
Abstract
Atherosclerosis develops over a long period of time and often begins in childhood. The goal of this study was to make a cross-sectional assessment of the pattern of cardiovascular disease risk factors among Australian vegetarian (n = 49) and nonvegetarian (n = 639) 14- to 17-year-old participants from New South Wales, Australia. Vegetarians had statistically significant lower mean total (4.05 vs 4.4 mmol/L;P < .001) and low-density lipoprotein (LDL) cholesterol (2.18 vs 2.55 mmol/L; P < .001) and lower incidence of abnormal total and LDL cholesterol (31.1% vs 46.2%, P = .036, having total cholesterol ≥4.4 mmol/L and 13.3% vs 29.6%, P = .021, having LDL cholesterol ≥2.84 mmol/L). Vegetarians had a higher diastolic BP (72.0 vs 69.7 mm Hg; P = .038). No statistically significant difference was found in other risk factors including high-density lipoprotein cholesterol (P = .83), triglycerides (P = .601), systolic blood pressure (P = .727), body mass index (P = .159), plasma glucose (P = .09), C-reactive protein (P = .527), or homocysteine (P = .45). The prevalence rate with 3 or more risk factors was 12.2% among vegetarians and 13.9% among nonvegetarians (P = .156). The high percentage of abnormal total cholesterol in both diet groups and, in addition, LDL cholesterol in nonvegetarians is a cause of concern and underlines the need for lifestyle change.
‘Cardiovascular disease (CVD) is the leading cause of mortality worldwide, causing more than 17 million deaths annually, which account for 31% of all mortalities . . .’
Cardiovascular disease (CVD) is the leading cause of mortality worldwide, causing more than 17 million deaths annually, which account for 31% of all mortalities (32% among women and 27% among men).1,2 In Australia, ischemic heart disease and cerebrovascular disease constitute the first and the third leading causes of mortality, respectively. 3 According to findings from the INTERHEART case-control study with 15 152 cases and 14 820 controls from 52 countries, modifiable risk factors, including smoking, blood lipids, blood pressure/hypertension, blood glucose/diabetes, abdominal obesity, intake of fruits and vegetables, physical activity, and alcohol consumption, account for about 90% of the population-attributable risk for myocardial infarction. 4
Vegetarian diets are devoid of all flesh foods, but may include eggs (ovo-vegetarian), milk and dairy products (lacto-vegetarian [LV]), or eggs, milk, and dairy (lacto-ovo-vegetarian [LOV]). A vegan diet (VD) does not contain meat, fish, or poultry and does not contain any products of animal origin (milk, dairy, or eggs). Studies with adults have shown that vegetarian diets improve several modifiable risk factors for CVD, including serum lipid profile, serum glucose concentration, and systolic and diastolic blood pressure (BP).5-9 These diets have also been associated with lower incidence of overweight and obesity. 6 Fewer vegetarians smoke or abuse alcohol, and they eat more fruits and vegetables compared with nonvegetarians.10-12 Additionally, recent findings have shown that vegetarian diets improve some nontraditional risk factors for CVD, including markers of inflammation, such as C-reactive protein, reduce oxidative stress, and protect against plaque formation.13,14
Although CVD may not be manifested until mid-adulthood, atherosclerosis develops over a long period of time and often begins in childhood. 15 Stary reported 65% of 12- to 14-year-old adolescents having foam cells along with lipid droplets in their arteries, and an additional 8% had atherosclerosis that advanced to pre-atheroma or atheroma stages. 16 Findings from the Bogalusa Heart Study showed that 50% of children and adolescents between 2 and 15 years old had fatty streaks and 8% of participants in this age group had fibrous plaques. 17
The presence of CVD risk factors mentioned earlier contributes not only to the development of atherosclerosis but also may influence disease progression among individuals who have already developed atherosclerosis. It has been suggested that the presence of multiple risk factors accelerates atherosclerosis and that a cluster of risk factors that is present during childhood persists into adulthood. 17 For example, in the Bogalusa Heart Study, the extent of atherosclerosis in the coronary arteries was markedly increased among individuals with multiple risk factors. 17 Thus, for the best results in terms of CVD prevention, it is prudent to study the patterns of occurrence of CVD risk factors among youth in order to design interventions to improve their profile and, thus, reduce their detrimental impact. The goal of our study was to assess the pattern of CVD risk factors among Australian adolescents who adhered to either a vegetarian or nonvegetarian diet pattern. The objectives were to (1) evaluate whether there were any statistically significant differences between the mean values of assessed CVD risk factors among adolescents in the 2 diet groups, (2) assess the prevalence of individuals in each diet group with abnormal values for each specific risk factor, and (3) assess the prevalence of participants with a cluster of risk factors.
