public. Method: We provided an overview of high-risk injury industries that could benefit from STB training. We also provided a review of the application of STB training and bleeding control methods in occupational settings with an emphasis on the role of the occupational health nurse. Findings: Suggested guidelines for occupational health nurses and employees in occupational settings who may respond to injured colleagues are provided. Implications for occupational health nurses are reviewed, including implementing STB training in the workplace and obtaining/storing bleeding control supplies. Resources for STB training, purchasing and storing bleeding control supplies, and general emergency response information are provided. Conclusions/application to practice: Occupational health nurses play a crucial role in emergency response in the workplace and have the ability to drive the implementation of STB training in their institution. Occupational health nurses often work in isolation or in small teams and serve as a primary resource for treatment of injured employees. Implementation of STB training for all employees is highly recommended given the limited availability of occupational health nurses in large or rural settings. Such training may reduce the morbidity and mortality associated with workplace injuries.
Keywords
Background
Trauma or unintentional injury is the fourth leading cause of death among people of all ages (Murphy, Xu, Kochanek, Curtin, & Arias, 2017). Uncontrolled, life-threatening bleeding is the primary preventable cause of trauma-associated death in the world, with many deaths occurring in the first 48 hours after injury (Kauvar, Lefering, & Wade, 2006). In 2017, more than 5,100 workers died from a work-related injury in the United States (U.S. Bureau of Labor Statistics, 2018). Nonfatal workplace injuries occurred at an incidence rate of 3.2 per 100 full-time workers overall; employees in the agriculture/forestry/fishing/hunting and transportation/warehousing industries experienced the highest incidence rates of nonfatal occupational injuries and illnesses at 5.0 and 4.6 per 100 workers, respectively (U.S. Bureau of Labor Statistics, 2018). The most common causes of workplace fatalities were related to transportation (e.g., roadway incidents, pedestrians struck by vehicles), followed by falls, violence, or injury from another person or animal, and contact with objects and equipment (U.S. Bureau of Labor Statistics, 2017).
With occupational injuries occurring more commonly in these industries, it is likely that those injured will experience delayed emergency response times based on several factors related to worker isolation including (a) the time to recognition of the injury by a co-worker or bystander, (b) the ability of the immediate responder to initiate treatment (if not the occupational health nurse), and (c) the geographic location of the incident (e.g., rural areas). Similar to Basic Life Support training that is widely implemented in occupational settings to train and empower workers to respond to those in cardiopulmonary arrest, workers may also be trained on bleeding control methods (American Heart Association, 2018).
Agricultural/Forestry/Fishing/Hunting Settings
In these settings, large machinery and livestock present work hazards that may lead to injury-associated bleeding due to fractures, amputations, and significant soft tissue damage (Missikpode et al., 2015). Mechanisms of injury commonly associated with motorized agricultural equipment include vehicle rollovers, personnel being run over by vehicles, and collisions (Swanton, Young, Leinenkugel, Torner, & Peek-Asa, 2015). Injuries may also result from encounters with livestock such as pigs, cows, horses, sheep, and/or goats, with larger animals weighing up to a ton (2,000 pounds) or more (Fox, Ricketts, & Minton, 2015).
In 2018, the agricultural/forestry/fishing/hunting workforce was comprised of roughly 1,121,000 workers, of which 516,000 were of Hispanic or Latino ethnicity (U.S. Bureau of Labor Statistics, 2019a, 2019b). Moreover, workers in the agricultural industry alone are generally less educated, less likely to be U.S. citizens, and more likely to be Hispanic (specifically Mexican) (U.S. Department of Agriculture Economic Research Service, 2019). Immigrant workers such as these may be more vulnerable to injury due to language barriers that prevent them from understanding instructions on proper operation of machinery (Byard, 2017). Other issues in agricultural settings that can contribute to injuries may include: pressure to work more quickly or longer hours when faced with impending inclement weather that may damage crops; lack of restriction on clothing that is loose and therefore unsafe when working with machinery; and working with equipment that is not well maintained and more likely to malfunction (Byard, 2017).
Transportation/Warehousing Industries
Daily work activities in the transportation/warehousing industries commonly involve the use of dangerous tools and equipment or operating machinery, all of which pose a major risk of injury to the worker. Risk of injury increases among workers who are inexperienced, fatigued, distracted, or are working in isolation (Mock, Nugent, Kobusingye, & Smith, 2017). For example, sleep deprivation and interrupted sleep cycles due to scheduling demands such as those experienced by long-haul truckers can lead to employees driving or operating machinery while cognitively impaired (Heaton, McManus, Mumbower, & Vance, 2017; Wise, Heaton, & Patrician, 2019). In addition, those in these industries may encounter dangers with completion of work-related duties that could require bleeding control, including loading, unloading, or transferring cargo, either with or without the use of heavy and/or automated machinery (Combs, Heaton, Raju, Vance, & Sieber, 2018).
