
Abstract
Cardiovascular disease is a leading cause of mortality in the United States. This study examined the cardiovascular disease risk factors and health beliefs of workers for the purpose of developing a social network service (SNS)-based (e.g., Facebook and KakaoTalk) lifestyle-modification program for workers. Participants included 68 hospital workers (aged 25-60 years), with more than two metabolic syndrome or cardiovascular disease risk factors. Participants were randomly assigned to one of three groups: SNS intervention group (n = 23), education-only intervention group (n = 19), or nonintervention group (n = 26). Data were collected to compare changes in risk indicators according to the intervention method and time and analyzed using repeated-measures analyses of variance. Compared to the education and nonintervention groups, the SNS intervention group demonstrated significant improvements in waist circumference, body mass index, total cholesterol, low-density lipoprotein cholesterol, health promotion behaviors, and self-efficacy. This type of program has potential for allowing occupational health professionals to work with workers to improve lifestyle behaviors that promote health and reduce the risk of cardiovascular disease.
Keywords
Background
The health of workers is significantly influenced by their work environment, where they spend much of their time (Choi & Jeon, 2016). Cardiovascular disease is a leading cause of death in workers (Hwang & Park, 2016). With the advancement of industry and science, workers have been exposed to excessive workloads and stress (H. K. Lee & Yang, 2016). In addition, certain lifestyle habits, such as frequent alcohol consumption and lack of exercise, are associated with an increased risk of cardiovascular disease (Nea, Kearney, Livingstone, Pourshahidi, & Corish, 2015). This warrants the development of effective health-promotion programs that support healthy lifestyles and systematic intervention programs targeted at cardiovascular disease prevention strategies for high-risk individuals.
Various preventive intervention methods have demonstrated to be effective for managing risk factors of cardiovascular disease (Kunihiko, Shoemaker, Tom, & Robert, 2009; Look AHEAD Research Group, 2010; Oh et al., 2011; Oh et al., 2008; Son, 2008); however, most studies have focused on presenting comprehensive content on smoking, alcohol consumption, diet improvement, and exercise to the general public. As workers often face difficulties with the execution and maintenance of these methods, it is essential to develop strategies that encourage workers to continuously practice prevention, rather than simply educating them on certain risk factors and activities. Factors that prevent the successful implementation of these prevention methods in the workplace include noncooperation from the organization and lack of support from co-workers (Sorensen, Colditz, Klar, & Emmons, 2001). Workers are largely influenced by their subjective beliefs and surrounding environment; therefore, it is vital to provide opportunities for them to engage in activities that promote healthy behaviors in the workplace (Chang et al., 2005).
Mobile health is based on information and communication technology (ICT), in particular, wireless communication technology and wearable smart devices. The intersection of smartphones and medical devices has been gaining significant attention in recent years (Jang & Cho, 2016). Furthermore, personal mobile devices and social network services (SNSs) are becoming increasingly popular as community tools that facilitate communication and information exchange among people with various interests. An SNS is a platform for building social networks or social relations among people who share similar interests, activities, backgrounds, or real-life connections over the Internet (e.g., Facebook, KakaoTalk, and Naver Band). Specifically, the marketing and advertising industry is increasingly using SNSs due to their flexibility and broad reach. In the health care industry, the use of SNSs is also gradually increasing (Dang & Lee, 2012); however, there are very few studies on the use of SNSs within the industry. Thus, we sought to develop and evaluate the effectiveness of a SNS-based lifestyle-modification program for workers at risk of developing cardiovascular disease.
Methods
This study was approved by the Catholic Medical Center Institutional Review Board in Seoul, South Korea. The study consisted of two phases including a lifestyle improvement program development phase and the intervention phase, in which the researchers applied the health promotion intervention to a group of workers and compared them to a group of workers who received only educational information and a group that received no intervention.
The program was multidisciplinary and consisted of health administrators, doctors, and nutritionists. The basic structure included basic education and counseling, goal setting, regular doctor consultation, nutrition education, and SNS activities as a follow up.
Phase 1: Development and Implementation of an SNS-Based Lifestyle-Modification Program
We developed a 12-week SNS-based lifestyle-modification program that aimed to improve the lifestyle of workers with cardiovascular disease risk factors. The program intended to provide intervention activities to help participants recognize harmful lifestyles, understand the benefits of improvement and practice, and maintain these habits.
The program consisted of basic education, general counseling, goal setting, regular physical counseling, and education on nutritional management (program outlined in Table 1). This program was based on the Health Belief Model (Rosenstock, 1990). Its main concept was to improve health behavior by considering health beliefs and improving self-efficacy. The program’s content was structured to reduce perceived disability and increase perceived benefits and self-efficacy. These three factors have a major impact on health behavior enhancement (Jo, Kim, Lee, & Jeong, 2004). The SNS activities that we developed were based on these concepts (outlined in Table 2).