Materials and Methods
The study protocol was approved by the Sydney Adventist Hospital Human Research Ethics Committee. We have done a cross-sectional analysis to estimate differences in CVD risk factors among 49 vegetarian and 639 nonvegetarian, 14- to 17-year-old, participants. Table 1 contains demographic information of study participants. Specifically, we compared the total and low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides (TAG), systolic and diastolic BP, plasma glucose, and body mass index (BMI). Additionally, we assessed differences between C-reactive protein (CRP) and homocysteine (Hcy) concentrations. Criteria for normal/abnormal cutoff values are listed in Table 2.
Demographic Characteristics of Participants.
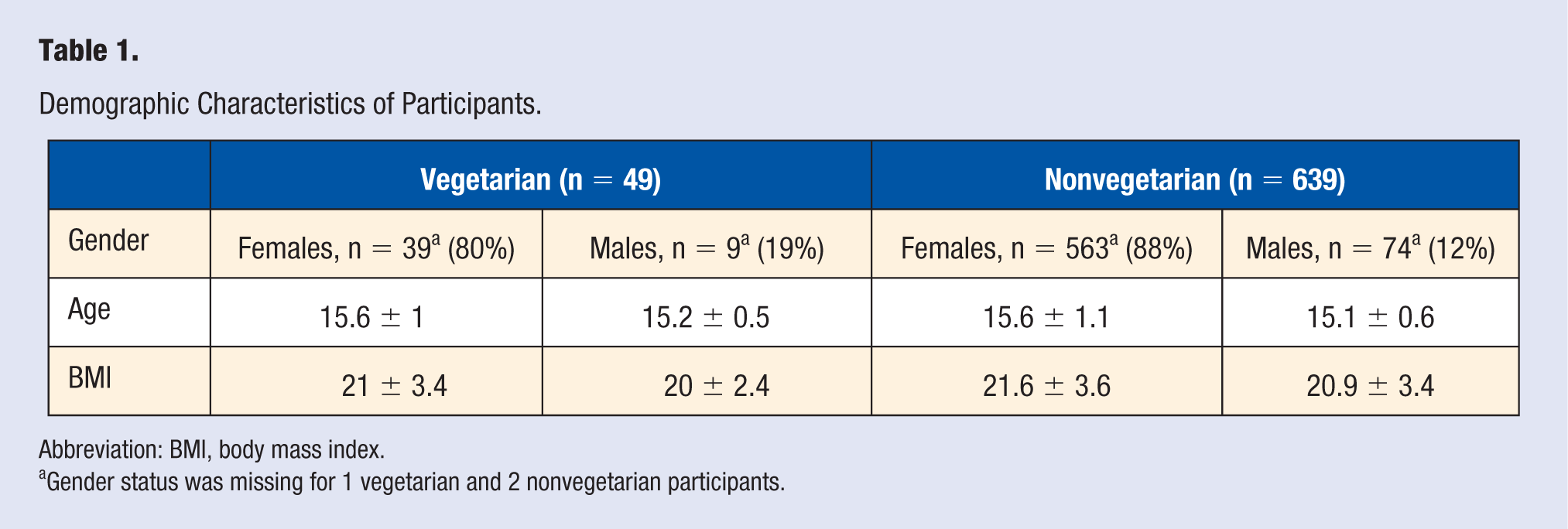
Abbreviation: BMI, body mass index.
Gender status was missing for 1 vegetarian and 2 nonvegetarian participants.
Cutoff Criteria for Abnormal Values for Heart Disease Risk Factors.