Implementation of bleeding control training in occupational health settings such as those described could prove beneficial to workers at risk for blood loss postinjury. Here we provide an overview of the Stop the Bleed (STB) Initiative and suggested application of bleeding control training in occupational health settings.
STB Initiative
Development of the STB initiative resulted from a series of events beginning in 2011 when President Barack Obama introduced Presidential Policy Directive 8 in which he called on the U.S. Department of Homeland Security (2018a) to develop a national preparedness system. The purpose of this system was to strengthen the ability of the United States to prevent and respond to security risks such as acts of terrorism or natural disasters. Per the Policy Directive, the term “response” included measures to “save lives” and “meet basic human needs after an incident has occurred” (U.S. Department of Homeland Security, 2018a). After the shooting at Sandy Hook Elementary School in 2012 and many other mass casualty events, the American College of Surgeons (ACS) convened a committee to improve survivability due to traumatic blood loss. Collectively, the recommendations brought forth from this collaboration are referred to as The Hartford Consensus III: Implementation of Bleeding Control, and served to disseminate bleeding control education to the general public (Jacobs et al., 2015). Since that time, the ACS Committee on Trauma has partnered with federal agencies and private and public medical organizations to promote bleeding control training across the country via the STB campaign.
STB Training
STB training was developed by a partnership between the Hartford Consensus Group, the ACS Committee on Trauma, the Committee on Tactical Combat Casualty Care, and the National Association of Emergency Medical Technicians (ACS, 2019a). Table 1 provides an overview of the training agenda. First, trainees are guided through a 30-slide PowerPoint presentation by instructors that includes identification of life-threatening bleeding, criteria for applying the appropriate bleeding control method (tourniquet, wound packing, manual pressure) based on the location of injury, and an algorithm for responding to people who are actively bleeding. Trainees are instructed on use of military-style tourniquets, packing open wounds, and applying manual pressure until emergency responders arrive. In addition, trainees are instructed on assessing scene safety, moving injured persons to safety if necessary, and preventing contact with bodily fluids through the use of gloves when available. Trainees are also informed that everyday items such as clean shirts