The Lifestyle Education Modification Program
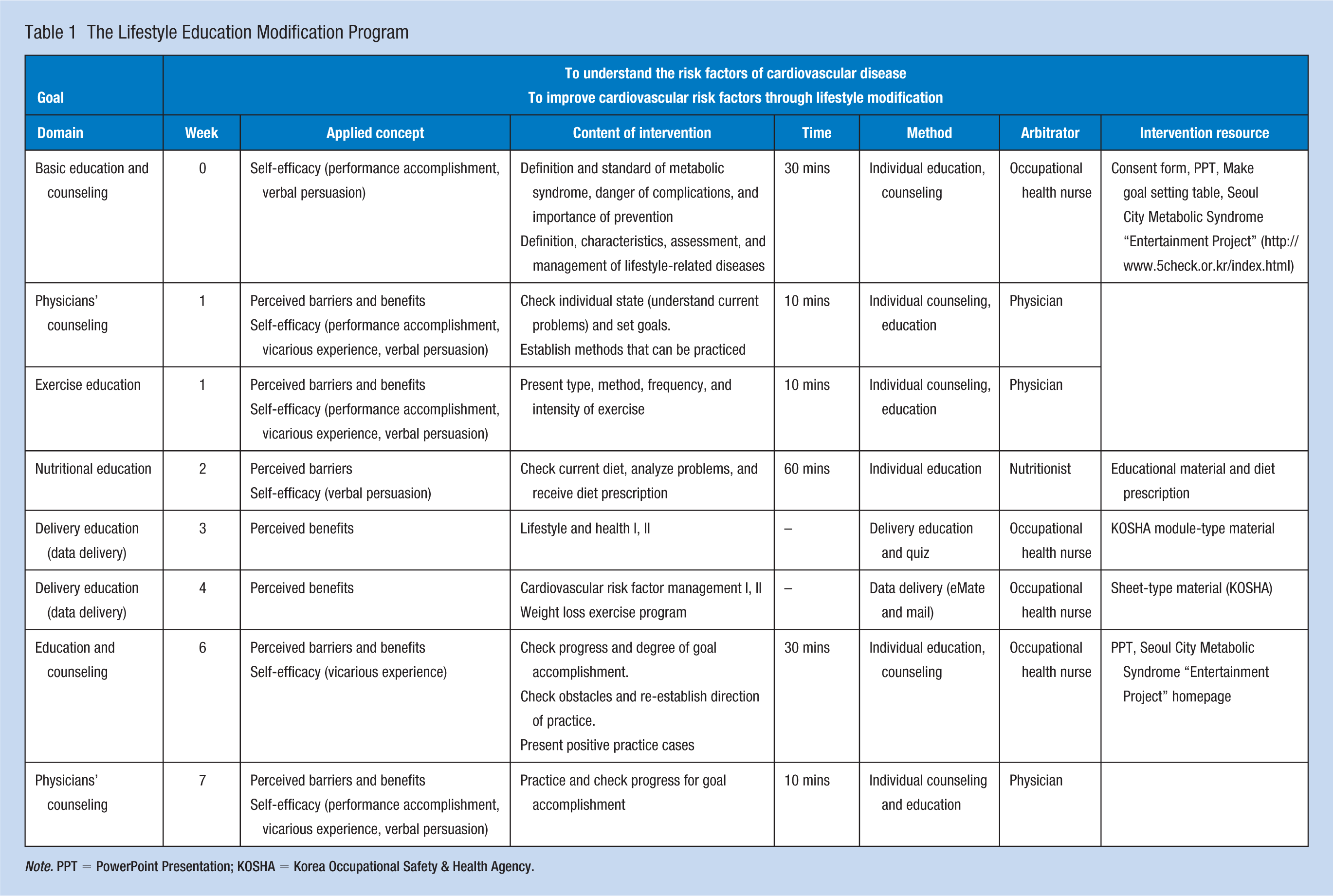
Note. PPT = PowerPoint Presentation; KOSHA = Korea Occupational Safety & Health Agency.
Final Lifestyle-Modification Program of Included SNS Activity
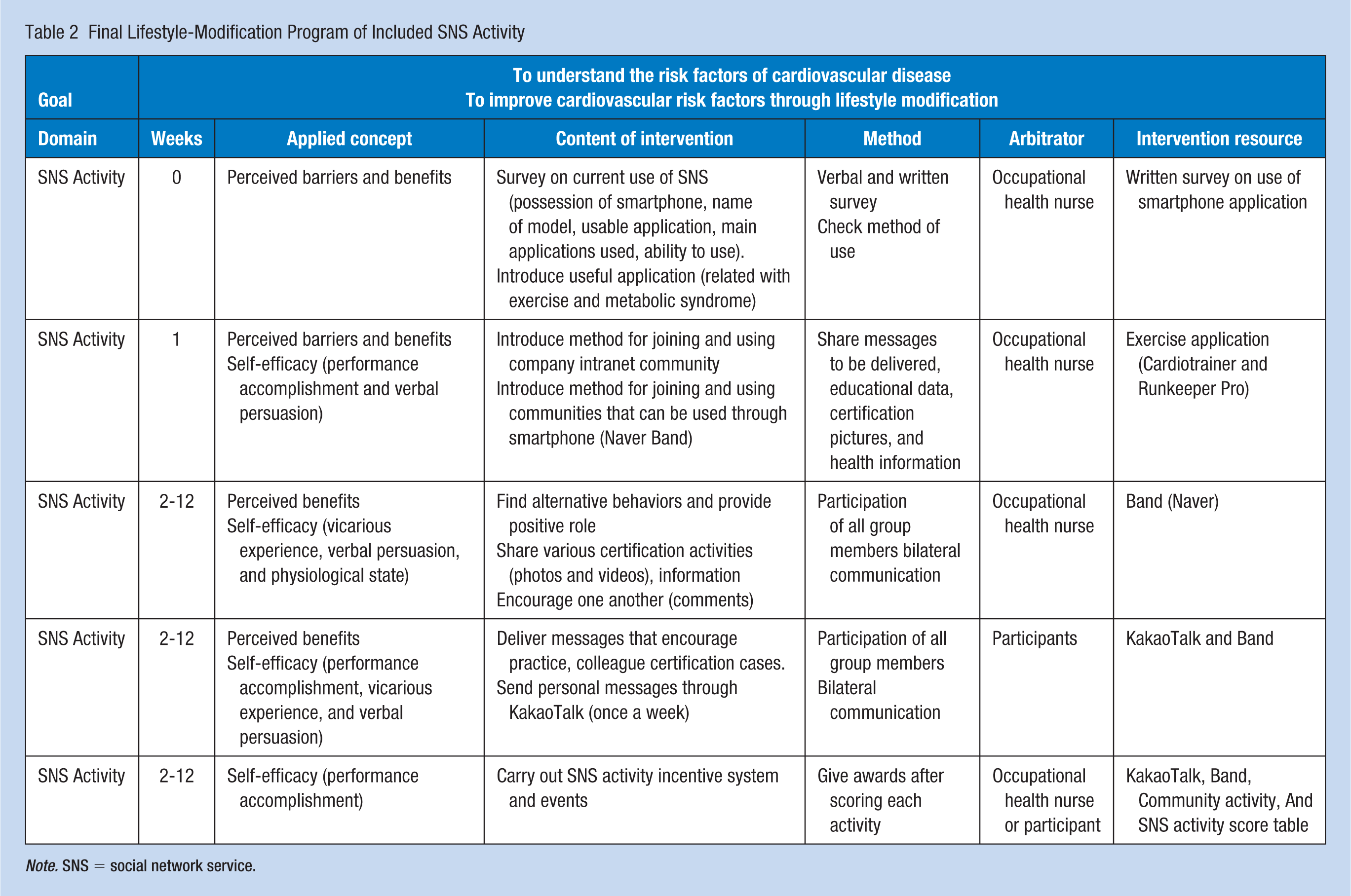
Note. SNS = social network service.
In order to enhance self-efficacy, performance accomplishment, vicarious experience, verbal persuasion, and physiological and emotional awakening were used as intervention strategies (Bandura, 1977). SNSs were used in various components of the program, such as setting individual goals, certifying achievement, exchanging feedback, and compensation (i.e., strengthening).
The methods of using SNSs, how to obtain community membership, and an introduction to and methods of using the SNS applications were included in the basic education component. Participants could freely communicate anytime through the SNS program KakaoTalk. This is a global mobile instant messenger service launched by Kakao Co, Ltd, on March 18, 2010. It is currently available as freeware for smartphone users. Participants could also simultaneously establish communities via company intranets (e.g., Healthy Workplace CMC Seoul, a health-related community created by health managers, where members share useful information, educational materials, and notices and recruit health care program participants) and engage in other SNS community activities, such as Naver Band, which is a closed-membership SNS launched by Naver, launched in August 2012 and operated by Camp Mobile, a subsidiary of Naver. Through SNSs, participants were expected to be able to easily access health-related information, become motivated, and certify their achievements anytime and anywhere.