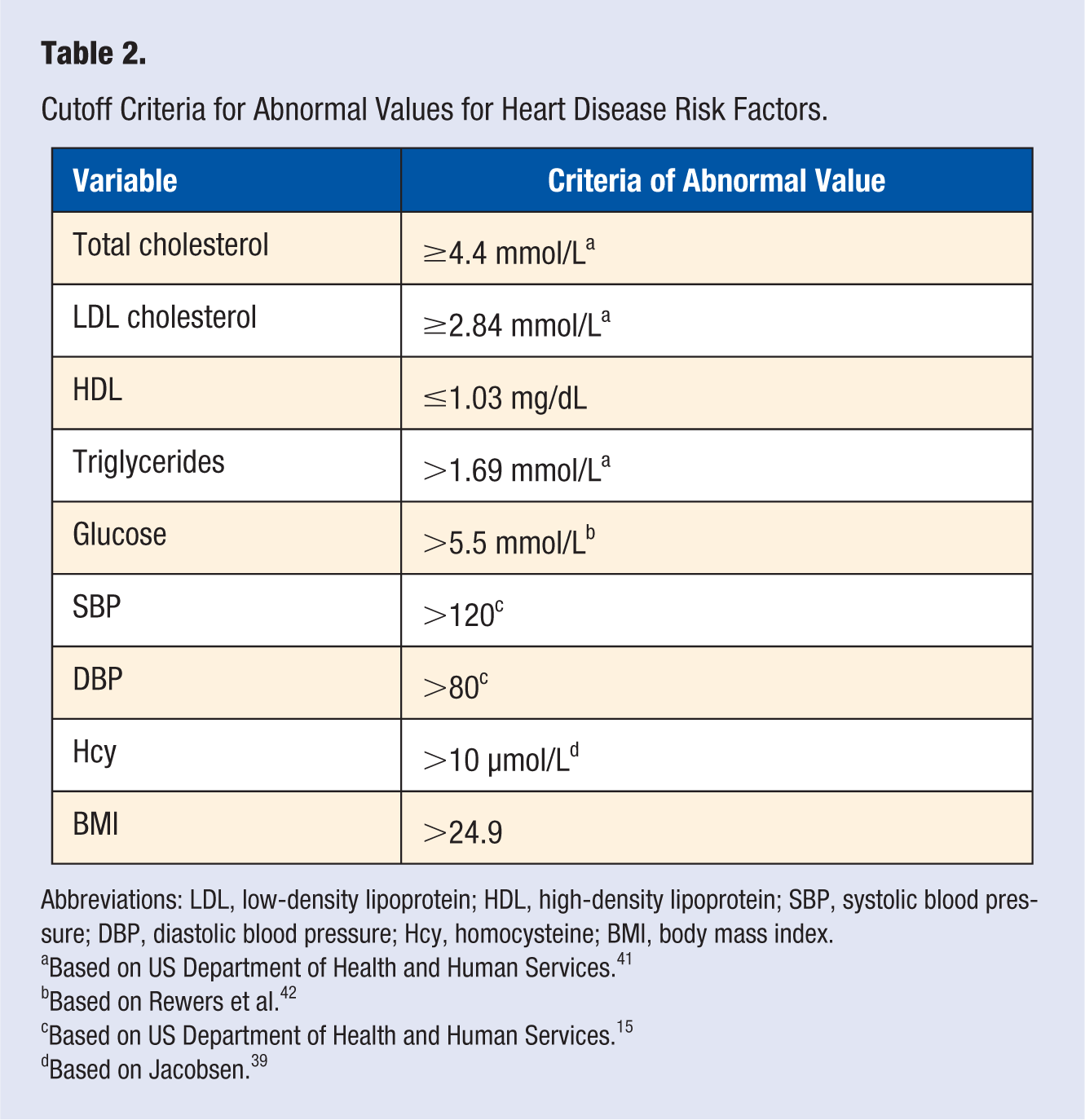
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure; Hcy, homocysteine; BMI, body mass index.
Based on US Department of Health and Human Services. 41
Based on Rewers et al. 42
Based on US Department of Health and Human Services. 15
Based on Jacobsen. 39
Vegetarian Diet
Participants who consumed any amount of meat, poultry, or fish were classified as nonvegetarians though they may have used milk, dairy, and eggs. Considering there were only 49 vegetarians, all of them, regardless of the type, were grouped in the same category.
Recruitment and Data Collection
The analysis is based on combined datasets from 2 previous studies: the Sydney Newcastle Adventist Schools Teen Physical Activity and Nutrition Study and the Healthy under the Skin You’re In study. Detailed description of recruitment has been described previously.18,19 Participants were recruited from public and private secondary schools in the Sydney, Central Coast, and Hunter regions of New South Wales, Australia. Parental consent and participants assent was obtained.