may be used to improvise should recommended bleeding control materials not be readily available. The slide presentation includes pictures of various wounds and equipment and allows for group discussion of bleeding control methods. Second, trainees are divided into small groups to work with instructors on application of bleeding control methods reviewed in the slide presentation. To receive a certificate of completion, all trainees are required to demonstrate competency in the use of military-style tourniquets, wound packing, and application of manual pressure. Task trainer hemorrhage control mannequin legs (shown in Figure 1) are used to simulate wounds for skill practice.
Stop the Bleed Training Session Agenda
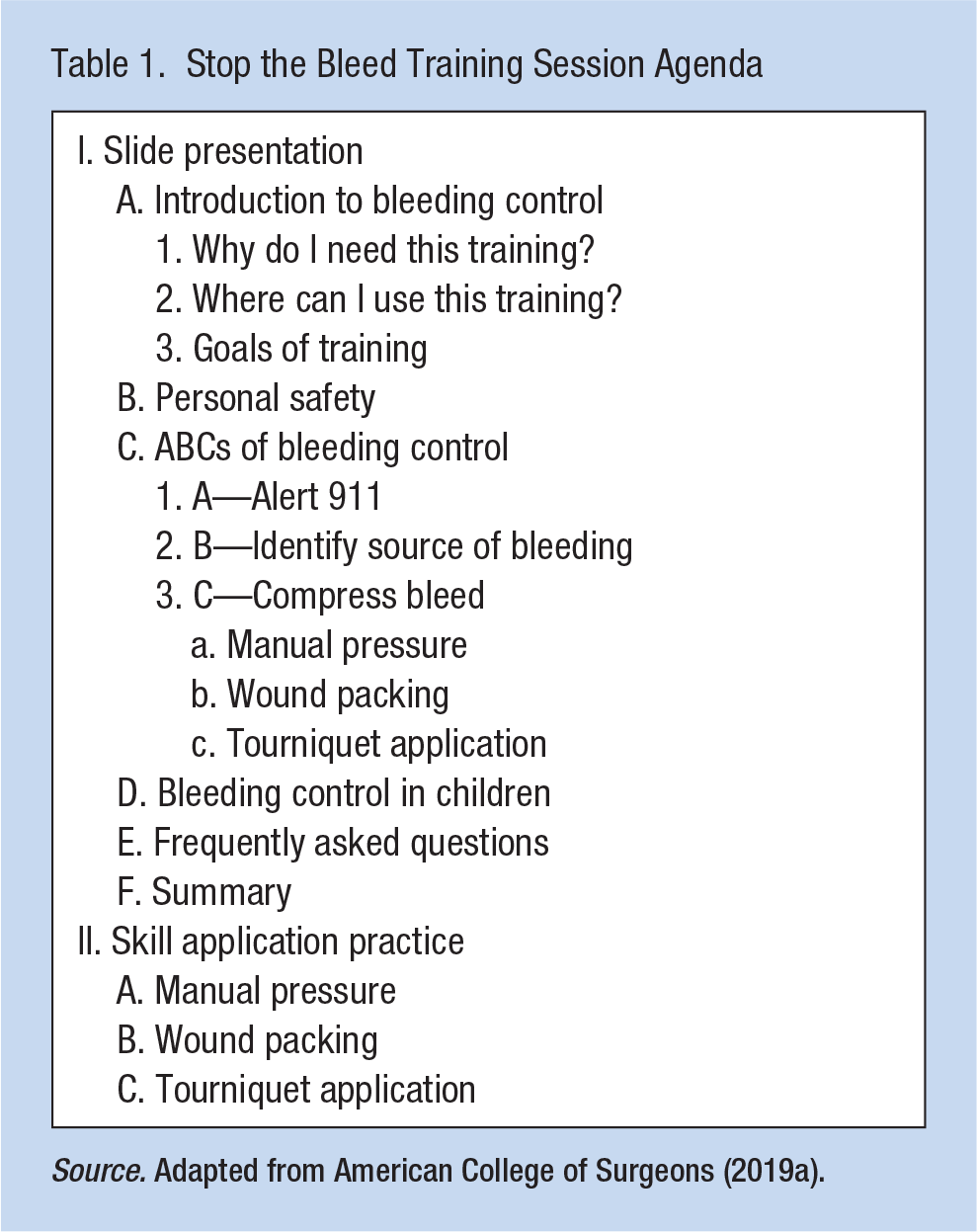
Source. Adapted from American College of Surgeons (2019a).

Participant using STB training model.
Application of STB Training in Occupational Settings
General Guidelines
Occupational health nurses are well positioned to influence employees’ health and educate them on appropriate actions to take in the presence of worker injury (Campbell & Burns, 2015). In the occupational setting, onsite medical professionals such as occupational health nurses are considered ideal candidates for providing STB training to employees. Once trained, occupational health nurses may provide training to any employees physically capable of applying bleeding control methods. Currently, once a person receives STB training, there is no expiration date for STB certification, nor do guidelines exist to support timelines for completion of refresher courses or recertification. As such, employers may consider including STB training as part of annual competencies or pair it with Basic Life Support and Cardiopulmonary Resuscitation training offered by the American Heart Association (2018).
Emergency Response System
As identified in the STB training, proper and timely activation of the emergency response system, or calling 9-1-1 if within the United States, is crucial (ACS, 2019a). Those who are critically injured may experience death or decompensation due to blood loss within a matter of minutes and will require emergency medical services for stabilization. If the initial employee responding to the injured person is alone, they should first call 9-1-1, then locate the bleeding control kit, and follow the STB algorithm accordingly. If two employees are present, one should call 9-1-1 while the other applies bleeding control measures. (Full instructions for application of bleeding control methods are available in the STB training program; employers should not consider these guidelines as a replacement for completion of the STB training.)