The core of SNS-based continuous management was centered on the health beliefs of the workers and on boosting their self-efficacy to increase confidence and performance achievement for lifestyle changes based on easy access, voluntary participation, and maintenance. As the principal agents of the activity, participants served as positive role models for one another by exchanging experiences, opinions, and useful information and by sharing and encouraging improvement activities. To this end, the health administrator assumed the role of the facilitator, helping participants independently assess their areas for improvement and continuously practice health behaviors as community members. Community news were individually delivered to members. The criteria for an activity score was provided and notified to boost motivation and increase the use of the SNS. Activity scores were determined by the number of articles and pictures left by participants on the SNSs (Naver Band, KakaoTalk, and Intranet). Comments on the articles and pictures were given a 50% score. Incentives were given to reward individuals demonstrating outstanding activity performance. The authors provided café coupons to the three people who had the highest activity scores once a month.
Furthermore, apart from community activity, messages were sent to participants once a week through KakaoTalk or eMate ON (a solution that makes IBM Sametime functionality easier, enabling free and rapid communication within the organization through message forwarding, online meeting [chat room], file transmission, announcement forwarding function, etc., and thus supporting smooth collaboration within the organization) via the corporate intranet to encourage and maintain improvement activities. For 1 to 4 weeks, participants received messages based on the theoretical concepts of the health belief theory, such as “check your health condition,” “reflect on your life,” and “re-perceive information on lifestyle risks.” Furthermore, participants received messages that were sent to promote and maintain improvement activities (Tables 2 and 3).