Blood Samples Collection and Analysis
Following an overnight, ~12 hour fast, 5 to 10 mL of blood was drawn by normal venipuncture. Serum samples for biochemical analyses were stored at −80°C until analysis. All assays were performed by the Pathology Department at the Sydney Adventist Hospital using routine methods.
Blood Pressure Assessment Procedure
BP measurements were measured on the same day as blood collection. Participants were asked to wait at least 5 minutes before BP was measured. The measurement was done on the right arm. At least 2 measurements were taken. If the difference between the readings was 5% or more the participant was asked to rest for an additional 3 to 5 minutes before a third reading was taken. BP readings were taken using an Omron (SEM-2) automatic BP monitor. The health care professionals who assisted in BP measurements were blind to the dietary classification of each participant.
Anthropometric Assessments
BMI was calculated from the following formula: weight/height (m2). Participants’ weight was measured using the Tanita body composition analyzer (BC-420MA) and their height was assessed using a calibrated height stick.
Analyses
Assessment of means and standard deviations of the blood lipids, glucose, BP, Hcy, and CRP were performed. T-test analysis was performed to assess whether any differences in the mean values for each of the risk factors was statistically significant. In addition, prevalence of participants that did not meet the recommended guidelines for each of the risk factors was assessed. The resulting 2 by 2 table for comparing prevalence was analyzed using Fisher’s exact test. Data analysis was performed with the statistical software R, version 3.4.2. 20 Significance was set at P < .05.
Results
Assessment of CVD Risk Factors by Diet Group
Vegetarians had statistically significant lower mean total (4.05 vs 4.4 mmol/L;P < .001) and LDL cholesterol (2.18 vs 2.55 mmol/L; P < .001) and higher diastolic BP (72.0 vs 69.7 mm Hg; P = .038). No statistically significant difference was found in other risk factors including HDL cholesterol (P = .83), TAG (P = .601), systolic BP (P = .727), BMI (P = .159), plasma glucose (P = .09), CRP (P = .527), or homocysteine (P = .45). The means and median for each CVD risk factor are shown in Table 3.