Bleeding Control Training and Supplies
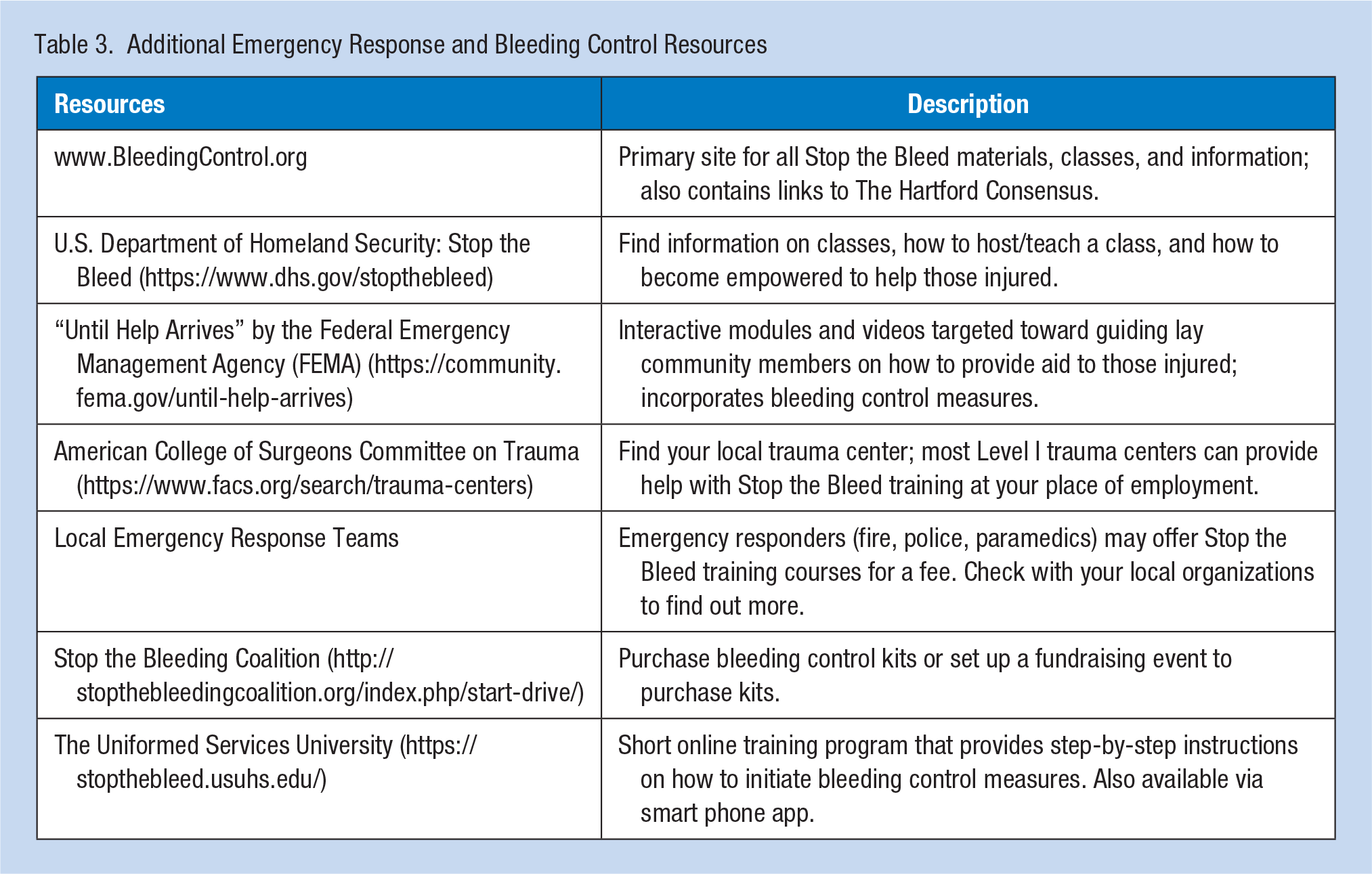
For occupational health nurses interested in STB training, classes are offered from a variety of sources, such as local fire or police departments, local hospitals, or the public health department (U.S. Department of Homeland Security, 2018b). Local course listings are also available at WWW.BLEEDINGCONTROL.ORG. Once training is completed and occupational health nurses are registered as STB instructors at www.bleedingcontrol.org, they can work with employers to obtain bleeding control training kits for their institution. Training kits will allow occupational health nurses to educate employees on bleeding control methods and to refresh employee skills on a regular basis. It should be noted that training kits are intended for use by medical professionals or registered STB instructors only. Bleeding control training kits, personal bleeding control kits, and other related supplies are available for purchase through the ACS website (https://controlbleedingkits.com/; ACS, 2019b). Contents of personal bleeding control kits are listed in Table 2. A comprehensive list of resources for information on bleeding control and STB training, purchase of bleeding control supplies, and general tips for emergency response can be found in Table 3.