Types of SNS Used in the Program
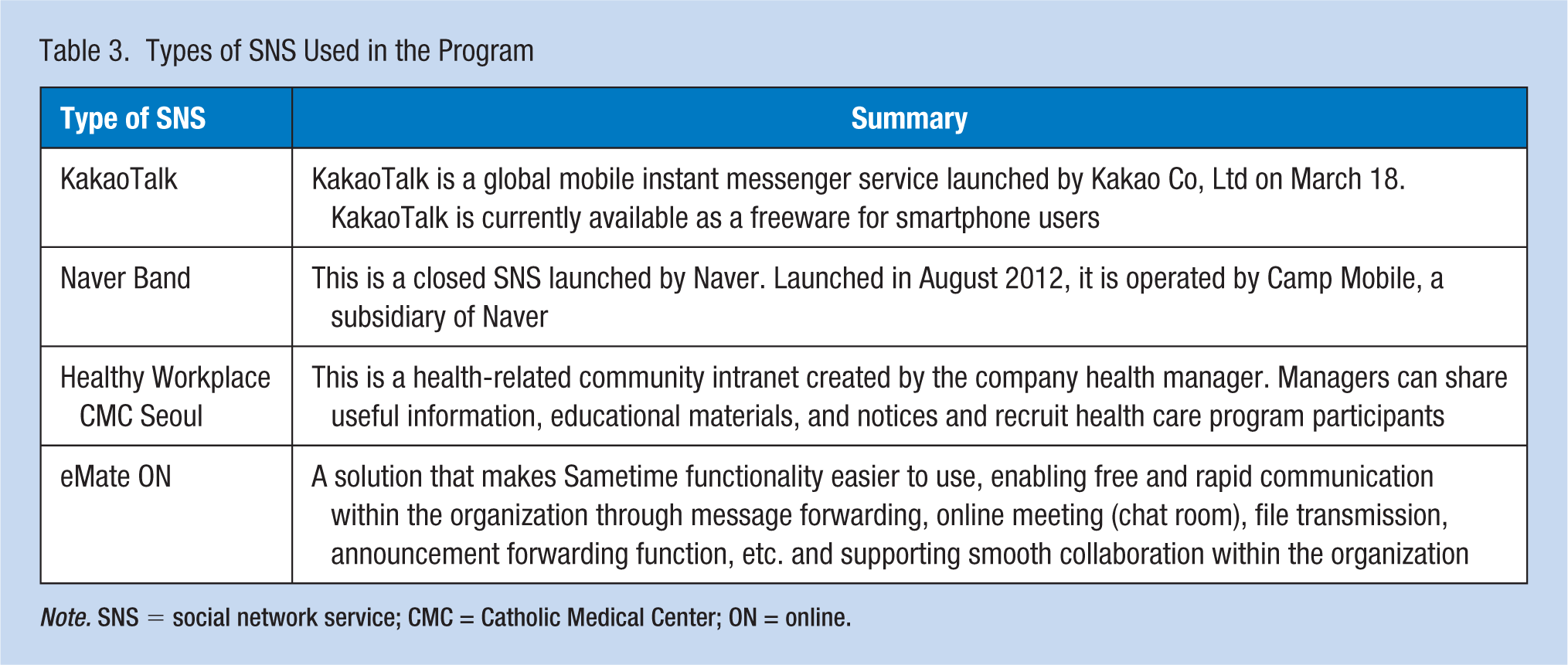
Note. SNS = social network service; CMC = Catholic Medical Center; ON = online.
Phase 2: Evaluation of the Intervention
The researchers, with the help of an occupational health nurse (OHN), recruited individuals aged 25 to 60 years who had more than two metabolic syndrome risk factors or risk factors for cardiovascular disease (e.g., body mass index [BMI], fasting blood sugar (FBS), abdominal circumference, low-density lipoprotein (LDL) cholesterol) via an information mail-out distributed to university hospital workers in Seoul, South Korea. Seventy participants met the selection criteria and consented to participate in the experiment. Participants directly selected envelopes containing random numbers and were assigned to groups according to the prepared random assignment table: the SNS intervention group (details in Tables 1-3) (n = 23), the education-only intervention group (details in Table 1) (n = 19), or the nonintervention group (n = 26). Sixty-eight participants were ultimately included in data analyses (two people left the experiment and were not included).
Measures
Data collection was performed at baseline (pretest) and at 6 and 12 weeks in all three groups. The measured variables were cardiovascular risk factors, health beliefs, health promotion behaviors, and self-efficacy.
Cardiovascular Risk Factors
Blood Pressure
Blood pressure was measured by the researcher using an automatic sphygmomanometer (TM-2655P, A&D, Japan). Before the blood pressure measurement, participants were asked to sit in a comfortable position and rest for at least 10 minutes.
Body Mass Index (BMI)
Participants’ BMI was measured by the researcher using a weight and height scale (GL-310) (G-Tech, Hong Kong). Participants were dressed lightly, without their shoes, and were asked to stand up straight. The BMI was calculated (body weight [kg]/height [m2]) and categorized as 25.0 kg/m² or more versus less than 25.0 kg/m².
Abdominal Circumference
Abdominal circumference was measured by the researcher using a tape measure. Participants were asked to stand with their feet 25 to 30 cm apart and breathe calmly while the underside of the ribs and the center part of the pelvic iliac crest were measured.