Mean, Standard Deviation, and Median Values for Heart Disease Risk Factors.
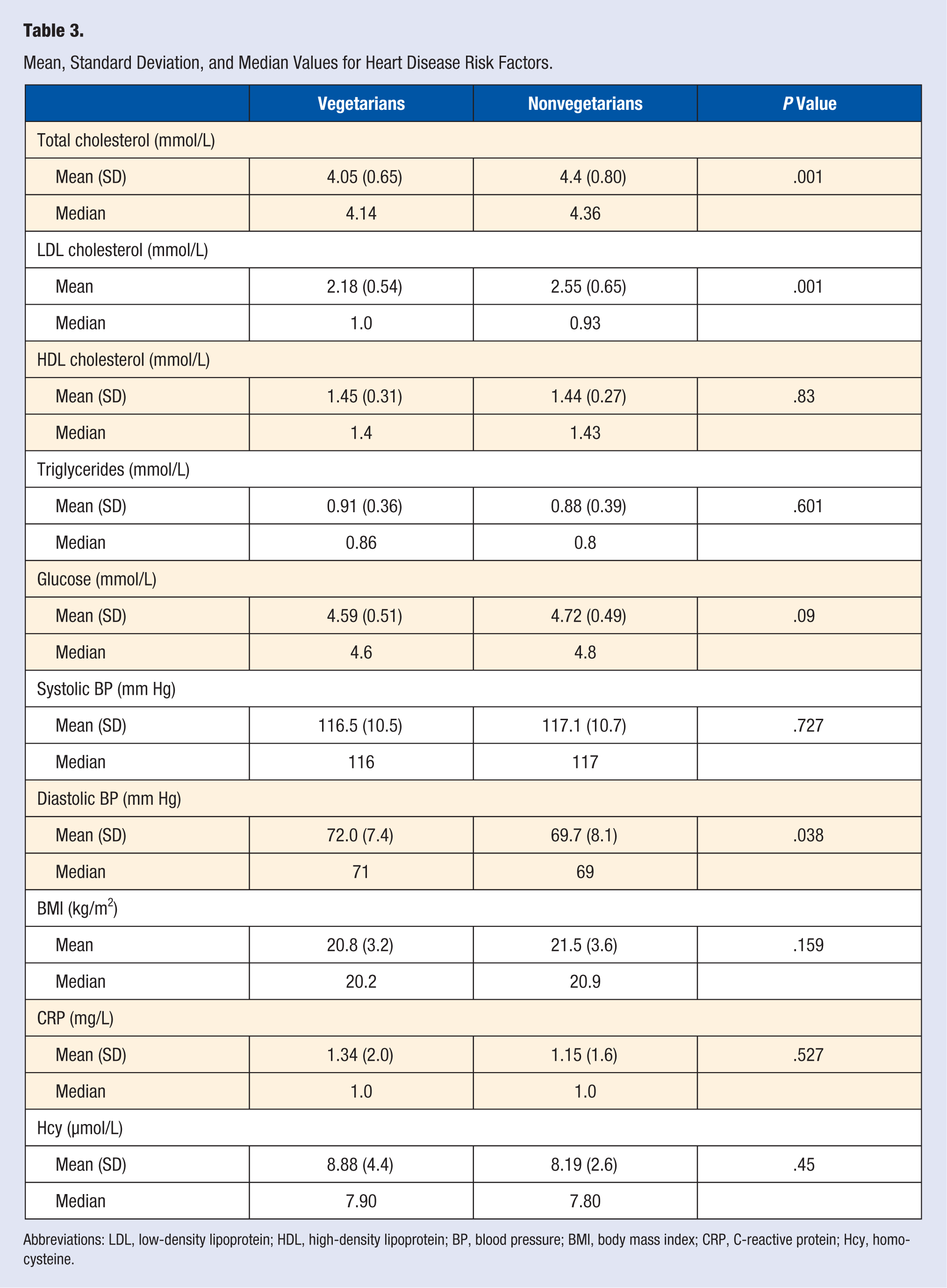
Abbreviations: LDL, low-density lipoprotein; HDL, high-density lipoprotein; BP, blood pressure; BMI, body mass index; CRP, C-reactive protein; Hcy, homocysteine.
Prevalence of Participants With Abnormal Values
There was a statistically significant difference in the percentage of participants with abnormal total and LDL cholesterol level between vegetarians and nonvegetarians (31.1% vs 46.2%,P = .036, having total cholesterol ≥4.4 mmol/L and 13.3% vs 29.6%, P = .021, having LDL cholesterol ≥2.84 mmol/L). A statistically significant greater percentage of vegetarians, compared with nonvegetarians, had elevated diastolic BP (≥80 mm Hg; 12.2% vs 6.8%, P = .038). There was no statistically significant difference in the percentage of participants in different diet groups of all other risk factors (HDL: P = .527; TAG: P = .608; systolic BP:P = .724; glucose: P = 1; BMI: P = .159; Hcy: P = .33; and CRP: P = .527).
Prevalence of Participants With a Cluster of Risk Factors
Cluster analyses included assessment of 3 or more and 4 or more risk factors from total cholesterol, LDL, HDL, TAG, BMI > 24.9, systolic BP > 120, and diastolic BP > 80. The percentage of vegetarian participants with 3 or more risk factors was comparable to that of nonvegetarians (12.2% vs 13.9%, P = 1). The percentage of participants with 4 or more risk factors was 2.0% in the vegetarian and 2.7% in the nonvegetarian (P = 1.0) groups.
Discussion
Since CVD constitutes the leading cause of mortality and because the development of atherosclerosis begins in childhood, it is important to evaluate the presence of CVD risk factors among the youth. In the current study, we have evaluated the presence of CVD risk factors in adolescents adhering to vegetarian and nonvegetarian diets. Consistent with our hypothesis, vegetarians had both a lower mean total and mean LDL cholesterol. Also, fewer vegetarians, compared with nonvegetarians, had abnormal total and LDL cholesterol levels. Inconsistent with our hypothesis, we found no statistically significant difference in most of the other risk factors, except for diastolic BP, which was higher among vegetarians though the mean was still well within the normal range (Table 3).