Contents of Personal Bleeding Control Kit
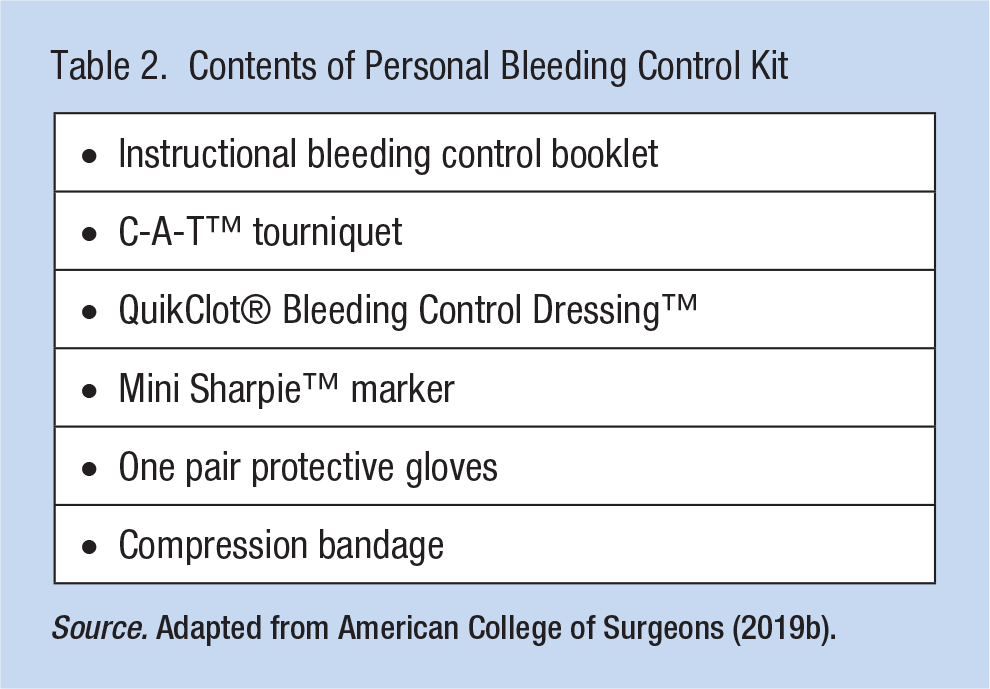
Source. Adapted from American College of Surgeons (2019b).
Additional Emergency Response and Bleeding Control Resources
Occupational Setting Considerations
The number of bleeding control kits required for the occupational setting will depend on the size and layout of the workplace, as well as the number of employees. No guidelines are available to support the exact number of kits to be purchased per organization; however, recommendations indicate that number of bleeding control kits should, at a minimum, match that of automatic external defibrillators in the workplace (Jacobs et al., 2015). Although institutions commonly store only a few automatic external defibrillators, bleeding control kits are smaller, cheaper, and more easily stored in a variety of locations. For example, bleeding control kits may be placed throughout buildings in locations such as high-traffic areas, at reception desks, or at individual work stations for those operating heavy machinery. No matter the number of personal bleeding control kits available at an institution, all kits should be stored in well-marked, central locations easily accessible within 3 minutes of injury (Jacobs et al., 2015). In buildings with multiple areas or floors, it is suggested that kits are consistently placed in areas such as near elevators or bathrooms. Although the ACS does not indicate who should be responsible for maintaining or replenishing bleeding control kit supplies, we suggest the occupational health nurse or those involved with emergency management at the organization assume this role.
Employee Considerations
It is highly recommended that all employees receive STB training, with refresher courses offered at routine intervals such as annual evaluations. Employees working in isolation or in remote areas are encouraged to carry a bleeding control kit with them and should consider wearing a tourniquet (preferably a one-handed model) on their person. This is especially important for employees who routinely work away from their vehicle or equipment where a bleeding control kit may be stored, such as those using farm machinery or long-haul truck drivers. When possible, supervisors or occupational health nurses should make regular rounds to visualize employee safety. Alternatively, predetermined contact times either in-person or via cellular phone or two-way radios may be used to ensure ongoing employee safety. At minimum, all workers should have access to a cellular phone or two-way radio to facilitate timely activation of the emergency response system.
Conclusion
We have reviewed guidelines and considerations for application of STB methods in occupational settings. Occupational health nurses play a crucial role in emergency response in the workplace and have the ability to drive the implementation of bleeding control training in their institution. Training of all employees on bleeding control methods is highly recommended and may reduce the morbidity and mortality associated with workplace injuries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Allison R. Jones, PhD, RN, CCNS, is a certified Stop the Bleed instructor with a background in emergency/trauma nursing. Her current research focuses on methods to enhance Stop the Bleed education and development of a Stop the Bleed community-based train-the-trainer program.
Melanie Gibbons Hallman, DNP, CRNP, CEN, FNP-BC, ACNP-BC, ENP-C, TCRN, FAEN, has provided prehospital and emergency nursing care for more than 35 years. She currently practices as an emergency nurse practitioner and focuses on providing care to the medically underserved population.
Karen Heaton, PhD, COHN-S, CRNP, FNP-BC, FAAN, FAAOHN has extensive experience in emergency/trauma nursing and occupational health nursing. Her program of research is primarily focused on the effects of sleep deprivation and obstructive sleep apnea on cognition and injury risk in workers.