Blood Tests
Blood was drawn from participants after they had fasted for 8 hours the previous night. FBS was analyzed via the UV-Rate method (Hitachi 7600-210 DDP, Hitachi Co, Japan) using Hexokinase. Triglycerides (TG) and total cholesterol (TC) were analyzed via enzyme colorimetry (Hitachi 7600-210 DDP). High-density lipoprotein (HDL) cholesterol and LDL cholesterol were analyzed via the selective inhibition method (Hitachi 7600-210 DDP). The analysis was performed by the outpatient laboratory of the study hospital.
Health Beliefs (Perceived Barriers and Benefits)
A tool modified by Paek (2005) based on J. S. Moon’s (1990) Health Belief Measurement Tool for Adult Diseases was used; (Cronbach’s α for perceived barrier = 0.75, Cronbach’s α for perceived barrier = 0.91). Perceived barriers questions covered factors that impeded the conduct of health promotion activities during the past month (10 items; 4-point Likert-type scale), for example, “I think that I can’t do health promoting activities because of busy daily life.” Perceived benefits questions covered health promotion activities during the past month (11 items), for example, “I think that eating a healthy diet helps me to improve my or my family’s health.”
Health Promotion Behaviors
Health promotion behaviors were measured using a tool translated into Korean and modified for Koreans by Yun and Kim (1999). This scale was based on the Health Promoting Lifestyle Profile version II (HPLP-II), which was developed by Walker, Sechrist, and Pender (1995) by modifying the original HPLP (52 items, 4-point scale, Cronbach’s α = 0.91). Questions covered health maintenance and health promotion behaviors, for example, “I exercise intensely at least three times a week for 20 minutes or more.”
Self-Efficacy
Self-efficacy was measured using a scale developed by Sherer and Maddux (1982) for measuring self-efficacy in general situations (17 items, Likert-type 5-point scale, Cronbach’s k = 0.87). Questions covered participants’ confidence in their ability to manage demands in their normal situation (in daily life), for example, “I am confident that when I make a plan I can achieve.”