Assessment of CVD Risk Factors by Diet Group
Statistically significant differences in the mean values of the CVD risk factors that we assessed was found only for the total and LDL cholesterol, and diastolic BP. Findings that have shown lower total and LDL cholesterol among vegetarian participants is consistent with research reports with adults. In a meta-analysis based on 11 randomized control trials, participants assigned to a vegetarian diet had a reduced mean total (−0.36 mmol/L; 95% confidence interval [CI] = 0.55-0.17; P < .001) and LDL cholesterol (−0.34 mmol/L; 95% CI = 0.57-0.11; P < .001) compared with participants assigned to control diets. 21 Similarly, Ferdowsian and Barnard concluded, based on 27 randomized control and observational studies, that primary plant-based and LOV dietary interventions decreased both total and LDL cholesterol by about 10% to 15%, while vegan dietary interventions decreased total and LDL cholesterol by approximately 15% to 25%. 5
Data on CVD risk factors among adolescents, especially vegetarian adolescents, is scarce. We found only one previously published study that reported total cholesterol among vegetarian adolescents from Australia (89 girls and 94 boys). 22 Adolescents in this group were from Seventh-Day Adventist schools around Sydney, Australia. They were between 12 and 17 years of age. Although this study was published more than 40 years ago, their results are remarkably consistent with those from our study. The mean total cholesterol among these participants was 4.2 ± 0.73 mmol/L, compared with 4.04 ± 0.65 mmol/L in our study. When these individuals were divided into those who occasionally or regularly consumed meat, fish, or fowl (n = 78) and those who were total vegetarians (n = 105), the mean total cholesterol in these diet groups was 4.4 ± 0.73 mmol/L and 4.0 ± 0.70 mmol/L, respectively. Total cholesterol of a control group that was composed of 1456 “free living” non-Adventist individuals was 5.2 ± 0.83 mmol/L, which is higher than the total cholesterol level among nonvegetarians from our sample (4.4 mmol/L). 22
Blood lipids were also assessed among 40 adolescents who, for 8 months, lived at a Seventh-day Adventists boarding school near Chicago, Illinois. Their mean total cholesterol of 137.5 ± 14.9 mg/dL (3.56 ± 0.37 mmol/L) was lower than among vegetarian participants in our study (Table 3). 23
Leung et al reported data on lipid profiles among 47 vegetarian children from Hong Kong. In the subgroup of participants older than 11 years, the total and LDL cholesterol was 3.77 ± 0.41 and 2.09 ± 0.48, respectively. 24 Shridhar et al compared CVD risk factors among 50 vegetarian and 50 nonvegetarian participants, 18 to 25 years old. 25 The mean total cholesterol level for vegetarian and nonvegetarian groups was 143.4 mg/dL (3.71 mmol/L) versus 146.8 mg/dL (3.80 mmol/L), respectively. The low mean total cholesterol among nonvegetarians in this study may reflect relatively low meat and/or fat intake of the Indian population. They also found no statistically significant difference in any of the risk factors they assessed (fasting blood glucose, total, LDL, HDL and VLDL cholesterol, TAG, BP, and BMI) between participants in the respective dietary groups.
The findings that have shown vegetarian participants having a statistically significantly higher mean diastolic BP is contrary to our hypothesis and inconsistent with findings reported from studies with adults. In a meta-analysis based on 7 control clinical trials and 32 observational studies, Yokoyama et al found vegetarians to have a reduced diastolic BP (−2.2 mm Hg; 95% CI = −3.5 to −1.0; P < 0.001). 26 In the only study that we found that reported BP among vegetarian adolescents, the mean diastolic BP was low (65.7 ± 9.70 mm Hg). 22 It is unclear why, unlike in studies with adults, vegetarians had a higher mean diastolic BP, compared with nonvegetarians. However, Tamai et al found that in children with high folic acid intake, vitamin B12 intake was significantly inversely associated with both systolic and diastolic BP among children 4 to 6 years of age (mean diastolic BP in the lowest vitamin B12 quartile intake was 62.8 vs 56.9 [P = .002], for the highest quartile intake). 27 Thus, the difference in vitamin B12 concentration between participants in the 2 diet groups may have affected their BP reading. Nonetheless, we found the mean diastolic BP among both groups was relatively low and within the normal range.
Prevalence of Participants With Abnormal Values
We found statistically significant differences in the percentage of participants in different diet groups with abnormal total and LDL cholesterol levels (31.1% vs 46.2%, P = .036, and 13.3% vs 29.6%, P = .021, for vegetarians and nonvegetarians, respectively). The prevalence of vegetarian adolescents with abnormal total cholesterol in our study was considerably higher compared with that reported in vegetarians from Hong Kong (31.1% vs 6.4%). 24 The prevalence of total cholesterol 200 mg/dL (5.17 mmol/L) or more among 12- to 15-year-old American adolescents is 6.8%, while it is 8.9% among those 16 to 19 years of age. 28 In our sample, the prevalence of those with total cholesterol above 5.17 mmol/L among vegetarians was 2.0%, while among nonvegetarians it was 16.5%. In the Bogalusa Heart Study, 9% of 11- to 17-year-old participants had total cholesterol above 200 mg/dL (5.17 mmol/L). 29
In the Bogalusa Heart Study, 11% of 11- to 19-year-old participants had HDL cholesterol below 35 mg/dL (0.91 mmol/L). 29 Williams et al reported 12.3% of 12- to 17-year-old participants of the 2007-2010 National Health and Nutrition Examination Survey having HDL cholesterol below 40 mg/dL (1.03 mmol/L). 30 In our samples, low HDL cholesterol was found in 8.1% of vegetarian and 5.9% nonvegetarian participants (P = .527).
