
Abstract
Background: Employees in the Veterans Affairs (VA) hospital experience psychological stress from caring for vulnerable veteran populations. Evidence suggests that mindfulness meditation decreases stress in health care employees and military personnel. The purpose of this worksite program was to explore the acceptability of a mindfulness meditation program among VA workers. Methods: Chaplain residents developed the “Promoting Spiritual Healing by Stress Reduction Through Meditation” (Spiritual Meditation) program for employees in a VA hospital. To evaluate acceptability, a 13-multiple-choice-item survey with an open-ended question was administered after the intervention. Descriptive statistics and qualitative content analysis were performed. Findings: In 29 participants, 70% to 100% agreed with positive statements for the personal learning experience, program components, teacher quality, time to practice, and place to practice. Two categories emerged from qualitative responses: “positive practical experience of Spiritual Meditation” and “perceived values from Spiritual Meditation.” Conclusion/Application to Practice: Occupational health nurses are uniquely positioned to lead and collaborate with chaplains to deliver Spiritual Meditation in their workplace setting.
Background
Veterans experience high levels of stress during the transition from military to civilian life (Mobbs & Bonanno, 2018). In turn, employees in the Veterans Affairs (VA) hospital experience additional psychological stress due to caring for this vulnerable population. VA employees have a moderate level of burnout and psychological stress (Locatelli & LaVela, 2015). Most importantly, burnout and loss of compassion are suggested to contribute to the turnover of VA employees. Kukla, McGuire, and Salyers (2016) identified that psychological stress was a strong barrier to job success among VA employees.
Mindfulness meditation has been an important part of religious, philosophical, and humanistic traditions. It has recently been incorporated into contemporary and alternative medicine (“Meditation: In Depth,” 2019). Mindfulness is the awareness that emerges through paying attention on purpose, currently, and nonjudgmentally to the unveiling of experience moment by moment (Kabat-Zinn, 2003). Mindfulness meditation is a mental and physical activity that creates awareness of present-moment experience with a compassionate, nonjudgmental stance (Brown, Creswell, & Ryan, 2016). An individual’s thoughts and feelings are recognized as events happening in the general awareness. Mindfulness meditation is associated with a perceptual shift. Worldview and perspective play roles in moderating the effect of mindfulness meditation (Dahl & Davidson, 2018). Traditional mindfulness meditation is typically embedded in an individual’s worldview, and the meditation practice subsequently reflecting and reinforcing the individual’s perspective. Therefore, mindfulness meditation can link to spiritual perspective related to cultural, religious, and philosophical context.
The health benefits of mindfulness meditation may be grounded in physical modifications of the brain (“Meditation: In Depth,” 2019). Mindfulness meditation has been identified as a process of awareness (Brown et al., 2016). A study used brain images to understand brain modifications (mainly concerning cortical structure) in meditator and matched control groups (Luders et al., 2012). Positive relationships between gyrification (i.e., function of processing information) in the right anterior dorsal insula and numbers of meditation years were found. These results indicated that mindfulness meditation may facilitate an integration of autonomic, affective, and cognitive processes. Mindfulness could induce the growth and preservation of brain tissues, thereby slowing the negative effects of aging, especially in relation to cognitive impairment (Luders, 2014). A prior study reported that a meditator group had greater thickness of the cortex than a matched control group (Lazar et al., 2005), and there were significant age-related decreases of the thickness of the cortex in the control group but nonsignificant decreases in the meditator group. Furthermore, an increase in the gray matter over time in the meditator individuals suggested an antiaging mechanism related to neuroprotection (preservation) and neuroplasticity (growth) (Pagnoni & Cekic, 2007). In addition, fractional anisotropy indicated integrity of connectivity between different parts of the brain within the white matter (Tang et al., 2010). In one study, the fractional anisotropy value was negatively correlated with age in both meditator and control groups (i.e., smaller fractional anisotropy in older participants) (Luders, Clark, Narr, & Toga, 2011). In the meditator group, the diminished fractional anisotropy was slower over time when compared with the control group. Furthermore, it has been well known that mindfulness meditation mitigates psychological stress and improves emotional well-being (Goyal et al., 2014). One brain image study suggested that mindfulness meditation can change amygdala activities to process emotional stimuli (Desbordes et al., 2012). In this study, participation in an 8-week mindfulness mediation led to a reduction in amygdala response to emotional stimuli which was not seen in the nonparticipation (control) group. In general, the amygdala has been found its involvement in emotional process and the interaction between attention and emotion (Pessoa, 2008).
Mindfulness meditation has been practiced for thousands of years, with origins in the Eastern philosophy of Buddhism (Kabat-Zinn, 2003). In early Buddhism, mindfulness existed in the core of the teaching of the Buddha. Mindfulness was considered as a remedy to delusion and as a power which contributed to the attainment of nirvana. Nirvana was a state of being overcoming/abandoning “dis-ease,” categorized as the three “poisons” of greed, hatred, and delusion in the mind. The historical practice of mindfulness meditation has been found all over the world (Trousselard, Steiler, Claverie, & Canini, 2014). Its practice can be traced back to 1500 BCE in Hinduism (yoga), to the 6th c. BCE in Daoism (qui gong), and to 535 BCE in Buddhism (focused breathing). Similar practices were also found in Christian, Muslim, and Jewish religions.