Statistical Analyses
We compared the cardiovascular risk factors among the three groups (SNS intervention group, education-only intervention group, and nonintervention group) across three time periods (pretest, 6 weeks, and 12 weeks) to evaluate the SNS-based lifestyle-modification program. Participants’ general characteristics and health-related characteristics were analyzed using descriptive statistics. The homogeneity of the three groups was analyzed using an analysis of variance (ANOVA), χ2-tests, and Fisher’s exact tests. The effect of the program was analyzed using a repeated-measures ANOVA to verify the differences between groups.
Results
Assessment of the SNS-Based Lifestyle-Modification Program
Sixty-eight workers participated in the study, including those randomized to the SNS intervention group (n = 23), the education-only intervention group (n = 19), and the nonintervention group (n = 26). The three groups did not demonstrate any significant differences at pretest in terms of general demographic characteristics (data not shown), cardiovascular risk factors (Table 4), health beliefs of perceived barriers and benefits, or health promotion behaviors (Table 5). However, the SNS intervention group demonstrated lower self-efficacy at baseline relative to the other two groups (p < .001).
Comparison of Changes in Cardiovascular Risk Factors Between the SNS, Education, and Nonintervention Groups Over Time (N = 68)
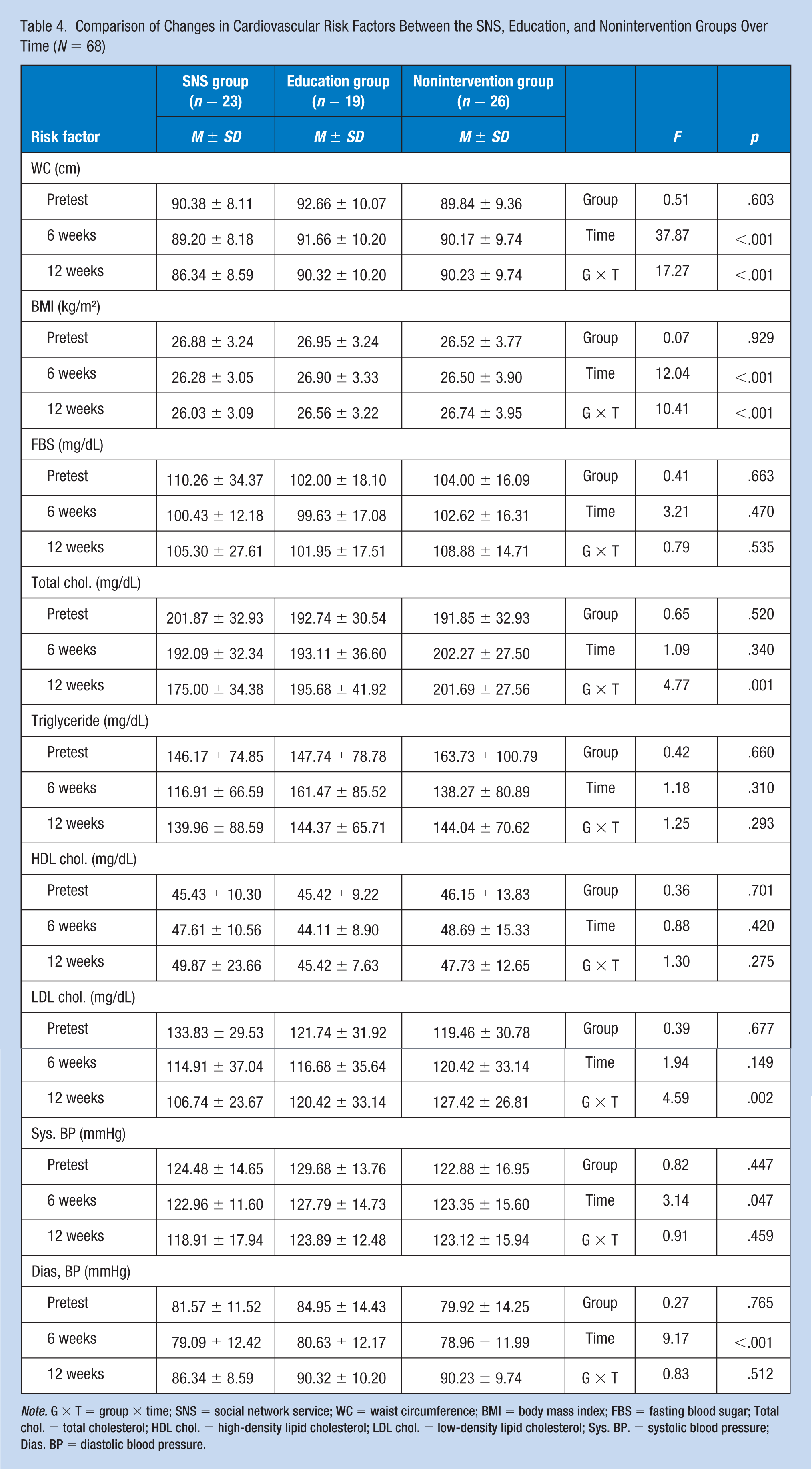
Note. G × T = group × time; SNS = social network service; WC = waist circumference; BMI = body mass index; FBS = fasting blood sugar; Total chol. = total cholesterol; HDL chol. = high-density lipid cholesterol; LDL chol. = low-density lipid cholesterol; Sys. BP. = systolic blood pressure; Dias. BP = diastolic blood pressure.
Comparison of Changes in Perceived Barriers and Benefits, Health Promotion Behaviors, and Self-Efficacy Between the SNS, Education, and Nonintervention Groups Over Time (N = 68)
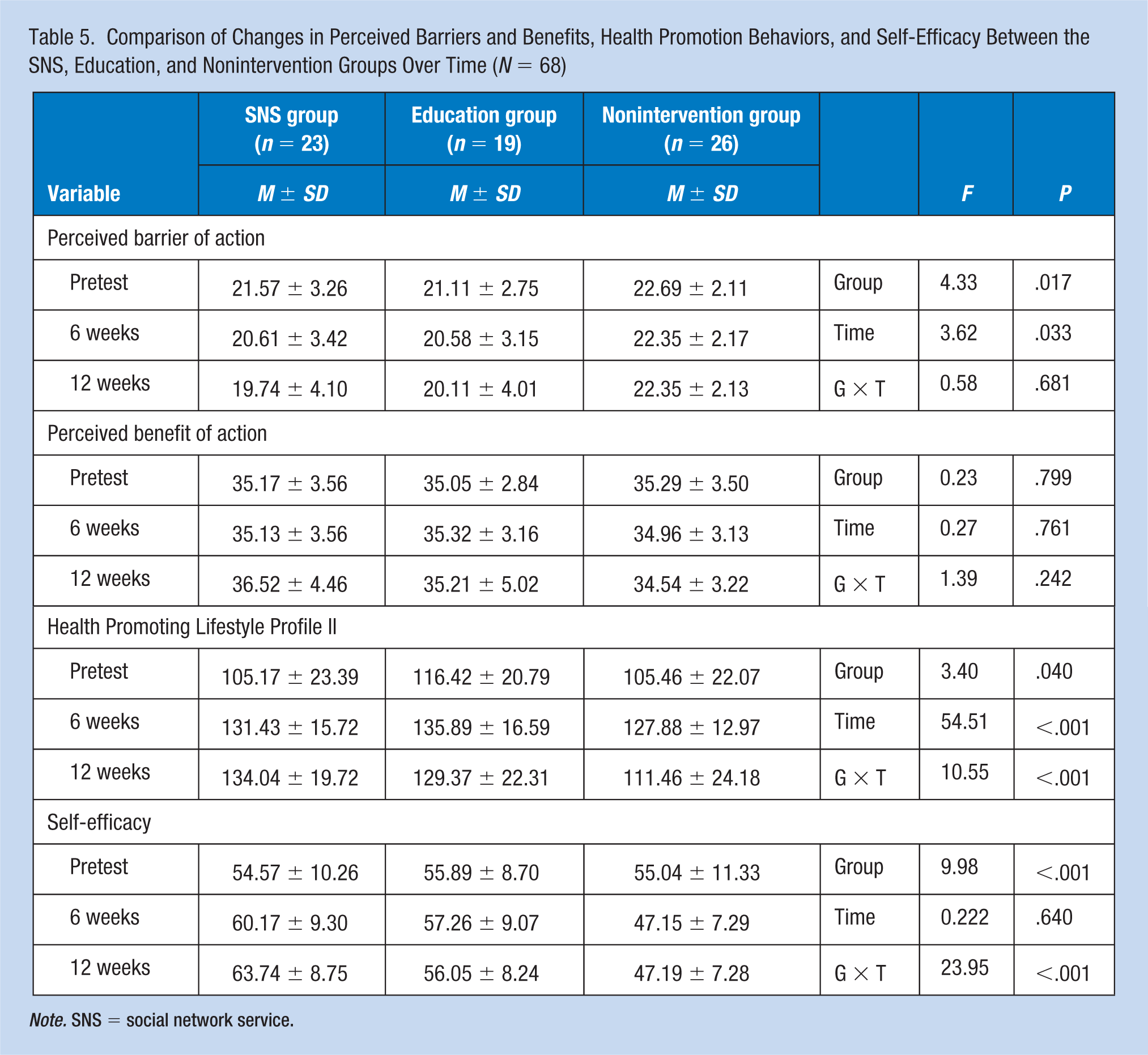
Note. SNS = social network service.