As indicated, the percentage of participants with total cholesterol≥4.4 mmol/L was relatively high (31.1% vs 46.2%, in vegetarian and nonvegetarian participants, respectively). In adults, it has been shown that a considerably lower total cholesterol (<3.8 mmol/L or <4.14 mmol/L) is the most protective.31-33 The fact that a high percentage of participants had an abnormal total cholesterol and that, in addition, close to 30% of nonvegetarian adolescents had LDL cholesterol ≥2.84 mmol/L, constitute the most worrisome finding of this study. In adults, LDL cholesterol is considered a key risk factor for CVD. It is associated with ischemic heart disease mortality among adults of all ages. This finding stresses the need for cholesterol screening among Australian adolescents and, potentially, to implement appropriate lifestyle modifications to improve their blood lipid profile.
More than one third of participants in each diet group (34.7% for vegetarians and 35.9% in nonvegetarians) had systolic BP above 120 mm Hg. Considerably lower prevalence of raised diastolic BP was found in each diet group (12.2% vs 6.8%). According to the World Health Organization, in some age groups each increase of 20 mm Hg of systolic BP and 10 mm Hg of diastolic BP, starting as low as 115 mm Hg over 75 mm Hg, doubles the risk of CVD. 34 While the above statement may not be true for adolescents, as BP increases with age, if elevated BP is carried into adulthood, it will increase risk of future CVD.
As is the case with most other CVD risk factors, there are limited data on BP and the prevalence of hypertension among adolescents. Findings from the Australian Health Survey 2011-2012 have shown that 28% males and 14% females 15 to 24 years of age had high normal BP, defined as BP between 120/80 and 140/90 mm Hg. 35 Data from the United States showed that 14% of 8- to 17-year-old adolescent males and 6% of their female counterparts have pre-hypertension, while 3% to 4% have hypertension. 36 The above data indicate that, among adolescents, elevated BP is more prevalent that may have been expected. The high prevalence of higher than normal systolic BP among vegetarian participants in our study is especially surprising considering findings among vegetarian adults. A meta-analysis based on studies that assessed BP among vegetarian and nonvegetarian adults have shown vegetarians having a mean 6.9 mm Hg lower systolic BP and a mean 4.7 mm Hg lower diastolic BP among vegetarians. 25 Vegetarians have been shown to have a high prevalence of vitamin B12 deficiency along with high prevalence of hyperhomocysteinemia, both of which are associated with elevated BP. Lowering of Hcy has been shown to lower BP in children. 37 In this sample, over 81% of vegetarian participants had Hcy concentration above 10 µmol/L. Thus, Hcy may have been a contributing factor to the surprisingly high prevalence of elevated BP among vegetarians.
Prevalence of Participants With a Cluster of Risk Factors
It has been shown that the presence of a cluster of CVD risk factors in childhood is associated with premature atherosclerosis and future clinical manifestations of CVD in adulthood.15,17 For example, findings from the Bogalusa Heart Study have shown that the extent of atherosclerosis in the coronary arteries was markedly increased among individuals with multiple risk factors. 17 In that study, individuals with 3 or 4 risk factors had 8.5 times greater fatty streak lesions and 12 times the number of fibrous-plaque lesions in the coronary arteries, compared with those with no risk factors.
In our study, 6 vegetarians (12.2%) and 89 nonvegetarians (13.9%) (P = 1) had 3 or more risk factors, and 1 vegetarian (2.0%) and 17 nonvegetarians (2.7%) (P = 1.0) had 4 or more risk factors. Only 2 participants, both nonvegetarians, had abnormal values for all lipids (total, LDL, and HDL cholesterol, and TAG) and none of the participants had all abnormal traditional risk factors (all lipids, glucose, systolic and diastolic BP, and BMI).