In 1979, Dr. Jon Kabat-Zinn founded the Mindfulness Based Stress Reduction (MBSR) Clinic at the University of Massachusetts Medical School (Kabat-Zinn, 1990). As many as 18,000 individuals have completed MBSR at this clinic for conditions, such as chronic pain, heart disease, anxiety, depression, and insomnia. Dr. Kabat-Zinn has brought the practice of mindfulness meditation to mainstream medicine. Research funded by the National Institutes of Health has suggested that mindfulness meditation reduces pain (Cherkin et al., 2016), high blood pressure (Brook et al., 2013), symptoms of irritable bowel syndrome (Gaylord et al., 2011), anxiety (Chen et al., 2012), depression (Goyal et al., 2014), and insomnia (Ong et al., 2014) and promotes smoking cessation (Brewer et al., 2011).
Spirituality is defined as an awareness of connections with all creation, an appreciation of presence and a purpose that includes a sense of meaning (“Section I: The Meaning and Practice of Spiritual Care,” 2016). Theoretically, mindfulness meditation can increase spirituality by freeing the individual from a narrow self-focus but taking part of a boarder interconnectedness of everyday activities, surrendering people, and the world (Kabat-Zinn, 1994). Empirically, mindfulness meditation training promoted daily spirituality in healthy, but mentally stressed adults (Greeson et al., 2011). Mindfulness meditation training was also found to significantly improve daily spirituality in health care employees (Geary & Rosenthal, 2011). More importantly, increases in daily spirituality after mindfulness meditation training supported the improved mental health as a result of greater mindfulness (Greeson et al., 2011). This means daily spirituality is a key mechanism by which mindfulness meditation training benefits mental health. Given the theoretical basis and empirical evidence, it is suggested that mindfulness meditation could provide spiritual healing by removing negative energy from stress.
Multiple studies have reported that mindfulness meditation training decreased stress in health care employees and military personnel. For example, Krasner and colleagues (2009) found that a group of physicians reported improvements in terms of burnout, depersonalization, personal accomplishment, empathy, physician belief of psychosocial care, mood disturbance, consciousness, and emotional stability after mindfulness meditation training. In a separate study, mindfulness meditation training was implemented in a primary care service which included physicians, nurse practitioners, and physician assistants in Family Medicine, Internal Medicine, and Pediatrics (Fortney, Luchterhand, Zakletskaia, Zgierska, & Rakel, 2013). The important findings in this study included greater depression and anxiety symptom relief after the training. Moreover, some other studies have found that mindfulness meditation training reduced physiological responses to stress among active-duty Marines preparing for deployment (Haase et al., 2016; Johnson et al., 2014). In active-duty Army volunteers, mindfulness meditation training improved attention performance during a high-demand interval of pre-deployment training (Jha et al., 2015). These results indicated that mindfulness meditation training could mitigate negative cognitive/emotional responses during stressful tasks.
The purpose of this worksite program was to explore the acceptability of a mindfulness meditation program, “Promoting Spiritual Healing by Stress Reduction Through Meditation” (Spiritual Meditation), among employees in a Southeastern VA hospital. Similar to other types of meditation (“Meditation: In Depth,” 2019), the Spiritual Meditation program in this project included four elements: a quiet location (a chapel), specific and easily performed activities (stretching, walking, and sitting), a focus of attention on breathing, and an open attitude (letting distractions come and go naturally without judging them). Chaplain residents in the VA offered the Spiritual Meditation program to VA employees. The program was a health-focused ministry as part of the Clinical Pastoral Education of the VA. Clinical Pastoral Education combines multicultural and interfaith training that uses real-life ministry experiences to gain competency in providing health-related ministry and pastoral care (“What Is Clinical Pastoral Education?” 2017).
Framework for Program Evaluation
The Center for Disease Control and Prevention Framework for Program Evaluation (CDC Framework) (“Framework for program evaluation in public health”; CDC, 1999) was used to guide this program evaluation. The CDC Framework defines a program evaluation as a systematic method to improve and account for a health-promotion program by involving effective procedures that are useful, feasible, ethical, and accurate. A program is defined as a public health action, such as employee health promotion. There are two elements in the program evaluation: a systematic method (six-step evaluation process used to evaluate the program value) and an effective procedure (four evaluation standards to maintain an effective program evaluation) (Figure 1). The program value is considered to have three aspects: quality (i.e., merit), cost-effectiveness (i.e., worth), and importance (i.e., significance). Using this framework as a guide, we aimed to evaluate the acceptability of the Spiritual Meditation program that promoted health among the VA employees. The acceptability was conceptualized as the level of acceptance of the Spiritual Meditation program that would meet the needs among the VA employees (i.e., the acceptance of quality of program value).