At the week-6 time point, the SNS intervention group demonstrated a significant decrease in abdominal circumference, BMI, TC, and LDL cholesterol. In addition, health promotion behaviors and self-efficacy improved in this group; however, these were not significantly higher than those of the other two groups. Regarding the program’s effects over time, the SNS intervention group demonstrated a significant difference in abdominal circumference, BMI, TC, LDL cholesterol, health promotion behaviors, and self-efficacy. In addition, participants’ health promotion behaviors improved to a greater degree in the SNS intervention group—which used the SNS-based lifestyle improvement program—compared to the education intervention or nonintervention groups (which did not use SNSs). Moreover, participants’ self-efficacy demonstrated greater improvement in the SNS intervention group than in the other two groups (Table 5).
Discussion
The rapid growth of the Internet has facilitated the use of less time- and space-consuming methods compared to previous web applications. SNSs are a key medium that can be effectively used for educational purposes. Therefore, the SNS-based lifestyle-modification program developed for the workers in this study is a method of treating workers based on their health belief theories to provide “clues of action,” which can stimulate interest and promote the maintenance of health promotion behavior.
The use of SNSs distinguishes this research from previous studies (Kang et al., 2010; Kunihiko et al., 2009; Magkos, Yannakoulia, Chan, & Mantzoros, 2009; Oh et al., 2008). SNSs differ from existing Web-based training programs in which they support communication among members and help them in building relationships through interaction. However, unlike with media such as intranets, this is based on the willingness and participation of users; thus, the authors need to analyze individual characteristics and cognitive factors. Therefore, this study investigated individuals’ ability to use SNSs and their variants. In addition, the authors provided criteria for measuring incentive grants and incentive activity points to increase the use of SNSs. In this study, motivational activities were conducted through information exchange and certification activities between participants based on SNS community activities. This study is significant because the program used mobile SNSs and an intranet community to separately allot time to each session and minimize the burden felt by participants in participating in educational activities.
Furthermore, individual messages were sent once a week to encourage and promote the health improvement activities of participants who participated less in SNS-based community activities. The message content was based on concepts related to health belief theories and changed based on the initial message and how the program progressed. The authors also found that individual differences existed according to the degree of SNS use because participants were not coerced or obligated to participate in the activities, although the workers that used SNSs had a high level of satisfaction and experienced little burden. Repetitive studies conducted in the future should consider strategies that can promote and maintain individuals’ participation in SNS activities. Furthermore, participation methods must be standardized and the level of participation must be measured to re-verify the effects of SNS use.
The authors developed a program that uses mobile-based SNSs that can be realized anywhere and anytime in a rapidly changing Internet environment to promote healthy activities and habits among workers. The authors attempted to minimize the burden of using SNSs by allotting separate times for education and triggered participants’ interest and motivation through mutual support and competition, to ultimately improve their lifestyles. The SNS-based lifestyle-modification program, which considers the time and convenience of workers, was effective in improving some cardiovascular risk factors. However, participants in the SNS intervention group demonstrated a slight, nonsignificant decrease in FBS. This result is similar to that in other studies focusing on face-to-face education (S. H. Kim, Ryu, Pyeon, Cha, & Park, 2014; M. S. Lee et al., 2008; Lundgren, Malcolm, Bink, & O’Neil, 2009; K. E. Moon et al., 2011). This finding stipulates the need to repeat this study with more participants. TG and HDL cholesterol did not demonstrate any significant changes. This is assumed to be the result of either increased insulin resistance from a high-carbohydrate diet, the influence of HDL-cholesterol adjustment, lack of continuous monitoring after diet education, seasonal factors, or increased amount of exercise with no dietary control (e.g., frequent corporate get-togethers). This observation also implies the need to increase the number of participants and repeat the study. In addition, it demonstrates the importance of strict dietary control and intake management.
For participants in the SNS intervention group, average LDL cholesterol levels were significantly reduced after 12 weeks of intervention, demonstrating reciprocal action between time and group. The final value was close to 100 mg/dL, which is the optimal number presented in the guidelines for treating adult diseases (National Cholesterol Education Program, 2002) by the National Heart, Lung, and Blood Institute of the United States. Thus, the program proved effective in reducing a well-known risk factor of cardiovascular disease.