The prevalence of metabolic syndrome (participants had to meet 3 of 5 risk factors to be classified as having metabolic syndrome) in Australian adolescents was reported to be 3.6% or 4.0%. 38 We found a higher percentage of participants, especially among nonvegetarians, having 3 or more CVD risk factors. The prevalence of abnormal risk factors increases with age. Our participants were slightly older, compared with the other sample (14-17 years old vs 13-15 years old.) The older age of the participants in our study may, at least in part, explain why we found a higher percentage of participants with 3 or more risk factors. Another explanation may have to do with the cutoff for abnormal risk factors that we used versus the definition used to identify individuals with metabolic syndrome.
Nontraditional Risk Factors for CVD
Although there was no statistically significant difference in the mean Hcy or CRP between the 2 diet groups and the means were somewhat low and within normal ranges, the prevalence of abnormal Hcy and CRP concentrations was somewhat high. In each diet group, the prevalence of Hcy ≥ 10 µmol/L was over 18%. CRP > 3 was found in 8.3% of vegetarian and 6.5% of nonvegetarian participants. The high prevalence of elevated Hcy in such young age should be of concern. In adults, studies have shown a risk for coronary artery disease is represented by a continuum of total homocysteine concentration, with substantial risk occurring between 10 and 15 µmol/L, and that each increase of 5 µmol/L increases the risk by close to 20%.39,40 It is thus important to ensure adequate vitamin B12 intake and status among vegetarians, as Hcy in vegetarians is mainly reflective of vitamin B12 level.43,44 It is also important to screen vegetarians for their vitamin B12 and Hcy concentrations to ensure any deficiency is promptly diagnosed and treated. 45 This is especially important among vegetarians with gene mutation affecting Hcy metabolism, such as methylene tetrahydrofolate reductase. 46
Strengths and Limitations
One of the strengths of our study is the somewhat narrow age range of vegetarian and nonvegetarian participants (14-17 years). Nonetheless, the findings represent a cross-sectional analysis with adolescents from Central Coast regions and Hunter regions of New South Wales, Australia. Most of the participants were Caucasian. Thus, the findings may not reflect CVD risk factors for adolescents from other parts of Australia and other countries and for adolescents of other than Caucasian ethnic background. Also, we have applied adult criteria for abnormal BMI (BMI > 24.9) in our analyses rather than above 85th percentile, which is used in children and adolescents. This may have misclassified some of our participants. Last, food and nutrient intake is important to identify specific dietary pattern along with excessive or inadequate intake of specific nutrients that may contribute to CVD risk. Even a vegetarian diet may increase CVD risk if it contains excessive amounts of certain nutrients (eg, sodium) or is deficient in nutrients (eg, vitamin B12). Future studies should examine nutrient intake and its effect on risk of CVD.
Conclusions
The findings are somewhat consistent with those reported in research with adult vegetarian and nonvegetarian individuals showing a lower mean concentration of total and LDL cholesterol among the former. Surprisingly high prevalence rate of participants had abnormal total and LDL cholesterol, which was especially true for nonvegetarians. A higher percentage of vegetarian versus nonvegetarian participants had elevated diastolic BP, while the mean diastolic BP was within normal range for participants in each diet group. The prevalence rate of participants with 3 or more risk factors was similar among vegetarian (12.2%) and nonvegetarian (13.9%) participants. While the means for Hcy and CRP were within normal ranges, almost 1 of 5 participants in each diet group had elevated Hcy concentration.
Other risk factors that we did not assess, including physical activity and psychosocial index, also play a role in atherosclerosis and CVD risk. 4 Future studies should assess how these factors affect atherosclerosis risk in adolescents and whether there are any differences in between factors among vegetarians and nonvegetarians.
Footnotes
Acknowledgements
We would like to thank all participating individuals and schools where data collection took place.
Author’s note
Ross Grant is also affiliated with From the Sydney Adventist Hospital Clinical School, Faculty of Health Sciences, University of Sydney, New South Wales, Australia; Australasian Research Institute, Sydney Adventist Hospital, Sydney, New South Wales, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was sponsored by the Novus Foundation, Australia, and Sanitarium Food Company, Australia.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
The study protocol was approved by the Sydney Adventist Hospital Human Research Ethics Committee.
Trial Registration
Not applicable, because this article does not contain any clinical trials.