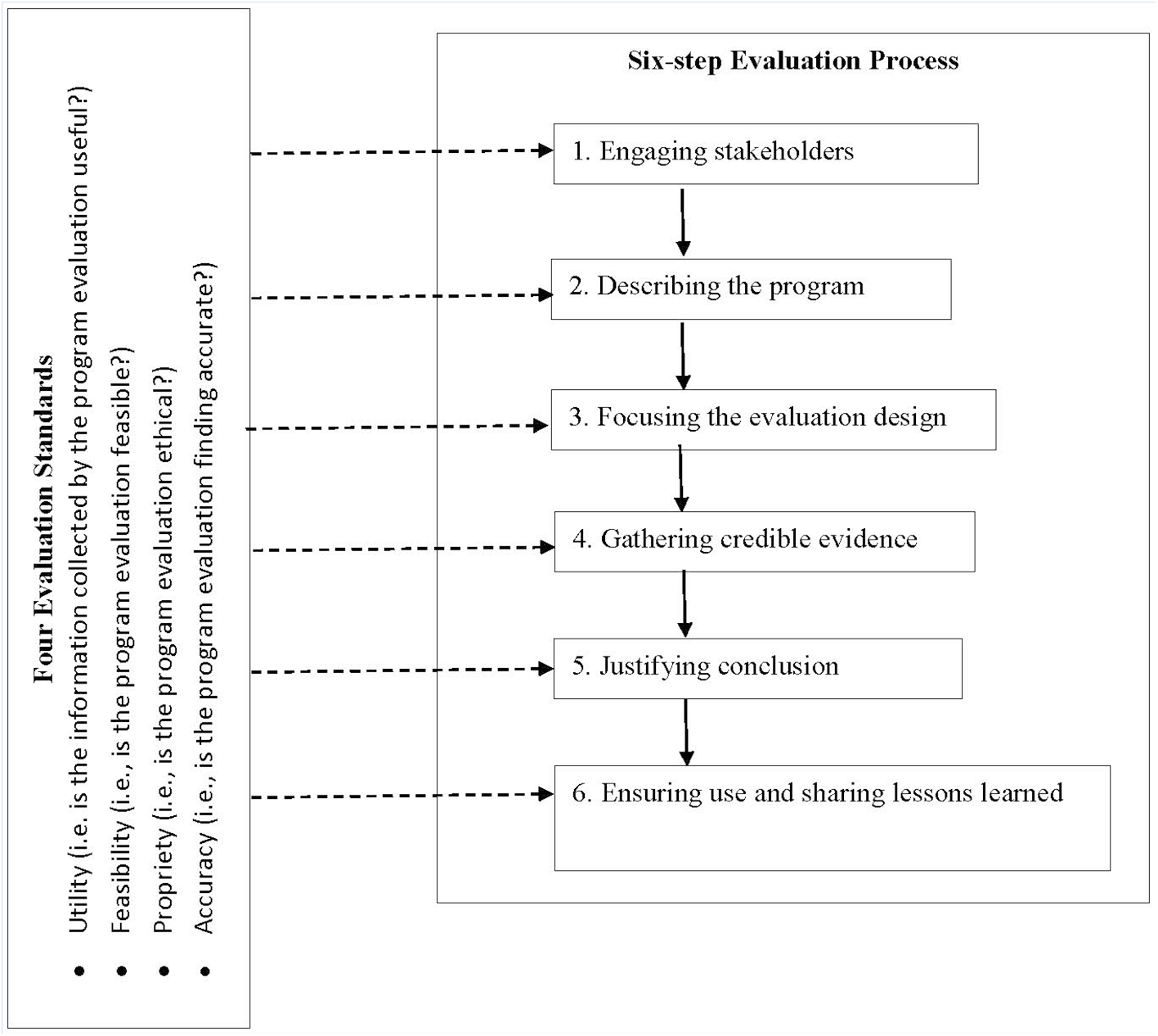
Framework of program evaluation.
Spiritual Meditation Program
The Spiritual Meditation program was designed based on the Handbook of Mindfulness Theory, Research, and Practice (Brown et al., 2016). This program focused on the spiritual aspect of mindfulness meditation. It connected body movement in the present moment with stress mitigation in a nonjudgmental way.
A cohort of chaplain residents of the VA Clinical Pastoral Education developed this program, and the Clinical Pastoral Education supervisor provided support and guidance. The program development, implementation, and program evaluation were a part of the Clinical Pastoral Education curriculum. It was considered to be a health-focused ministry for the employees. The goal for this program was to deliver a practical method for employees to connect mind, body, and spirit. The mission of the program was to help employees understand spiritually specific meditation and to take the techniques back to their areas of practice in the VA so they could better care for the veterans. A logic model to describe the sequence of service components of the Spiritual Meditation program for bringing about health promotion among VA employees and the infrastructure components to support the program operations is shown in Figure 2.