No differences were observed between the groups regarding systolic or diastolic blood pressure. The pretest indicated that the blood pressure levels of the three groups were within the normal range and any subsequent changes were not clinically significant. The health promotion behaviors of the workers in the SNS intervention group demonstrated greater improvement than those of the education intervention group and the nonintervention group. This is similar to the results of a study that implemented an intervention with a small group-based education program using group dynamics (E. Y. Kim & Hwang, 2011) and one that evaluated online health education through personal e-mail using the company intranet (Kang et al., 2010).
Furthermore, the self-efficacy of the SNS intervention group significantly improved. This result supports the theory of J. H. Kim, Kwon, and Jung (2017), who stated that self-efficacy is a significant variable that influences the health promotion behaviors of middle-aged Koreans. In addition, this result corresponds with social learning theory, which states that self-efficacy is a key medium for synchronizing health promotion behaviors and that it indirectly influences implementation or behavioral maintenance. This study used SNSs to increase self-efficacy and motivate participants to practice their health promotion behaviors, such as climbing stairs, healthy diets and exercise, sharing useful and interesting information, conducting activities to encourage one another through KakaoTalk and the eMate ON chat server, posting comments for encouragement, providing incentives and rewarding SNS activities. These intervention activities were conducted to reflect self-efficacy resources, such as performance accomplishment and vicarious experience, and efficacy resources, such as verbal persuasion. This result suggests that health-related behaviors can be improved through SNS-based continuous management compared to previous educational methods, such as face-to-face education.
The three groups did not demonstrate different changes in perceived barriers or benefits over time. However, perceived barriers and benefits are variables that effectively explain health behaviors, and many of the participants were medical professionals (i.e., they possessed broad knowledge of diseases), which could, in turn, have influenced the perceived barriers and benefits. Alternatively, the result could be due to the small sample size. Thus, larger cohort studies should be conducted with workers from diverse fields and professions. This study demonstrated that an SNS-based lifestyle-modification program for workers can be applied at clinical sites. This program proved to be effective in improving some cardiovascular risk factors of workers at high risk of developing cardiovascular diseases and in enhancing their self-efficacy and health behaviors.
Conclusion
This study developed an SNS-based lifestyle improvement program for workers at high risk of developing cardiovascular disease. The multidisciplinary program consisted of basic education, professional counseling, nutritional education, individual exercise, and SNS activities (including the mobile community Band, KakaoTalk, a company intranet community, and a company messenger program), all facilitated and managed by health administrators, physicians, and nutritionists. The detailed content of the intervention was informed by health belief theory. In conclusion, the SNS-based lifestyle-modification program improved the self-efficacy and health behaviors of workers, which ultimately improved cardiovascular risk factors.
Applying Research to Practice
The SNS-based lifestyle-modification program developed in this study could be useful for OHNs in managing various health problems of workers because of its lack of restrictions in terms of time and space. This type of program also allows OHNs to obtain objective data for education and the development of various health promotion apps. A smart program can involve not only SNSs, but also setting and managing exercise goals through the measurement of physical activity, such as providing health information and exercise. Furthermore, occupational health intervention programs using various applications such as stress level measurement can be applied. Using these methods, both OHNs and workers could jointly improve the health of their workplaces, as well as coordinate with each other for sustained and effective lifestyle management.
Footnotes
Acknowledgements
This study was a doctoral dissertation and was not supported by grants.
Ethical approval
This study has been reviewed by the Research Ethics Committee of Catholic University in Korea and has confirmed that it meets ethical guidelines, including adherence to the legal requirements of the study country.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research,authorship, and/or publication of this article.
Author Biographies
Soo Hee Woo obtained a master’s degree and PhD in nursing from Yonsei University. Her research interests include cardiovascular and metabolic syndrome prevention and heart rate variability.
Eui Geum Oh obtained a master’s degree in nursing from Yonsei University and a PhD from the University of Illinois at Chicago. She is now an Institutional Review Board (IRB) Chairman at Yonsei University Medical Center and Educational Director of Korean Society of Nursing Science. She is also an American Academy of Nursing Fellow and ICN Evidence–based practice adviser. Her research interests include chronic pulmonary disease and pulmonary rehabilitation, Emergency/Chronic Illness Symptom Management and Quality of Life, Evidence-based Health care, Community Participatory Research: Metabolic Syndrome, Osteoporosis Management Redevelopment during Nursing Research, and development of nursing service (R & D).
Kyung-SOO Kim obtained his master’s degree and PhD from the Catholic University of Korea. Currently, he is the director of the Department of Family Medicine and the Director of the Clinical Research Support Center at the St. Mary’s Hospital, Catholic University Hospital. Areas of interest include obesity, metabolic imbalance, and geriatric disease.
Sang Hui Chu received her doctorate in medicine from Yonsei University. Her research interests include clinical trials, cardiovascular disease, and pharmacology.
Gwang Suk Kim earned her master’s degree and doctor’s degree in nursing from Yonsei University. Research interests include worker health care, stress, and health.
Chung Mo Nam obtained his master’s degree and doctoral degree in computational statistics from Seoul National University. He is currently a professor at the Department of Preventive Medicine, Yonsei University College of Medicine. His research interests are health statistics, survival analysis, clinical trials, and genetic statistics.