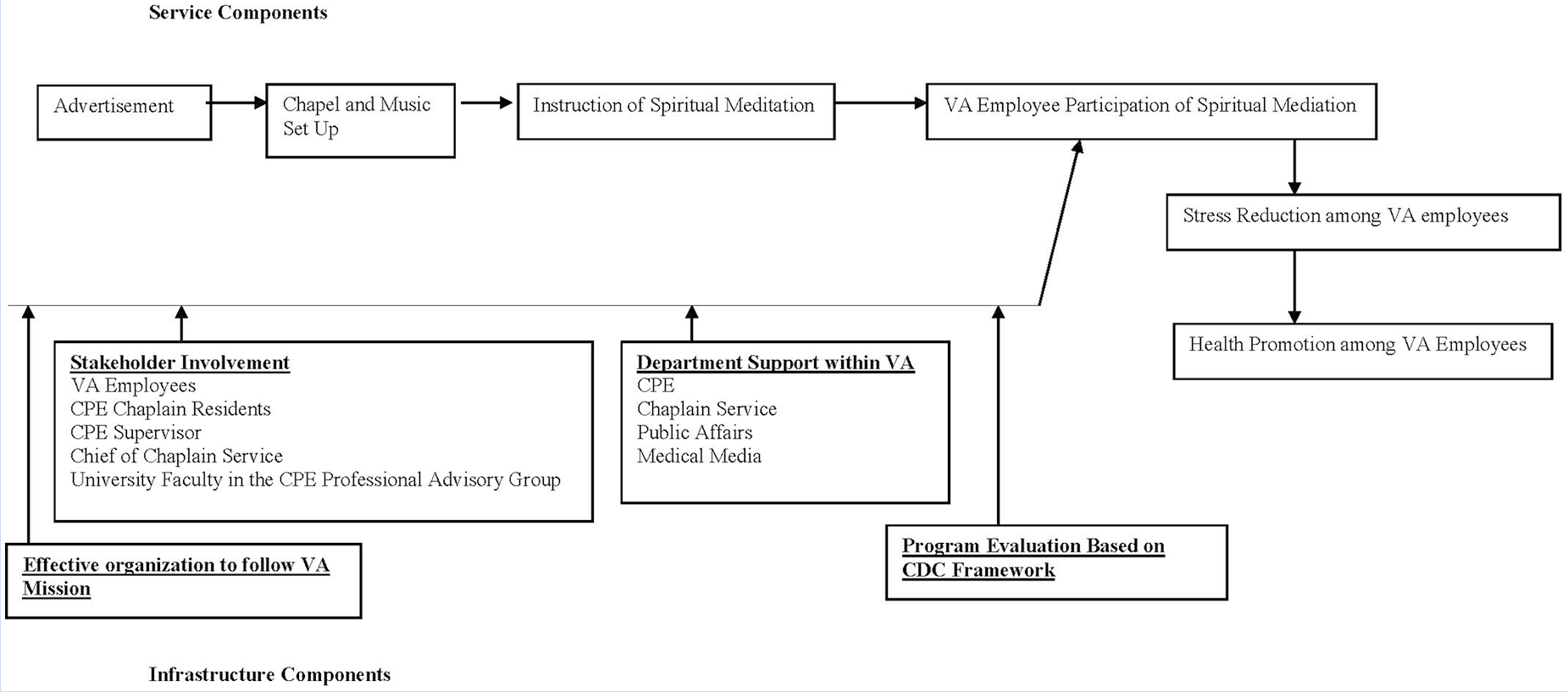
Spiritual Meditation Program Logic model.
Program Evaluation
The personnel who evaluated the Spiritual Meditation program included the chaplain residents, the Clinical Pastoral Education supervisor, and the chief of Chaplain Service in the VA where the program was implemented. A nursing faculty member, who is a member of Clinical Pastoral Education Professional Advisory Group, assisted with analyzing data, finding interpretations, and disseminating results. This VA is a tertiary care hospital classified as a Clinical Referral Level 1 Facility. At the time of this project, there were approximately 5,000 full- and part-time employees at this teaching and research hospital, which offered a full range of patient care services with state-of-the-art technology, along with education and research.
Participant Recruitment
Advertising was used to recruit interested employees for the Spiritual Meditation program (i.e., convenience sampling) which included health care providers (e.g., physicians, nurses, and therapists) and business/administrative staff. An in-house publication of the VA was the first venue where this was advertised. A written announcement was developed by the chaplain residents, edited by the Clinical Pastoral Education supervisor, and approved by the chief of Chaplain Services. The announcement was printed weekly in the VA in-house publication, which was distributed through the Public Affairs Director’s office. The announcement included the title of the program, the time, and the meeting place. The VA intercom system was utilized as the second venue for promoting the Spiritual Meditation program. The chaplain residents created a written announcement that was edited and approved, and then submitted to the Public Affairs Director’s office via email. The VA policy required the announcement be renewed every 12 weeks in the duration of the Spiritual Meditation program. A chaplain resident was tasked with the responsibility of ensuring that the announcements were made through the intercom system. Posters were used as the third approach. The chaplain residents first created a flyer that was approved and then placed it in strategic locations throughout the VA. Later, the chief of Chaplain Services recommended that the flyers be made into posters by the Medical Media department. These posters were then placed in existing display stands in the VA. The chief of Chaplain Services also directed the posters to be put up on Friday and removed on Tuesday after each Spiritual Meditation session.
Program Implementation
The Spiritual Meditation program began in 2016 and ended in 2018. The program was offered in the chapel of the VA. The interested employees could contact Clinical Pastoral Education or Chaplain Services if they had any questions before coming to the program sessions. The employees who were interested in the Spiritual Meditation program went to the session at the designated time and location voluntarily. Each weekly session was about an hour. The schedule of participation was not required to be routine. Employees could participate in one session, multiple sessions, consecutive sessions, or according to their availability.
Before each Spiritual Meditation program session, one of the chaplain residents announced the program through the intercom system in the VA. At the same time, the chapel was prepared for the Spiritual Meditation session by setting the ambient lighting, removing the kneeling prayer benches, closing the shutters, and playing quiet, soothing music. A bell was used to announce the beginning and ending of the session. A sign posted on the door to the chapel announced that the session was ongoing and that participants should enter quietly.
At the beginning of the session, participants were welcomed and the goal and mission of the Spiritual Meditation program was presented. There was also a reminder to participants to put their cell phones in vibrate mode and to practice Spiritual Meditation movements as they were able. The time flow was explained by saying that there would be a certain time period for spiritual stretching, spiritual walking, and spiritual sitting meditation movements. These movements were demonstrated by the chaplain residents. Each movement took 5 to 7 minutes and began with a brief introduction and explanation. Soothing music was played to help participants relax and release stress. Participants were reminded to continuously practice spiritual breathing along with each movement. Spiritual breathing is a way to focus breathing on the spiritual being as a human so that the mind, body, and spirit are connected.
The first movement was spiritual stretching. Participants breathed and stretched, beginning with the head, then progressively working down the body, as a way to release stress and tension and to energize the body. This movement allowed the mind to become more focused on subsequent movements. The second movement was spiritual walking, during which participants paced the room in the space available to them while focusing on breathing and walking. The time concluded with the third movement, spiritual sitting, along with spiritual breathing.
The Spiritual Meditation program session ended with a few minutes of conclusion that included an announcement of the next session. Participants were encouraged to practice the three Spiritual Meditation movements as part of their daily routine. Participants’ questions related to the Spiritual Meditation program were also answered at the end of the session.
Evaluation Survey
The program evaluation survey was based on the Handbook of Mindfulness Theory, Research, and Practice (Brown et al., 2016). There were five categories with 13 multiple-choice items. The responses were on levels of agreement from “strongly disagree,” “disagree,” “agree,” to “strongly agree.” There was one qualitative feedback question in the survey. Efforts were made to limit the participation burden as much as possible; therefore, each category had only three items, except for the last category, which had one item.
In the first category, “Personal Learning Experience,” there were three questions. These covered seeking spiritual healing in the program, fitting in spiritual healing in the program, and being willing to continue participation and invite other employees. In the second category, “The Spiritual Meditation Program Components,” there were three questions, which asked about the influence of spiritual healing, opportunities for individual experience, and opportunities to learn how to teach meditation to others. In the third category, “Quality of the Spiritual Meditation Teacher,” there were three questions rating the effectiveness of the teacher’s instruction, his or her understanding of meditation, and his or her response to questions. In the fourth category, “Time to Practice Spiritual Meditation During the Session,” there were three questions, which asked about spiritual stretching, spiritual walking, and spiritual sitting. In the fifth category, there was one question, which asked whether the chapel was an appropriate location for the Spiritual Meditation program. At the end of the survey, there was a column asking for participants’ testimony in response to the open-ended question (qualitative feedback): “How have you benefited from the Promoting Spiritual Healing by Stress Reduction Through Meditation program?”
Chaplain residents implemented the program evaluation by administering a one-time self-report survey over the first 4 weeks of the Spiritual Meditation program. Each participant completed one survey after his or her Spiritual Meditation session. The participants completed the survey using paper and pencil. The survey was filled out voluntarily and anonymously.
Data Analyses
For the quantitative data, the Likert-type scale responses were changed to dichotomous values (“disagree” vs. “agree”) for easier interpretation. Descriptive statistics were used to present these quantitative results. Frequency and percentage were calculated for each item. For the qualitative data, the testimonies (responses) to the open-ended question were analyzed by developing categories with the method proposed by Hsieh and Shannon (2005). The nursing faculty member conducted the qualitative data analysis. She began with reading all testimonies repeatedly to achieve immersion and obtain a sense of the whole. Next, testimonies were read word-by-word to derive codes by first highlighting the exact words from the text that appear to capture key thoughts or concepts. Notes were then made for the first impressions, thoughts, and initial analysis. As this process continued, codes emerged that were reflective of more than one key thought. These codes were then sorted into categories based on how different codes were related and linked. The final categories were determined by all authors, who cross-reviewed, discussed, and determined the findings.
Results
The survey was completed by 29 participants (Table 1). Over 80% agreed that they had a positive personal learning experience in the Spiritual Meditation program. More than 70% gave positive feedback about the Spiritual Meditation program components, and more than 95% agreed on the good quality of the Spiritual Meditation teacher. Only three participants (10.3%) did not have sufficient time for practicing the spiritual stretching and spiritual walking during the session. All participants (100%) thought the chapel was an appropriate place for the sessions.
Spiritual Meditation Program: Participants’ Acceptability Survey (N = 29)
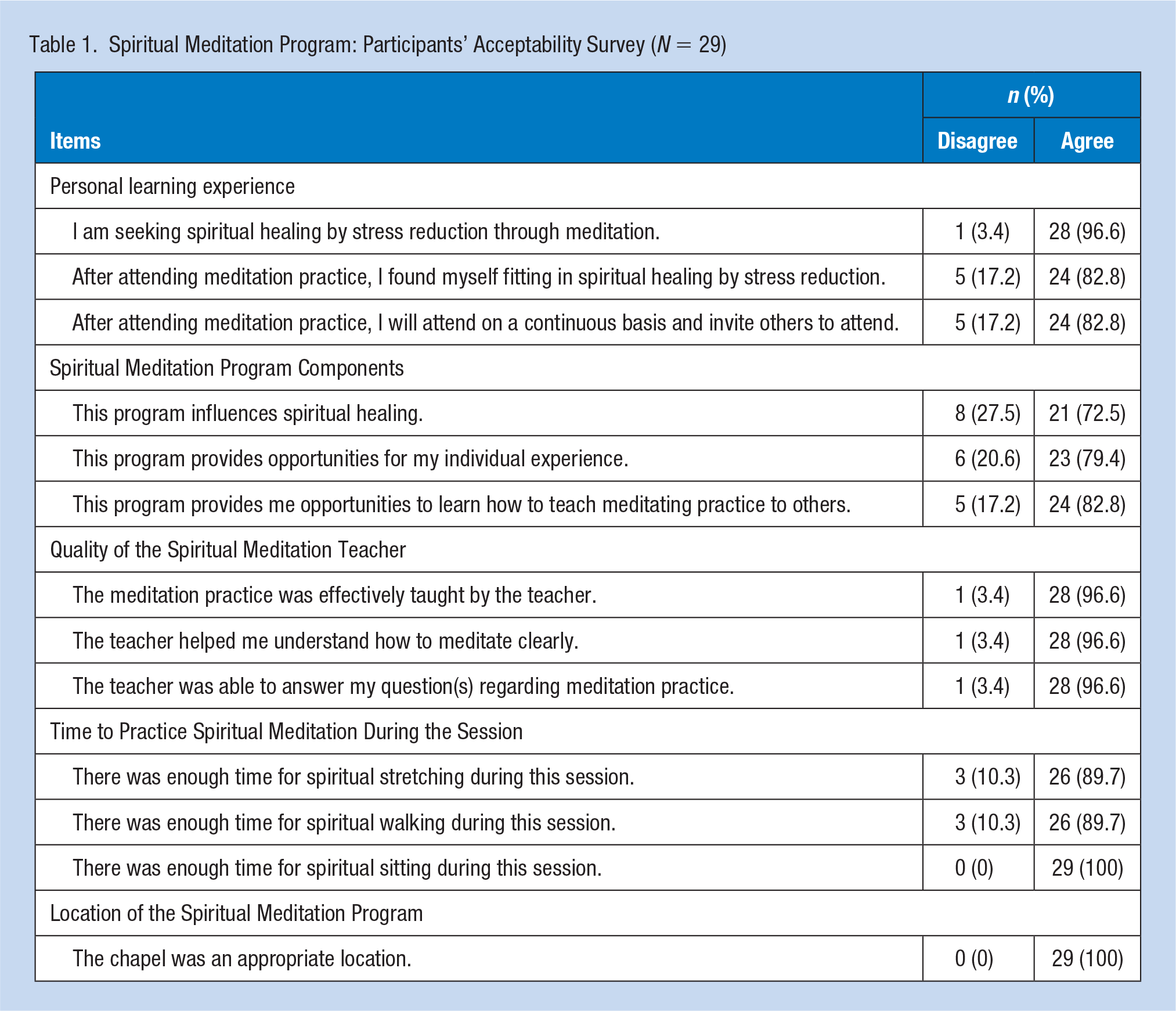
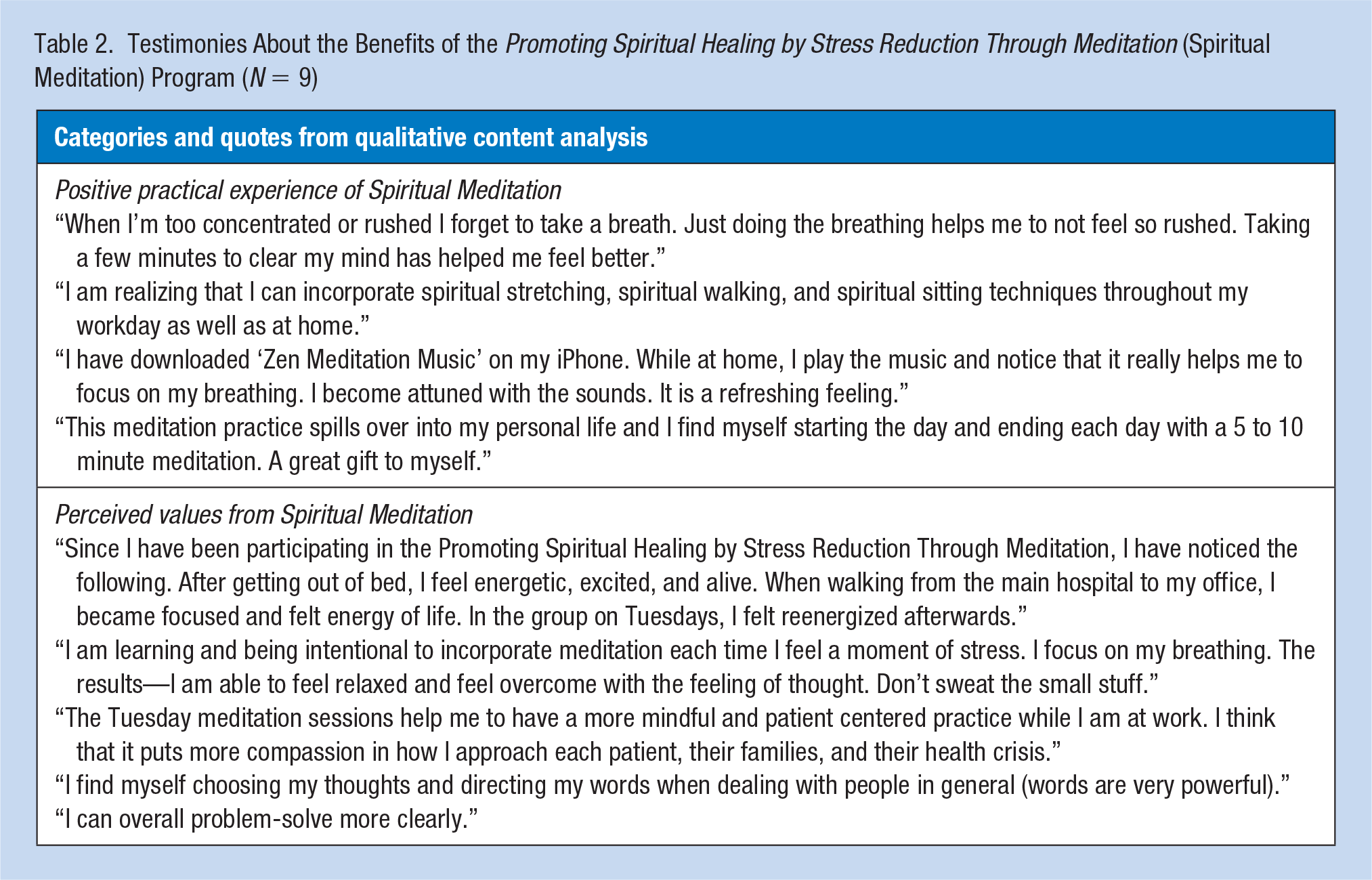
Table 2 shows the nine participants’ testimonies. There were two categories emerging from these responses: “positive practical experience of Spiritual Meditation” and “perceived values from Spiritual Meditation.” These responses both pointed to the positive outcomes of the program.
Testimonies About the Benefits of the Promoting Spiritual Healing by Stress Reduction Through Meditation (Spiritual Meditation) Program (N = 9)
Discussion
The Spiritual Meditation program was implemented by the chaplain residents as part of their Clinical Pastoral Education curriculum. The program was developed based on evidence from the literature that mindfulness meditation training led to improvement of well-being in health care employees and military personnel. The program aimed to meet the needs of VA employees who were working in a highly demanding environment. The components of the program focused on stress reduction through connecting mind, body, and spirit. The Spiritual Meditation program was an evidence-based and health-focused ministry.
A survey was given to determine the acceptability of the Spiritual Meditation program. The majority agreed that the program was a positive personal learning experience, that the program components were helpful, and that the quality of the teaching was good. However, some participants disagreed with two items related to spiritual healing: “fitting in spiritual healing” (17.2%) and “influences of spiritual healing” (27.5%). It is possible that spiritual healing was not clearly defined in the survey. Some (20.6%) did not agree that the program provided opportunities for individual experience; some (17.2%) did not want to continue, nor did they want to invite other employees; and some (17.2%) did not agree that the program guided them to teach meditation to others. These disagreements might be because participants had other resources to practice and learn meditation. They could gain similar benefits from other more flexible resources. Very few participants (10.3%) thought the time was insufficient for practicing spiritual stretching and spiritual walking. Generally, participants agreed that the time and place for the Spiritual Meditation program were appropriate.
In the testimony, participants first described their positive practical experience of Spiritual Meditation. They were able to use their breathing to connect the mind to the body during the practice, and they realized the need for self-care. They were able to apply the techniques they learned in their own daily lives and were able to feel more refreshed throughout their day. Second, participants also recognized perceived values from Spiritual Meditation in multiple ways in their personal and professional lives. They became reenergized and remained focused to confront the day’s possible stressors. In their assigned areas of duty, participants were able to problem-solve more effectively. They said that they became more patient-centric because they were more compassionate about the patients’ needs. After practicing the three spiritual movements, participants were more relaxed and better able to handle stressful situations.
The program evaluation concludes that the quality of the Spiritual Meditation program was accepted by the participating VA employees. The program might lead to improvement of health among those who practiced Spiritual Meditation routinely. Healthier employees would provide better care for patients in a health care institution. This is especially important because the employees in the VA take care of high-risk veteran populations who may experience post-traumatic stress disorders, traumatic brain injuries, and moral injuries (pathological violations of moral values). The Spiritual Meditation program could also be used in civilian health care facilities, as well as in the larger community. Health care providers who deliver care to patients in need of end-of-life care, palliative care, and mental health care may benefit most from this program. In the future, it will be necessary to develop evidence to support this program’s effectiveness in dealing with stress reduction and spiritual healing in health care employees. The weakness found in the program evaluation was an unclear definition of spiritual healing. To solve this, we explained to participants that a key of spiritual healing is to gain positive energy that can remove the negative energy resulting from stress (“Section I: The Meaning and Practice of Spiritual Care,” 2016). More specifically, we instructed participants to mentally focus on breathing and body motion with a clear mind-set when they engaged in spiritual movements.
Finally, because of its positive acceptance, the Spiritual Meditation program continued to be offered by chaplain residents in the VA until 2018. It should be noted that the development, implementation, and evaluation of the Spiritual Meditation program was part of the Clinical Pastoral Education curriculum in the VA. One study found that medical students who had mindfulness meditation training in their courses would be more likely to administer this training or recommend it to their patients than those who had not (McKenzie, Hassed, & Gear, 2012). The chaplain residents who were involved in the Spiritual Meditation program also expressed their willingness to use this approach to deliver spiritual care in a health care institution where they might serve in the future. They pointed out that Spiritual Meditation is also a great self-care remedy for themselves when they face the challenges of patient care.
Conclusion
There are several methodological limitations in this program evaluation. First, the psychometric quality of the survey should be improved and tested in the future. Second, the VA employees needed to spend their lunch break to participate in the Spiritual Meditation program. Due to the exploratory nature of this project and for the purpose of encouraging participation, Clinical Pastoral Education and Chaplain Services decided that participation was voluntary and that consistency in the number of sessions attended was not required. Thus, every participant might attend a different number of sessions. Participants were only required to complete the program evaluation survey once, over the first 4 weeks of the Spiritual Meditation program. This strategy limited the program evaluation, as it did not make possible the observation of the long-term health benefit of the Spiritual Meditation program. Third, the method of obtaining the qualitative data in this program evaluation was not rigorous and did not consider whether or not the data were saturated. The qualitative finding in this program evaluation was simply the answers to an open-ended question. Finally, the sample size was relatively small (N = 29), which limited the generalizability of data. This was due to limitations of time and resources. Therefore, the program evaluation was only conducted over the first 4 weeks of the Spiritual Meditation program. The short duration of the data collection phase led to a small sample size. A larger sample size with multiple data collection time points is suggested for future program evaluation.
In summary, the Spiritual Meditation program was designed for hospital staff caring for veterans and aimed at promoting stress reduction. The program evaluation was guided by the CDC Framework (“Framework for program evaluation in public health,” CDC, 1999). The results of program evaluation provide valuable information to general occupational health nurses caring for health care populations for which the care burden is a source of stress. It is important to develop a collaborative effort when a hospital-wide health-promotion program is created and implemented for employees in a health care system. Occupational health nurses and chaplains may collaborate to deliver the Spiritual Meditation program in a very efficient way.
Applying Research to Practice
A mindfulness meditation program, called “Promoting Spiritual Healing by Stress Reduction Through Meditation” (Spiritual Meditation) was found to be acceptable by employees in a VA hospital. Most health care employees face various sources of care burden. It is suggested that occupational health nurses routinely monitor the needs of employees at the health care setting with regard to stress reduction and the possible benefits of a meditation intervention or offering. Occupational health nurses are uniquely positioned to lead a Spiritual Meditation program, with the collaboration of chaplains or employee assistance program (EAP) personnel. These types of interventions promote better health for workers and improve the overall health of the work environment.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Robert C. Freeman, Jr. was the Clinical Pastoral Education Supervisor of James A. Haley Veterans’ Hospital and led the Spiritual Meditation project.
Niphon Sukuan, BA, MA, MDiv, NAVAC was a chaplain resident of James A. Haley Veterans’ Hospital and member of the Spiritual Meditation project. He co-led the Spiritual Meditation session.
Nicole M. Tota, BS, MDiv, CBF was a chaplain resident of James A. Haley Veterans’ Hospital and member of the Spiritual Meditation project. She provided administrative support for the project and co-led the Spiritual Meditation session.
S. Maria Bell, AS, BSN, MDiv, cNAVAC was a chaplain resident of James A. Haley Veterans’ Hospital and member of the Spiritual Meditation project. She managed the time schedule and provided Meditation Music during Spiritual Meditation sessions. She was also responsible for data collection for project evaluation.
Anthony G. Harris, BA, MDiv, NAVAC, CCC was a chaplain resident of James A. Haley Veterans’ Hospital and member of the Spiritual Meditation project. He was responsible for participant recruitment.
Hsiao-Lan Wang, PhD, RN, CMSRN, ACSM EP-C was an associate professor, University of South Florida College of Nursing, and a Professional Advisory Group member, Clinical Pastoral Education Program of James A. Haley Veterans’ Hospital. She led project dissemination.